

Classification of Blood Pressure Levels Based on Photoplethysmogram and Electrocardiogram Signals with a Concatenated Convolutional Neural Network
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset and Preprocessing
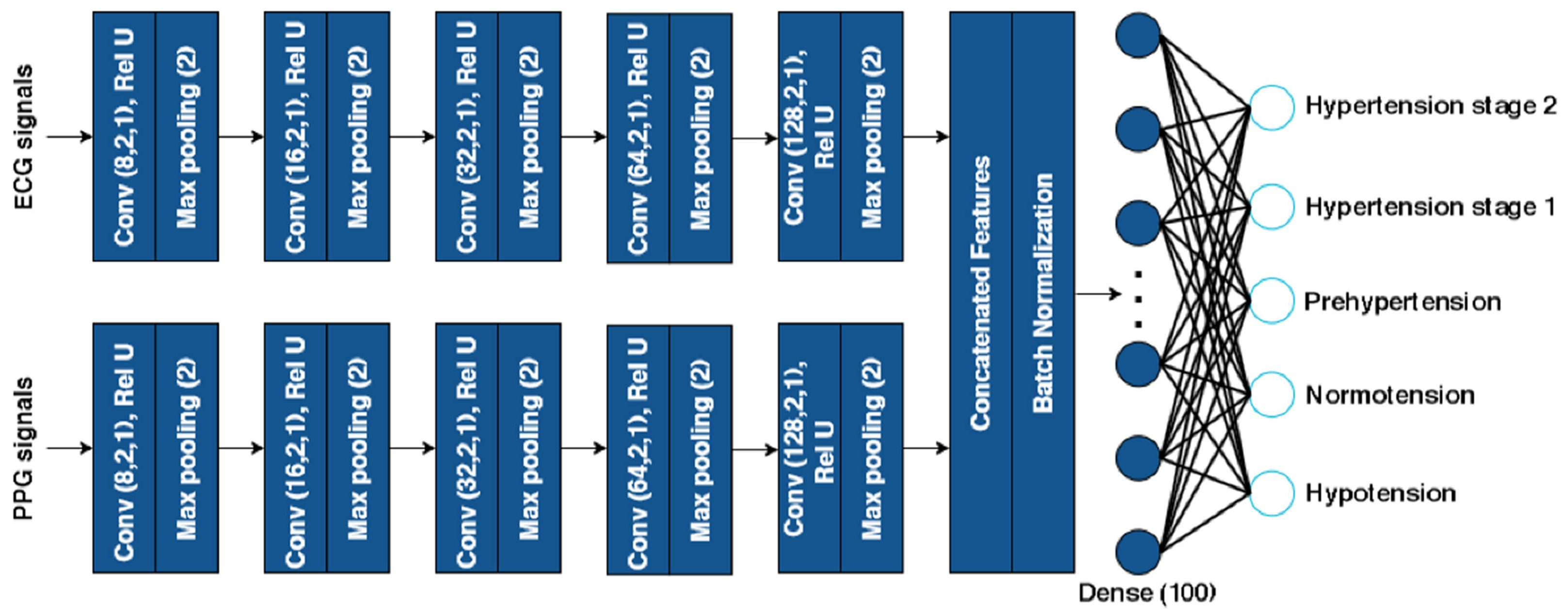
2.2. Concatenated 1D CNN Architecture
2.3. Evaluation Matrix
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Ji, X.; Xiao, Y.; Zhang, Y.; Chen, B.; Liu, H.; Zhou, S. Prediction of hypertension outcomes based on gain sequence forward tabu search feature selection and xgboost. Diagnostics 2021, 11, 792. [Google Scholar] [CrossRef]
- Abbas Q, Qureshi I, Ibrahim MEA. An automatic detection and classification system of five stages for hypertensive retinopathy using semantic and instance segmentation in densenet architecture. Sensors 2021, 21, 6936. [Google Scholar] [CrossRef] [PubMed]
- Kumanan, T.; Guruparan, M.; Sreeharan, N. Hypertension “The Silent Killer” A Guide for Primary Care Physicians and Healthcare Professionals; Kumaran Book House: Chennai, India, 2018; pp. 1–81. [Google Scholar]
- Hansen, E.; Grimm, D.; Wehland, M. Current Knowledge about the New Drug Firibastat in Arterial Hypertension. Int. J. Mol. Sci. 2022, 23, 1459. [Google Scholar] [CrossRef]
- Ogedegbe, G.; Agyemang, C.; Ravenell, J.E. Masked hypertension: Evidence of the need to treat. Curr. Hypertens. Rep. 2010, 12, 349–355. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Barbosa, K.; Ho, V.; Griggs, D.; Ghirmai, T.; Krishnan, S.K.; Hsiai, T.K.; Chiao, J.C.; Cao, H. Cuff-Less and Continuous Blood Pressure Monitoring: A Methodological Review. Technologies 2017, 5, 21. [Google Scholar] [CrossRef] [Green Version]
- Palatini, P.; Asmar, R. Cuff challenges in blood pressure measurement. J. Clin. Hypertens. 2018, 20, 1100–1103. [Google Scholar] [CrossRef] [Green Version]
- Sagirova, Z.; Kuznetsova, N.; Gogiberidze, N.; Gognieva, D.; Suvorov, A.; Chomakhidze, P.; Omboni, S.; Saner, H.; Kopylov, P. Cuffless blood pressuremeasurement using a smartphone-case based ECG monitor with photoplethysmography in hypertensive patients. Sensors 2021, 21, 3525. [Google Scholar] [CrossRef]
- Bard, D.M.; Joseph, J.I.; van Helmond, N. Cuff-Less Methods for Blood Pressure Telemonitoring. Front. Cardiovasc. Med. 2019, 6, 40. [Google Scholar] [CrossRef]
- Ibrahim, B.; Jafari, R. Cuffless blood pressure monitoring from a wristband with calibration-free algorithms for sensing location based on bio-impedance sensor array and autoencoder. Sci. Rep. 2022, 12, 319. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.H.; Kang, M.K.; Choi, C.E.; Min, J.; Lee, H.Y.; Lim, S. Validation of a wearable cuff-less wristwatch-type blood pressure monitoring device. Sci. Rep. 2020, 10, 19015. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D.U.; Lim, K.M. Combined deep CNN–LSTM network-based multitasking learning architecture for noninvasive continuous blood pressure estimation using difference in ECG-PPG features. Sci Rep. 2021, 11, 13539. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.H.; Shuzan, M.N.I.; Chowdhury, M.E.; Mahbub, Z.B.; Uddin, M.M.; Khandakar, A.; Reaz, M.B.I. Estimating blood pressure from the photoplethysmogram signal and demographic features using machine learning techniques. Sensors 2020, 20, 3127. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M.; Fletcher, R.; Liang, Y.; Howard, N.; Lovell, N.H.; Abbott, D.; Lim, K.; Ward, R. The use of photoplethysmography for assessing hypertension. NPJ Digit. Med. 2019, 2, 60. [Google Scholar] [CrossRef] [Green Version]
- Xing, X.; Ma, Z.; Zhang, M.; Zhou, Y.; Dong, W.; Song, M. An Unobtrusive and Calibration-free Blood Pressure Estimation Method using Photoplethysmography and Biometrics. Sci. Rep. 2019, 9, 8611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.; Park, N.; Lee, H.; Hwang, C.; Kim, J.H.; Park, S. Systematic review on human skin-compatible wearable photoplethysmography sensors. Appl. Sci. 2021, 11, 2313. [Google Scholar] [CrossRef]
- Přibil, J.; Přibilová, A.; Frollo, I. Comparative Measurement of the PPG Signal on Different Human Body Positions by Sensors Working in Reflection and Transmission Modes. Eng. Proc. 2020, 2, 69. [Google Scholar] [CrossRef]
- Uwamahoro, R.; Mushikiwabeza, A.; Minani, G.; Murari, B.M. Universal design of a microcontroller and IoT system to detect the heart rate. IOP Conf. Ser. Mater. Sci. Eng. 2017, 263, 052037. [Google Scholar] [CrossRef] [Green Version]
- Liang, Y.; Chen, Z.; Ward, R.; Elgendi, M. Hypertension assessment using photoplethysmography: A risk stratification approach. J. Clin. Med. 2019, 8, 12. [Google Scholar] [CrossRef]
- Elgendi, M. On the Analysis of Fingertip Photoplethysmogram Signals. Curr. Cardiol. Rev. 2012, 8, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Seok, H.S.; Kim, S.S.; Shin, H. Photoplethysmogram Analysis and Applications: An Integrative Review. Front. Physiol. 2022, 12, 2511. [Google Scholar] [CrossRef] [PubMed]
- Mejía-Mejía, E.; Kyriacou, P.A. Duration of Photoplethysmographic Signals for the Extraction of Pulse Rate Variability. SSRN Electron. J. 2022, 80, 104214. [Google Scholar] [CrossRef]
- Schäfer, A.; Vagedes, J. How accurate is pulse rate variability as an estimate of heart rate variability?: A review on studies comparing photoplethysmographic technology with an electrocardiogram. Int. J. Cardiol. 2013, 166, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Abbott, D.; Howard, N.; Lim, K.; Ward, R.; Elgendi, M. How Effective is Pulse Arrival time for Evaluating Blood Pressure? Challenges and Recommendations from a study using the MIMIC Database. J. Clin. Med. 2019, 8, 337. [Google Scholar] [CrossRef] [Green Version]
- Takazawa, K.; Tanaka, N.; Fujita, M.; Matsuoka, O.; Saiki, T.; Aikawa, M.; Tamura, S.; Ibukiyama, C. Assessment of vasoactive agents and vascular aging by the second derivative of photoplethysmogram waveform. Hypertension 1998, 32, 365–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Po, L.M.; Fu, H. Cuffless Blood Pressure Estimation Based on Photoplethysmography Signal and Its Second Derivative. Int. J. Comput. Theory Eng. 2017, 9, 202–206. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Singh, A.; Sharma, A.; Tripathy, R.K. Higher-order Derivatives-based Integrated Model for Cuff-less Blood Pressure Estimation and Stratification using PPG Signals. IEEE Sens. J. 2022, 22, 22030–22039. [Google Scholar] [CrossRef]
- Khodabakhshi, M.B.; Eslamyeh, N.; Sadredini, S.Z.; Ghamari, M. Cuffless blood pressure estimation using chaotic features of photoplethysmograms and parallel convolutional neural network. Comput. Methods Programs Biomed. 2022, 226, 107131. [Google Scholar] [CrossRef]
- Wu, J.; Liang, H.; Ding, C.; Huang, X.; Huang, J.; Peng, Q. Improving the Accuracy in Classification of Blood Pressure from Photoplethysmography Using Continuous Wavelet Transform and Deep Learning. Int. J. Hypertens. 2021, 2021, 9938584. [Google Scholar] [CrossRef]
- Sun, X.; Zhou, L.; Chang, S.; Liu, Z. Using cnn and hht to predict blood pressure level based on photoplethysmography and its derivatives. Biosensors 2021, 11, 120. [Google Scholar] [CrossRef]
- Yen, C.T.; Chang, S.N.; Liao, C.H. Deep learning algorithm evaluation of hypertension classification in less photoplethysmography signals conditions. Meas. Control. 2021, 54, 439–445. [Google Scholar] [CrossRef]
- Tanveer, M.S.; Hasan, M.K. Cuffless blood pressure estimation from electrocardiogram and photoplethysmogram using waveform based ANN-LSTM network. Biomed. Signal Process. Control 2019, 51, 382–392. [Google Scholar] [CrossRef] [Green Version]
- Fuadah, Y.N.; Lim, K.M. Optimal Classification of Atrial Fibrillation and Congestive Heart Failure Using Machine Learning. Front. Physiol. 2022, 12, 2571. [Google Scholar] [CrossRef] [PubMed]
- Fu’adah, Y.N.; Lim, K.M. Classification of Atrial Fibrillation and Congestive Heart Failure Using Convolutional Neural Network with Electrocardiogram. Electronics 2022, 11, 2456. [Google Scholar] [CrossRef]
- Taye, G.T.; Hwang, H.J.; Lim, K.M. Application of a convolutional neural network for predicting the occurrence of ventricular tachyarrhythmia using heart rate variability features. Sci. Rep. 2020, 10, 6769. [Google Scholar] [CrossRef] [Green Version]
- Monroy Estrada, G.; Mendoza, L.E.; Molina, V. Relationship of blood pressure with the electrical signal of the heart using signal processing. Tecciencia 2014, 9, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Hassing, G.J.; van der Wall, H.E.; van Westen, G.J.; Kemme, M.J.; Adiyaman, A.; Elvan, A.; Burggraaf, J.; Gal, P. Blood pressure-related electrocardiographic findings in healthy young individuals. Blood Press. 2020, 29, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.Y.; Jang, J.H.; Kwon, J.M.; Lee, H.C.; Jung, C.W.; Byun, S.; Jeong, H.G. Predicting intraoperative hypotension using deep learning with waveforms of arterial blood pressure, electroencephalogram, and electrocardiogram: Retrospective study. PLoS ONE 2022, 17, e0272055. [Google Scholar] [CrossRef]
- Bae, T.W.; Kim, M.S.; Park, J.W.; Kwon, K.K.; Kim, K.H. Multilayer Perceptron-Based Real-Time Intradialytic Hypotension Prediction Using Patient Baseline Information and Heart-Rate Variation. Int. J. Environ. Res. Public Health 2022, 19, 10373. [Google Scholar] [CrossRef]
- Soh, D.C.K.; Ng, E.Y.K.; Jahmunah, V.; Oh, S.L.; Tan, R.S.; Acharya, U.R. Automated diagnostic tool for hypertension using convolutional neural network. Comput. Biol. Med. 2020, 126, 10399. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Gajbhiye, P.; Tripathy, R.K.; Acharya, U.R. A two-stage deep CNN architecture for the classification of low-risk and high-risk hypertension classes using multi-lead ECG signals. Inform. Med. Unlocked 2020, 21, 100479. [Google Scholar] [CrossRef]
- Rajput, J.S.; Sharma, M.; Acharya, U.R. Hypertension diagnosis index for discrimination of high-risk hypertension ECG signals using optimal orthogonal wavelet filter bank. Int. J. Environ. Res. Public Health 2019, 16, 4068. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.; Rajput, J.S.; Tan, R.S.; Acharya, U.R. Automated detection of hypertension using physiological signals: A review. Int. J. Environ. Res. Public Health 2021, 18, 5838. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, Z.; Ward, R.; Elgendi, M. Hypertension Assessment via ECG and PPG Signals: An Evaluation Using MIMIC Database. Diagnostics 2018, 8, 65. [Google Scholar] [CrossRef] [Green Version]
- Kuzmanov, I.; Bogdanova, A.M.; Kostoska, M.; Ackovska, N. Fast Cuffless Blood Pressure Classification with ECG and PPG signals using CNN-LSTM Models in Emergency Medicine. In Proceedings of the 2022 45th Jubilee International Convention on Information, Communication and Electronic Technology (MIPRO), Opatija, Croatia, 23–27 May 2022; pp. 362–367. [Google Scholar] [CrossRef]
- Kuzmanov, I.; Kostoska, M.; Bogdanova, A.M. Blood pressure class estimation using CNN-GRU model. In proceeding of the 19th International Conference on Informatics and Information Technologies, CIIT, North Macedonia, 5–6 May 2022; pp. 1–6. [Google Scholar]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Lehman, L.W.H.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Anthony Celi, L.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [Green Version]
- Malayeri, A.B.; Khodabakhshi, M.B. Concatenated convolutional neural network model for cuffless blood pressure estimation using fuzzy recurrence properties of photoplethysmogram signals. Sci. Rep. 2022, 12, 6633. [Google Scholar] [CrossRef]
- Novakovic, J.D.; Veljovic, A.; Ilic, S.S.; Papic, Z.; Tomovic, M. Evaluation of Classification Models in Machine Learning. Theory Appl. Math. Comput. Sci. 2017, 7, 39–46. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| BP Levels | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Hypotension | <90 | And | <60 |
| Normotension | <120 | And | <80 |
| Prehypertension | 120–129 | And | <80 |
| Hypertension Stage 1 | 130–139 | Or | 80–89 |
| Hypertension Stage 2 | 140–180 | Or | 90–120 |
| Input | Number of Convolutional Layers | Train Accuracy | Validation Accuracy | Test Accuracy | p-Value |
|---|---|---|---|---|---|
| PPG | 1 layer | 47.70–49.10% | 47.51–49.29% | 47.94–49.66% | |
| 2 layers | 49.45–50.55% | 49.45–50.15% | 49.45–50.15% | ||
| 3 layers | 53.56–57.64% | 53.58–58.42% | 53.43–56.57% | ||
| 4 layers | 54.39–60.42% | 54.39–60.42% | 53.82–58.58% | ||
| 5 layers | 59.50–62.90% | 59.63–63.57% | 57.97–61.23% | ||
| ECG | 1 layer | 68.89–71.11% | 68.89–71.10% | 63.44–69.36% | |
| 2 layers | 71.94–73.66% | 71.94–73.66% | 69.64–71.96% | ||
| 3 layers | 69.33–73.07% | 69.62–73.98% | 67.87–70.93% | ||
| 4 layers | 70.63–74.57% | 70.71–75.29% | 69.40–72.20% | ||
| 5 layers | 76.16–79.84% | 76.16–79.84% | 75.63–79.57% | ||
| PPG and ECG | 1 layer | 92.34–94.06% | 92.34–94.06% | 88.76–86.04% | |
| 2 layers | 99.45–99.82% | 99.45–99.82% | 93.55–94.23% | ||
| 3 layers | 100% | 100% | 94.05–94.64% | ||
| 4 layers | 100% | 100% | 94.37–94.97% | ||
| 5 layers | 100% | 100% | 94.56–95.15% |
| CNN Architectures | Configuration (Parallel) | Precision | Recall | F1-Score | AUC |
|---|---|---|---|---|---|
| Architecture 1 | 1 layer (number of filters 8) | 0.86–0.88 | 0.85–0.87 | 0.86–0.87 | 0.96–0.97 |
| Architecture 2 | 2 layers (number of filters 8 and 16) | 0.92–0.93 | 0.92–0.93 | 0.92–0.93 | 0.97–0.98 |
| Architecture 3 | 3 layers (number of filters 8, 16, and 32) | 0.93–0.94 | 0.93–0.94 | 0.93–0.94 | 0.98–0.99 |
| Architecture 4 | 4 layers (number of filters 8, 16, 32, and 64) | 0.93–0.94 | 0.93–0.94 | 0.93–0.94 | 0.98–0.99 |
| Architecture 5 | 5 layers (number of filters 8, 16, 32, 64, and 128) | 0.93–0.95 | 0.93–0.95 | 0.93–0.95 | 0.98–0.99 |
| Authors | Dataset | No of Classes | Method | Performance |
|---|---|---|---|---|
| Wu et al. [31] | PPG signal | 2 classes (normal and abnormal) | CWT and 2D CNN | Accuracy of 90% |
| Sun et al. [32] | PPG signal | 3 classes (normotension, prehypertension, and hypertension) | HHT and 2D CNN | Accuracy of 93.54% |
| Yen et al. [33] | PPG signal | 4 classes (normotension, prehypertension, hypertension stage 1, and hypertension stage 2) | BILSTM and ResNet | Accuracy of 76% |
| Soh et al. [42] | ECG signal | 2 classes (normotension and hypertension) | CNN | Accuracy of 99.99% |
| Jain et al. [43] | ECG signal | 2 classes (normotension and hypertension) | CNN | Accuracy of 99.68% |
| Rajput et al. [44] | ECG signal | 2 classes (normotension and hypertension) | OWFB | Accuracy of 99.95% |
| Sharma et al. [45] | ECG signal | 2 classes (normotension and hypertension) | SVM | Accuracy of 98.05% |
| Liang et al. [46] | PPG and ECG signal | 3 classes (normotension, prehypertension, and hypertension) | K-NN | F1 score of 88.49% |
| Kuzmanov et al. [47] | PPG and ECG signal | 2 classes (hypotension and not hypotension) | LSTM and CNN | Accuracy of 76% |
| Kuzmanov et al. [48] | PPG and ECG signal | 3 classes (normotension, prehypertension, and hypertension) | GRU and CNN | Accuracy of 78% |
| Our study | PPG and ECG signal | 5 classes (hypotension, normotension, prehypertension, hypertension stage 1, and hypertension stage 2) | Concatenated 1D CNN | Accuracy of 95% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuadah, Y.N.; Lim, K.M. Classification of Blood Pressure Levels Based on Photoplethysmogram and Electrocardiogram Signals with a Concatenated Convolutional Neural Network. Diagnostics 2022, 12, 2886. https://doi.org/10.3390/diagnostics12112886
Fuadah YN, Lim KM. Classification of Blood Pressure Levels Based on Photoplethysmogram and Electrocardiogram Signals with a Concatenated Convolutional Neural Network. Diagnostics. 2022; 12(11):2886. https://doi.org/10.3390/diagnostics12112886
Chicago/Turabian StyleFuadah, Yunendah Nur, and Ki Moo Lim. 2022. "Classification of Blood Pressure Levels Based on Photoplethysmogram and Electrocardiogram Signals with a Concatenated Convolutional Neural Network" Diagnostics 12, no. 11: 2886. https://doi.org/10.3390/diagnostics12112886