
Outcome Measures and Biomarkers for Disease Assessment in Takayasu Arteritis
 , , and
, , and
Abstract
:1. Introduction
2. Clinical Assessment of Disease Activity and Damage
2.1. Disease Activity
2.1.1. NIH Score
2.1.2. DEI.TAK
2.1.3. ITAS2010
2.1.4. Other Criteria for the Assessment of TAK Disease Activity
2.2. Damage
2.2.1. Vasculitis Damage Index
2.2.2. Takayasu Arteritis Damage Score
2.3. Patient-Reported Outcome Measures
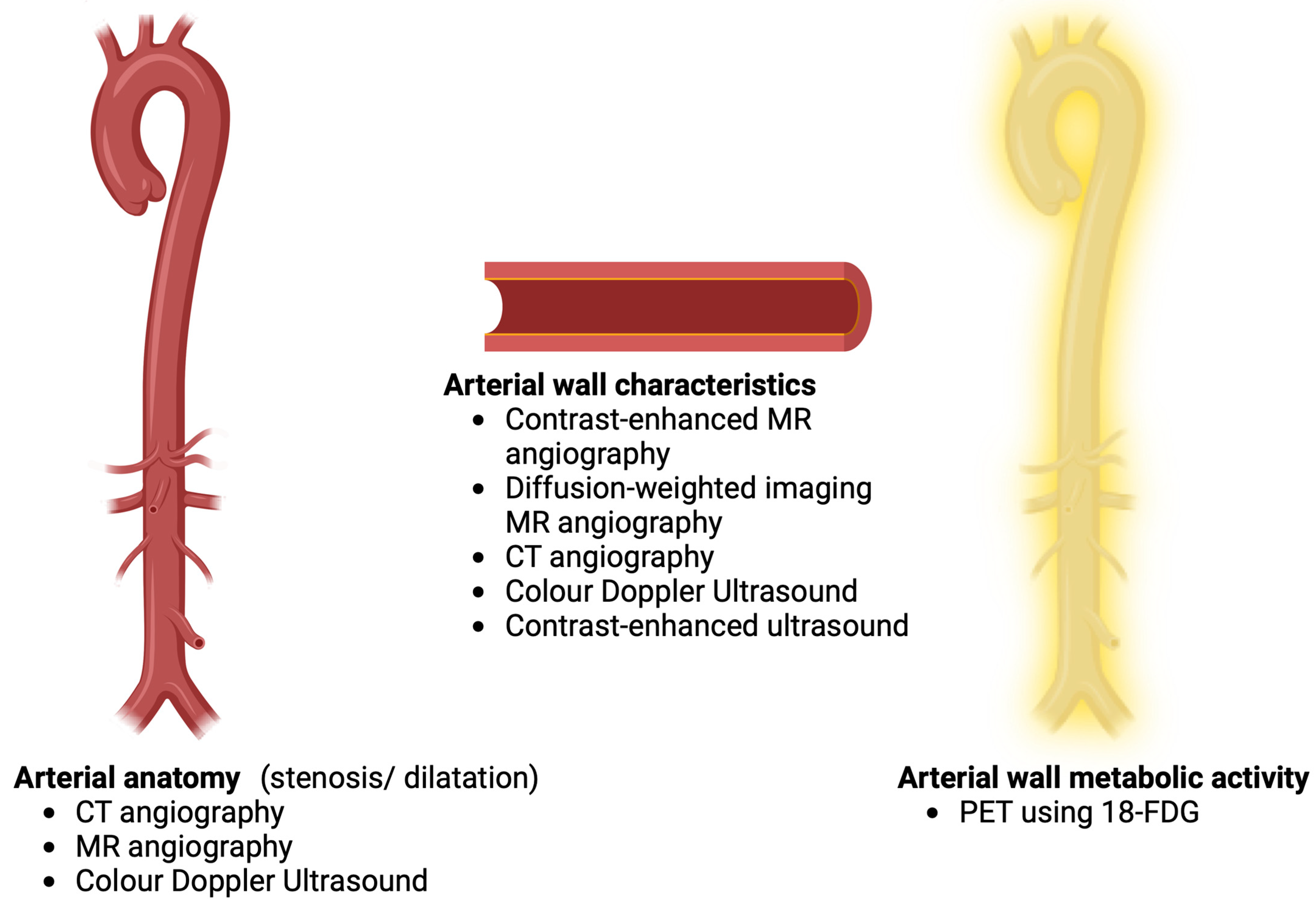
3. Angiographic and Imaging Outcomes in TAK
3.1. CT Angiography
3.2. MR Angiography
3.3. Angiographic Scoring Systems
3.4. Color Doppler Ultrasound
3.5. PET-CT and PET-MRI
4. Circulating Biomarkers of Disease Activity in TAK
4.1. ESR
4.2. Pentraxins
4.2.1. C-Reactive Protein
4.2.2. Pentraxin-3
4.3. Biomarkers Derived from Routine Hemogram Reports
4.4. Cell Populations in the Peripheral Blood and Their Related Trophic Factors
4.5. Cytokines
4.6. Autoantibodies
4.7. Markers of Endothelial Injury
4.8. Matrix Metalloproteinases
4.9. Other Biomarkers of Disease Activity in TAK
4.10. Circulating Proteomic Signatures
4.11. Serum Metabolomic Signatures
4.12. Circulating Markers of Vascular Damage
5. Composite Scoring Systems Involving Clinical Assessment, Radiologic Findings, and Circulating Biomarkers
6. Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAV | ANCA-associated vasculitis |
| ACS | Angiographic Composite Score |
| ADS | Angiographic Dilatation Score |
| AGATA | Abatacept in Giant Cell Arteritis and Takayasu arteritis |
| ANCA | Antineutrophil cytoplasmic antibody |
| APRs | Acute phase reactants |
| ASS | Angiographic Stenosis Score |
| AUC | Area under the curve |
| BVAS | Birmingham Vasculitis Activity Score |
| CA125 | Cancer antigen 125 |
| CA15-3 | Cancer antigen 15-3 |
| CARDS | Combined Arteritis Damage Score |
| CCL | Chemokine (C-C motif) ligand |
| CDUS | Colour Doppler ultrasound |
| CDUS-K | Colour Doppler ultrasound in Takayasu arteritis score from Kolkata |
| CDA | Combined Damage Assessment Index |
| CECs | Circulating endothelial cells |
| CEMRA | Contrast-enhanced MRA |
| CRP | C-reactive protein |
| CTA | Computerized tomographic angiography |
| C4BP | C4 binding protein |
| DEI.TAK | Disease Extent Index in TAK |
| DMARDs | Disease-modifying anti-rheumatic drugs |
| DSA | Digital subtraction angiography |
| EPCs | Endothelial progenitor cells |
| ESR | Erythrocyte sedimentation rate |
| EULAR | European Alliance of Associations for Rheumatology |
| FAPI | Fibroblast Activator Protein Inhibitor |
| 18-FDG | 18-fluorodeoxyglucose |
| GCA | Giant cell arteritis |
| GFR | Glomerular filtration rate |
| GROα | Growth-regulated oncogene α |
| IGFBP-2 | Insulin like growth factor binding protein 2 |
| IL | Interleukin |
| ICAM-1 | Intercellular adhesion molecule 1 |
| ITAS | Indian TAK Clinical Activity Score |
| LVV | Large vessel vasculitis |
| LYVE-1 | Lymphatic vessel endothelial hyaluronan receptor 1 |
| MRA | Magnetic resonance angiography |
| MMPs | Matrix metalloproteinases |
| MRP 8/14 | Myeloid-related protein 8/14 |
| NLR | Neutrophil-to-lymphocyte ratio |
| PAAT | Periaortic adipose tissue |
| PCAT | Pericoronary adipose tissue |
| PETVAS | PET vascular activity score |
| PET-CT | Positron emission tomography computerized tomography |
| PET-MRI | PET-magnetic resonance imaging |
| PGA | Physician global assessment |
| PLR | Platelet-to-lymphocyte ratio |
| PROMs | Patient-reported outcome measures |
| PTX-3 | Pentraxin-related protein |
| RAG-1 | Recombination activating gene 1 |
| RCTs | Randomized controlled trials |
| RDW | Red cell distribution width |
| SAA | Serum amyloid A |
| SAP | Serum amyloid P |
| SNPs | Single nucleotide polymorphisms |
| SST2 | Somatostatin receptor subtype 2 |
| SUVmax | Maximum standardized uptake values |
| SUVmean | Mean standardized uptake values |
| TADS | Takayasu Arteritis Damage Score |
| TAK | Takayasu arteritis |
| TBR | Target-to-blood pool ratio |
| TNF | Tumor necrosis factor |
| TIMP-1 | Tissue inhibitor of metalloproteinases 1 |
| VCAM-1 | Vascular cell adhesion molecule 1 |
| VDI | Vasculitis Damage Index |
| VEGF | Vascular endothelial growth factor |
References
- Misra, D.P.; Wakhlu, A.; Agarwal, V.; Danda, D. Recent advances in the management of Takayasu arteritis. Int. J. Rheum. Dis. 2019, 22 (Suppl. 1), 60–68. [Google Scholar] [CrossRef]
- Pugh, D.; Karabayas, M.; Basu, N.; Cid, M.C.; Goel, R.; Goodyear, C.S.; Grayson, P.C.; McAdoo, S.P.; Mason, J.C.; Owen, C.; et al. Large-vessel vasculitis. Nat. Rev. Dis. Primers 2022, 7, 93. [Google Scholar] [CrossRef]
- Arnaud, L.; Haroche, J.; Mathian, A.; Gorochov, G.; Amoura, Z. Pathogenesis of Takayasu’s arteritis: A 2011 update. Autoimmun. Rev. 2011, 11, 61–67. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Direskeneli, H.; Merkel, P.A. Assessment of Disease Activity in Large-vessel Vasculitis: Results of an International Delphi Exercise. J. Rheumatol. 2017, 44, 1928–1932. [Google Scholar] [CrossRef] [Green Version]
- Kerr, G.S.; Hallahan, C.W.; Giordano, J.; Leavitt, R.Y.; Fauci, A.S.; Rottem, M.; Hoffman, G.S. Takayasu arteritis. Ann. Intern. Med. 1994, 120, 919–929. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Yilmaz, N.; Akar, S.; Aksu, K.; Kamali, S.; Yucel, E.; Karadag, O.; Bicakcigil, M.; Ozer, H.; Kiraz, S.; et al. Assessment of disease activity and progression in Takayasu’s arteritis with Disease Extent Index-Takayasu. Rheumatology 2010, 49, 1889–1893. [Google Scholar] [CrossRef] [Green Version]
- Misra, R.; Danda, D.; Rajappa, S.M.; Ghosh, A.; Gupta, R.; Mahendranath, K.M.; Jeyaseelan, L.; Lawrence, A.; Bacon, P.A. Development and initial validation of the Indian Takayasu Clinical Activity Score (ITAS2010). Rheumatology 2013, 52, 1795–1801. [Google Scholar] [CrossRef] [Green Version]
- Langford, C.A.; Cuthbertson, D.; Ytterberg, S.R.; Khalidi, N.; Monach, P.A.; Carette, S.; Seo, P.; Moreland, L.W.; Weisman, M.; Koening, C.L.; et al. A Randomized, Double-Blind Trial of Abatacept (CTLA-4Ig) for the Treatment of Takayasu Arteritis. Arthritis Rheumatol. 2017, 69, 846–853. [Google Scholar] [CrossRef] [Green Version]
- Siemons, L.; Ten Klooster, P.M.; Vonkeman, H.E.; van Riel, P.L.; Glas, C.A.; van de Laar, M.A. How age and sex affect the erythrocyte sedimentation rate and C-reactive protein in early rheumatoid arthritis. BMC Musculoskelet. Disord. 2014, 15, 368. [Google Scholar] [CrossRef] [Green Version]
- Goel, R.; Kumar, T.S.; Danda, D.; Joseph, G.; Jeyaseelan, V.; Surin, A.K.; Bacon, P. Childhood-onset Takayasu arteritis—Experience from a tertiary care center in South India. J. Rheumatol. 2014, 41, 1183–1189. [Google Scholar] [CrossRef]
- Luqmani, R.A.; Bacon, P.A.; Moots, R.J.; Janssen, B.A.; Pall, A.; Emery, P.; Savage, C.; Adu, D. Birmingham Vasculitis Activity Score (BVAS) in systemic necrotizing vasculitis. QJM Int. J. Med. 1994, 87, 671–678. [Google Scholar]
- Misra, D.P.; Chowdhury, A.C.; Lal, H.; Mohindra, N.; Agarwal, V. Gangrene in Takayasu’s arteritis: A report of two cases and review of literature. Rheumatol. Int. 2016, 36, 449–453. [Google Scholar] [CrossRef]
- Alibaz-Oner, F.; Aydin, S.Z.; Akar, S.; Aksu, K.; Kamali, S.; Yucel, E.; Karadag, O.; Ozer, H.; Kiraz, S.; Onen, F.; et al. Assessment of Patients with Takayasu Arteritis in Routine Practice with Indian Takayasu Clinical Activity Score. J. Rheumatol. 2015, 42, 1443–1447. [Google Scholar] [CrossRef] [Green Version]
- Kenar, G.; Karaman, S.; Çetin, P.; Yarkan, H.; Akar, S.; Can, G.; Alataş, Ö.; Gülcü, A.; Önen, F. Imaging is the major determinant in the assessment of disease activity in Takayasu’s arteritis. Clin. Exp. Rheumatol. 2020, 38 (Suppl. 124), 55–60. [Google Scholar]
- Misra, D.P.; Rathore, U.; Patro, P.; Agarwal, V.; Sharma, A. Disease-modifying anti-rheumatic drugs for the management of Takayasu arteritis—A systematic review and meta-analysis. Clin. Rheumatol. 2021, 40, 4391–4416. [Google Scholar] [CrossRef]
- Dabague, J.; Reyes, P.A. Takayasu arteritis in Mexico: A 38-year clinical perspective through literature review. Int. J. Cardiol. 1996, 54, S103–S109. [Google Scholar] [CrossRef]
- Hellmich, B.; Agueda, A.; Monti, S.; Buttgereit, F.; de Boysson, H.; Brouwer, E.; Cassie, R.; Cid, M.C.; Dasgupta, B.; Dejaco, C.; et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann. Rheum. Dis. 2020, 79, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Nakaoka, Y.; Isobe, M.; Takei, S.; Tanaka, Y.; Ishii, T.; Yokota, S.; Nomura, A.; Yoshida, S.; Nishimoto, N. Efficacy and safety of tocilizumab in patients with refractory Takayasu arteritis: Results from a randomised, double-blind, placebo-controlled, phase 3 trial in Japan (the TAKT study). Ann. Rheum. Dis. 2018, 77, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Exley, A.R.; Bacon, P.A.; Luqmani, R.A.; Kitas, G.D.; Gordon, C.; Savage, C.O.; Adu, D. Development and initial validation of the Vasculitis Damage Index for the standardized clinical assessment of damage in the systemic vasculitides. Arthritis Rheum. 1997, 40, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Kaymaz-Tahra, S.; Alibaz-Oner, F.; Direskeneli, H. Assessment of damage in Takayasu’s arteritis. Semin. Arthritis Rheum. 2020, 50, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Aeschlimann, F.A.; Barra, L.; Alsolaimani, R.; Benseler, S.M.; Hebert, D.; Khalidi, N.; Laxer, R.M.; Noone, D.; Pagnoux, C.; Twilt, M.; et al. Presentation and Disease Course of Childhood-Onset Versus Adult-Onset Takayasu Arteritis. Arthritis Rheumatol. 2019, 71, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Dolezalova, P.; Wilkinson, N.; Brogan, P.A.; Anton, J.; Benseler, S.M.; Brunner, J.; Cabral, D.A.; Cimaz, R.; Neil, K.M.; Özen, S.; et al. SAT0286 Paediatric Vasculitis Damage Index: A New Tool for Standardised Disease Assessment. Ann. Rheum Dis. 2014, 73, 696. [Google Scholar] [CrossRef]
- Seo, P.; Luqmani, R.A.; Flossmann, O.; Hellmich, B.; Herlyn, K.; Hoffman, G.S.; Jayne, D.; Kallenberg, C.G.; Langford, C.A.; Mahr, A.; et al. The future of damage assessment in vasculitis. J. Rheumatol. 2007, 34, 1357–1371. [Google Scholar] [PubMed]
- Nakagomi, D.; Cousins, C.; Sznajd, J.; Furuta, S.; Mohammad, A.J.; Luqmani, R.; Jayne, D. Development of a score for assessment of radiologic damage in large-vessel vasculitis (Combined Arteritis Damage Score, CARDS). Clin. Exp. Rheumatol. 2017, 35 (Suppl. 103), 139–145. [Google Scholar] [PubMed]
- Mehta, P.; Gupta, L.; Muhammed, H.; Misra, D.P.; Lawrence, A.; Agarwal, V.; Aggarwal, A.; Misra, R. Spectrum of Myelitis in Systemic Lupus Erythematosus: Experience from a Single Tertiary Care Centre over 25 Years. Mediterr. J. Rheumatol. 2021, 32, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Shu, J.; Gu, C.; Ren, Y.; Wei, W. ANCA-Associated Hypertrophic Spinal Pachymeningitis Presenting with Longitudinally Extensive Transverse Myelitis: A Case Report. Ann. Indian Acad. Neurol. 2020, 23, 131–132. [Google Scholar] [CrossRef]
- Jennette, J.C.; Falk, R.J.; Bacon, P.A.; Basu, N.; Cid, M.C.; Ferrario, F.; Flores-Suarez, L.F.; Gross, W.L.; Guillevin, L.; Hagen, E.C.; et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013, 65, 1–11. [Google Scholar] [CrossRef]
- Misra, D.P.; Rathore, U.; Patro, P.; Agarwal, V.; Sharma, A. Corticosteroid monotherapy for the management of Takayasu arteritis-a systematic review and meta-analysis. Rheumatol. Int. 2021, 41, 1729–1742. [Google Scholar] [CrossRef]
- Misra, D.P.; Rathore, U.; Patro, P.; Agarwal, V.; Sharma, A. Patient-Reported Outcome Measures in Takayasu Arteritis: A Systematic Review and Meta-Analysis. Rheumatol. Ther. 2021, 8, 1073–1093. [Google Scholar] [CrossRef]
- Sreih, A.G.; Alibaz-Oner, F.; Easley, E.; Davis, T.; Mumcu, G.; Milman, N.; Robson, J.; Direskeneli, H.; Merkel, P.A.; Cronholm, P. Health-related outcomes of importance to patients with Takayasu’s arteritis. Clin. Exp. Rheumatol. 2018, 36 (Suppl. 111), 51–57. [Google Scholar]
- Misra, D.P.; Sharma, A.; Kadhiravan, T.; Negi, V.S. A scoping review of the use of non-biologic disease modifying anti-rheumatic drugs in the management of large vessel vasculitis. Autoimmun. Rev. 2017, 16, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Barra, L.; Kanji, T.; Malette, J.; Pagnoux, C. Imaging modalities for the diagnosis and disease activity assessment of Takayasu’s arteritis: A systematic review and meta-analysis. Autoimmun. Rev. 2018, 17, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Park, J.H.; Chung, J.W.; Kim, H.C.; Lee, W.; So, Y.H.; Jae, H.J. Follow-up CT evaluation of the mural changes in active Takayasu arteritis. Korean J. Radiol. 2007, 8, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.P.; Luo, S.; Wang, Z.J.; Jin, Z.Y.; Zhang, L.J.; Lu, G.M. Takayasu arteritis: Imaging spectrum at multidetector CT angiography. Br. J. Radiol. 2012, 85, e1282–e1292. [Google Scholar] [CrossRef] [Green Version]
- Meléndez-Ramírez, G.; Soto, M.E.; Meave, A.; Ruiz-Elizondo, L.A.; Kimura, E.; Alexanderson, E. Aortic Calcification in Takayasu Arteritis: Risk Factors and Relationship With Activity and Vascular Lesion. It Is Not Only an Aging Question. J. Clin. Rheumatol. 2021, 27, S265–S273. [Google Scholar] [CrossRef]
- Wall, C.; Huang, Y.; Le, E.P.V.; Ćorović, A.; Uy, C.P.; Gopalan, D.; Ma, C.; Manavaki, R.; Fryer, T.D.; Aloj, L.; et al. Pericoronary and periaortic adipose tissue density are associated with inflammatory disease activity in Takayasu arteritis and atherosclerosis. Eur. Heart J. Open 2021, 1, oeab019. [Google Scholar] [CrossRef]
- Campochiaro, C.; Misra, D.P. PET in Takayasu arteritis: Onwards and upwards towards a future of robust multimodality disease activity assessment? Rheumatology 2021, 61, SI4–SI5. [Google Scholar] [CrossRef]
- Spira, D.; Xenitidis, T.; Henes, J.; Horger, M. MRI parametric monitoring of biological therapies in primary large vessel vasculitides: A pilot study. Br. J. Radiol. 2016, 89, 20150892. [Google Scholar] [CrossRef]
- Garg, S.K.; Mohan, S.; Kumar, S. Diagnostic value of 3D contrast-enhanced magnetic resonance angiography in Takayasu’s arteritis—A comparative study with digital subtraction angiography. Eur. Radiol. 2011, 21, 1658–1666. [Google Scholar] [CrossRef]
- John, R.A.; Keshava, S.N.; Danda, D. Correlating MRI with clinical evaluation in the assessment of disease activity of Takayasu’s arteritis. Int. J. Rheum. Dis. 2017, 20, 882–886. [Google Scholar] [CrossRef]
- Jiang, L.; Li, D.; Yan, F.; Dai, X.; Li, Y.; Ma, L. Evaluation of Takayasu arteritis activity by delayed contrast-enhanced magnetic resonance imaging. Int. J. Cardiol. 2012, 155, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ma, L.; Ji, Z.; Zhang, Z.; Chen, H.; Liu, H.; Shan, Y.; Yan, F.; Jiang, L. Value of whole-body contrast-enhanced magnetic resonance angiography with vessel wall imaging in quantitative assessment of disease activity and follow-up examination in Takayasu’s arteritis. Clin. Rheumatol. 2016, 35, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Pan, L.; Liu, J.; Li, Y.; Xu, L.; Sun, Z.; Wang, Z. Comparison of Different Thoracic Aortic Wall Characteristics for Assessment of Disease Activity in Takayasu Arteritis: A Quantitative Study with 3.0 T Magnetic Resonance Imaging. Rev. Cardiovasc. Med. 2022, 23, 92. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Liu, W.; Li, H.; Shu, X.; Tao, X.; Zhai, Z. Evaluation of takayasu arteritis with delayed contrast-enhanced MR imaging by a free-breathing 3D IR turbo FLASH. Medicine 2017, 96, e9284. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.H.; Tian, X.P.; Wang, H.Y.; Li, J.; Ge, Z.T.; Yang, Y.J.; Cai, S.; Zeng, X.F.; Li, J.C. Contrast-enhanced ultrasound for evaluating arteritis activity in Takayasu arteritis patients. Clin. Rheumatol. 2020, 39, 1229–1235. [Google Scholar] [CrossRef]
- Tombetti, E.; Godi, C.; Ambrosi, A.; Doyle, F.; Jacobs, A.; Kiprianos, A.P.; Youngstein, T.; Bechman, K.; Manfredi, A.A.; Ariff, B.; et al. Novel Angiographic Scores for evaluation of Large Vessel Vasculitis. Sci. Rep. 2018, 8, 15979. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, C.; Rance, A.; Paul, J.F.; Beguin, C.; Bletry, O.; Amoura, Z.; Piette, J.C.; Fiessinger, J.N. The role of B-mode ultrasonography and electron beam computed tomography in evaluation of Takayasu’s arteritis: A study of 43 patients. Semin. Arthritis Rheum. 2000, 30, 25–32. [Google Scholar] [CrossRef]
- Dasgupta, B.; Smith, K.; Khan, A.A.S.; Coath, F.; Wakefield, R.J. ‘Slope sign’: A feature of large vessel vasculitis? Ann. Rheum. Dis. 2019, 78, 1738. [Google Scholar] [CrossRef]
- Milchert, M.; Brzosko, M.; Bull Haaversen, A.; Diamantopoulos, A.P. Correspondence to ‘Slope sign’: A feature of large vessel vasculitis? Ann. Rheum. Dis. 2021, 80, e198. [Google Scholar] [CrossRef] [Green Version]
- Sebastian, A.; Kayani, A.; Dasgupta, B. Response to: ‘Correspondence to ‘Slope sign’: A feature of large vessel vasculitis?’ by Milchert et al. Ann. Rheum. Dis. 2021, 80, e199. [Google Scholar] [CrossRef] [Green Version]
- Sinha, D.; Mondal, S.; Nag, A.; Ghosh, A. Development of a colour Doppler ultrasound scoring system in patients of Takayasu’s arteritis and its correlation with clinical activity score (ITAS 2010). Rheumatology 2013, 52, 2196–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Geest, K.S.M.; Borg, F.; Kayani, A.; Paap, D.; Gondo, P.; Schmidt, W.; Luqmani, R.A.; Dasgupta, B. Novel ultrasonographic Halo Score for giant cell arteritis: Assessment of diagnostic accuracy and association with ocular ischaemia. Ann. Rheum. Dis. 2020, 79, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathore, U.; Thakare, D.R.; Patro, P.; Agarwal, V.; Sharma, A.; Misra, D.P. A systematic review of clinical and preclinical evidences for Janus kinase inhibitors in large vessel vasculitis. Clin. Rheumatol. 2022, 41, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Giordana, P.; Baqué-Juston, M.C.; Jeandel, P.Y.; Mondot, L.; Hirlemann, J.; Padovani, B.; Raffaelli, C. Contrast-enhanced ultrasound of carotid artery wall in Takayasu disease: First evidence of application in diagnosis and monitoring of response to treatment. Circulation 2011, 124, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Schinkel, A.F.; van den Oord, S.C.; van der Steen, A.F.; van Laar, J.A.; Sijbrands, E.J. Utility of contrast-enhanced ultrasound for the assessment of the carotid artery wall in patients with Takayasu or giant cell arteritis. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 541–546. [Google Scholar] [CrossRef] [Green Version]
- Lottspeich, C.; Dechant, C.; Köhler, A.; Tischler, M.; Treitl, K.M.; Treitl, M.; Schulze-Koops, H.; Hoffmann, U.; Czihal, M. Assessment of Disease Activity in Takayasu Arteritis: Potential Role of Contrast-Enhanced Ultrasound. Ultraschall Med. 2019, 40, 638–645. [Google Scholar] [CrossRef]
- Germanò, G.; Macchioni, P.; Possemato, N.; Boiardi, L.; Nicolini, A.; Casali, M.; Versari, A.; Pipitone, N.; Salvarani, C. Contrast-Enhanced Ultrasound of the Carotid Artery in Patients With Large Vessel Vasculitis: Correlation With Positron Emission Tomography Findings. Arthritis Care Res. 2017, 69, 143–149. [Google Scholar] [CrossRef]
- Li, Z.; Zheng, Z.; Ding, J.; Li, X.; Zhao, Y.; Kang, F.; Li, Y.; Pang, L.; Du, W.; Wu, Z.; et al. Contrast-enhanced Ultrasonography for Monitoring Arterial Inflammation in Takayasu Arteritis. J. Rheumatol. 2019, 46, 616–622. [Google Scholar] [CrossRef]
- Ma, L.Y.; Li, C.L.; Ma, L.L.; Cui, X.M.; Dai, X.M.; Sun, Y.; Chen, H.Y.; Huang, B.J.; Jiang, L.D. Value of contrast-enhanced ultrasonography of the carotid artery for evaluating disease activity in Takayasu arteritis. Arthritis Res. Ther. 2019, 21, 24. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Ma, X.; Li, M.; Dong, H.; Wan, Y.; Zhu, J. Carotid contrast-enhanced ultrasonographic assessment of disease activity in Takayasu arteritis. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 789–795. [Google Scholar] [CrossRef]
- Slart, R.H.J.A.; Glaudemans, A.W.J.M.; Chareonthaitawee, P.; Treglia, G.; Besson, F.L.; Bley, T.A.; Blockmans, D.; Boellaard, R.; Bucerius, J.; Carril, J.M.; et al. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: Joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1250–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grayson, P.C.; Alehashemi, S.; Bagheri, A.A.; Civelek, A.C.; Cupps, T.R.; Kaplan, M.J.; Malayeri, A.A.; Merkel, P.A.; Novakovich, E.; Bluemke, D.A.; et al. 18F-Fluorodeoxyglucose-Positron Emission Tomography As an Imaging Biomarker in a Prospective, Longitudinal Cohort of Patients With Large Vessel Vasculitis. Arthritis Rheumatol. 2018, 70, 439–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tezuka, D.; Haraguchi, G.; Ishihara, T.; Ohigashi, H.; Inagaki, H.; Suzuki, J.; Hirao, K.; Isobe, M. Role of FDG PET-CT in Takayasu arteritis: Sensitive detection of recurrences. JACC Cardiovasc. Imaging 2012, 5, 422–429. [Google Scholar] [CrossRef]
- Santhosh, S.; Mittal, B.R.; Gayana, S.; Bhattacharya, A.; Sharma, A.; Jain, S. F-18 FDG PET/CT in the evaluation of Takayasu arteritis: An experience from the tropics. J. Nucl. Cardiol. 2014, 21, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Alibaz-Oner, F.; Dede, F.; Ones, T.; Turoglu, H.T.; Direskeneli, H. Patients with Takayasu’s arteritis having persistent acute-phase response usually have an increased major vessel uptake by 18F-FDG-PET/CT. Mod. Rheumatol. 2015, 25, 752–755. [Google Scholar] [CrossRef]
- De Souza Santos, M.P.; Ramos, C.D.; Paixão, M.; Pignaton Naseri, E.; Barros Bertolo, M.; Sachetto, Z. 18F-FDG PET/CT in Late Acquisition Identifies Sites of Active Disease in Treated Takayasu Arteritis. J. Clin. Rheumatol. 2022, 28, 14–20. [Google Scholar] [CrossRef]
- Banerjee, S.; Quinn, K.A.; Gribbons, K.B.; Rosenblum, J.S.; Civelek, A.C.; Novakovich, E.; Merkel, P.A.; Ahlman, M.A.; Grayson, P.C. Effect of Treatment on Imaging, Clinical, and Serologic Assessments of Disease Activity in Large-vessel Vasculitis. J. Rheumatol. 2020, 47, 99–107. [Google Scholar] [CrossRef]
- Alessi, H.D.; Quinn, K.A.; Ahlman, M.A.; Novakovich, E.; Saboury, B.; Luo, Y.; Grayson, P.C. Longitudinal Characterization of Vascular Inflammation and Disease Activity in Takayasu’s Arteritis and Giant Cell Arteritis: A single-center prospective study. Arthritis Care Res. 2022. [CrossRef]
- Dashora, H.R.; Rosenblum, J.S.; Quinn, K.A.; Alessi, H.; Novakovich, E.; Saboury, B.; Ahlman, M.A.; Grayson, P.C. Comparing Semiquantitative and Qualitative Methods of Vascular (18)F-FDG PET Activity Measurement in Large-Vessel Vasculitis. J. Nucl. Med. 2022, 63, 280–286. [Google Scholar] [CrossRef]
- Galli, E.; Muratore, F.; Mancuso, P.; Boiardi, L.; Marvisi, C.; Besutti, G.; Spaggiari, L.; Casali, M.; Versari, A.; Giorgi Rossi, P.; et al. The role of PET/CT in disease activity assessment in patients with large vessel vasculitis. Rheumatology 2022, keac125. [Google Scholar] [CrossRef]
- Youngstein, T.; Tombetti, E.; Mukherjee, J.; Barwick, T.D.; Al-Nahhas, A.; Humphreys, E.; Nash, J.; Andrews, J.; Incerti, E.; Tombolini, E.; et al. FDG Uptake by Prosthetic Arterial Grafts in Large Vessel Vasculitis Is Not Specific for Active Disease. JACC Cardiovasc. Imaging 2017, 10, 1042–1052. [Google Scholar] [CrossRef] [PubMed]
- Incerti, E.; Tombetti, E.; Fallanca, F.; Baldissera, E.M.; Alongi, P.; Tombolini, E.; Sartorelli, S.; Sabbadini, M.G.; Papa, M.; De Cobelli, F.; et al. 18F-FDG PET reveals unique features of large vessel inflammation in patients with Takayasu’s arteritis. Eur. J. Nucl. Med. Mol. Imaging. 2017, 44, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Van der Geest, K.S.M.; Treglia, G.; Glaudemans, A.; Brouwer, E.; Sandovici, M.; Jamar, F.; Gheysens, O.; Slart, R. Diagnostic value of [18F]FDG-PET/CT for treatment monitoring in large vessel vasculitis: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging. 2021, 48, 3886–3902. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.C.; Jeon, T.J.; Park, M.C. Vascular Uptake on 18F-FDG PET/CT During the Clinically Inactive State of Takayasu Arteritis Is Associated with a Higher Risk of Relapse. Ynsei Med. J. 2021, 62, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Janes, A.L.F.; Castro, M.F.; Arraes, A.E.D.; Savioli, B.; Sato, E.I.; de Souza, A.W.S. A retrospective cohort study to assess PET-CT findings and clinical outcomes in Takayasu arteritis: Does 18F-fluorodeoxyglucose uptake in arteries predict relapses? Rheumatol. Int. 2020, 40, 1123–1131. [Google Scholar] [CrossRef]
- Fan, J.; Wei, D.; Zhang, H.; Sun, X.; Cai, J.; Fan, L.; Yu, J.; Ma, W.; Song, L.; Zhou, X. 18F-FDG PET/CT plays a unique role in the management of Takayasu arteritis patients with atypical manifestations. Clin. Rheumatol. 2021, 40, 625–633. [Google Scholar] [CrossRef]
- Gao, W.; Gong, J.N.; Guo, X.J.; Wu, J.Y.; Xi, X.Y.; Ma, Z.H.; Yang, Y.H.; Yang, M.F. Value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in the evaluation of pulmonary artery activity in patients with Takayasu’s arteritis. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 541–550. [Google Scholar] [CrossRef]
- Wu, S.; Pang, Y.; Zhao, L.; Zhao, L.; Chen, H. 68Ga-FAPI PET/CT Versus 18F-FDG PET/CT for the Evaluation of Disease Activity in Takayasu Arteritis. Clin. Nucl. Med. 2021, 46, 847–849. [Google Scholar] [CrossRef]
- Tarkin, J.M.; Wall, C.; Gopalan, D.; Aloj, L.; Manavaki, R.; Fryer, T.D.; Aboagye, E.O.; Bennett, M.R.; Peters, J.E.; Rudd, J.H.F.; et al. Novel Approach to Imaging Active Takayasu Arteritis Using Somatostatin Receptor Positron Emission Tomography/Magnetic Resonance Imaging. Circ. Cardiovasc. Imaging 2020, 13, e010389. [Google Scholar] [CrossRef]
- Quinn, K.A.; Alessi, H.; Ponte, C.; Rose, E.; Ahlman, M.A.; Redmond, C.; Luo, Y.; Bolek, E.C.; Langford, C.A.; Merkel, P.A.; et al. Use of 18F-fluorodeoxyglucose Positron Emission Tomography to Standardize Clinical Trial Recruitment in Takayasu’s Arteritis. Rheumatology 2022, 61, 4047–4055. [Google Scholar] [CrossRef]
- Laurent, C.; Ricard, L.; Fain, O.; Buvat, I.; Adedjouma, A.; Soussan, M.; Mekinian, A. PET/MRI in large-vessel vasculitis: Clinical value for diagnosis and assessment of disease activity. Sci. Rep. 2019, 9, 12388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerne, J.W.; Liu, S.; Umair, M.; Pathrose, A.; Moore, J.E.; Allen, B.D.; Markl, M.; Carr, J.C.; Savas, H.; Wilsbacher, L.; et al. Combined modality PET/MR for the detection of severe large vessel vasculitis. Eur. J. Hybrid. Imaging 2022, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Clemente, G.; de Souza, A.W.; Leão Filho, H.; Coelho, F.M.A.; Buchpiguel, C.; Lima, M.; Carneiro, C.; Pereira, R.M.R.; Aikawa, N.; Silva, C.A.; et al. Does [18F]F-FDG-PET/MRI add metabolic information to magnetic resonance image in childhood-onset Takayasu’s arteritis patients? A multicenter case series. Adv. Rheumatol. 2022, 62, 28. [Google Scholar] [CrossRef]
- Hoffman, G.S. Takayasu arteritis: Lessons from the American National Institutes of Health experience. Int. J. Cardiol. 1996, 54, S99–S102. [Google Scholar] [CrossRef]
- Lagneau, P.; Michel, J.B.; Vuong, P.N. Surgical treatment of Takayasu’s disease. Ann. Surg. 1987, 205, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Garlanda, C.; Doni, A.; Bottazzi, B. Pentraxins in innate immunity: From C-reactive protein to the long pentraxin PTX3. J. Clin. Immunol. 2008, 28, 1–13. [Google Scholar] [CrossRef]
- Kang, F.; Han, Q.; Zhou, X.; Zheng, Z.; Wang, S.; Ma, W.; Zhang, K.; Quan, Z.; Yang, W.; Wang, J.; et al. Performance of the PET vascular activity score (PETVAS) for qualitative and quantitative assessment of inflammatory activity in Takayasu’s arteritis patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3107–3117. [Google Scholar] [CrossRef]
- Gomez, L.; Chaumet-Riffaud, P.; Noel, N.; Lambotte, O.; Goujard, C.; Durand, E.; Besson, F.L. Effect of CRP value on 18F-FDG PET vascular positivity in Takayasu arteritis: A systematic review and per-patient based meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 575–581. [Google Scholar] [CrossRef]
- Lee, S.; Eun, Y.; Kim, H.; Lee, J.; Koh, E.M.; Kim, D.K.; Cha, H.S. Factors associated with radiographic progression in patients with Takayasu’s arteritis. Clin. Exp. Rheumatol. 2021, 39 (Suppl. 129), 46–51. [Google Scholar] [CrossRef]
- Sun, Y.; Ma, L.; Chen, H.; Kong, X.; Lv, P.; Dai, X.; Ji, Z.; Yang, C.; Dai, S.; Wu, L.; et al. Analysis of predictive factors for treatment resistance and disease relapse in Takayasu’s arteritis. Clin. Rheumatol. 2018, 37, 2789–2795. [Google Scholar] [CrossRef]
- Rimland, C.A.; Quinn, K.A.; Rosenblum, J.S.; Schwartz, M.N.; Bates Gribbons, K.; Novakovich, E.; Sreih, A.G.; Merkel, P.A.; Ahlman, M.A.; Grayson, P.C. Outcome Measures in Large Vessel Vasculitis: Relationship Between Patient-, Physician-, Imaging-, and Laboratory-Based Assessments. Arthritis Care Res. 2020, 72, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Carlson, C.S.; Aldred, S.F.; Lee, P.K.; Tracy, R.P.; Schwartz, S.M.; Rieder, M.; Liu, K.; Williams, O.D.; Iribarren, C.; Lewis, E.C.; et al. Polymorphisms within the C-reactive protein (CRP) promoter region are associated with plasma CRP levels. Am. J. Hum. Genet. 2005, 77, 64–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goel, R.; Kabeerdoss, J.; Ram, B.; Prakash, J.A.; Babji, S.; Nair, A.; Jeyaseelan, L.; Jeyaseelan, V.; Mathew, J.; Balaji, V.; et al. Serum Cytokine Profile in Asian Indian Patients with Takayasu Arteritis and its Association with Disease Activity. Open Rheumatol. J. 2017, 11, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, T.; Haraguchi, G.; Kamiishi, T.; Tezuka, D.; Inagaki, H.; Isobe, M. Sensitive assessment of activity of Takayasu’s arteritis by pentraxin3, a new biomarker. J. Am. Coll. Cardiol. 2011, 57, 1712–1713. [Google Scholar] [CrossRef] [Green Version]
- Dagna, L.; Salvo, F.; Tiraboschi, M.; Bozzolo, E.P.; Franchini, S.; Doglioni, C.; Manfredi, A.A.; Baldissera, E.; Sabbadini, M.G. Pentraxin-3 as a marker of disease activity in Takayasu arteritis. Ann. Intern. Med. 2011, 155, 425–433. [Google Scholar] [CrossRef]
- Pulsatelli, L.; Boiardi, L.; Assirelli, E.; Pazzola, G.; Muratore, F.; Addimanda, O.; Dolzani, P.; Versari, A.; Casali, M.; Bottazzi, B.; et al. Imbalance between angiogenic and anti-angiogenic factors in sera from patients with large-vessel vasculitis. Clin. Exp. Rheumatol. 2020, 38 (Suppl. 124), 23–30. [Google Scholar]
- Tombetti, E.; Di Chio, M.C.; Sartorelli, S.; Papa, M.; Salerno, A.; Bottazzi, B.; Bozzolo, E.P.; Greco, M.; Rovere-Querini, P.; Baldissera, E.; et al. Systemic pentraxin-3 levels reflect vascular enhancement and progression in Takayasu arteritis. Arthritis Res. Ther. 2014, 16, 479. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Hu, C.; Sun, F.; Li, J.; Yang, Y.; Tian, X.; Zeng, X. Study on the association of serum pentraxin-3 and lysosomal-associated membrane protein-2 levels with disease activity in Chinese Takayasu’s arteritis patients. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 117), 109–115. [Google Scholar]
- Dai, X.; Wang, J.; Zhang, X.; Wang, L.; Wu, S.; Chen, H.; Sun, Y.; Ma, L.; Ma, L.; Kong, X.; et al. Biomarker Changes and Molecular Signatures Associated with Takayasu Arteritis Following Treatment with Glucocorticoids and Tofacitinib. J. Inflamm. Res. 2022, 15, 4395–4407. [Google Scholar] [CrossRef]
- Alibaz-Oner, F.; Aksu, K.; Yentur, S.P.; Keser, G.; Saruhan-Direskeneli, G.; Direskeneli, H. Plasma pentraxin-3 levels in patients with Takayasu’s arteritis during routine follow-up. Clin. Exp. Rheumatol. 2016, 34, S73–S76. [Google Scholar]
- Wen, X.; Hou, R.; Xu, K.; Han, Y.; Hu, J.; Zhang, Y.; Su, Y.; Gao, J.; Zhang, G.; Zhang, L. Pentraxin 3 is more accurate than C-reactive protein for Takayasu arteritis activity assessment: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0245612. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Zhu, B.; Zhu, Q.; Tursun, D.; Liu, S.; Liu, S.; Hu, J.; Li, N. Study on Serum Pentraxin-3 Levels in Vasculitis with Hypertension. J. Interferon Cytokine Res. 2019, 39, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Du, J.; Li, T.; Liao, H. Platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio associated with disease activity in patients with Takayasu’s arteritis: A case-control study. BMJ Open 2017, 7, e014451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seringec Akkececi, N.; Yildirim Cetin, G.; Gogebakan, H.; Acipayam, C. The C-Reactive Protein/Albumin Ratio and Complete Blood Count Parameters as Indicators of Disease Activity in Patients with Takayasu Arteritis. Med. Sci. Monit. 2019, 25, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Dang, A.M.; Chen, B.W.; Lv, N.Q.; Wang, X.; Zheng, D.Y. The association of red blood cell distribution width with anemia and inflammation in patients with Takayasu arteritis. Clin. Chim. Acta 2015, 438, 205–209. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, D.; Garrido, M.; Comarmond, C.; Desbois, A.C.; Domont, F.; Savey, L.; Terrier, B.; Geri, G.; Rosenzwajg, M.; Klatzmann, D.; et al. Th1 and Th17 cytokines drive inflammation in Takayasu arteritis. Arthritis Rheumatol. 2015, 67, 1353–1360. [Google Scholar] [CrossRef]
- Misra, D.P.; Chaurasia, S.; Misra, R. Increased Circulating Th17 Cells, Serum IL-17A, and IL-23 in Takayasu Arteritis. Autoimmune Dis. 2016, 2016, 7841718. [Google Scholar] [CrossRef] [Green Version]
- Misra, D.P.; Agarwal, V. Th17.1 lymphocytes: Emerging players in the orchestra of immune-mediated inflammatory diseases. Clin. Rheumatol. 2022, 41, 2297–2308. [Google Scholar] [CrossRef]
- Singh, K.; Rathore, U.; Rai, M.K.; Behera, M.R.; Jain, N.; Ora, M.; Bhadauria, D.; Sharma, S.; Pande, G.; Gambhir, S.; et al. Novel Th17 Lymphocyte Populations, Th17.1 and PD1+Th17, are Increased in Takayasu Arteritis, and Both Th17 and Th17.1 Sub-Populations Associate with Active Disease. J. Inflamm. Res. 2022, 15, 1521–1541. [Google Scholar] [CrossRef]
- Tian, Y.; Li, J.; Tian, X.; Zeng, X. Using the co-expression network of T cell-activation-related genes to assess the disease activity in Takayasu’s arteritis patients. Arthritis Res. Ther. 2021, 23, 303. [Google Scholar] [CrossRef]
- Maciejewski-Duval, A.; Comarmond, C.; Leroyer, A.; Zaidan, M.; Le Joncour, A.; Desbois, A.C.; Fouret, J.P.; Koskas, F.; Cluzel, P.; Garrido, M.; et al. mTOR pathway activation in large vessel vasculitis. J. Autoimmun. 2018, 94, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Xu, M.; Cui, X.; Ma, L.; Cheng, H.; Hou, J.; Sun, X.; Ma, L.; Jiang, L. Potential Role of Macrophage Phenotypes and CCL2 in the Pathogenesis of Takayasu Arteritis. Front. Immunol. 2021, 12, 646516. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, B.F.; Mumtaz, I.M.; Loddenkemper, K.; Bruns, A.; Sengler, C.; Hermann, K.G.; Maza, S.; Keitzer, R.; Burmester, G.R.; Buttgereit, F.; et al. Takayasu arteritis is characterised by disturbances of B cell homeostasis and responds to B cell depletion therapy with rituximab. Ann. Rheum. Dis. 2012, 71, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Zanwar, A.; Jain, A.; Gupta, L.; Chaurasia, S.; Kumar, S.; Misra, D.P.; Misra, R. Serum BAFF and APRIL levels in Indian patients with Takayasu arteritis. Clin. Rheumatol. 2018, 37, 3439–3442. [Google Scholar] [CrossRef]
- González-Gay, M.A.; Castañeda, S. Rituximab in Takayasu arteritis: An unmet hope. Rheumatology 2018, 57, 1133–1134. [Google Scholar] [CrossRef] [Green Version]
- Pazzola, G.; Muratore, F.; Pipitone, N.; Crescentini, F.; Cacoub, P.; Boiardi, L.; Spaggiari, L.; Comarmond, C.; Croci, S.; Saadoun, D.; et al. Rituximab therapy for Takayasu arteritis: A seven patients experience and a review of the literature. Rheumatology 2018, 57, 1151–1155. [Google Scholar] [CrossRef]
- Tripathy, N.K.; Sinha, N.; Nityanand, S. Interleukin-8 in Takayasu’s arteritis: Plasma levels and relationship with disease activity. Clin. Exp. Rheumatol. 2004, 22, S27–S30. [Google Scholar]
- Alibaz-Oner, F.; Yentür, S.P.; Saruhan-Direskeneli, G.; Direskeneli, H. Serum cytokine profiles in Takayasu’s arteritis: Search for biomarkers. Clin. Exp. Rheumatol. 2015, 33, S32–S35. [Google Scholar]
- Kong, X.; Sun, Y.; Ma, L.; Chen, H.; Wei, L.; Wu, W.; Ji, Z.; Ma, L.; Zhang, Z.; Zhang, Z.; et al. The critical role of IL-6 in the pathogenesis of Takayasu arteritis. Clin. Exp. Rheumatol. 2016, 34, S21–S27. [Google Scholar]
- Arraes, A.E.; de Souza, A.W.; Mariz, H.A.; Silva, N.P.; Torres, I.C.; Pinto, P.N.; Lima, E.N.; Sato, E.I. 18F-Fluorodeoxyglucose positron emission tomography and serum cytokines and matrix metalloproteinases in the assessment of disease activity in Takayasu’s arteritis. Rev. Bras. Reumatol. Engl. Ed. 2016, 56, 299–308. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Wang, Y.; Wang, Y.; Wang, Y.; Yang, Y.; Zhao, J.; Li, M.; Tian, X.; Zeng, X. Association between acute phase reactants, interleukin-6, tumor necrosis factor-α, and disease activity in Takayasu’s arteritis patients. Arthritis Res. Ther. 2020, 22, 285. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Kong, X.; Cui, X.; Dai, X.; Ma, L.; Chen, H.; Chen, R.; Lv, P.; Lin, J.; Huang, Q.; et al. The value of interleukin-6 in predicting disease relapse for Takayasu arteritis during 2-year follow-up. Clin. Rheumatol. 2020, 39, 3417–3425. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ma, L.; Yan, F.; Liu, H.; Ding, Y.; Hou, J.; Jiang, L. MMP-9 and IL-6 are potential biomarkers for disease activity in Takayasu’s arteritis. Int. J. Cardiol. 2012, 156, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Nakaoka, Y.; Yanagawa, M.; Hata, A.; Yamashita, K.; Okada, N.; Yamakido, S.; Hayashi, H.; Jayne, D. Vascular imaging of patients with refractory Takayasu arteritis treated with tocilizumab: Post hoc analysis of a randomized controlled trial. Rheumatology 2022, 61, 2360–2368. [Google Scholar] [CrossRef]
- Mekinian, A.; Biard, L.; Dagna, L.; Novikov, P.; Salvarani, C.; Espitia, O.; Sciascia, S.; Michaud, M.; Lambert, M.; Hernández-Rodríguez, J.; et al. Efficacy and safety of TNF-α antagonists and tocilizumab in Takayasu arteritis: Multicentre retrospective study of 209 patients. Rheumatology 2022, 61, 1376–1384. [Google Scholar] [CrossRef]
- Nityanand, S.; Mishra, K.; Shrivastava, S.; Holm, G.; Lefvert, A.K. Autoantibodies against cardiolipin and endothelial cells in Takayasu’s arteritis: Prevalence and isotype distribution. Br. J. Rheumatol. 1997, 36, 923–924. [Google Scholar] [CrossRef] [Green Version]
- Tripathy, N.K.; Sinha, N.; Nityanand, S. Anti-annexin V antibodies in Takayasu’s arteritis: Prevalence and relationship with disease activity. Clin. Exp. Immunol. 2003, 134, 360–364. [Google Scholar] [CrossRef]
- Keşkek, Ş.; Bozkırlı-Ersözlü, E.D.; Kozanoglu, I.; Yücel, A.E. High Levels of Circulating Endothelial Progenitor Cells Are Associated with Acrotism in Patients with Takayasu Arteritis. Med. Princ. Pract. 2017, 26, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Tripathy, N.K.; Chandran, V.; Garg, N.K.; Sinha, N.; Nityanand, S. Soluble endothelial cell adhesion molecules and their relationship to disease activity in Takayasu’s arteritis. J. Rheumatol. 2008, 35, 1842–1845. [Google Scholar]
- Dogan, S.; Piskin, O.; Solmaz, D.; Akar, S.; Gulcu, A.; Yuksel, F.; Cakır, V.; Sari, I.; Akkoc, N.; Onen, F. Markers of endothelial damage and repair in Takayasu arteritis: Are they associated with disease activity? Rheumatol. Int. 2014, 34, 1129–1138. [Google Scholar] [CrossRef]
- Matsuyama, A.; Sakai, N.; Ishigami, M.; Hiraoka, H.; Kashine, S.; Hirata, A.; Nakamura, T.; Yamashita, S.; Matsuzawa, Y. Matrix metalloproteinases as novel disease markers in Takayasu arteritis. Circulation 2003, 108, 1469–1473. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Kong, X.; Wu, S.; Ma, L.; Yan, Y.; Lv, P.; Jiang, L. YKL-40 as a new biomarker of disease activity in Takayasu arteritis. Int. J. Cardiol. 2019, 293, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, N.; Dhawan, V.; Malik, S.; Jain, S. Implication of oxidative stress and its correlation with activity of matrix metalloproteinases in patients with Takayasu’s arteritis disease. Int. J. Cardiol. 2010, 145, 286–288. [Google Scholar] [CrossRef]
- Nair, A.M.; Goel, R.; Hindhumati, M.; Jayakanthan, K.; Visalakshi, J.; Joseph, G.; Danda, S.; Danda, D. Serum amyloid A as a marker of disease activity and treatment response in Takayasu arteritis. Rheumatol. Int. 2017, 37, 1643–1649. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.; Nair, A.; Kabeerdoss, J.; Mohan, H.; Jeyaseelan, V.; Joseph, G.; Danda, D. Study of serial serum myeloid-related protein 8/14 as a sensitive biomarker in Takayasu arteritis: A single centre study. Rheumatol. Int. 2018, 38, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Springer, J.M.; Monach, P.; Cuthbertson, D.; Carette, S.; Khalidi, N.A.; McAlear, C.A.; Pagnoux, C.; Seo, P.; Warrington, K.J.; Ytterberg, S.R.; et al. Serum S100 Proteins as a Marker of Disease Activity in Large Vessel Vasculitis. J. Clin. Rheumatol. 2018, 24, 393–395. [Google Scholar] [CrossRef]
- Cem, S.; Berkan, A.; Alper, S.; Abdulsamer, E.; Levent, K.; Ali, A. Fecal S100A12 in Takayasu arteritis predicts disease activity and intestinal involvement. Rheumatol. Int. 2022, 42, 737–742. [Google Scholar] [CrossRef]
- Chen, S.; Luan, H.; He, J.; Wang, Y.; Zeng, X.; Li, Y.; Yuan, H. Serum C1q concentration is associated with disease activity in Chinese Takayasu arteritis patients: A case-control study. Health Sci. Rep. 2021, 4, e252. [Google Scholar] [CrossRef]
- Chen, R.; Ma, L.; Lv, P.; Lin, J.; Li, C.; Yan, Y.; Jin, X.; Dai, X.; Ji, Z.; Chen, H.; et al. Serum complement 3 is a potential biomarker for assessing disease activity in Takayasu arteritis. Arthritis Res. Ther. 2021, 23, 63. [Google Scholar] [CrossRef]
- Ma, L.; Yu, W.; Dai, X.; Yin, M.; Wang, Y.; Sun, Y.; Kong, X.; Cui, X.; Wu, S.; Ji, Z.; et al. Serum leptin, a potential predictor of long-term angiographic progression in Takayasu’s arteritis. Int. J. Rheum. Dis. 2019, 22, 2134–2142. [Google Scholar] [CrossRef]
- Karadeniz, H.; Güler, A.A.; Koca, G.; Salman, R.B.; Satış, H.; Ataş, N.; Babaoğlu, H.; Paşaoğlu, H.; Küçük, H.; Tufan, A.; et al. Serum levels of fetuin-A as a novel biomarker for disease activity in patients with Takayasu arteritis and granulomatous polyangiitis. Clin. Rheumatol. 2022, 41, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Luo, X.; Wu, Q.; Chen, Z.; Kou, L.; Wang, H. Circulation levels of acute phase proteins in patients with Takayasu arteritis. J. Vasc. Surg. 2010, 51, 700–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, X.; Qin, F.; Song, L.; Wang, T.; Geng, B.; Zhang, W.; Jin, L.; Wang, W.; Li, S.; Tian, X.; et al. Novel Biomarkers for the Precisive Diagnosis and Activity Classification of Takayasu Arteritis. Circ. Genom. Precis. Med. 2019, 12, e002080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, X.; Zhang, F.; Huang, Y.; Wang, Z.; Wu, Q. Plasma proteomic screening and validation of novel biomarkers in Takayasu’s arteritis. Clin. Exp. Rheumatol. 2021, 39, 1352–1359. [Google Scholar] [CrossRef]
- Wen, X.; Song, G.; Hu, C.; Pan, J.; Wu, Z.; Li, L.; Liu, C.; Tian, X.; Zhang, F.; Qian, J.; et al. Identification of Novel Serological Autoantibodies in Takayasu Arteritis Patients Using HuProt Arrays. Mol. Cell Proteom. 2021, 20, 100036. [Google Scholar] [CrossRef]
- Kong, X.; Wu, S.; Dai, X.; Yu, W.; Wang, J.; Sun, Y.; Ji, Z.; Ma, L.; Dai, X.; Chen, H.; et al. A comprehensive profile of chemokines in the peripheral blood and vascular tissue of patients with Takayasu arteritis. Arthritis Res. Ther. 2022, 24, 49. [Google Scholar] [CrossRef]
- Jain, A.; Kumar, D.; Guleria, A.; Misra, D.P.; Zanwar, A.; Chaurasia, S.; Kumar, S.; Kumar, U.; Mishra, S.K.; Goel, R.; et al. NMR-Based Serum Metabolomics of Patients with Takayasu Arteritis: Relationship with Disease Activity. J. Proteome Res. 2018, 17, 3317–3324. [Google Scholar] [CrossRef]
- Kumar, U.; Jain, A.; Guleria, A.; Misra, D.P.; Goel, R.; Danda, D.; Misra, R.; Kumar, D. Circulatory Glutamine/Glucose ratio for evaluating disease activity in Takayasu arteritis: A NMR based serum metabolomics study. J. Pharm. Biomed. Anal. 2020, 180, 113080. [Google Scholar] [CrossRef]
- Stojanovic, M.; Raskovic, S.; Milivojevic, V.; Miskovic, R.; Soldatovic, I.; Stankovic, S.; Rankovic, I.; Stankovic Stanojevic, M.; Dragasevic, S.; Krstic, M.; et al. Enhanced Liver Fibrosis Score as a Biomarker for Vascular Damage Assessment in Patients with Takayasu Arteritis-A Pilot Study. J. Cardiovasc. Dev. Dis. 2021, 8, 187. [Google Scholar] [CrossRef]
- Terao, C.; Yoshifuji, H.; Kimura, A.; Matsumura, T.; Ohmura, K.; Takahashi, M.; Shimizu, M.; Kawaguchi, T.; Chen, Z.; Naruse, T.K.; et al. Two susceptibility loci to Takayasu arteritis reveal a synergistic role of the IL12B and HLA-B regions in a Japanese population. Am. J. Hum. Genet. 2013, 93, 289–297. [Google Scholar] [CrossRef]
- Terao, C.; Yoshifuji, H.; Matsumura, T.; Naruse, T.K.; Ishii, T.; Nakaoka, Y.; Kirino, Y.; Matsuo, K.; Origuchi, T.; Shimizu, M.; et al. Genetic determinants and an epistasis of LILRA3 and HLA-B*52 in Takayasu arteritis. Proc. Natl. Acad. Sci. USA 2018, 115, 13045–13050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, T.; Yoshifuji, H.; Shimizu, M.; Kitagori, K.; Murakami, K.; Nakashima, R.; Imura, Y.; Tanaka, M.; Ohmura, K.; Matsuda, F.; et al. A novel susceptibility locus in the IL12B region is associated with the pathophysiology of Takayasu arteritis through IL-12p40 and IL-12p70 production. Arthritis Res. Ther. 2017, 19, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadoba, K.; Watanabe, R.; Iwasaki, T.; Nakajima, T.; Kitagori, K.; Akizuki, S.; Murakami, K.; Nakashima, R.; Hashimoto, M.; Tanaka, M.; et al. A susceptibility locus in the IL12B but not LILRA3 region is associated with vascular damage in Takayasu arteritis. Sci. Rep. 2021, 11, 13667. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.Y.; Wu, B.; Jin, X.J.; Sun, Y.; Kong, X.F.; Ji, Z.F.; Chen, R.Y.; Cui, X.M.; Shi, H.C.; Jiang, L.D. A novel model to assess disease activity in Takayasu arteritis based on 18F-FDG-PET/CT: A Chinese cohort study. Rheumatology 2022, 61, Si14–Si22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items Common to the DEI.TAK and TADS | Items Common to the ITAS2010 and TADS | ||
|---|---|---|---|
| Domain | Items | Domain | Items |
| Renal | Systolic hypertension * Diastolic hypertension * Proteinuria Elevation of serum creatinine | Renal | Systolic hypertension * Diastolic hypertension * |
| Nervous system | Organic confusion/dementia Seizures Stroke Cord lesion | Nervous system | Stroke Seizures |
| Cardiovascular system | Vascular bruits Pulse and BP inequality Pulse loss Limb claudication Aortic regurgitation Ischemic cardiac pain Congestive cardiac failure Cardiomyopathy | Cardiovascular system | Vascular bruits Pulse and BP inequality Pulse loss Limb claudication Aortic regurgitation Ischemic cardiac pain Congestive cardiac failure Cardiomyopathy |
| Eyes | Vision loss | - | - |
| Chest | Persistent cough/wheeze/dyspnea | - | - |
| Domain | Scoring System or Criteria |
|---|---|
| Disease activity | |
| Clinical | National Institutes of Health (NIH) disease activity score |
| Disease Extent Index in Takayasu Arteritis (DEI.TAK) | |
| Indian Takayasu Clinical Activity Score (ITAS2010) and ITAS2010 modified for acute phase reactants ESR or CRP (ITAS-A) | |
| Abatacept in Giant Cell Arteritis and Takayasu arteritis (AGATA) criteria | |
| Dabague criteria | |
| European Alliance of Associations for Rheumatology (EULAR) criteria | |
| Future relapses | |
| Time-to-relapse | |
| Percentage reduction in corticosteroid dose from baseline | |
| Imaging | Positron Emission Tomography Vasculitis Activity Score (PETVAS) |
| Damage | |
| Clinical | Vasculitis Damage Index (VDI) |
| Combined Damage Assessment Score (CDA) | |
| Takayasu Arteritis Damage Score (TADS) | |
| Imaging | Color Doppler Ultrasound Score from Kolkata (CDUS-K) * |
| Angiographic Stenosis Score (ASS), Angiographic Dilatation Score (ADS) and Angiographic Composite Score (ACS) | |
| Combined Arteritis Damage Score (CARDS) | |
| Domain | Biomarker |
|---|---|
| Disease activity | |
| Acute phase reactants | ESR |
| CRP | |
| Pentraxin-3 | |
| Biomarkers from routine hemogram | Platelet-to-lymphocyte ratio |
| Neutrophil-to-lymphocyte ratio | |
| Monocyte-to-lymphocyte ratio | |
| Red cell distribution width | |
| Cell populations in peripheral blood and their related trophic factors | Th1, Th17 and Th17.1 lymphocytes |
| Gene expression of TCR, CD28, GATA3, RORC (increased expression) and CD40 (decreased expression) | |
| CCL-2 | |
| BAFF, APRIL | |
| Cytokines | IL-6, TNF-α, IL- 8, IL- 23, IL-10, IL-18 |
| Autoantibodies | Anti-cardiolipin antibodies |
| Anti-endothelial cell antibodies | |
| Anti-annexin V | |
| Markers of endothelial injury | Circulating ECs and EPCs |
| VCAM-1, ICAM-1, VEGF | |
| Matrix metalloproteinases | MMP-2, MMP-3, MMP-9, TIMP-1 |
| Miscellaneous biomarkers | SAA |
| S100A8/S100A9/MRP 8/14 | |
| S100A12 | |
| C1q | |
| C3 | |
| Leptin | |
| Fetuin-A | |
| Proteomics | Serum amyloid A, C4BP, RAG-1 |
| CA125, FLRG, IGFBP-2, CA15-3, GROα, LYVE-1, ULB-2, CD99 | |
| CCL-22, RANTES, CXCL-11, CXCL-16, IL-16 | |
| Metabolomics | Glutamate, proline, N-acetyl glycoprotein, glucose, glycerol, phosphoglyceride, phenylalanine, low-density lipoprotein cholesterol |
| Glutamine-to-glucose ratio; Lactate-to-glucose ratio | |
| Vascular damage | |
| ELF score | TIMP-1, hyaluronic acid, amino-terminal peptide of procollagen type III |
| Delineation of validated cut-offs for DEI.TAK and ITAS2010. |
| Modification of DEI.TAK and ITAS2010 to incorporate information from imaging. |
| Development and validation of new disease activity scoring systems using a data-driven approach. |
| Development and validation of damage indices for TAK using a data-driven approach. |
| Development of a TAK-specific patient-reported outcome measure. |
| Development and validation of composite scoring systems incorporating information from clinical disease activity scores, vascular imaging, and circulating biomarkers. |
| Identification of biomarkers to reflect vascular damage in TAK. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Misra, D.P.; Jain, N.; Ora, M.; Singh, K.; Agarwal, V.; Sharma, A. Outcome Measures and Biomarkers for Disease Assessment in Takayasu Arteritis. Diagnostics 2022, 12, 2565. https://doi.org/10.3390/diagnostics12102565
Misra DP, Jain N, Ora M, Singh K, Agarwal V, Sharma A. Outcome Measures and Biomarkers for Disease Assessment in Takayasu Arteritis. Diagnostics. 2022; 12(10):2565. https://doi.org/10.3390/diagnostics12102565
Chicago/Turabian StyleMisra, Durga Prasanna, Neeraj Jain, Manish Ora, Kritika Singh, Vikas Agarwal, and Aman Sharma. 2022. "Outcome Measures and Biomarkers for Disease Assessment in Takayasu Arteritis" Diagnostics 12, no. 10: 2565. https://doi.org/10.3390/diagnostics12102565