
A Nomogram for Predicting Prostate Cancer with Lymph Node Involvement in Robot-Assisted Radical Prostatectomy Era: A Retrospective Multicenter Cohort Study in Japan (The MSUG94 Group)
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Pathological Analysis
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
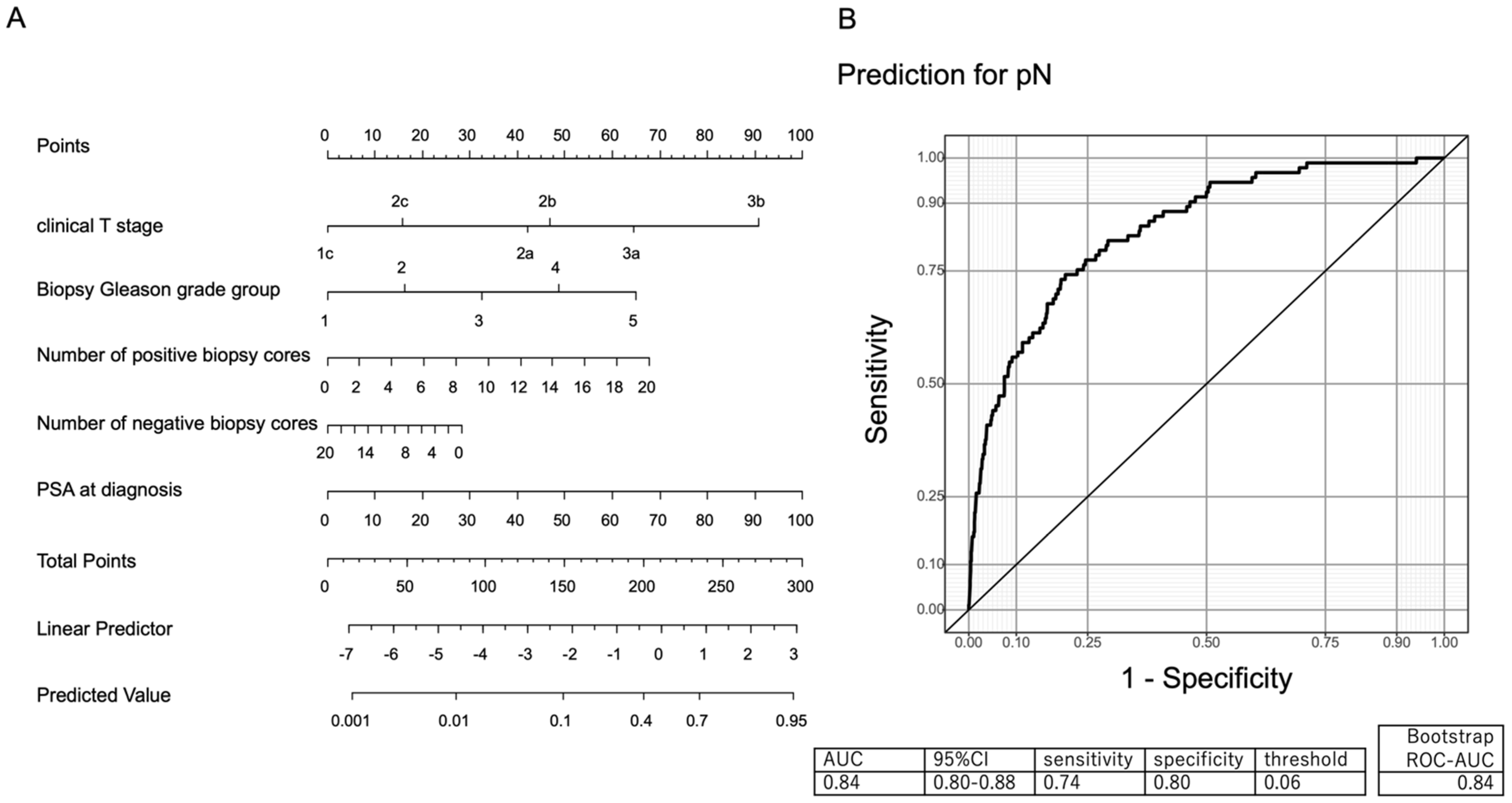
3.2. Development of a Clinically Applicable Nomogram Predicting PCa with Lymph Node Involvement
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rebello, R.J.; Oing, C.; Knudsen, K.E.; Loeb, S.; Johnson, D.C.; Reiter, R.E.; Gillessen, S.; Van der Kwast, T.; Bristow, R.G. Prostate cancer. Nat. Rev. Dis. Prim. 2021, 7, 9. [Google Scholar] [CrossRef] [PubMed]
- Grignon, D.J. Prostate cancer reporting and staging: Needle biopsy and radical prostatectomy specimens. Mod. Pathol. 2018, 31, S96–S109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corn, P.G. The tumor microenvironment in prostate cancer: Elucidating molecular pathways for therapy development. Cancer Manag. Res. 2012, 4, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; Santis, M.D.; Fnati, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Prostate Cancer (2022) NCCN Guidelines®. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 24 January 2022).
- Ilic, D.; Evans, S.M.; Allan, C.A.; Jung, J.H.; Murphy, D.; Frydenberg, M. Laparoscopic and robot-assisted vs open radical prostatectomy for the treatment of localized prostate cancer: A Cochrane systematic review. BJU Int. 2018, 121, 845–853. [Google Scholar] [CrossRef]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Santis, M.D.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- Fossati, N.; Willemse, P.M.; Van den Broeck, T.; van den Bergh, R.C.N.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; Santis, M.D.; et al. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: A systematic review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef]
- Carroll, P.R.; Parsons, J.K.; Andriole, G.; Bahnson, R.R.; Castle, E.P.; Catalona, W.J.; Dahl, D.M.; Davis, J.W.; Epstein, J.I.; Etzioni, R.B.; et al. NCCN Guidelines Insights: Prostate Cancer Early Detection, Version 2.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 509–519. [Google Scholar] [CrossRef]
- Partin, A.W.; Mangold, L.A.; Lamm, D.M.; Walsh, P.C.; Epstein, J.I.; Pearson, J.D. Contemporary update of prostate cancer staging nomograms (Partin Tables) for the new millennium. Urology 2001, 58, 843–848. [Google Scholar] [CrossRef]
- Briganti, A.; Larcher, A.; Abdollah, F.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Sun, M.; Freschi, M.; Salonia, A.; et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: The essential importance of percentage of positive cores. Eur. Urol. 2012, 61, 480–487. [Google Scholar] [CrossRef]
- Memorial Sloan Kettering Cancer Center. Pre-Radical Prostatectomy Tool to Predict Probability of Lymph Node Involvement in Prostate Cancer Patients. Available online: www.mskcc.org/nomograms/prostate/pre_op (accessed on 15 June 2020).
- Gandaglia, G.; Martini, A.; Ploussard, G.; Fossati, N.; Stabile, A.; Visschere, P.D.; Borgmann, H.; Heidegger, I.; Steinkohl, F.; Kretschmer, A.; et al. External Validation of the 2019 Briganti Nomogram for the Identification of Prostate Cancer Patients Who Should Be Considered for an Extended Pelvic Lymph Node Dissection. Eur. Urol. 2020, 78, 138–142. [Google Scholar] [CrossRef]
- Hueting, T.A.; Cornel, E.B.; Somford, D.M.; Jansen, H.; van Basten, J.P.; Pleijhuis, R.G.; Korthorst, R.A.; van der Palen, J.A.; Koffijberg, H. External Validation of Models Predicting the Probability of Lymph Node Involvement in Prostate Cancer Patients. Eur. Urol. Oncol. 2018, 1, 411–417. [Google Scholar] [CrossRef]
- Buyyounouski, M.K.; Choyke, P.L.; McKenney, J.K.; Sartor, O.; Sandler, H.M.; Amin, M.B.; Kattan, M.W.; Lin, D.W. Prostate cancer—Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017, 67, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Clark, T.; Parekh, D.J.; Cookson, M.S.; Chang, S.S.; Smith, E.R., Jr.; Wells, N.; Smith, J.A., Jr. Randomized prospective evaluation of extended versus limited lymph node dissection in patients with clinically localized prostate cancer. J. Urol. 2003, 169, 145–148. [Google Scholar] [CrossRef]
- Furubayashi, N.; Negishi, T.; Iwai, H.; Nagase, K.; Taguchi, K.; Shimokawa, M.; Nakamura, M. Determination of adequate pelvic lymph node dissection range for Japanese males undergoing radical prostatectomy. Mol. Clin. Oncol. 2017, 6, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Allsbrook, W.C.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [Green Version]
- Lestingi, J.F.P.; Guglielmetti, G.B.; Trinh, Q.D.; Coelho, R.F.; Pontes, J.; Bastos, D.; Cordeiro, M.D.; Sarkis, A.S.; Sheila, F.F.; Mitre, A.I.; et al. Extended Versus Limited Pelvic Lymph Node Dissection during Radical Prostatectomy for Intermediate- and High-risk Prostate Cancer: Early Oncological Outcomes from a Randomized Phase 3 Trial. Eur. Urol. 2021, 79, 595–604. [Google Scholar] [CrossRef]
- Yang, G.; Xie, J.; Guo, Y.; Yuan, J.; Wang, R.; Guo, C.; Peng, B.; Yao, X.; Yang, B. Identifying the Candidates Who Will Benefit from Extended Pelvic Lymph Node Dissection at Radical Prostatectomy among Patients with Prostate Cancer. Front. Oncol. 2021, 11, 790183. [Google Scholar] [CrossRef]
- Gandaglia, G.; Fossati, N.; Zaffuto, E.; Bandini, M.; Dell’Oglio, P.; Bravi, C.A.; Fallara, G.; Pellegrino, F.; Nocera, L.; Karakiewixz, P.I.; et al. Development and Internal Validation of a Novel Model to Identify the Candidates for Extended Pelvic Lymph Node Dissection in Prostate Cancer. Eur. Urol. 2017, 72, 632–640. [Google Scholar] [CrossRef]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Fossati, N.; Stabile, A.; Beauval, J.B.; Malavaud, B.; Roumiguie, M.; et al. A Novel Nomogram to Identify Candidates for Extended Pelvic Lymph Node Dissection among Patients with Clinically Localized Prostate Cancer Diagnosed with Magnetic Resonance Imaging-targeted and Systematic Biopsies. Eur. Urol. 2019, 75, 506–514. [Google Scholar] [CrossRef]
- Nave, O.; Elbaz, M. Method of directly defining the inverse mapping applied to prostate cancer immunotherapy—Mathematical model. Int. J. Biomath. 2018, 11, 1850072. [Google Scholar] [CrossRef]
- Nave, O.; Elbaz, M. Combination of singularly perturbed vector field method and method of directly defining the inverse mapping applied to complex ODE system prostate cancer model. J. Biol. Dyn. 2018, 12, 983–1008. [Google Scholar] [CrossRef]
- Leyh-Bannurah, S.R.; Budäus, L.; Pompe, R.; Zaffuto, E.; Briganti, A.; Abdollah, F.; Montorsi, F.; Schiffmann, J.; Menon, M.; Shariat, S.F.; et al. North American Population-Based Validation of the National Comprehensive Cancer Network Practice Guideline Recommendation of Pelvic Lymphadenectomy in Contemporary Prostate Cancer. Prostate 2017, 77, 542–548. [Google Scholar] [CrossRef]
- Francesco Claps, F.; de Pablos-Rodríguez, P.; Gómez-Ferrer, Á.; Mascarós, J.M.; Marenco, J.; Collado Serra, A.; Ramón-Borja, J.C.; Calatrava Fons, A.; Trombetta, C.; Rubio-Briones, J.; et al. Free-indocyanine green-guided pelvic lymph node dissection during radical prostatectomy. Urol. Oncol. Semin. Orig. Investig. 2022, 40, 489.e19–489.e26. [Google Scholar] [CrossRef]
- Claps, F.; Ramírez-Backhaus, M.; Mir Maresma, M.C.; Gómez-Ferrer, Á.; Mascarós, J.M.; Marenco, J.; Collado Serra, A.; Casanova Ramón-Borja, J.; Calatrava Fons, A.; Trombetta, C.; et al. Indocyanine green guidance improves the efficiency of extended pelvic lymph node dissection during laparoscopic radical prostatectomy. Int. J. Urol. 2021, 28, 566–572. [Google Scholar] [CrossRef]
- Mir, M.C.; Campi, R.; Loriot, Y.; Puente, J.; Giannarini, G.; Necchi, A.; Rouprêt, M. Adjuvant Systemic Therapy for High-risk Muscle-invasive Bladder Cancer after Radical Cystectomy: Current Options and Future Opportunities. Eur. Urol. Oncol. 2021, in press. [Google Scholar] [CrossRef]
- Claps, F.; Mir, M.C.; Zargar, H. Molecular markers of systemic therapy response in urothelial carcinoma. Asian J. Urol. 2021, 8, 376–390. [Google Scholar] [CrossRef]
- de Kruijff, I.E.; Beije, N.; Martens, J.W.M.; de Wit, R.; Boormans., J.L.; Sleijfer, S. Liquid Biopsies to Select Patients for Perioperative Chemotherapy in Muscle-invasive Bladder Cancer: A Systematic Review. Eur. Urol. Oncol. 2021, 4, 204–214. [Google Scholar] [CrossRef] [Green Version]
- Vano, Y.A.; Elaidi, R.; Bennamoun, M.; Chevreau, C.; Borchiellini, D.; Pannier, D.; Maillet, D.; Gross-Goupil, M.; Tournigand, C.; Laguerre, B.; et al. Nivolumab, nivolumab-ipilimumab, and VEGFR-tyrosine kinase inhibitors as first-line treatment for metastatic clear-cell renal cell carcinoma (BIONIKK): A biomarker-driven, open-label, non-comparative, randomised, phase 2 trial. Lancet Oncol. 2022, 23, 612–624. [Google Scholar] [CrossRef]
- Motzer, R.J.; Choueiri, T.K.; McDermott, D.F.; Powles, T.; Vano, Y.A.; Gupta, S.; Yao, J.; Han, C.; Ammar, R.; Papillon-Cavanagh, S.; et al. Biomarker analysis from CheckMate 214: Nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma. J. Immunother. Cancer. 2022, 10, e004316. [Google Scholar] [CrossRef]
- Casanova-Salas, I.; Athie, A.; Boutros, P.C.; Re, M.D.; Miyamoto, D.T.; Pienta, K.J.; Posadas, E.M.; Sowalsky, A.G.; Stenzl, A.; Wyatt, A.W.; et al. Quantitative and Qualitative Analysis of Blood-based Liquid Biopsies to Inform Clinical Decision-making in Prostate Cancer. Eur. Urol. 2021, 79, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Mertens, L.S.; Claps, F.; Mayr, R.; Bostrom, P.J.; Shariat, S.F.; Zwarthoff, E.C.; Boormans, J.L.; Abas, C.; van Leenders, G.J.L.H.; Götz, S.; et al. Prognostic markers in invasive bladder cancer: FGFR3 mutation status versus P53 and KI-67 expression: A multi-center, multi-laboratory analysis in 1058 radical cystectomy patients. Urol. Oncol. 2022, 40, 110.e1–100.e9. [Google Scholar] [CrossRef]
- Yazgan, S.C.; Yekeduz, E.; Utkan, G.; Urun, Y. Prognostic role of pan-immune-inflammation value in patients with metastatic castration-resistant prostate cancer treated with androgen receptor-signaling inhibitors. Prostate 2022, 82, 1456–1461. [Google Scholar] [CrossRef] [PubMed]
- Puche-Sanz, I.; Rodriguez-Martinez, A.; Garrido-Navas, M.C.; Robles-Fernandez, I.; Vazquez-Alonso, F.; Alvarez-Cubero, M.J.; Lorente-Acosta, J.A.; Serrano-Fernandez, M.J.; Cozar-Olmo, J.M. Liquid biopsy and prostate cancer. Current evidence applied to clinical practice. Actas Urol. Esp. 2020, 44, 139–147. [Google Scholar] [CrossRef]
- Ghadjar, P.; Hayoz, S.; Genitsch, V.; Zwahlen, D.R.; Holscher, T.; Gut, P.; Guckenberger, M.; Hildebrandt, G.; Muller, A.C.; Putora, P.M.; et al. Importance and outcome relevance of central pathology review in prostatectomy specimens: Data from the SAKK 09/10 randomized trial on prostate cancer. BJU Int. 2017, 120, 45. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.I.; Soeterik, T.; Puche-Sanz, I.; Broggi, G.; Lo Giudice, A.; De Nunzio, C.; Lombardo, R.; Marra, G.; Gandaglia, G. Oncological outcomes of cribriform histology pattern in prostate cancer patients: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2022, in press. [Google Scholar] [CrossRef]
- Soeterik, T.F.W.; Hueting, T.A.; Israel, B.; van Melick, H.H.E.; Dijksman, L.M.; Stomps, S.; Biesma, D.H.; Koffijberg, H.; Sedelaar, M.; Witjes, J.A.; et al. External validation of the Memorial Sloan Kettering Cancer Centre and Briganti nomograms for the prediction of lymph node involvement of prostate cancer using clinical stage assessed by magnetic resonance imaging. BJU Int. 2021, 128, 236–243. [Google Scholar] [CrossRef]


{kind=link}
| Variables | |
|---|---|
| Age (year, median, IQR) | 68 (64–72) |
| Body mass index (median, IQR) | 23.7 (21.8–25.7) |
| ECOG Performance Status (number, %) | |
| 0 | 1800 (97.0) |
| 1 | 51 (2.7) |
| 2 | 4 (0.2) |
| Initial PSA (ng/mL, median, IQR) | 8.1 (5.8–12.2) |
| Prostate volume (cc, median, IQR) | 30.0 (22.8–39.4) |
| Number of biopsy cores (median, IQR) | 10 (10–13) |
| Number of positive cores (median, IQR) | 4 (2–5) |
| Number of negative cores (median, IQR) | 8 (6–10) |
| Biopsy Gleason Grade (number, %) 1 2 3 4 5 | 182 (9.8) 572 (30.8) 442 (23.8) 488 (26.3) 171 (9.2) |
| Clinical T stage (number, %) | |
| T1c | 326 (17.6) |
| T2a | 770 (41.5) |
| T2b | 198 (10.7) |
| T2c | 364 (19.6) |
| T3a | 179 (9.7) |
| T3b | 18 (1.0) |
| Hemoglobin (g/dL, median, IQR) | 14.5 (13.8–15.2) |
| C-reactive protein (mg/dL, median, IQR) | 0.06 (0.03–0.11) |
| NLR (median, IQR) | 2.01 (1.52–2.71) |
| PLR (median, IQR) | 125 (97.1–163) |
| SII (median, IQR) | 417 (294–579) |
| Pelvic lymphadenectomy (number, %) Limited Standard Extended | 1312 (70.7) 214 (11.5) 320 (17.3) |
| Removed and examined lymph nodes count (median, IQR) | 7 (4–11) |
| Pathological Gleason Grade (number, %) 1 2 3 4 5 | 182 (9.8) 572 (30.8) 442 (23.8) 488 (26.3) 171 (9.2) |
| Pathological T stage (number, %) T2 T3 T4 | 1206 (65.0) 641 (34.6) 7 (0.4) |
| Positive surgical margin (number, %) | 632 (34.1) |
| Lymph node involvement (number, %) | 93 (5.0) |
| Variables | Odds Ratio | 95% Confidence Interval | p Value |
|---|---|---|---|
| Age | 1.02 | 0.75–1.38 | 0.910 |
| Body mass index | 0.95 | 0.69–1.30 | 0.748 |
| ECOG-PS | 2.19 | 0.26–18.52 | 0.470 |
| Initial PSA | 1.25 | 1.11–1.40 | <0.001 |
| Prostate volume | 1.08 | 0.82–1.41 | 0.58 |
| Number of positive cores | 1.43 | 1.13–1.80 | 0.003 |
| Number of negative cores | 0.80 | 0.59–1.09 | 0.156 |
| Biopsy Gleason Grade | 3.17 | 2.02–4.99 | <0.001 |
| Clinical T stage 2a † | 4.59 | 1.07–19.6 | 0.04 |
| Clinical T stage 2b † | 5.32 | 1.14–24.8 | 0.003 |
| Clinical T stage 2c † | 1.75 | 0.37–8.43 | 0.483 |
| Clinical T stage 3a † | 10.05 | 2.27–44.47 | 0.002 |
| Clinical T stage 3b † | 24.71 | 4.06–150.29 | <0.001 |
| Hemoglobin | 1.03 | 0.77–1.38 | 0.853 |
| C-reactive protein | 0.98 | 0.69–1.30 | 0.748 |
| NLR | 0.93 | 0.59–1.48 | 0.765 |
| PLR | 1.00 | 0.67–1.50 | 0.999 |
| SII | 0.98 | 0.67–1.44 | 0.909 |
| Nomogram Cutoff | Patient below Cutoff with pN1 | Patient below Cutoff with pN0 | Negative Predictive Value |
|---|---|---|---|
| 6% | 2 | 492 | 99.6% |
| 10% | 8 | 767 | 99.0% |
| 15% | 16 | 1041 | 98.5% |
| 20% | 23 | 1227 | 98.2% |
| 25% | 30 | 1362 | 97.8% |
| 30% | 39 | 1466 | 97.4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawase, M.; Ebara, S.; Tatenuma, T.; Sasaki, T.; Ikehata, Y.; Nakayama, A.; Toide, M.; Yoneda, T.; Sakaguchi, K.; Ishihara, T.; et al. A Nomogram for Predicting Prostate Cancer with Lymph Node Involvement in Robot-Assisted Radical Prostatectomy Era: A Retrospective Multicenter Cohort Study in Japan (The MSUG94 Group). Diagnostics 2022, 12, 2545. https://doi.org/10.3390/diagnostics12102545
Kawase M, Ebara S, Tatenuma T, Sasaki T, Ikehata Y, Nakayama A, Toide M, Yoneda T, Sakaguchi K, Ishihara T, et al. A Nomogram for Predicting Prostate Cancer with Lymph Node Involvement in Robot-Assisted Radical Prostatectomy Era: A Retrospective Multicenter Cohort Study in Japan (The MSUG94 Group). Diagnostics. 2022; 12(10):2545. https://doi.org/10.3390/diagnostics12102545
Chicago/Turabian StyleKawase, Makoto, Shin Ebara, Tomoyuki Tatenuma, Takeshi Sasaki, Yoshinori Ikehata, Akinori Nakayama, Masahiro Toide, Tatsuaki Yoneda, Kazushige Sakaguchi, Takuma Ishihara, and et al. 2022. "A Nomogram for Predicting Prostate Cancer with Lymph Node Involvement in Robot-Assisted Radical Prostatectomy Era: A Retrospective Multicenter Cohort Study in Japan (The MSUG94 Group)" Diagnostics 12, no. 10: 2545. https://doi.org/10.3390/diagnostics12102545