
Use of a Small Car-Mounted Magnetic Resonance Imaging System for On-Field Screening for Osteochondritis Dissecans of the Humeral Capitellum
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
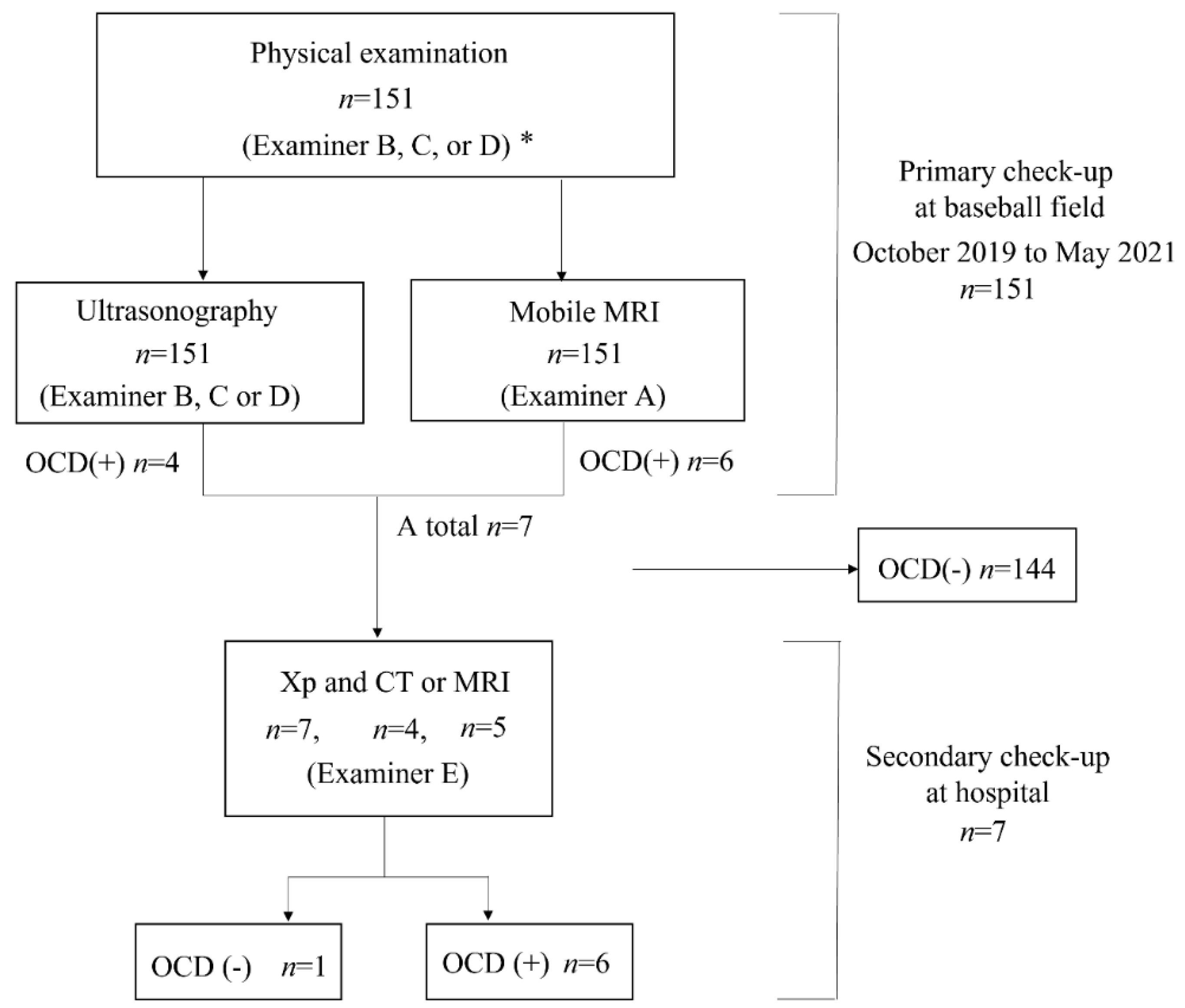
2.1. Study Design and Participants
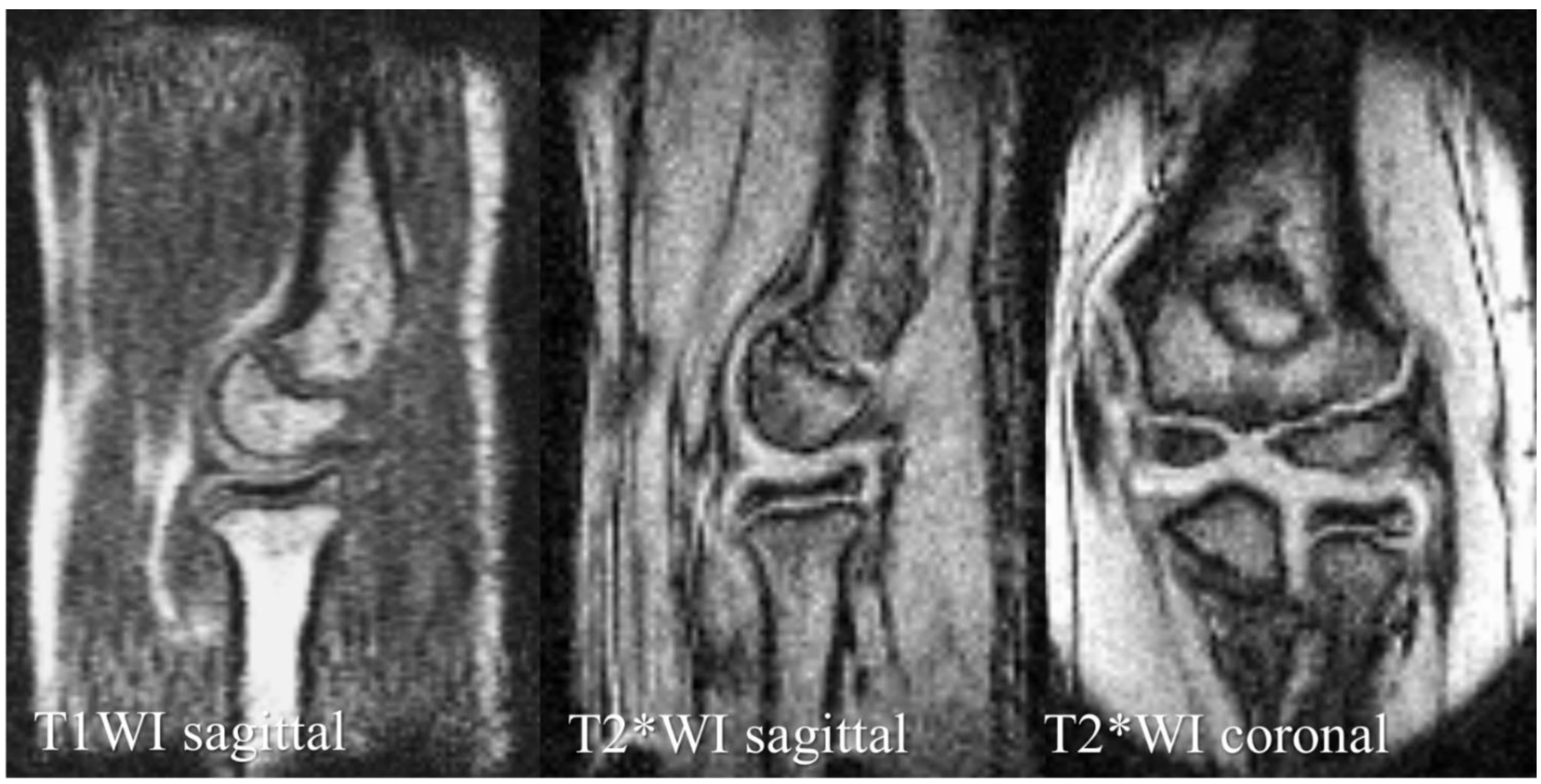
2.2. The Mobile MRI system
2.3. OCD Screening
2.4. Evaluation Components
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nakagomi, M.; Kajiwara, M.; Matsuzaki, J.; Tanabe, K.; Hoshiai, S.; Okamoto, Y.; Terada, Y. Development of a small car-mounted magnetic resonance imaging system for human elbows using a 0.2-T permanent magnet. J. Magn. Reson. 2019, 304, 1–6. [Google Scholar] [CrossRef] [PubMed]
- George, S.S.; Huang, M.C.; Ignjatovic, Z. Portable ultrasound imaging system with super-resolution capabilities. Ultrasonics 2019, 94, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Deoni, S.C.; Medeiros, P.; Deoni, A.; Burton, P.; Beauchemin, J.; D’Sa, V.; Boskamp, E.; By, S.; Nulty, C.M.; Mileski, W.; et al. Development of a mobile low-field MRI scanner. Sci. Rep. 2022, 12, e5690. [Google Scholar] [CrossRef]
- Takahashi, Y.; Doi, M.; Yamada, T.; Tamanoi, T.; Murase, K.; Mochizuki, T. Present status and issues regarding X-ray medical checkup vehicles in preventive medicine: Usefulness of mass screening for lung cancer by an X-ray medical checkup vehicle. Nihon Hoshasen Gijutsu Gakkai Zasshi 2005, 61, 847–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okamoto, Y.; Maehara, K.; Kanahori, T.; Hiyama, T.; Kawamura, T.; Minami, M. Incidence of elbow injuries in adolescent baseball players: Screening by a low field magnetic resonance imaging system specialized for small joints. Jpn. J. Radiol. 2016, 34, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Kamada, H.; Tsukagoshi, Y.; Tomaru, Y.; Nakagawa, S.; Tanaka, K.; Mataki, Y.; Takeuchi, Y.; Ymazaki, M. Influence of commuting methods on low back pain and musculoskeletal function of the lower limbs in elementary school children: A cross-sectional study. J. Orthop. Sci. 2022, 27, 1120–1125. [Google Scholar] [CrossRef]
- Matsuura, T.; Suzue, N.; Iwame, T.; Nishio, S.; Sairyo, K. Prevalence of osteochondritis dissecans of the capitellum in young baseball players: Results based on ultrasonographic findings. Orthop. J. Sports. Med. 2014, 2, e2325967114545298. [Google Scholar] [CrossRef]
- Iwame, T.; Matsuura, T.; Suzue, N.; Kashiwaguchi, S.; Iwase, T.; Fukuta, S.; Hamada, D.; Goto, T.; Tsutsui, T.; Wada, K.; et al. Outcome of an elbow check-up system for child and adolescent baseball players. J. Med. Invest. 2016, 63, 171–174. [Google Scholar] [CrossRef] [Green Version]
- Takagishi, K.; Matsuura, T.; Masatomi, T.; Chosa, E.; Takika, T.; Watanabe, M.; Iwame, T.; Otani, T.; Inagaki, K.; Ikegami, H.; et al. Shoulder and elbow pain in elementary school baseball players: The results from a nation-wide survey in Japan. J. Orthop. Sci. 2017, 22, 682–686. [Google Scholar] [CrossRef]
- Kida, Y.; Morihara, T.; Kotoura, Y.; Hojo, T.; Tachiiri, H.; Sukenari, T.; Iwata, Y.; Furukawa, R.; Oda, R.; Arai, Y.; et al. Prevalence and clinical characteristics of osteochondritis dissecans of the humeral capitellum among adolescent baseball players. Am. J. Sports. Med. 2014, 42, 1963–1971. [Google Scholar] [CrossRef]
- Matsuura, T.; Kashiwaguchi, S.; Iwase, T.; Takeda, Y.; Yasui, N. Conservative treatment for osteochondrosis of the humeral capitellum. Am. J. Sports. Med. 2008, 36, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, T.; Iwame, T.; Iwase, J.; Sairyo, K. Osteochondritis dissecans of the capitellum: Review of the literature. J. Med. Invest. 2020, 67, 217–221. [Google Scholar] [CrossRef] [PubMed]
- Matsuura, T.; Iwame, T.; Suzue, N.; Takao, S.; Nishio, S.; Arisawa, K.; Sairyo, K. Cumulative incidence of osteochondritis dissecans of the capitellum in preadolescent baseball players. Arthroscopy 2019, 35, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Kohyama, S.; Ogawa, T.; Mamizuka, N.; Hara, Y.; Yamazaki, M. A magnetic resonance imaging-based staging system for osteochondritis dissecans of the elbow: A validation study against the International Cartilage Repair Society Classification. Orthop. J. Sports. Med. 2018, 6, e2325967118794620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohyama, S.; Nishiura, Y.; Hara, Y.; Ogawa, T.; Ikumi, A.; Okano, E.; Totoki, Y.; Yoshii, Y.; Yamazaki, M. Preoperative evaluation and surgical simulation for osteochondritis dissecans of the elbow using three-dimensional MRI-CT image fusion images. Diagnostics. 2021, 11, 2337. [Google Scholar] [CrossRef]
- Takahara, M.; Shundo, M.; Kondo, M.; Suzuki, K.; Nambu, T.; Ogino, T. Early detection of osteochondritis dissecans of the capitellum in young baseball players. Report of three cases. J. Bone. Joint. Surg. Am. 1998, 80, 892–897. [Google Scholar] [CrossRef]
- Carpenter, C.; Pines, J.M.; Schuur, J.D.; Muir, M.; Calfee, R.P.; Raja, A.S. Adult scaphoid fracture. Acad. Emerg. Med. 2014, 21, 101–121. [Google Scholar] [CrossRef]
- Schutz, U.; Ehrhardt, M.; God, S.; Billich, C.; Beer, M.; Trattnig, S. A mobile MRI field study of the biochemical cartilage reaction of the knee joint during a 4,486 km transcontinental multistage ultramarathon using T2* mapping. Sci. Rep. 2020, 10, e8157. [Google Scholar] [CrossRef]
- Schomoller, A.; Risch, L.; Kaplick, H.; Wochatz, M.; Engel, T.; Schraplau, A.; Sonnenburg, D.; Huppertz, A.; Mayer, F. Inter-rater and inter-session reliability of lumbar paraspinal muscle composition in a mobile MRI device. Br. J. Radiol. 2021, 94, e20210141. [Google Scholar] [CrossRef]
- Mateen, F.J.; Cooley, C.Z.; Stockmann, J.; Rice, D.R.; Vogel, A.C.; Wald, L.L. Low-field portable brain MRI in CNS demyelinating Disease. Mult. Scler. Relat. Disord. 2021, 51, e102903. [Google Scholar] [CrossRef]
- Deoni, S.C.L.; Bruchhage, M.M.K.; Beauchemin, J.; Volpe, A.; D’Sa, V.; Huentelman, M.; Williams, S.C.R. Accessible pediatric neuroimaging using a low field strength MRI scanner. Neuroimage 2021, 238, e118273. [Google Scholar] [CrossRef] [PubMed]
- Harada, M.; Takahara, M.; Sasaki, J.; Mura, N.; Ito, T. Using sonography for the early detection of elbow injuries among young baseball players. Am. J. Roentgenol. 2006, 187, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Takahara, M.; Ogino, T.; Tsuchida, H.; Takagi, M.; Kashiwa, H.; Nambu, T. Sonographic assessment of osteochondritis Dissecans of the humeral capitellum. Am. J. Roentgenol. 2000, 174, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Niu, E.L.; Tepolt, F.A.; Bae, T.S.; Lebrun, D.G.; Kocher, M.S. Nonoperative management of stable pediatric osteochondritis dissecans of the capitellum: Predictors of treatment success. J. Shoulder. Elbow. Surg. 2018, 27, 2030–2037. [Google Scholar] [CrossRef] [PubMed]
- Uno, T.; Takahara, M.; Maruyama, M.; Harada, M.; Satake, H.; Takagei, M. Qualitative and quantitative assessments of radiographic healing of osteochondritis dissecans of the humeral capitellum. JSES Int. 2021, 5, 554–560. [Google Scholar] [CrossRef]
- Marques, J.P.; Simonis, F.F.J.; Webb, A.G. Low-field MRI: An MR physics perspective. J. Magn. Reson. Imaging 2019, 49, 1528–1542. [Google Scholar] [CrossRef] [Green Version]
- Ghazinoor, S.; Crues, J.V., 3rd; Crowley, C. Low-field musculoskeletal MRI. J. Magn. Reson. Imaging 2007, 25, 234–244. [Google Scholar] [CrossRef]
- Hori, M.; Hagiwara, A.; Goto, M.; Wada, A.; Aoki, S. Low-Field Magnetic Resonance Imaging: Its History and Renaissance. Invest. Radiol. 2022, 56, 669–679. [Google Scholar] [CrossRef]
- Gach, H.M.; Curcuru, A.N.; Wittland, E.J.; Maraghechi, B.; Cai, B.; Mutic, S.; Green, O.L. MRI quality control for low-field MR-IGRT systems: Lessons learned. J. Appl. Clin. Med. Phys. 2019, 20, 53–66. [Google Scholar] [CrossRef]
- Blehar, D.J.; Barton, B.; Gaspari, R.J. Learning curves in emergency ultrasound education. Acad. Emerg. Med. 2015, 22, 574–582. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence Type | T1WI | T2*WI | T2*WI |
|---|---|---|---|
| Image plane | Sagittal | Sagittal | Coronal |
| FOV | 180 × 120 × 90 mm3 | 180 × 180 mm2 | 180 × 180 mm2 |
| Matrix size | 256 × 128 × 32 | 256 × 192 | 256 × 192 |
| Slice thickness, mm | - | 3 | 3 |
| TR, ms | 40 | 500 | 500 |
| TE, ms | 4 | 16 | 16 |
| Flip angel | 60° | 75° | 75° |
| Scan time | 1 min 22 s | 1 min 38 s | 1 min 38 s |
| OCD (−) | OCD (+) | |
|---|---|---|
| Cases | 145 | 6 |
| Mean age (years) | 11.6 ± 1.3 | 12.3 ± 1.2 |
| Sex | Male: 143 | Male: 6 |
| Female: 2 | Female: 0 | |
| Medial elbow pain, n (%) | 30 (20.7) | 3 (50.0) |
| Lateral elbow pain, n (%) | 6 (4.2) | 3 (50.0) |
| No elbow pain, n (%) | 113 (77.9) | 3 (50.0) |
| Definitive Diagnosis | ||||
|---|---|---|---|---|
| OCD (+) | OCD (−) | |||
| mobile MRI | OCD (+) | 5 | 1 | 6 |
| OCD (−) | 1 | 144 | 145 | |
| 6 | 145 | 151 | ||
| Definitive Diagnosis | ||||
|---|---|---|---|---|
| OCD (+) | OCD (−) | |||
| US | OCD (+) | 4 | 0 | 4 |
| OCD (−) | 2 | 145 | 147 | |
| 6 | 145 | 151 | ||
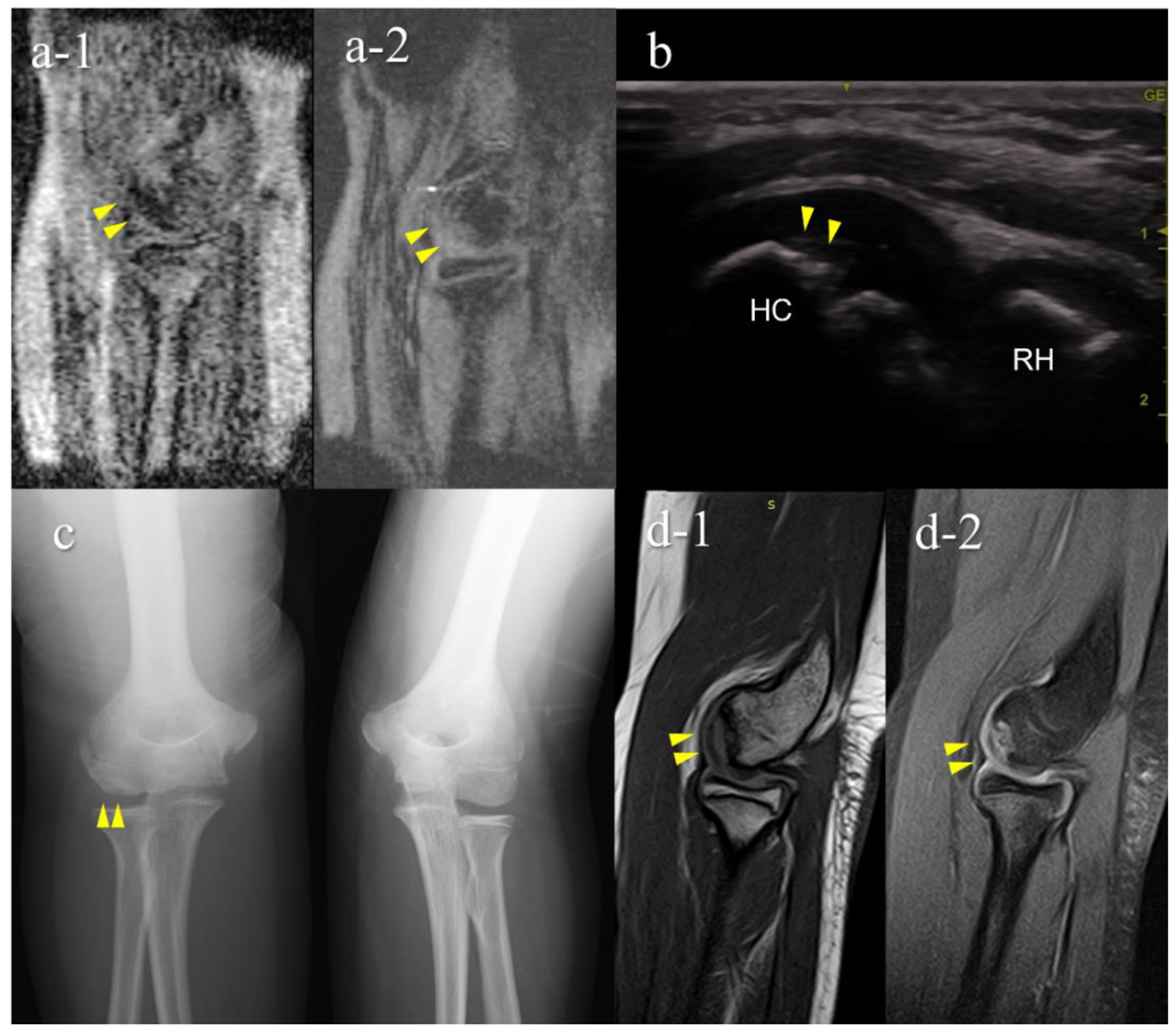
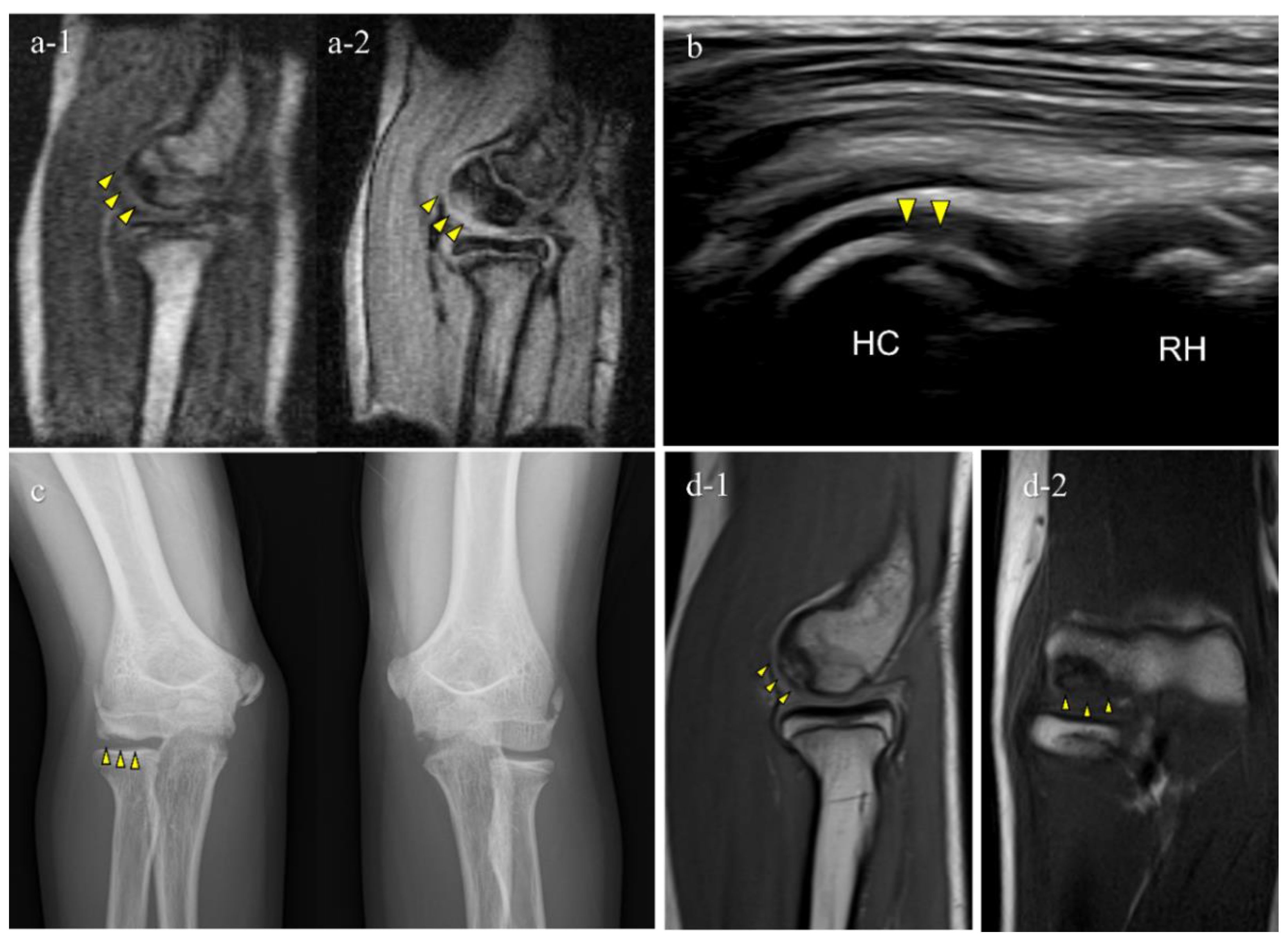
| Case | Age | Sex | Primary Check-Up | Secondary Check-Up | |||||
|---|---|---|---|---|---|---|---|---|---|
| Elbow Symptom | Mobile MRI (RF Probe- Generation) | US (Examiner) | Diagnosis | Stage | Lesion Location | Lesion Diameter (mm) | |||
| 1 | 12 | M | - | − (1st) | + (B) | OCD | II | lateral | 15 |
| 2 | 11 | M | + | + (1st) | + (B) | OCD | I | central | 10 |
| 3 | 12 | M | - | + (2nd) | + (B) | OCD | II | central | 9 |
| 4 | 12 | M | + | + (2nd) | + (B) | OCD | II | lateral | 11 |
| 5 | 12 | M | + | + (2nd) | − (B) | OCD | I | central | 3.5 |
| 6 | 15 | F | - | + (2nd) | − (C) | not OCD | posterior | 3.5 | |
| 7 | 12 | M | - | + (2nd) | − (D) | OCD | I | central | 5.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, K.; Okamoto, Y.; Ogawa, T.; Terada, Y.; Kajiwara, M.; Miyasaka, T.; Michinobu, R.; Hara, Y.; Yoshii, Y.; Nakajima, T.; et al. Use of a Small Car-Mounted Magnetic Resonance Imaging System for On-Field Screening for Osteochondritis Dissecans of the Humeral Capitellum. Diagnostics 2022, 12, 2551. https://doi.org/10.3390/diagnostics12102551
Ikeda K, Okamoto Y, Ogawa T, Terada Y, Kajiwara M, Miyasaka T, Michinobu R, Hara Y, Yoshii Y, Nakajima T, et al. Use of a Small Car-Mounted Magnetic Resonance Imaging System for On-Field Screening for Osteochondritis Dissecans of the Humeral Capitellum. Diagnostics. 2022; 12(10):2551. https://doi.org/10.3390/diagnostics12102551
Chicago/Turabian StyleIkeda, Kazuhiro, Yoshikazu Okamoto, Takeshi Ogawa, Yasuhiko Terada, Michiru Kajiwara, Tomoki Miyasaka, Ryuhei Michinobu, Yuki Hara, Yuichi Yoshii, Takahito Nakajima, and et al. 2022. "Use of a Small Car-Mounted Magnetic Resonance Imaging System for On-Field Screening for Osteochondritis Dissecans of the Humeral Capitellum" Diagnostics 12, no. 10: 2551. https://doi.org/10.3390/diagnostics12102551