

Probabilistic Approach to COVID-19 Data Analysis and Forecasting Future Outbreaks Using a Multi-Layer Perceptron Neural Network
 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
Key Contributions
- Awareness about emerging variants of COVID-19: We have collected information about COVID-19 including its types and emerging variants. It is important to note that some of the variants can appear without any prior symptoms.
- Literature review: This article gives a brief overview of the related work recently undertaken in the field of COVID-19 forecasting using data mining approaches including machine learning, and deep learning techniques.
- Proposed Methodology: We proposed an artificial neural network-based methodology for the statistical analysis of the current pandemic situation in some eastern and western countries. The results show that our approach works well in terms of precision and model fitting to statistical data.
- Challenges and future directions: We discussed the current issues associated with utilizing Artificial Intelligence methods to resolve the COVID-19 pandemic. Furthermore, we demonstrate how machine learning and deep learning can assist in preventing the spread of COVID-19 in the future. We also address the potential future contributions of AI and blockchain-based solutions to analyze the outbreak response.
2. Coronavirus
2.1. Symptoms of COVID-19
- Temperature or chills
- Runny nose
- Coughing
- Breathing problems
- Fatigue
- Aches in the muscles or throughout the body
- Loss of smell or taste
- Diarrhea
- Sore throat
- Nausea or vomiting
2.2. Types of Coronavirus
- Flu-like without a temperatureFatigue, muscle aches, absence of smell, sore throat, coughing, shortness of breath, and no temperature are some of the additional symptoms.
- Flu-like with temperatureFatigue, absence of smell, sore throat, coughing, uncontrollable shaking, a decrease in hunger, and a temperature.
- GastrointestinalFatigue, absence of smell, sore throat, a decrease in hunger, chest pain, no coughing, and diarrhea.
- Extreme level one, severe exhaustionFatigue, loss of smell, cough, chest pain, a temperature, and hoarseness.
- Extreme level two, misconception (uncertainty)Fatigue, absence of smell, a decrease in hunger, coughing, sore throat, chest pain, a temperature, hoarseness, muscle pain, and confusion.
- Extreme level three, abdominal and pulmonaryFatigue, absence of smell, a decrease in hunger, coughing, sore throat, chest pain, a temperature, hoarseness, and muscle pain.
2.3. Emerging Variants of COVID-19
2.4. Variants of Interest (VOI)
2.5. Variants under Observation
3. Related Work
4. Methods
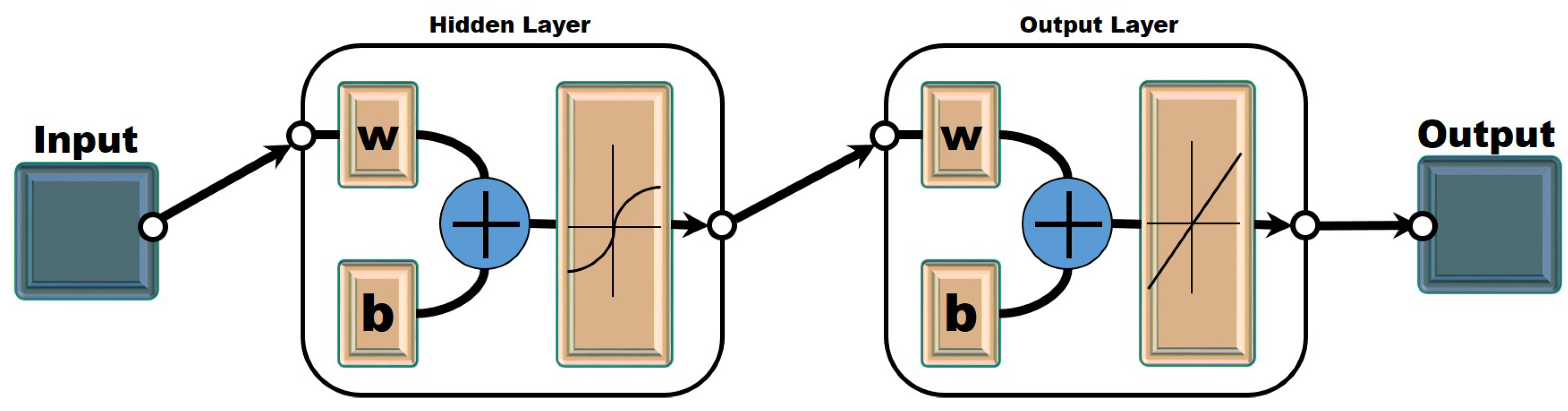
4.1. Multi-Layer Perceptron Neural Network
4.2. Mortality/Fatality Rate
4.3. Cronbach’s Alpha
4.4. Mean Absolute Error (MAE)
4.5. Mean Absolute Scaled Error (MASE)
4.6. Symmetric Mean Absolute Percentage Error (SMAPE)
4.7. Root Mean Square Error (RMSE)
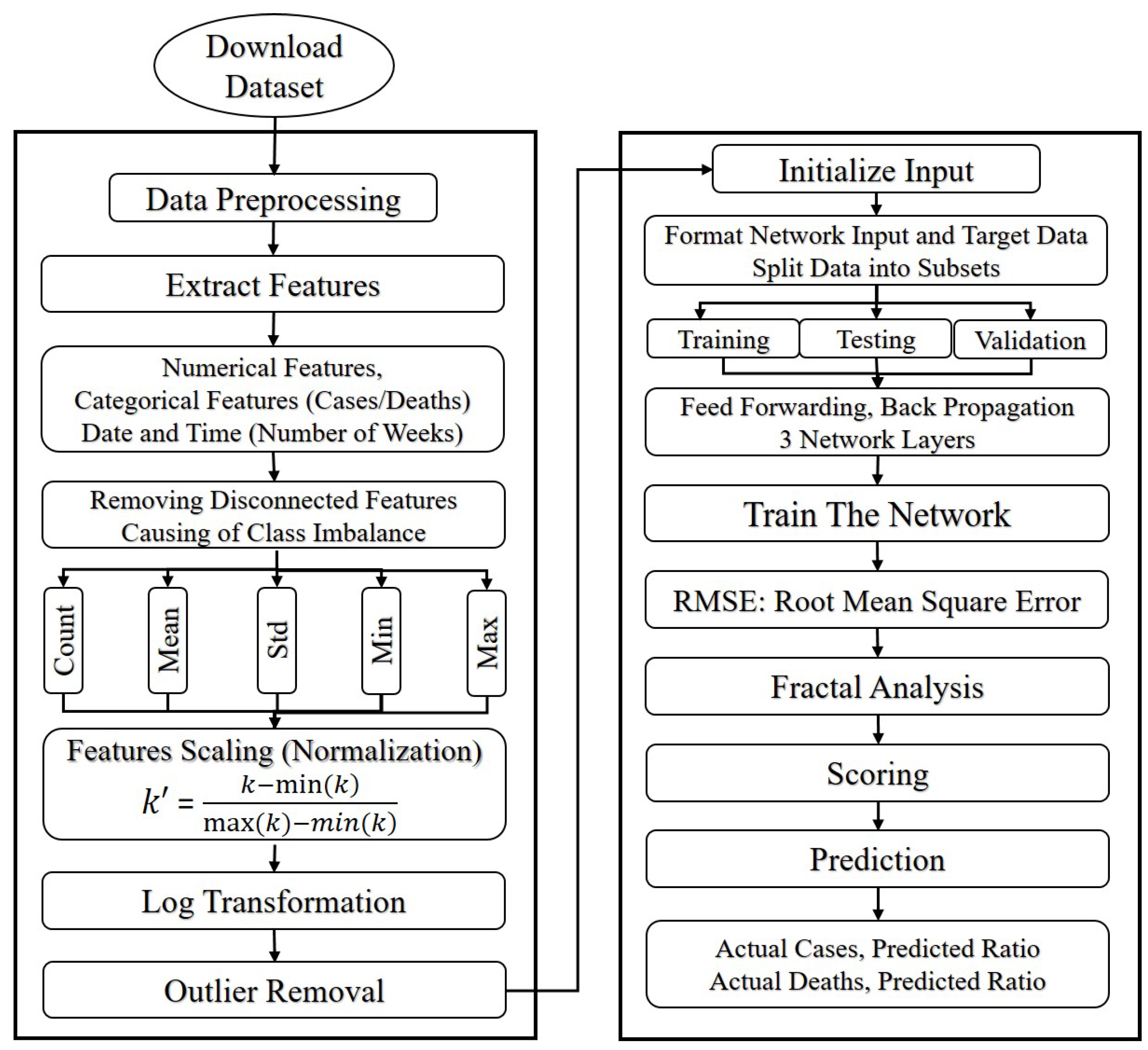
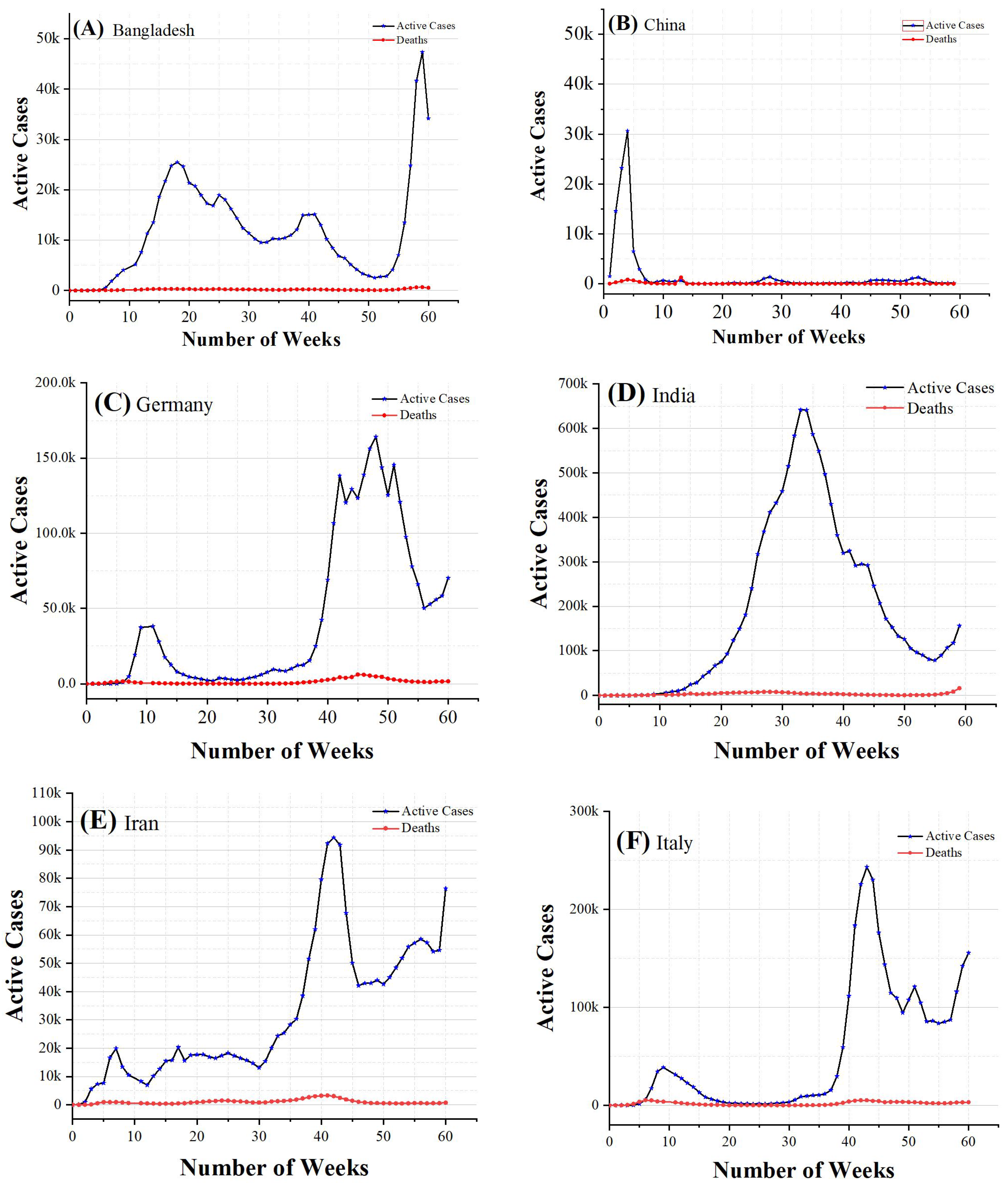
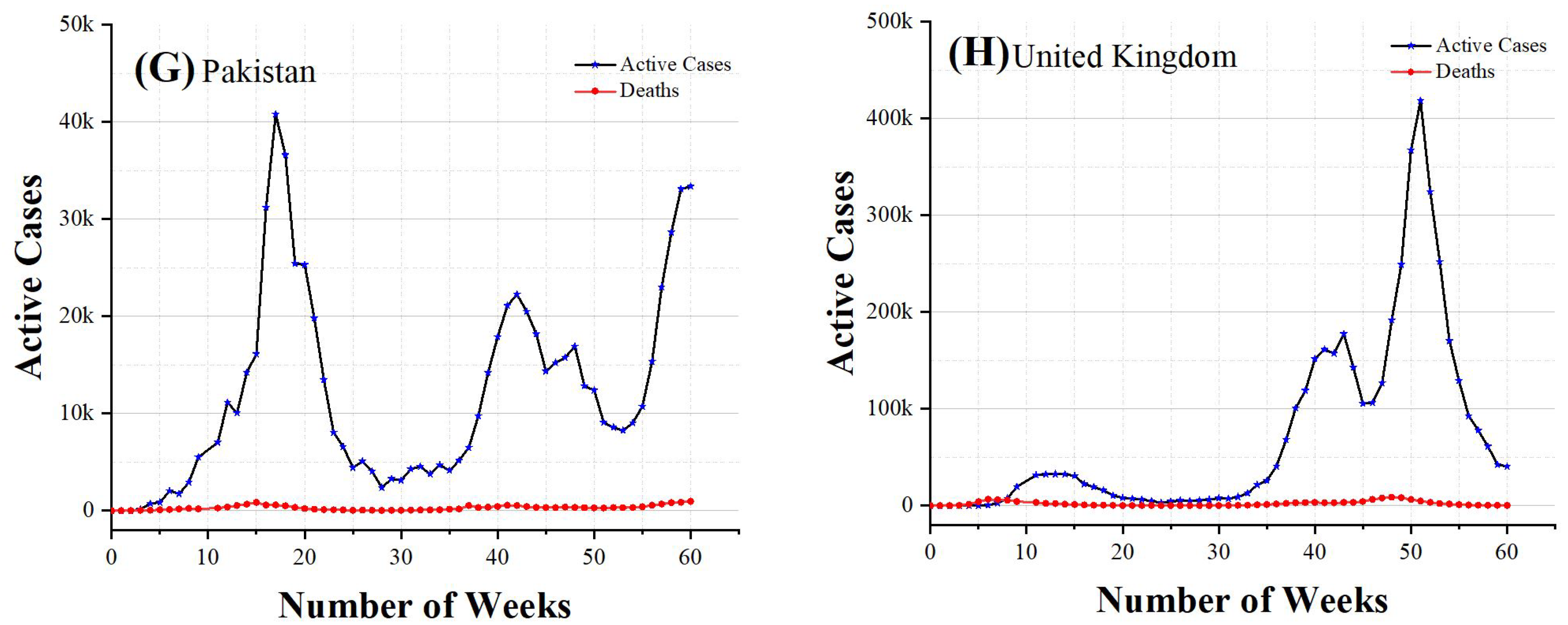
4.8. Data Pre-Processing and Experimental Setup
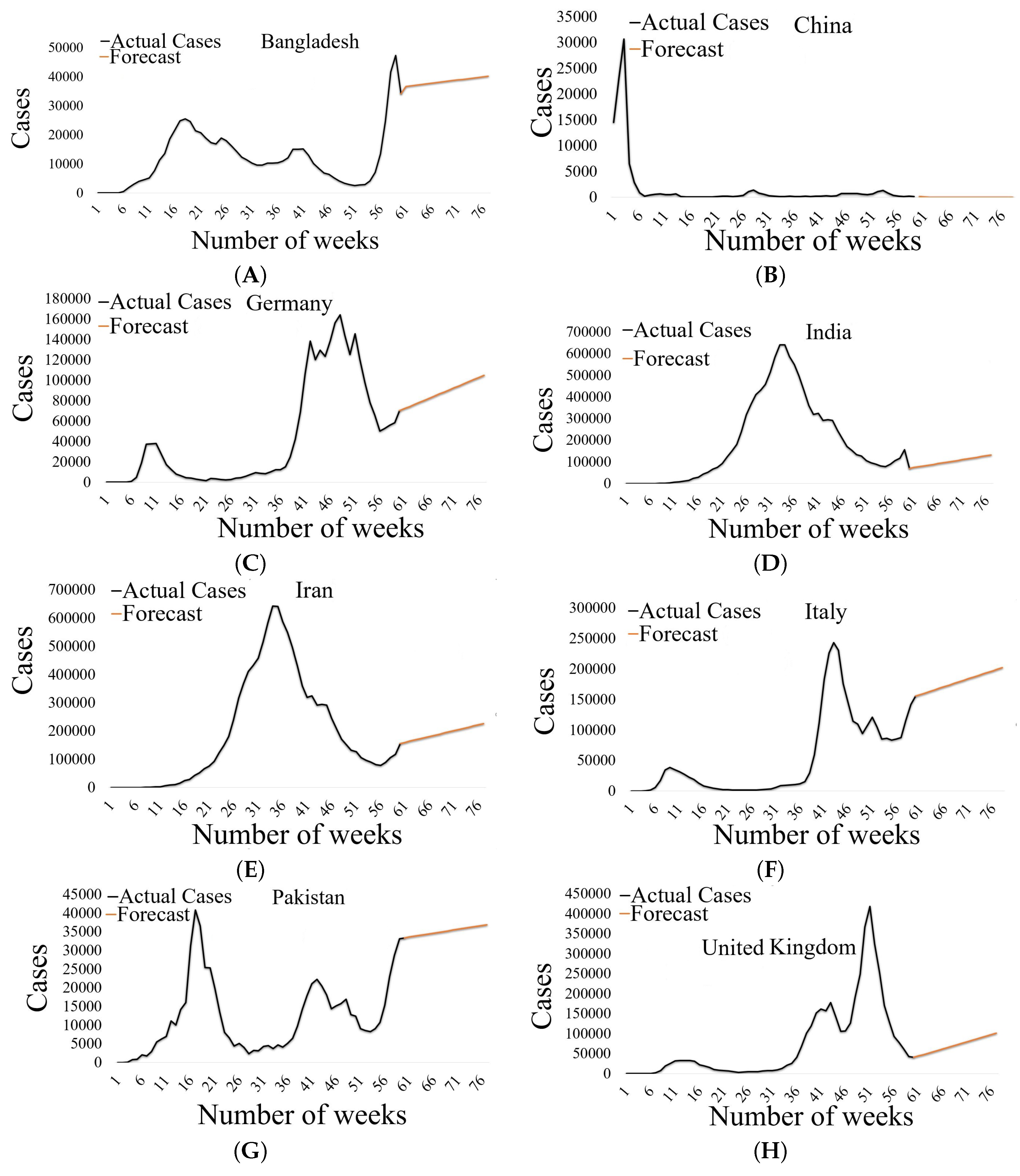
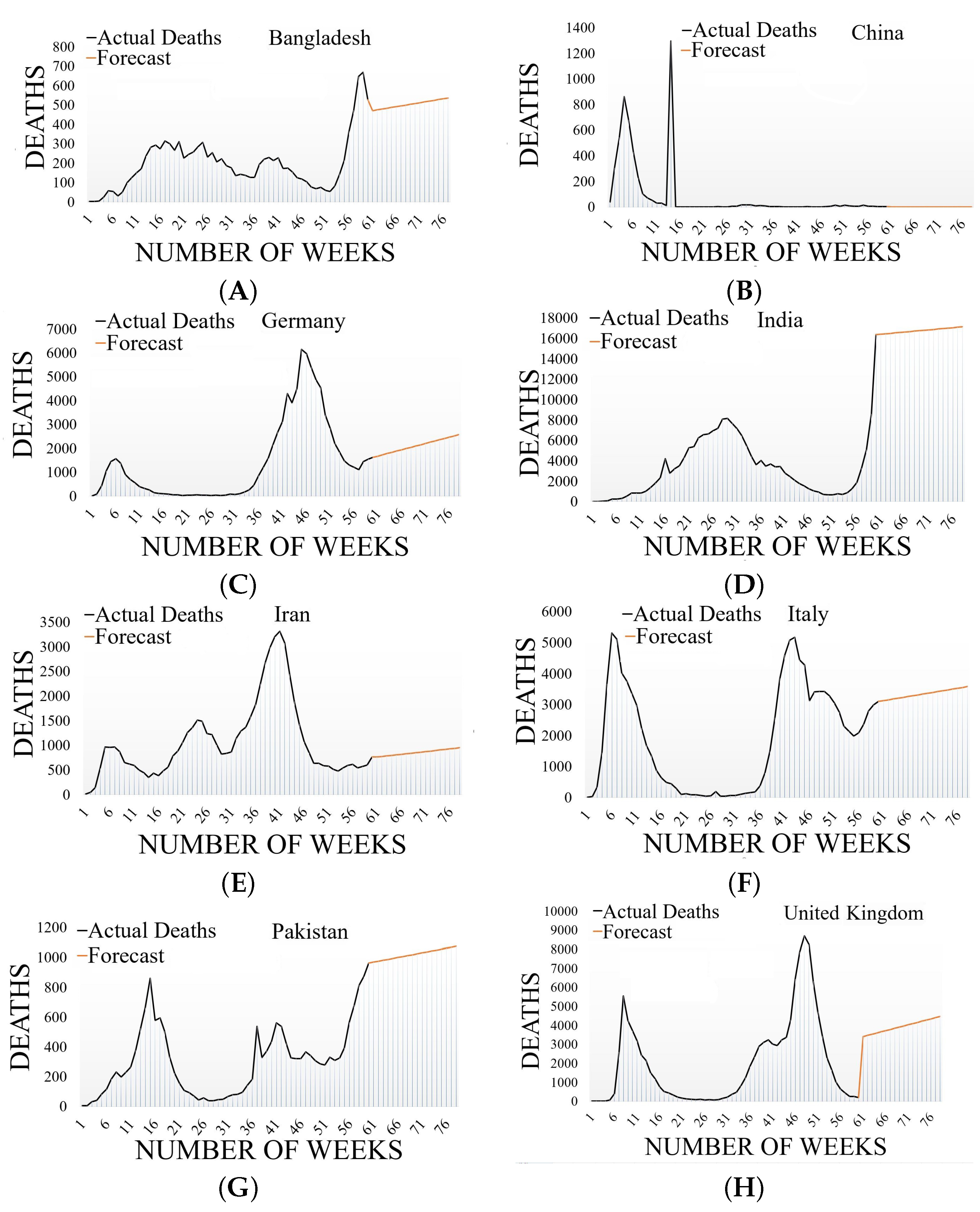
4.9. Model Forecasting
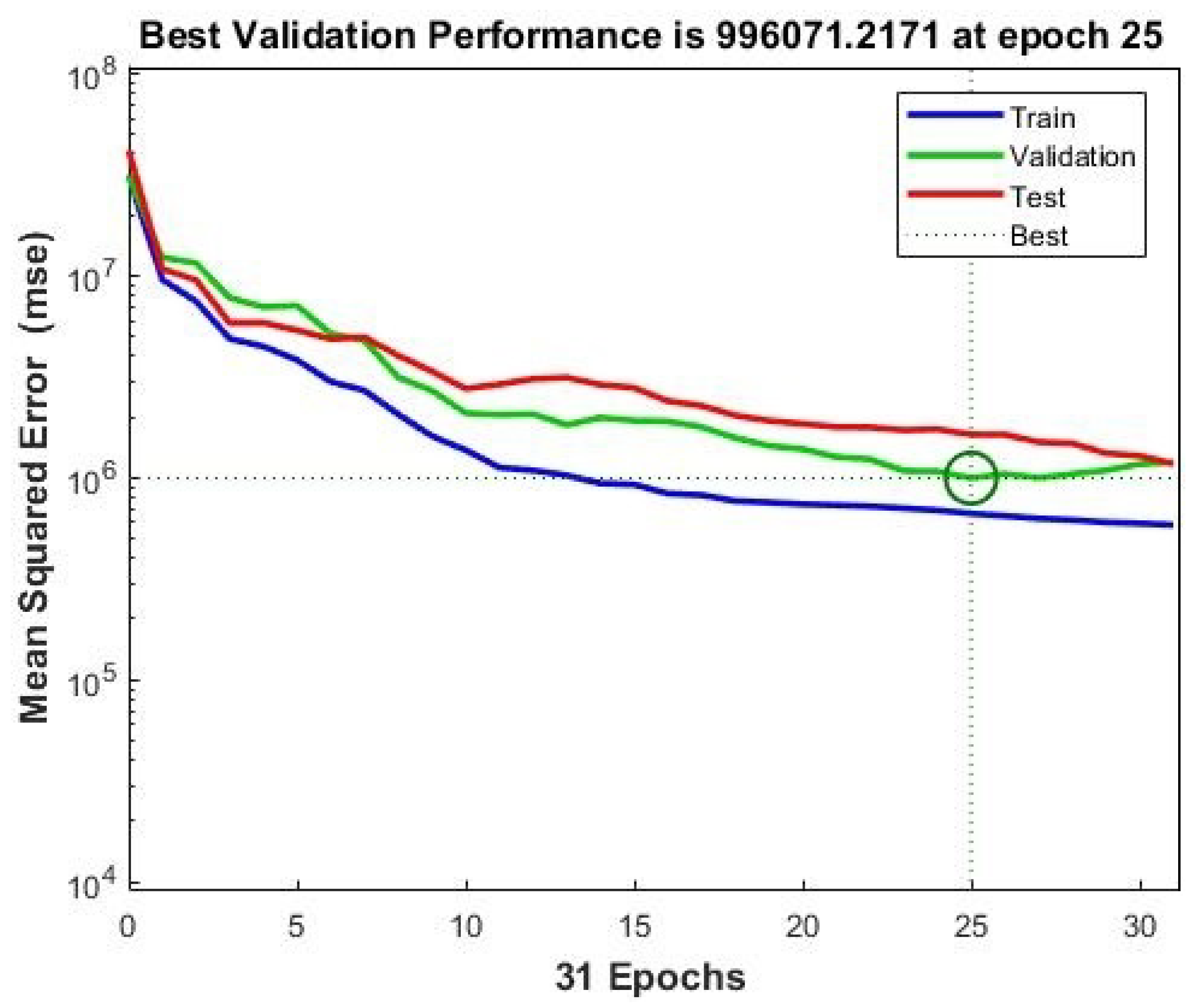
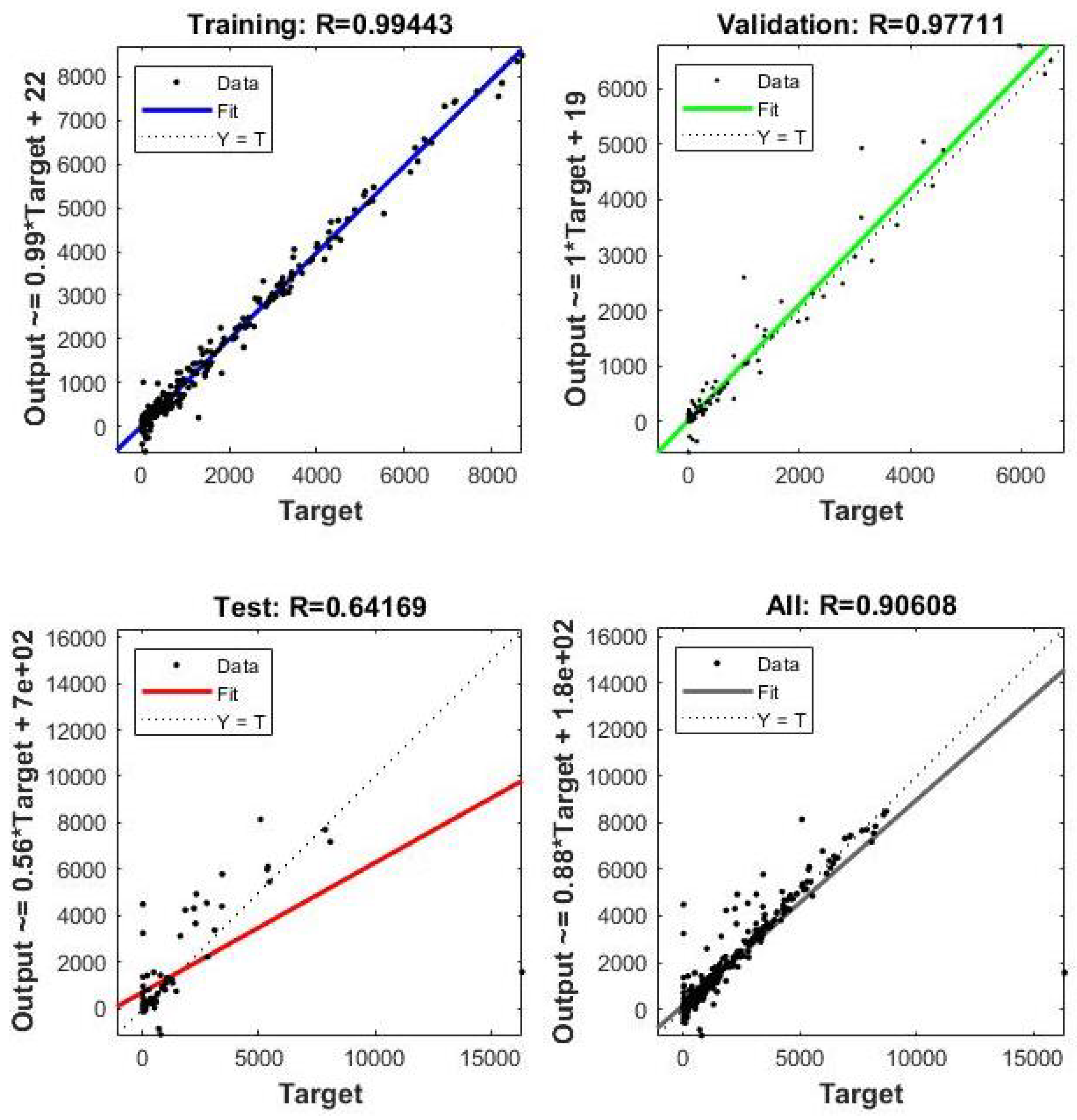
4.10. The Model’s Performance
5. Challenges and Future Directions
5.1. Challenges
5.2. Future Research Direction
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Burgess, S.; Sievertsen, H.H. Schools, Skills, and Learning: The Impact of COVID-19 on Education. 2020. Available online: https://cepr.org/voxeu/columns/schools-skills-and-learning-impact-covid-19-education (accessed on 12 January 2021).
- Fernandes, N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. SSRN Electron. J. 2020, 2, 1–33. [Google Scholar] [CrossRef]
- Bellan, M.; Patti, G.; Hayden, E.; Azzolina, D.; Pirisi, M.; Acquaviva, A.; Aimaretti, G.; Valletti, P.A.; Angilletta, R.; Arioli, R.; et al. Fatality rate and predictors of mortality in an Italian cohort of hospitalized COVID-19 patients. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Cheng, J.; Jiang, Y.; Liu, K. A time delay dynamic system with external source for the local outbreak of 2019-nCoV. Appl. Anal. 2020, 101, 146–157. [Google Scholar] [CrossRef] [Green Version]
- Noh, J.; Danuser, G. Estimation of the fraction of COVID-19 infected people in U.S. states and countries worldwide. PLoS ONE 2021, 16, e0246772. [Google Scholar] [CrossRef] [PubMed]
- Böhning, D.; Rocchetti, I.; Maruotti, A.; Holling, H. Estimating the undetected infections in the Covid-19 outbreak by harnessing capture–recapture methods. Int. J. Infect. Dis. 2020, 97, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus infections—More than just the common cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Tomar, A.; Gupta, N. Prediction for the spread of COVID-19 in India and effectiveness of preventive measures. Sci. Total Environ. 2020, 728, 138762. [Google Scholar] [CrossRef]
- Feroze, N. Forecasting the patterns of COVID-19 and causal impacts of lockdown in top five affected countries using Bayesian Structural Time Series Models. Chaos Solitons Fractals 2020, 140, 110196. [Google Scholar] [CrossRef]
- Greaney, A.J.; Loes, A.N.; Crawford, K.H.D.; Starr, T.N.; Malone, K.D.; Chu, H.Y.; Bloom, J.D. Comprehensive mapping of mutations in the SARS-CoV-2 receptor-binding domain that affect recognition by polyclonal human plasma antibodies. Cell Host Microbe 2021, 29, 463–476. [Google Scholar] [CrossRef]
- Silva, R.F.; Xavier, F.; Saraiva, A.M.; Cugnasca, C.E. Unsupervised machine learning and pandemics spread: The case of COVID-19. In Proceedings of the 20th Brazilian Symposium on Computing Applied to Healthcare (SBCAS2020), SBC, Virtual, 18–22 October 2020; pp. 506–511. [Google Scholar] [CrossRef]
- Khan, R.U.; Hussain, S.M.; Ul Haq, A.; Asif, M.; Yousaf, M.; Zafar, A.; Almakdi, S.; Li, J.; Malghani, M.A. Forecasting Time Series COVID-19 Statistical Data with Auto-Regressive Integrated Moving Average and Box-Jenkins’ Models. In Proceedings of the 18th International Computer Conference on Wavelet Active Media Technology and Information Processing (ICCWAMTIP), Chengdu, China, 17–19 December 2022; pp. 353–358. [Google Scholar] [CrossRef]
- Zakary, O.; Larrache, A.; Rachik, M.; Elmouki, I. Effect of awareness programs and travel-blocking operations in the control of HIV/AIDS outbreaks: A multi-domains SIR model. Adv. Differ. Equ. 2016, 2016, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Khaleque, A.; Sen, P. An empirical analysis of the Ebola outbreak in West Africa. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godio, A.; Pace, F.; Vergnano, A. SEIR modeling of the Italian epidemic of SARS-CoV-2 using computational swarm intelligence. Int. J. Environ. Res. Public Health 2020, 17, 3535. [Google Scholar] [CrossRef] [PubMed]
- Baleanu, D.; Mohammadi, H.; Rezapour, S. A fractional differential equation model for the COVID-19 transmission by using the Caputo–Fabrizio derivative. Adv. Differ. Equ. 2020, 2020, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Ullah, A.; Shah, K.; Salahshour, S.; Ahmadian, A.; Ciano, T. Fuzzy fractional-order model of the novel coronavirus. Adv. Differ. Equ. 2020, 2020, 1–17. [Google Scholar] [CrossRef]
- Salahshour, S.; Ahmadian, A.; Pansera, B.A.; Ferrara, M. Uncertain inverse problem for fractional dynamical systems using perturbed collage theorem. Commun. Nonlinear Sci. Numer. Simul. 2021, 94, 105553. [Google Scholar] [CrossRef]
- Meng, F.; Uversky, V.N.; Kurgan, L. Comprehensive review of methods for prediction of intrinsic disorder and its molecular functions. Cell. Mol. Life Sci. 2017, 74, 3069–3090. [Google Scholar] [CrossRef] [PubMed]
- Al-Qaness, M.A.A.; Ewees, A.A.; Fan, H.; Abd El Aziz, M. Optimization method for forecasting confirmed cases of COVID-19 in China. J. Clin. Med. 2020, 9, 674. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wang, Z.; Qu, H.; Liu, S. Optimal forecast combination based on neural networks for time series forecasting. Appl. Soft Comput. 2018, 66, 1–17. [Google Scholar] [CrossRef]
- Eriksson, T.A.; Bülow, H.; Leven, A. Applying neural networks in optical communication systems: Possible pitfalls. IEEE Photonics Technol. Lett. 2017, 29, 2091–2094. [Google Scholar] [CrossRef] [Green Version]
- King Abdullah Petroleum Studies and Research Center. Saudi Arabia Coronavirus Disease (COVID-19) Situation—Demographics; King Abdullah Petroleum Studies and Research Center: Riyadh, Saudi Arabia, 2021. [Google Scholar]
- Tilahun, S.L.; Ong, H.C. Prey-predator algorithm: A new metaheuristic algorithm for optimization problems. Int. J. Inf. Technol. Decis. Mak. 2015, 14, 1331–1352. [Google Scholar] [CrossRef]
- Public Health England. SARS-CoV-2 Variants of Concern and Variants under Investigation in England-Technical Briefing 11; Technical report; Public Health England: London, UK, 2021. [Google Scholar]
- Public Health England. SARS-CoV-2 Variants of Concern and Variants under Investigation in England-Technical Briefing 12; Technical report; Public Health England: London, UK, 2021. [Google Scholar]
- ECDC. SARS-CoV-2 Variants of Concern as of 5 August 2021; ECDC: Solna, Sweden, 2021. [Google Scholar]
- Callaway, E. Heavily mutated coronavirus variant puts scientists on alert. Nature 2021, 600, 21. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Communicable Diseases. New COVID-19 Variant Detected in South Africa-NICD; National Institute for Communicable Diseases: Johannesburg, South Africa, 2021. [Google Scholar]
- Focosi, D.; Tuccori, M.; Baj, A.; Maggi, F. SARS-CoV-2 Variants: A Synopsis of In Vitro Efficacy Data of Convalescent Plasma, Currently Marketed Vaccines, and Monoclonal Antibodies. Viruses 2021, 13, 1211. [Google Scholar] [CrossRef] [PubMed]
- Aarts, M.; Dekker, M.; de Vries, S.; van der Wal, A.; te Riele, H. Generation of a mouse mutant by oligonucleotide-mediated gene modification in ES cells. Nucleic Acids Res. 2006, 34, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health England. Confirmed Cases of COVID-19 Variants Identified in UK-GOV.UK; Public Health England: London, UK, 2021. [Google Scholar]
- Collier, D.A.; De Marco, A.; Ferreira, I.A.; Meng, B.; Datir, R.P.; Walls, A.C.; Kemp, S.A.; Bassi, J.; Pinto, D.; Silacci-Fregni, C.; et al. Sensitivity of SARS-CoV-2 B. 1.1. 7 to mRNA vaccine-elicited antibodies. Nature 2021, 593, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.G.; Jarvis, C.I.; Edmunds, W.J.; Jewell, N.P.; Diaz-Ordaz, K.; Keogh, R.H. Increased mortality in community-tested cases of SARS-CoV-2 lineage B. 1.1. 7. Nature 2021, 593, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Tut, G.; Lancaster, T.; Krutikov, M.; Sylla, P.; Bone, D.; Kaur, N.; Spalkova, E.; Bentley, C.; Amin, U.; Jadir, A.; et al. Profile of Humoral and Cellular Immune Responses to Single BNT162b2 or ChAdOx1 Vaccine in Residents and Staff within Residential Care Homes (VIVALDI): An observational study. Lancet Healthy Longev. 2021, 2, E544–E553. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 vaccines against the B. 1.617. 2 (delta) variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Aziz, S.; Jim, M.; Bob, T.; Chris, R. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated transmissibility and impact of SARS-CoV-2 lineage B. 1.1. 7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]
- Tegally, H.; Wilkinson, E.; Giovanetti, M.; Iranzadeh, A.; Fonseca, V.; Giandhari, J.; Doolabh, D.; Pillay, S.; San, E.J.; Msomi, N.; et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature 2021, 592, 438–443. [Google Scholar] [CrossRef]
- Cele, S.; Gazy, I.; Jackson, L.; Hwa, S.H.; Tegally, H.; Lustig, G.; Giandhari, J.; Pillay, S.; Wilkinson, E.; Naidoo, Y.; et al. Escape of SARS-CoV-2 501Y. V2 from neutralization by convalescent plasma. Nature 2021, 593, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Baillie, V.; Cutland, C.L.; Voysey, M.; Koen, A.L.; Fairlie, L.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 vaccine against the B. 1.351 variant. N. Engl. J. Med. 2021, 384, 1885–1898. [Google Scholar] [CrossRef]
- Carl AB Pearson; Russell, T.W.; Davies, N.G.; Kucharski, A.J.; CMMID COVID-19 working group; Edmunds, W.J.; Eggo, R.M. Estimates of Severity and Transmissibility of Novel South Africa SARS-CoV-2 Variant 501Y.V2. Working Paper. Available online: https://cmmid.github.io/topics/covid19/sa-novel-variant.html (accessed on 19 March 2021).
- Funk, T.; Pharris, A.; Spiteri, G.; Bundle, N.; Melidou, A.; Carr, M.; Gonzalez, G.; Garcia-Leon, A.; Crispie, F.; O’Connor, L.; et al. Characteristics of SARS-CoV-2 variants of concern B. 1.1. 7, B. 1.351 or P. 1: Data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Eurosurveillance 2021, 26, 2100348. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.U.; Haq, A.U.; Hussain, S.M.; Ullah, S.; Almakdi, S.; Kumar, R.; Shah, H.H.; Li, J. Analyzing and Battling The Emerging Variants Of Covid-19 Using Artificial Neural Network And Blockchain. In Proceedings of the 18th International Computer Conference on Wavelet Active Media Technology and Information Processing (ICCWAMTIP), Chengdu, China, 16–18 December 2022; pp. 101–105. [Google Scholar] [CrossRef]
- Al-Qaness, M.A.; Ewees, A.A.; Fan, H.; Abualigah, L.; Elaziz, M.A. Marine Predators Algorithm for Forecasting Confirmed Cases of COVID-19 in Italy, USA, Iran and Korea. Int. J. Environ. Res. Public Health 2020, 17, 3520. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, A.; Sadir, H.; Kamil, R.; Sari, H. Prediction of Epidemic Peak and Infected Cases for COVID-19 Disease in Malaysia, 2020. Int. J. Environ. Res. Public Health 2020, 17, 4076. [Google Scholar] [CrossRef]
- Behnood, A.; Mohammadi Golafshani, E.; Hosseini, S.M. Determinants of the infection rate of the COVID-19 in the U.S. using ANFIS and virus optimization algorithm (VOA). Chaos Solitons Fractals 2020, 139, 110051. [Google Scholar] [CrossRef]
- Arora, P.; Kumar, H.; Panigrahi, B.K. Prediction and analysis of COVID-19 positive cases using deep learning models: A descriptive case study of India. Chaos Solitons Fractals 2020, 139, 110017. [Google Scholar] [CrossRef]
- Fokas, A.S.; Dikaios, N.; Kastis, G.A. Mathematical models and deep learning for predicting the number of individuals reported to be infected with SARS-CoV-2. J. R. Soc. Interface 2020, 17, 1–12. [Google Scholar] [CrossRef]
- Yadav, R.S. Data analysis of COVID-2019 epidemic using machine learning methods: A case study of India. Int. J. Inf. Technol. 2020, 12, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kang, J.; Kim, D.; Song, H.; Min, H.; Nam, Y.; Park, D.; Lee, J.G. Hi-COVIDNet: Deep Learning Approach to Predict Inbound COVID-19 Patients and Case Study in South Korea. In Proceedings of the ACM SIGKDD International Conference on Knowledge Discovery and Data Mining. Association for Computing Machinery, Virtual, 6–10 July 2020; pp. 3466–3473. [Google Scholar] [CrossRef]
- Abbasimehr, H.; Paki, R. Prediction of COVID-19 confirmed cases combining deep learning methods and Bayesian optimization. Chaos Solitons Fractals 2021, 142, 110511. [Google Scholar] [CrossRef]
- Worldometer. COVID-19-Coronavirus Pandemic Weekly Trends. 2021. Available online: https://www.worldometers.info/coronavirus/weekly-trends (accessed on 10 June 2021).
- Hamadneh, N.N.; Tahir, M.; Khan, W.A. Using Artificial Neural Network with Prey Predator Algorithm for Prediction of the COVID-19: The Case of Brazil and Mexico. Mathematics 2021, 9, 180. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef] [Green Version]
- Alshehri, M.; Panda, B.; Alazeb, A.; Halawani, H.; Al Mudawi, N.; Khan, R.U.; Lera, I.; Juiz, C. A Novel Blockchain-Based Encryption Model to Protect Fog Nodes from Behaviors of Malicious Nodes. Electronics 2021, 10, 3135. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scientific Name | Name Given by the WHO | Spike Protein Substitutions | Attributes |
|---|---|---|---|
| 70del, A570D, | 1. 50% higher spread capability | ||
| B..1.1.7 | Alpha | 69del, | 2. Possible enhanced severity based |
| (S494P), | on hospital admissions and case | ||
| (E484K), | mortality rates | ||
| P681H, 144del, | 3. Treatment with EUA monoclonal | ||
| N501Y, D614G, | antibodies has no effect on | ||
| T716I, D1118H, | susceptibility | ||
| S982A | 4. Minimal effect on recovery and | ||
| (K1191N) | post-vaccination serum | ||
| neutralizing | |||
| A701V, D215G, | 1. higher spread capability | ||
| B.1.351 | Beta | D614G, D80A, | 2. Susceptibility to a combination |
| E484K, | of bamlanivimab and etesevimab | ||
| N501Y, | monoclonal antibody treatment | ||
| K417N, | was drastically lowered; however, | ||
| 241del | there are other EUA monoclonal | ||
| 242del | antibody treatments available | ||
| 243del | 3. Condensed neutralization by | ||
| convalescent and post-vaccination sera | |||
| D138Y, D614G, | 1. Susceptibility to the combination | ||
| P.1 | Gamma | E484K, H655Y, | of bamlanivimab and etesevimab |
| K417T, L18F, | monoclonal antibody treatment was | ||
| N501Y, P26S | drastically lowered; however, there | ||
| R190S, T20N, | are other EUA monoclonal antibody | ||
| T1027I | treatments available | ||
| 2. Condensed neutralization by convalescent | |||
| and post-vaccination sera | |||
| T95I, G142D, | 1. Higher spread capability | ||
| B.1.617.2 | Delta | T19R, (V70F), | 2. Possible decrease in neutralization |
| R158G, (A222V), | by some EUA monoclonal antibody | ||
| E156-, F157-, | treatments | ||
| D614G, D950N, | 3. Possible decrease in neutralization | ||
| (W258L), (K417N) | by post-vaccination sera | ||
| P681R, L452R, | |||
| T478K |
| Labeled by the WHO | Additional Variations in the Lineage | Country First Discovered | Spike Changes of Interest | Date of First Detection | Influence on Transmissibility | Possibility of a Negative Effect on Immunity | Transmission in Europe |
|---|---|---|---|---|---|---|---|
| Eta | E484K | Nigeria | Q677H | December 2020 | – | Neutralization (m) [33] | Communities |
| D614G | |||||||
| B.1.525 | |||||||
| Epsilon | B.1.429, | United States | D614G | September 2020 | Ambiguous [26] | Neutralization (v) [26] | Inconsistent/Travels |
| B.1.427 | L452R | ||||||
| Theta | P.3 | Philippine | D614G | January 2021 | Yes (m) [34] | Neutralization (m) [33] | Inconsistent/Travels |
| E484K | |||||||
| P681H | |||||||
| N501Y | |||||||
| B.1.616 | France | D614G | February 2021 | Recognition (c) [25] | – | One-Time Occurrence | |
| G669S | |||||||
| H655Y | |||||||
| V483A | |||||||
| Kappa | B.1.617.1 | India | D614G | December 2020 | Yes (v) [35] | Neutralization (v) [25,36] | Multiple Occurrences |
| E484Q | |||||||
| L452R | |||||||
| P681R | |||||||
| B.1.620 | Not clear | D614G | February 2021 | Neutralization (m) [33,37] | Multiple Occurrences | ||
| E484K | |||||||
| P681H | |||||||
| S477N | |||||||
| B.1.621 | Colombia | D614G | January 2021 | Yes (m) [34] | Neutralization (m) [33] | Inconsistent/Travels | |
| E484K | |||||||
| P681H | |||||||
| N501Y | |||||||
| R346K |
| Labeled by the WHO | Additional Variations in the Lineage | Country First Discovered | Spike Changes of Interests | Date of First Detection | Influence on Transmitability | Possibility of a Negative Effect on Immunity | Proof of Link to Intensity | Transmission in Europe |
|---|---|---|---|---|---|---|---|---|
| B.1.617.3 | India | D614G | February 2021 | Yes (m) [34] | Neutralization (m) [26,33] | – | Not found | |
| E484Q | ||||||||
| L452R | ||||||||
| P681R | ||||||||
| B.1.214.2 | not clear (b) | D614G | December 2020 | – | – | – | found (a) | |
| ins214TDR | ||||||||
| N450K | ||||||||
| Q414K | ||||||||
| A.23.1+E484K | UK | E484K | December 2020 | – | Neutralization (m) [33] | – | found (a) | |
| Q613H | ||||||||
| V367F | ||||||||
| A.27 | not clear (b) | A653V | December 2020 | Yes (m) [34] | Neutralization (m) [26] | – | found (a) | |
| N501Y | ||||||||
| L452R | ||||||||
| H655Y | ||||||||
| A.28 | not clear (b) | E484K | October 2020 | – | Neutralization (m) [33] | – | found (a) | |
| H655Y | ||||||||
| N501T | ||||||||
| C.16 | not clear (b) | L452R | December 2020 | – | Neutralization (m) [33] | – | found (a) | |
| D614G | ||||||||
| Labmda | C.37 | Peru | D614G | December 2020 | – | – | – | found (a) |
| F490S | ||||||||
| L452Q | ||||||||
| B.1.351+P384L | South Africa | A701V | December 2020 | Yes (v) [39] | Escape (v) [40,41] | not clear [42] | found (a) | |
| D614G | ||||||||
| E484K | ||||||||
| K417N | ||||||||
| N501Y | ||||||||
| P384L | ||||||||
| B.1.351+E516Q | not clear (b) | A701V | January 2021 | Yes (v) [39] | Escape (v) [40,41] | not clear [42] | found (a) | |
| D614G | ||||||||
| E484K | ||||||||
| E516Q | ||||||||
| K417N | ||||||||
| N501Y | ||||||||
| B.1.1.7+L452R | UK | D614G | January 2021 | Yes (v) [34] | Neutralization (m) [26] | Yes (v) [43] | found (a) | |
| L452R | ||||||||
| P681H | ||||||||
| N501Y | ||||||||
| B.1.1.7+S494P | UK | D614G | January 2021 | Yes (v) [34] | Neutralization (m) [36] | Yes (v) [43] | found (a) | |
| N501Y | ||||||||
| P681H | ||||||||
| S494P | ||||||||
| C.36+L452R | Egypt | D614G | December 2020 | – | Neutralization (m) [26] | – | found (a) | |
| L452R | ||||||||
| Q677H | ||||||||
| AT.1 | Russia | D614G | January 2021 | – | Neutralization (m) [33] | – | found (a) | |
| E484K | ||||||||
| ins679GIAL | ||||||||
| N679K | ||||||||
| Iota | B.1.526 | US | A701V | December 2020 | – | Neutralization (m) [33] | – | found (a) |
| D614G | ||||||||
| E484K | ||||||||
| B.1.526.1 | US | D614G | October 2020 | – | Neutralization (m) [26] | – | found (a) | |
| L452R | ||||||||
| B.1.526.2 | US | D614G | December 2020 | – | – | – | found (a) | |
| S477N | ||||||||
| B.1.1.318 | not clear (b) | D614G | January 2021 | – | Neutralization (m) [33] | – | found (a) | |
| E484K | ||||||||
| P681H | ||||||||
| Zeta | P.2 | Brazil | D614G | January 2021 | – | Neutralization (m) [33] | – | found (a) |
| E484K | ||||||||
| B.1.1.519 | Mexico | D614G | November 2020 | – | Neutralization (m) [26] | – | found (a) | |
| T478K | ||||||||
| AV.1 | UK | D614G | March 2021 | – | Neutralization (m) [33] | – | found (a) | |
| E484K | ||||||||
| P681H | ||||||||
| N439K | ||||||||
| P.1+P681H | Italy | D614G | February 2021 | – | not clear | – | – | |
| H655Y | ||||||||
| E484K | ||||||||
| N501Y | ||||||||
| P681H | ||||||||
| K417T |
| Countries | CFR (%) |
|---|---|
| Bangladesh | 1.58 |
| India | 1.17 |
| China | 5.33 |
| Pakistan | 2.25 |
| Iran | 2.75 |
| Germany | 2.39 |
| Italy | 2.99 |
| United Kingdom | 2.85 |
| World-wide | 2.08 |
| Country | Alpha | MASE | SMAPE | MAE | RMSE |
|---|---|---|---|---|---|
| Bangladesh | 0.5 | 5 | 0.47 | 66,660.96 | 10,128.56 |
| China | 0.9 | 0.15 | 0.45 | 205.99 | 270.5 |
| Germany | 0.25 | 3.2 | 0.34 | 19,705.31 | 22,740.67 |
| India | 1 | 0.86 | 0.2 | 20,950.76 | 30,570.1 |
| Iran | 1 | 0.59 | 0.14 | 14,199.15 | 18,578.85 |
| Italy | 1 | 1.33 | 0.12 | 12,815.17 | 15,552.92 |
| Pakistan | 1 | 0.97 | 0.17 | 2418.55 | 2875.24 |
| United Kingdom | 0.1 | 15.74 | 0.69 | 135,707.55 | 152,719.52 |
| Country | Alpha | MASE | SMAPE | MAE | RMSE |
|---|---|---|---|---|---|
| Bangladesh | 0.25 | 5.3 | 0.58 | 137.17 | 180.56 |
| China | 0.25 | 0.23 | 2 | 21.05 | 21.6 |
| Germany | 1 | 0.88 | 0.13 | 213.27 | 313.1 |
| India | 0.1 | 6.04 | 0.8 | 2508.59 | 4225.44 |
| Iran | 0.9 | 0.28 | 0.09 | 52.28 | 64.89 |
| Italy | 1 | 0.45 | 0.07 | 176.9 | 199.38 |
| Pakistan | 0.5 | 0.9 | 0.13 | 58.35 | 71.94 |
| United Kingdom | 0 | 5.84 | 1.04 | 2523.59 | 2861.2 |
| Countries | Best Model | MAPE | DFT p-Value * | ACF1 ** |
|---|---|---|---|---|
| Bangladesh | 1,1,0 | 19.22 * | 0.04 | −0.002 |
| China | 5,1,1 | inf * | 0.01 | −0.077 |
| Germany | 1,1,0 | 24.87 | 0.01 | −0.042 |
| India | 0,2,0 | 16.24 * | 0.01 | 0.089 |
| Iran | 0,1,3 | 13.39 * | 0.01 | 0.040 |
| Italy | 4,1,0 | 36.17 | 0.01 | 0.010 |
| Pakistan | 1,1,0 | 18.62 * | 0.01 | −0.078 |
| UK | 2,1,1 | 27.59 | 0.01 | 0.029 |
| World | 1,1,0 | 12.01 | 0.05 | −0.073 |
| Pakistan | Iran | ||||
|---|---|---|---|---|---|
| Month | Week | Point Forecast | CI(Upper) | Point Forecast | CI(Upper) |
| 1 | 1 | 380 | 537 | 1367 | 1732 |
| 2 | 342 | 615 | 1362 | 2070 | |
| 3 | 326 | 696 | 1338 | 2493 | |
| 4 | 320 | 772 | 1338 | 2878 | |
| 2 | 1 | 317 | 842 | 1338 | 3185 |
| 2 | 316 | 905 | 1338 | 3447 | |
| 3 | 316 | 962 | 1338 | 3681 | |
| 4 | 315 | 1016 | 1338 | 3893 | |
| 3 | 1 | 315 | 1065 | 1338 | 4089 |
| 2 | 315 | 1112 | 1338 | 4271 | |
| 3 | 315 | 1156 | 1338 | 4443 | |
| 4 | 315 | 1198 | 1338 | 4606 | |
| 4 | 1 | 315 | 1238 | 1338 | 4762 |
| 2 | 315 | 1276 | 1338 | 4910 | |
| 3 | 315 | 1313 | 1338 | 5053 | |
| 4 | 315 | 1349 | 1338 | 5190 | |
| India | Italy | ||||
| Month | Week | Point Forecast | CI(Upper) | Point Forecast | CI(Upper) |
| 1 | 1 | 30,506 | 32,639 | 714 | 1522 |
| 2 | 31,094 | 35,864 | 697 | 2310 | |
| 3 | 31,682 | 39,664 | 740 | 3164 | |
| 4 | 32,270 | 43,954 | 798 | 3910 | |
| 2 | 1 | 32,858 | 48,679 | 845 | 4500 |
| 2 | 33,446 | 53,796 | 871 | 4944 | |
| 3 | 34,034 | 59,275 | 878 | 5279 | |
| 4 | 34,622 | 65,091 | 872 | 5549 | |
| 3 | 1 | 35,210 | 71,223 | 861 | 5787 |
| 2 | 35,798 | 77,655 | 851 | 6014 | |
| 3 | 36,386 | 84,372 | 845 | 6241 | |
| 4 | 36,974 | 91,361 | 843 | 6469 | |
| 4 | 1 | 37,562 | 98,612 | 844 | 6695 |
| 2 | 38,150 | 106,113 | 846 | 6917 | |
| 3 | 38,738 | 113,858 | 848 | 7132 | |
| 4 | 39,326 | 121,836 | 849 | 7338 | |
| Bangladesh | UK | ||||
| Month | Week | Point Forecast | CI(Upper) | Point Forecast | CI(Upper) |
| 1 | 1 | 198 | 292 | 92 | 978 |
| 2 | 194 | 360 | 122 | 2148 | |
| 3 | 192 | 420 | 140 | 3333 | |
| 4 | 191 | 473 | 145 | 4344 | |
| 2 | 1 | 191 | 520 | 141 | 5122 |
| 2 | 190 | 562 | 133 | 5695 | |
| 3 | 190 | 599 | 126 | 6126 | |
| 4 | 190 | 634 | 122 | 6476 | |
| 3 | 1 | 190 | 667 | 120 | 6790 |
| 2 | 190 | 697 | 121 | 7094 | |
| 3 | 190 | 726 | 123 | 7400 | |
| 4 | 190 | 753 | 125 | 7709 | |
| 4 | 1 | 190 | 779 | 126 | 8015 |
| 2 | 190 | 804 | 126 | 8314 | |
| 3 | 190 | 828 | 126 | 8601 | |
| 4 | 190 | 851 | 126 | 8876 | |
| Germany | China | ||||
| Month | Week | Point Forecast | CI(Upper) | Point Forecast | CI(Upper) |
| 1 | 1 | 881 | 1587 | 1 | 100 |
| 2 | 824 | 2078 | 1 | 204 | |
| 3 | 798 | 2525 | 1 | 277 | |
| 4 | 786 | 2923 | 1 | 354 | |
| 2 | 1 | 780 | 3278 | 1 | 391 |
| 2 | 777 | 3597 | 0 | 400 | |
| 3 | 776 | 3887 | 0 | 404 | |
| 4 | 776 | 4154 | 0 | 404 | |
| 3 | 1 | 775 | 4403 | 0 | 404 |
| 2 | 775 | 4635 | 0 | 412 | |
| 3 | 775 | 4855 | 1 | 427 | |
| 4 | 775 | 5063 | 1 | 458 | |
| 4 | 1 | 775 | 5262 | 1 | 497 |
| 2 | 775 | 5453 | 1 | 522 | |
| 3 | 775 | 5636 | 1 | 539 | |
| 4 | 775 | 5812 | 0 | 545 | |
| World | |||||
| Month | Week | Point Forecast | CI(Upper) | ||
| 1 | 1 | 73,427 | 83,134 | ||
| 2 | 71,635 | 89,025 | |||
| 3 | 70,763 | 94,891 | |||
| 4 | 70,339 | 100,348 | |||
| 2 | 1 | 70,133 | 105,326 | ||
| 2 | 70,032 | 109,863 | |||
| 3 | 69,983 | 114, 019 | |||
| 4 | 69,960 | 117,857 | |||
| 3 | 1 | 69,948 | 121,430 | ||
| 2 | 69,942 | 124,779 | |||
| 3 | 69,940 | 127,941 | |||
| 4 | 69,938 | 130,941 | |||
| 4 | 1 | 69,938 | 133,801 | ||
| 2 | 69,937 | 136,539 | |||
| 3 | 69,937 | 139,169 | |||
| 4 | 69,937 | 141,702 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, R.U.; Almakdi, S.; Alshehri, M.; Kumar, R.; Ali, I.; Hussain, S.M.; Haq, A.U.; Khan, I.; Ullah, A.; Uddin, M.I. Probabilistic Approach to COVID-19 Data Analysis and Forecasting Future Outbreaks Using a Multi-Layer Perceptron Neural Network. Diagnostics 2022, 12, 2539. https://doi.org/10.3390/diagnostics12102539
Khan RU, Almakdi S, Alshehri M, Kumar R, Ali I, Hussain SM, Haq AU, Khan I, Ullah A, Uddin MI. Probabilistic Approach to COVID-19 Data Analysis and Forecasting Future Outbreaks Using a Multi-Layer Perceptron Neural Network. Diagnostics. 2022; 12(10):2539. https://doi.org/10.3390/diagnostics12102539
Chicago/Turabian StyleKhan, Riaz Ullah, Sultan Almakdi, Mohammed Alshehri, Rajesh Kumar, Ikram Ali, Sardar Muhammad Hussain, Amin Ul Haq, Inayat Khan, Aman Ullah, and Muhammad Irfan Uddin. 2022. "Probabilistic Approach to COVID-19 Data Analysis and Forecasting Future Outbreaks Using a Multi-Layer Perceptron Neural Network" Diagnostics 12, no. 10: 2539. https://doi.org/10.3390/diagnostics12102539