
Non-Invasive Prenatal Testing in Germany


Abstract
:1. Introduction
2. Technical Bases of NIPT
- (a)
- trisomy 13, 18 and 21, only;
- (b)
- aforementioned trisomies and for changes in the copy numbers of sex chromosomes;
- (c)
- all mentioned in b) plus only DiGeorge syndrome [19];
- (d)
- all mentioned in b) plus other selected microdeletion or microduplication syndromes [20];
- (e)
- all mentioned in (b), (c) or (d) plus all other copy number changes of all other autosomes;
- (f)
- whole genome, for any kind of copy number alteration.
- (g)
- Finally, some NIPT providers have started to also offer screening for point mutations of specific genes, such as the Rhesus factor and blood groups.
3. NIPT and Its Advantages
- I.
- can be applied earlier than other tests during pregnancy;
- II.
- has the potential to reach populations with no access to centers offering invasive diagnostics [23];
- III.
- can exclude and detect a trisomy 21 with the highest probability of all non-invasive approaches—the positive predictive value (PPV) in cases of a NIPT suggesting trisomy 21 is >99%;
- IV.
- can bring a psychological relief to an anxious pregnant woman in the case of a normal NIPT result; and
- V.
4. NIPT and Its Practical Restrictions and Shortcuts
- (a)
- The term NIPT suggests to the uninformed public that the platform studies cell free fetal DNA (cffDNA); however, all cell free DNA in the pregnant individual’s blood (not being of maternal origin) derives from the placenta (and not the fetus); thus, in 1–2% of the cases studied by NIPT, a placenta confined mosaic condition must be expected. They constitute a part of the false positive and negative NIPT results [14,18].
- (b)
- Each abnormal NIPT result has to be checked by an invasive prenatal test, optimally an AC, as indicated by each commercial NIPT provider in the package leaflet [8]. However, one major motivation to do NIPT is to avoid any invasive procedure, due to the previously suggested high abortion risk [3,4,5,6].
- (c)
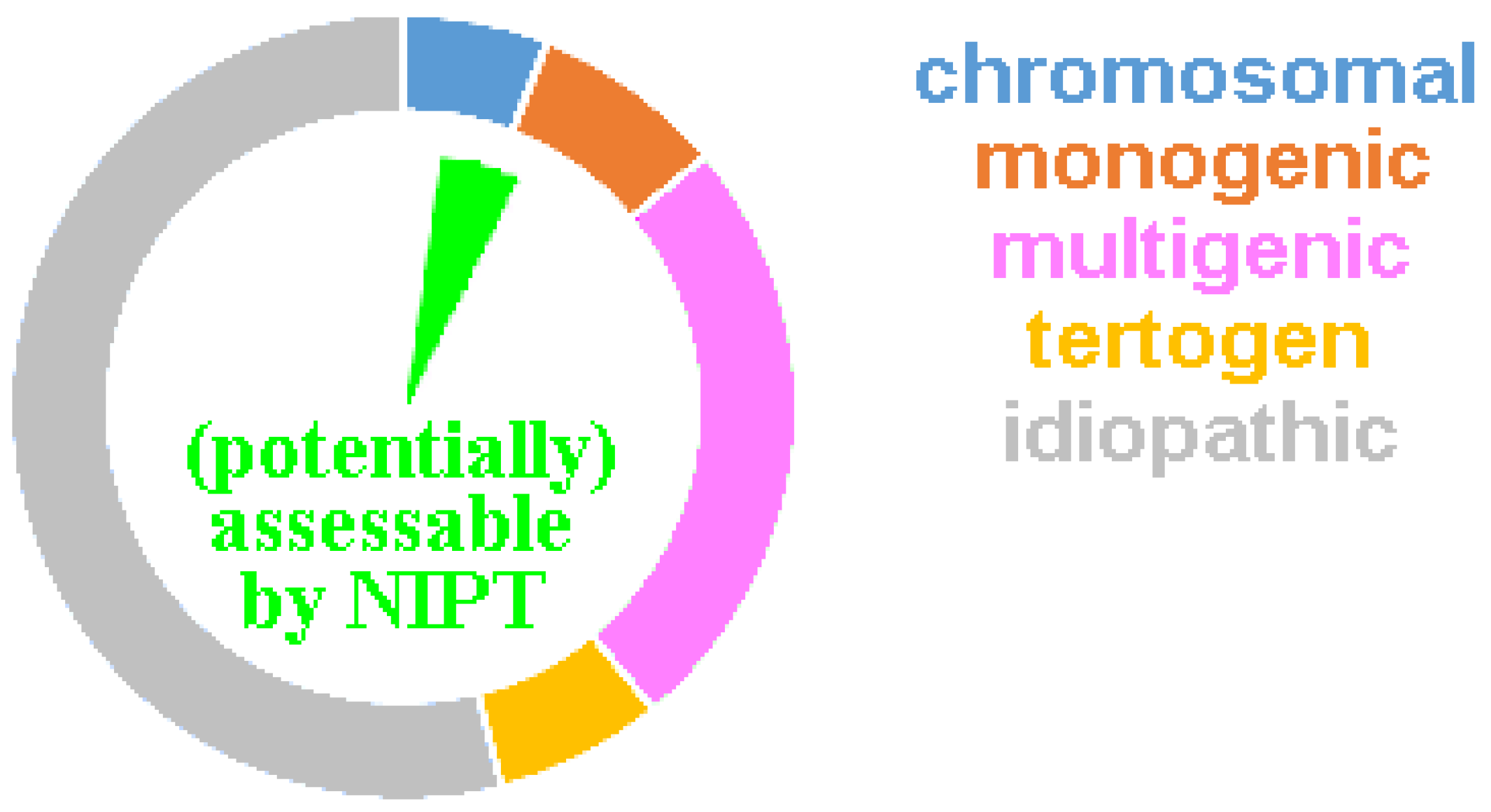
- A normal NIPT result can maximally exclude (to a certain extent) genetic conditions, which are covered by the NIPT platform used. A normal NIPT is never synonymous with the statement: ‘a healthy child will be born’ [25]. As recently shown, NIPT can at best detect 5–10% of all cases potentially born with birth defects [18] (Figure 1).
- (d)
- 90% of aneuploid fetuses detected in NIPT would be aborted naturally and do not survive to birth [18]. Thus, 90% of pregnant women with a true abnormal NIPT result would not have to undergo an induced abortion.
- (e)
- 5–10% of NIPTs provide no result at the first attempt—this is most often due to the low fraction of cell-free placenta derived DNA. The greater the obesity severity in pregnant women, the more likely a ‘no-call’ result will occur [14,18]. The number of cases repeated is not extensively reported in the literature, which could yield data on how many of these cases ultimately yield an informative result. However, it should be noted that within this population, there is overrepresentation of cases ending in an early abortion, largely attributed to a placenta that is too small for the gestational age and preeclampsia.
- (f)
- (g)
- (h)
- As aforementioned, the PPV for trisomy 21 is >99% in all available NIPTs; however, it is neither known nor studied why screening for trisomies 13 and 18, is less reliable. PPVs for all other tested copy number changes (including sex chromosomes, other autosomes, and microdeletion/-duplications) remain substantially lower between 5 and 60—which means 40 to 95% of women receiving an abnormal NIPT result have indeed received a false positive result [18].
- (i)
- In a worldwide perspective, there are hints in the literature that in ~20% of cases, there is a strong tendency to trust an abnormal NIPT result so much that a second test is skipped and termination of the pregnancy is simply based on a single screening test [18,29]. Such policies are also reinforced by the cost-effectiveness of NIPT analyses, which inappropriately encourage NIPT use as a diagnostic versus a screening tool [30].
(1) “The high specificity, efficiency and safety (non-invasiveness) of NIPT can effectively improve the detection rate of common chromosomal aneuploidy, thereby reducing the occurrence of birth defects” [32]; or (2) “NIPT has revolutionized the approach to prenatal diagnosis and, to date, it is the most superior screening method for the common autosomal aneuploidies”. [33]
5. NIPT in Germany
“Although the NIPT is part of the statutory health insurance benefits, it is not one of the generally recommended preventive examinations for all pregnant women. This has been repeatedly emphasized by the Federal Joint Committee, which decides on health insurance benefits. The fund pays for the test if there are indications of a trisomy, such as a conspicuous ultrasound, or if “a woman, together with her doctor, comes to the conclusion that the test is necessary in her personal situation”, according to the information for insured persons. Maternal age alone - often a risk factor for a trisomy—is not yet a reason for a NIPT”.(translated from [34])
“The trisomy test NIPT has been included in the statutory benefits catalog of health insurance companies. Only specialists in gynecology and obstetrics with the qualification “specialized genetic counseling, as well as specialists in human genetics” are allowed to perform the NIPT test after intensive counseling. The NIPT is not part of the generally recommended screening examinations during pregnancy. It is only paid for by health insurance companies if the doctor and patient decide together, after intensive counseling, that the trisomy test makes sense in the personal situation of the pregnant woman. The trisomy test can be useful, especially if there are indications of trisomies through the normal screening examinations or as part of the FTS”.(translated from [35])
- for
- (a) It is not clear to the German public that cffDNA tested in NIPT derives from the placenta [34]; even the NIPT-specific German Genetic Diagnostics Commission (GEKO)-paper does not mention this fact explicitly [37]. In addition, not all German gynecologists working with NIPT, since its introduction, have this issue and the implications in mind [14].
- for
- for
- for
- (d) There is no data for Germany on the number of positive NIPTs, however, the use of NIPT has not led to increases in induced abortions within the last 10 years. There was even a statistically significant decline (Chi squared test: p < 0.0001) in induced abortions from 13.69% down to 10.62% of all pregnancies between 2012 to 2021. This decline was only observable in terminations before the 12th w.o.g. from 13.34% down to 10.28% (Table 2). The reason for this remains unclear, but could be due to a false “feeling of security” after getting a normal NIPT result. This would also correlate well with the use of NIPT in Germany, which was previously (2019) used in ~25% of pregnancies [38] and is nowadays between 50 and 75% [39].
- for
- (e) ‘No-call’ results are also a problem in Germany, but no detailed data is available.
- for
- (f) False positive NIPT results experienced in Germany have been described in a newspaper article in 2020 [25], and negative NIPT results have to be double checked by sonography/FTS to exclude a false negative NIPT result and conditions not tested by the applied NIPT.
- for
- (g) unexpected findings for NIPTs evaluating only trisomies 13, 18 and 21 were also observed in the lab of the author.
- for
- (h) The fact that women with false positive NIPT results feel that not enough recognition to this issue is available to the public, cannot be understated; views that have also been highlighted in the previously mentioned interviews completed by a journalist [25] that covered 10–15 cases with false positive NIPT results. In Germany there also seems to be a lack of information or awareness by gynecologists and obstetricians on the restrictions of NIPT; and many of them seem to be overtaxed in cases of an abnormal NIPT result and how to guide and counsel the concerned woman. Still, as according to the German Gene Diagnostics Act (GenDG) [42] pre- and post-genetic-test counselling must be offered, through time, more training and adaptations to the special conditions of the test can be expected in clinics. Another interesting point implied by the GenDG is that prenatal genetic diagnostics may only be performed for medical purposes, i.e., exclusively targeting disease-relevant genetic characteristics. However, most prenatal diagnostic measures do not have a medical benefit in the narrower sense for the fetus, since the diagnosed diseases or variations (for example, trisomy 21) are not yet accessible to prenatal therapy. For other, e.g., obstetric, considerations concerning the welfare of the future child, ultrasound examinations would usually be perfectly adequate. Most procedures also do not have a preventive benefit. Consequently, special demands are made on education and counseling in the context of prenatal genetic diagnostics. The overriding ethical principle in the context of prenatal diagnostics is the reproductive autonomy of the pregnant woman or couple, and this must be supported by the comprehensive information and experience-oriented counseling [43].
- for
- (i) According to Table 2, NIPT did not lead to an increase, but instead a decrease of first trimester induced abortions in Germany. An increase was also not expected, as all genetic studies in patients are regulated by GenDG, which among other demands stipulates, that before and after each genetic testing, genetic counselling must be offered. Furthermore, German MDs closely attend, supervise, and examine each pregnant woman regularly; thus, it is not conceivable that an induced abortion could be carried out solely based on an abnormal NIPT. At a minimum, an abnormal sonogram must be present, and in cases where a genetic condition is the rationale for an induced abortion, a council consisting of MDs from different departments, including human genetics must always approve the desire for pregnancy termination (at least after the 12th w.o.g.).

{kind=link}
| Year | All Pregnancies | TOP Overall [%] | TOP >12 w.o.g. % | TOP 12–21 w.o.g. % | TOP >21 w.o.g. % |
|---|---|---|---|---|---|
| 2012 | 780,359 | 106,815 [13.69] | 13.34 | 0.30 | 0.06 |
| 2013 | 784,871 | 102,802 [13.10] | 12.74 | 0.29 | 0.07 |
| 2014 | 814,642 | 99,715 [12.24] | 11.90 | 0.27 | 0.07 |
| 2015 | 836,812 | 99,237 [11.86] | 11.52 | 0.26 | 0.08 |
| 2016 | 890,862 | 98,721 [11.08] | 10.76 | 0.25 | 0.07 |
| 2017 | 886,110 | 101,209 [11.42] | 11.11 | 0.23 | 0.07 |
| 2018 | 889,509 | 101,986 [11.47] | 11.04 | 0.24 | 0.07 |
| 2019 | 878,983 | 100,893 [11.48] | 11.15 | 0.26 | 0.07 |
| 2020 | 873,092 | 99,948 [11.15] | 11.11 | 0.26 | 0.07 |
| 2021 | 890,088 | 94,596 [10.62] | 10.28 | 0.27 | 0.08 |
- The GenDG has been interpreted by the GEKO. Surprisingly, the GEKO classified NIPT not as a “prenatal risk screening” but in opposition to all of the corresponding literature data (see above), as a “prenatal genetic analysis for determining the genetic properties” [36]. This is surprising and the rationale for this conclusion may be attributed to political reasons connected to the introduction of NIPT to the scope of services to be billed via the health insurance funds in 2022.
- According to GenDG, it is valid that “if the sex of an embryo or fetus is determined during a prenatal examination, the pregnant woman may be informed of this after the 12th w.o.g. with her consent” (translated from [44]). Thus, NIPT before the 12th w.o.g. can per se only be financed by the insurance companies in Germany if trisomies 13, 18 or 21 are tested exclusively. Other chromosomal imbalances, such as microdeletion and microduplication syndromes are not recommended for evaluation by NIPT in Germany, as they largely result in more invasive procedures in normal fetuses [44].
- Hessel and Henn [45] (2022) also pointed out the following problem: presently it is not possible to select individual NIPT analyses for trisomy 13, 18 or 21, separately. “Therefore, if a pregnant woman wishes to continue a pregnancy for a child with Down syndrome, because she considers this finding reasonable, she may not realize this” (translated from [45]). Furthermore, this conundrum interferes with the “right not to know with regard to parts of the examination result” defined in the GenDG [42,43]. Given that in the context of all current NIPT services, there is no isolated screening for trisomy 21, the prenatal search for Down syndrome has become a medical standard or at worst even a social norm [45].
“We are only at the beginning of a worrisome development because more tests for genetic dispositions are in development and are about to be approved”; and “We are united in our conviction that prenatal screening for trisomy 21, 18 and 13 and others must not become routine in pregnancy under any circumstances”.(translated from [48])
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Darouich, A.A.; Liehr, T.; Weise, A.; Schlembach, D.; Schleußner, E.; Kiehntopf, M.; Schreyer, I. Alpha-fetoprotein and its value for predicting pregnancy outcomes—A re-evaluation. J. Prenat. Med. 2015, 9, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Benn, K.N.; Benn, P.; Campbell, W.A.; Moaddab, A.; Shamshira, A.A. Genetic sonogram: Components and role in the era of prenatal screening. Fetal Matern. Med. Rev. 2014, 25, 214–231. [Google Scholar] [CrossRef]
- Liehr, T.; Lauten, A.; Schneider, U.; Schleussner, E.; Weise, A. Noninvasive prenatal testing (NIPT)—When is it advantageous to apply? Biomed. Hub. 2017, 2, 458432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wulff, C.B.; Gerds, T.A.; Rode, L.; Ekelund, C.K.; Petersen, O.B.; Tabor, A.; Danish Fetal Medicine Study Group. Risk of fetal loss associated with invasive testing following combined first-trimester screening for Down syndrome: A national cohort of 147,987 singleton pregnancies. Ultrasound Obstet. Gynecol. 2016, 47, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Tabor, A.; Alfirevic, Z. Update on procedure-related risks for prenatal diagnosis techniques. Fetal Diagn. Ther. 2010, 27, 1–7. [Google Scholar] [CrossRef]
- Akolekar, R.; Beta, J.; Picciarelli, G.; Ogilvie, C.; D’Antonio, F. Procedure-related risk of miscarriage following amniocentesis and chorionic villus sampling: A systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2015, 45, 16–26. [Google Scholar] [CrossRef]
- Available online: https://www.google.com/search?q=invasive+pr%C3%A4nataldiagnostik+risiken&client=firefox-b-d&biw=1876&bih=970&ei=Wu8_Y-i6OLuBxc8PlsyV0AY&oq=invasive+pr%C3%A4nataldiagnsotik+&gs_lcp=Cgdnd3Mtd2l6EAMYADIHCAAQgAQQDTIHCAAQgAQQDTIHCAAQgAQQDTIHCAAQgAQQDTIICAAQHhAWEAoyBggAEB4QFjIGCAAQHhAWMgYIABAeEBYyBggAEB4QFjIGCAAQHhAWOgoIABBHENYEELADOg0IABBHENYEELADEMkDOgQIABBDOgsIABCABBCxAxCDAToRCC4QgAQQsQMQgwEQxwEQ0QM6CAgAELEDEIMBOgsILhCABBCxAxCDAToLCC4QgAQQxwEQ0QM6CAguEIAEENQCOggIABCABBCxAzoLCC4QgAQQsQMQ1AI6BQgAEIAEOgcIABCxAxBDOggIABAeEA0QBUoECEEYAEoECEYYAFC0BFj8J2DsPmgBcAF4AIABSogB4wySAQIyOJgBAKABAcgBCMABAQ&sclient=gws-wiz (accessed on 16 September 2022).
- Kypri, E.; Ioannides, M.; Achilleos, A.; Koumbaris, G.; Patsalis, P.; Stumm, M. Non-invasive prenatal screening tests—Update. Lab. Med. 2022, 46, 311–320. [Google Scholar] [CrossRef]
- Kuo, P.L.; Guo, H.R. Nucleated red blood cells in maternal blood during pregnancy. Obstet. Gynecol. 1999, 94, 464–468. [Google Scholar]
- Zhang, Q.; Zhang, K.; Guo, Y.; Wei, X.; Sun, Y.; Cai, B.; Shi, Y.; Du, Y.; Liu, Y.; Fan, C.; et al. The isolation and analysis of fetal nucleated red blood cells using multifunctional microbeads with a nanostructured coating toward early noninvasive prenatal diagnostics. J. Mater. Chem. B 2021, 9, 3047–3054. [Google Scholar] [CrossRef]
- Cheng, L.; Wei, X.; Wang, Z.; Feng, C.; Gong, Q.; Fu, Y.; Zhao, X.; Zhang, Y. Silica microbeads capture fetal nucleated red blood cells for noninvasive prenatal testing of fetal ABO genotype. Electrophoresis 2020, 41, 966–972. [Google Scholar] [CrossRef]
- Seppo, A.; Frisova, V.; Ichetovkin, I.; Kim, Y.; Evans, M.I.; Antsaklis, A.; Nicolaides, K.H.; Tafas, T.; Tsipouras, P.; Kilpatrick, M.W. Detection of circulating fetal cells utilizing automated microscopy: Potential for noninvasive prenatal diagnosis of chromosomal aneuploidies. Prenat. Diagn. 2008, 28, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.J.; Qian, C.; Leshane, E.S.; Yu, K.F.; England, L.J.; Schisterman, E.F.; Wataganara, T.; Romero, R.; Bianchi, D.W. Two-stage elevation of cell-free fetal DNA in maternal sera before onset of preeclampsia. Am. J. Obstet. Gynecol. 2004, 190, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Liehr, T. Non-invasive prenatal testing, what patients do not learn, may be due to lack of specialist genetic training by gynecologists and obstetricians? Front. Genet. 2021, 12, 682980. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Lau, T.K.; Zhang, C.; Xu, C.; Xu, Z.; Hu, P.; Xu, J.; Huang, H.; Pan, L.; Jiang, F.; et al. A method for noninvasive detection of fetal large deletions/duplications by low coverage massively parallel sequencing. Prenat. Diagn. 2013, 33, 584–590. [Google Scholar] [CrossRef] [Green Version]
- Koumbaris, G.; Kypri, E.; Tsangaras, K.; Achilleos, A.; Mina, P.; Neofytou, M.; Velissariou, V.; Christopoulou, G.; Kallikas, I.; González-Liñán, A.; et al. Cell-free DNA analysis of targeted genomic regions in maternal plasma for non-invasive prenatal testing of trisomy 21, trisomy 18, trisomy 13, and fetal sex. Clin. Chem. 2016, 62, 848–855. [Google Scholar] [CrossRef] [Green Version]
- Dahl, F.; Ericsson, O.; Karlberg, O.; Karlsson, F.; Howell, M.; Persson, F.; Roos, F.; Stenberg, J.; Ahola, T.; Alftrén, I.; et al. Imaging single DNA molecules for high precision NIPT. Sci. Rep. 2018, 8, 4549. [Google Scholar] [CrossRef] [Green Version]
- Liehr, T. False-positives and false-negatives in non-invasive prenatal testing (NIPT): What can we learn from a meta-analyses on > 750,000 tests? Mol. Cytogenet. 2022, 15, 36. [Google Scholar] [CrossRef]
- Cortés-Martín, J.; Peñuela, N.L.; Sánchez-García, J.C.; Montiel-Troya, M.; Díaz-Rodríguez, L.; Rodríguez-Blanque, R. Deletion syndrome 22q11.2: A systematic review. Children 2022, 9, 1168. [Google Scholar] [CrossRef]
- Weise, A.; Mrasek, K.; Klein, E.; Mulatinho, M.; Llerena, J.C., Jr.; Hardekopf, D.; Pekova, S.; Bhatt, S.; Kosyakova, N.; Liehr, T. Microdeletion and microduplication syndromes. J. Histochem. Cytochem. 2012, 60, 346–358. [Google Scholar] [CrossRef] [Green Version]
- Zaninović, L.; Bašković, M.; Ježek, D.; Katušić Bojanac, A. Validity and utility of non-invasive prenatal testing for copy number variations and microdeletions: A systematic review. J. Clin. Med. 2022, 11, 3350. [Google Scholar] [CrossRef]
- Weise, A.; Liehr, T. Fluorescence in situ hybridization for prenatal screening of chromosomal aneuploidies. Expert Rev. Mol. Diagn. 2008, 8, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Vossaert, L.; Chakchouk, I.; Zemet, R.; Van den Veyver, I.B. Overview and recent developments in cell-based noninvasive prenatal testing. Prenat. Diagn. 2021, 41, 1202–1214. [Google Scholar] [CrossRef] [PubMed]
- Lewit-Mendes, M.F.; Robson, H.; Kelley, J.; Elliott, J.; Brown, E.; Menezes, M.; Archibald, A.D. Experiences of receiving an increased chance of sex chromosome aneuploidy result from non-invasive prenatal testing in Australia: “A more complicated scenario than what I had ever realized”. J. Genet. Couns. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Krafft, E. Geschäft mit der Falschen Sicherheit [Business with the Wrong Security]. 2020. Available online: https://www.pressreader.com/germany/ostthuringer-zeitung-stadtroda/20200831/282200833311280 (accessed on 16 September 2022).
- Lau, T.K.; Jiang, F.M.; Stevenson, R.J.; Lo, T.K.; Chan, L.W.; Chan, M.K.; Lo, P.S.; Wang, W.; Zhang, H.Y.; Chen, F.; et al. Secondary findings from non-invasive prenatal testing for common fetal aneuploidies by whole genome sequencing as a clinical service. Prenat. Diagn. 2013, 33, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Tolva, G.; Silipigni, R.; Quarenghi, A.; Vergani, P.; Guerneri, S.; Milani, D. Tetrasomy 18p: The challenges of noninvasive prenatal testing and combined test. J. Obstet. Gynaecol. Res. 2019, 45, 705–708. [Google Scholar] [CrossRef]
- Tamaki, Y.; Katagiri, Y.; Umemura, N.; Takeshita, N.; Morita, M. Noninvasive prenatal testing aids identification of tetrasomy 18p: A case report. Case Rep. Womens Health 2020, 27, e00236. [Google Scholar] [CrossRef]
- Zelig, C.M.; Knutzen, D.M.; Ennen, C.S.; Dolinsky, B.M.; Napolitano, P.G. Chorionic villus sampling, early amniocentesis, and termination of pregnancy without diagnostic testing: Comparison of fetal risk following positive non-invasive prenatal testing. J. Obstet. Gynaecol. Can. 2016, 38, 441–445. [Google Scholar] [CrossRef]
- Ohno, M.; Caughey, A. The role of noninvasive prenatal testing as a diagnostic versus a screening tool—A cost-effectiveness analysis. Prenat. Diagn. 2013, 33, 630–635. [Google Scholar] [CrossRef]
- Haidar, H.; Birko, S.; Laberge, A.M.; Le Clerc-Blain, J.; Ravitsky, V. Views of Canadian healthcare professionals on the future uses of non-invasive prenatal testing: A mixed method study. Eur. J. Hum. Genet. 2022, 30, 1269–1275. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, H.; Zhang, W.; Liu, K. Non-invasive prenatal testing for the detection of trisomy 13, 18, and 21 and sex chromosome aneuploidies in 68,763 cases. Front. Genet. 2022, 13, 864076. [Google Scholar] [CrossRef]
- D’Ambrosio, V.; Squarcella, A.; Vena, F.; Di Mascio, D.; Corno, S.; Pajno, C.; Piccioni, M.G.; Brunelli, R.; Pizzuti, A.; Benedetti Panici, P.; et al. Update in non-invasive prenatal testing. Minerva Ginecol. 2019, 71, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Elfmann, P. Wann Zahlt die Kasse den NIPT? (Translated: When Does the Health Insurance Pay for the NIPT? Available online: https://www.apotheken-umschau.de/familie/schwangerschaft/wann-zahlt-die-kasse-den-nipt-847907.html (accessed on 16 September 2022).
- Krankenkassen Zahlen für Trisomie-Test NIPT (Translated: Health Insurance Companies Pay for Trisomy Test NIPT). Available online: https://www.krankenkassen.de/gesetzliche-krankenkassen/leistungen-gesetzliche-krankenkassen/gesetzlich-vorgeschriebene-leistungen/neue-leistungen/nipt/ (accessed on 16 September 2022).
- Maternity Guidelines (Mutterschafts-Richtlinien). Available online: https://www.g-ba.de/downloads/62-492-1829/Mu-RL_2019-03-22_iK_2019-05-28.pdf (accessed on 16 September 2022).
- Rosenau, H.; Tönnies, H. Vierter Tätigkeitsbericht der Gendiagnostik-Kommission (Translated: Fourth Activity Report of the Gene Diagnostics Commission). Available online: https://www.rki.de/DE/Content/Kommissionen/GendiagnostikKommission/Taetigkeitsbericht/Taetigkeitsbericht_04.pdf?__blob=publicationFile (accessed on 16 September 2022).
- Gadsbøll, K.; Petersen, O.B.; Gatinois, V.; Strange, H.; Jacobsson, B.; Wapner, R.; Vermeesch, J.R.; NIPT-map Study Group; Vogel, I. Current use of noninvasive prenatal testing in Europe, Australia and the USA: A graphical presentation. Acta Obstet. Gynecol. Scand. 2020, 99, 722–730. [Google Scholar] [CrossRef] [PubMed]
- Hollands Steffensen, E.; Skakkebæk, A.; Gadsbøll, K.; Petersen, O.B.; Westover, T.; Strange, H.; NIPT-SCA-map study group; Vogel, I. Current coverage and reporting of sex chromosomes in noninvasive prenatal testing in Asia, Australia, Europe and the USA: A survey study. Prenat. Diagn. 2022, in press. [Google Scholar]
- Statistisches Bundesamt (Translation: Federal Office of Statistics Germany), Subpage “Anzahl der Schwangerschaftsabbrüche in Deutschland nach rechtlicher Begründung” (Translation: Number of Abortions in Germany Based on Legal Justification). Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Schwangerschaftsabbrueche/Tabellen/03-schwangerschaftsabbr-rechtliche-begruendung-schwangerschaftsdauer_zvab2012.html (accessed on 16 September 2022).
- Statistisches Bundesamt (Translation: Federal Office of Statistics Germany), Subpage “Bevölkerung und Erwerbstätigkeit, Zusammenfassende Übersichten Eheschließungen, Geborene und Gestorbene” (Translation: Population and Employment, Summary Overviews of Marriages, Births and Deaths). Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Eheschliessungen-Ehescheidungen-Lebenspartnerschaften/Publikationen/Downloads-Eheschliessungen/zusammen-eheschliessungen-geborene-gestorbene-5126102217004.pdf?__blob=publicationFile (accessed on 16 September 2022).
- Gesetz über Genetische Untersuchungen bei Menschen (Gendiagnostikgesetz–GenDG) (Translation: Gene Diagnostics Act). Available online: https://www.gesetze-im-internet.de/gendg/BJNR252900009.html (accessed on 16 September 2022).
- Schmitz, D. Ethische Herausforderungen der Neuen Nichtinvasiven Pränataltestung (Translation: Ethical Challenges of New Noninvasive Prenatal Testing). Gynäkologe 2016, 49, 442–447. [Google Scholar] [CrossRef]
- Kozlowski, P.; Burkhardt, T.; Gembruch, U.; Gonser, M.; Kähler, C.; Kagan, K.O.; von Kaisenberg, C.; Klaritsch, P.; Merz, E.; Steiner, H.; et al. Recommendations for the implementation of first-trimester screening, detailed ultrasound, cell-free DNA screening and diagnostic procedures. Ultraschall Med. 2019, 40, 176–193. [Google Scholar] [PubMed] [Green Version]
- Hessel, L.; Henn, W. Nichtinvasive Pränataltests—Fragwürdige Parameterauswahl (translation: Non-invasive prenatal testing—Questionable parameter selection). Dt. Ärztebl. 2022, 24, 1076–1077. [Google Scholar]
- Liehr, T.; Carreira, I.M.; Balogh, Z.; Garrido, E.D.; Verdorfer, I.; Coviello, D.A.; Florentin, L.; Scheffer, H.; Rincic, M.; Williams, H.E. Regarding the rights and duties of Clinical Laboratory Geneticists in genetic healthcare systems; results of a survey in over 50 countries. Eur. J. Hum. Genet. 2019, 27, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Zerres, K.; Scholz, C. “Genetische Beratung durch Nichtärzte?“—Ergebnisse einer GfH-Mitgliederumfrage (translation: “Genetic counseling by non-physicians?”—Results of a GfH member survey). Medgen 2013, 25, 295–308. [Google Scholar]
- Abgeordnetengruppe zur Pränataldiagnostik Hat Sich Konstituiert (Translation: Group of Deputies on Prenatal Diagnostics Has Been Constituted). Available online: https://www.aerzteblatt.de/nachrichten/136286/Abgeordnetengruppe-zur-Praenataldiagnostik-hat-sich-konstituiert?rt=4042379a9bb8e1c39b1230f00a2ec69a (accessed on 16 September 2022).
- Schwangerschaft: Weniger Frauen Nehmen Amniozentese in Anspruch (Translation: Pregnancy: Fewer Women Take Advantage of Amniocentesis). Dt. Ärztebl. 2019, 116, A1872.
- Richtlinie der Bundesärztekammer zur Qualitätssicherung Laboratoriumsmedizinischer Untersuchungen—Gemäß des Beschlusses des Vorstands der Bundesärztekammer in Seiner Sitzung am 18.10.2019 (Translation: Guideline of the German Medical Association for the Quality Assurance of Laboratory Medical Examinations—In Accordance with the Resolution of the Executive Board of the German Medical Association at Its Meeting on 18.10.2019) Deutsches Ärzteblatt. Available online: https://www.aerzteblatt.de/down.asp?id=27352 (accessed on 16 September 2022).

| Type of Test | Invasive | |
|---|---|---|
| Can be Carried out from w.o.g.: | Is the Fetus Studied? | |
| (cyto)genetics from CVS | ~11 | No |
| (cyto)genetics from AC | ~14 | Yes |
| (cyto)genetics from UCB | ~20 | Yes |
| Type of test | Non-invasive | |
| Can be carried out from w.o.g.: | Is the fetus studied? | |
| Early sonography | ~6 | (Yes) 1 |
| Late fine sonography | ~19 | (Yes) 1 |
| First trimester-screening (FTS) | 11–14 | (No) 2 |
| Tests for protein markers (e.g., alpha fetoprotein, etc.) from maternal blood serum | ~11 | No |
| Non-invasive prenatal testing (NIPT) from free placenta-derived DNA in maternal blood serum | ~10 | No |
| Molecular genetic/molecular cytogenetic tests on fetal nucleated erythrocytes from maternal blood | before 10 | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liehr, T.; Harutyunyan, T.; Williams, H.; Weise, A. Non-Invasive Prenatal Testing in Germany. Diagnostics 2022, 12, 2816. https://doi.org/10.3390/diagnostics12112816
Liehr T, Harutyunyan T, Williams H, Weise A. Non-Invasive Prenatal Testing in Germany. Diagnostics. 2022; 12(11):2816. https://doi.org/10.3390/diagnostics12112816
Chicago/Turabian StyleLiehr, Thomas, Tigran Harutyunyan, Heather Williams, and Anja Weise. 2022. "Non-Invasive Prenatal Testing in Germany" Diagnostics 12, no. 11: 2816. https://doi.org/10.3390/diagnostics12112816