
Automatic Cardiopulmonary Endurance Assessment: A Machine Learning Approach Based on GA-XGBOOST

Abstract
:1. Introduction
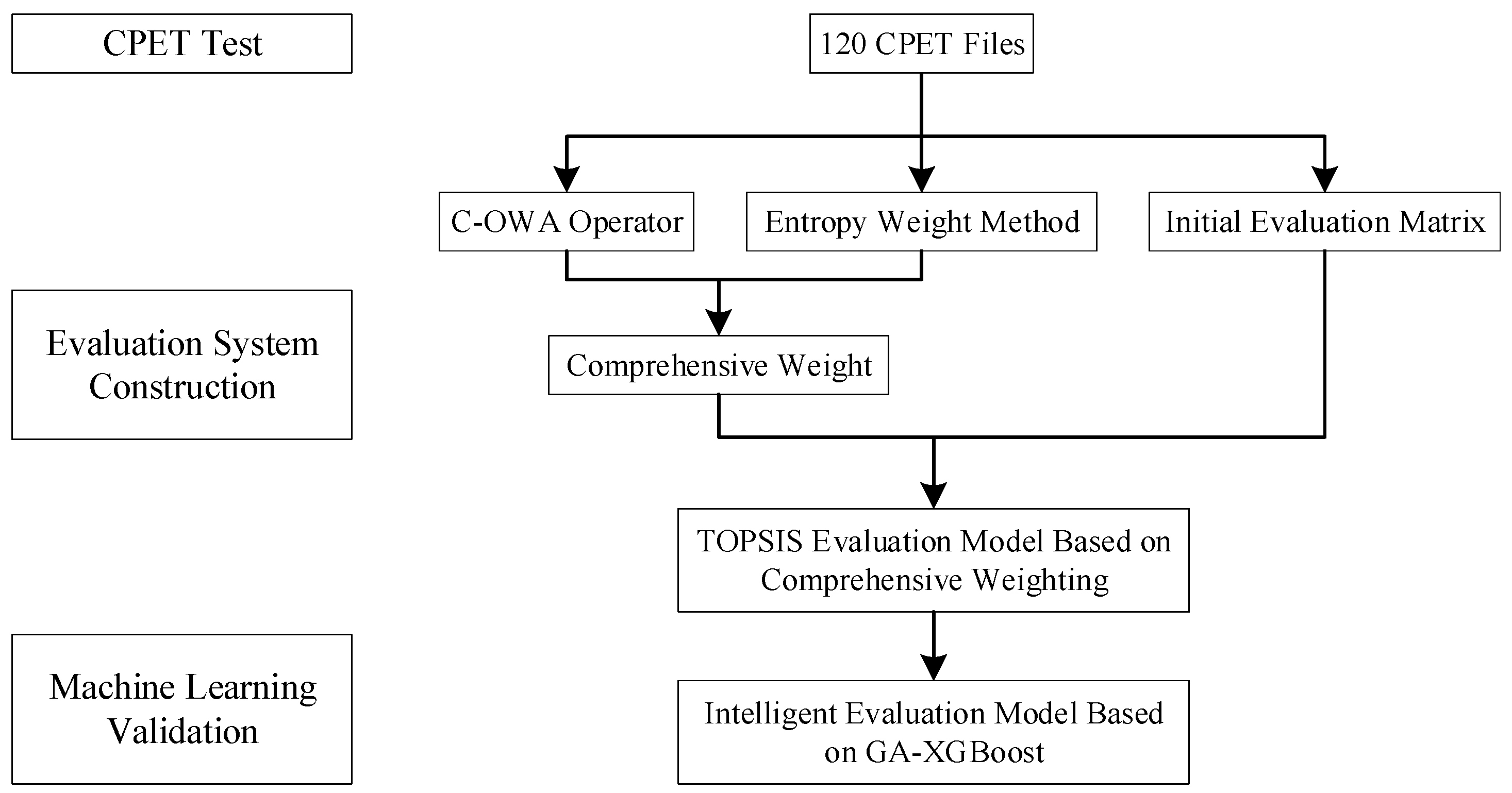
2. Materials and Methods
2.1. Participants
2.2. The Cardiopulmonary Test (CPET)
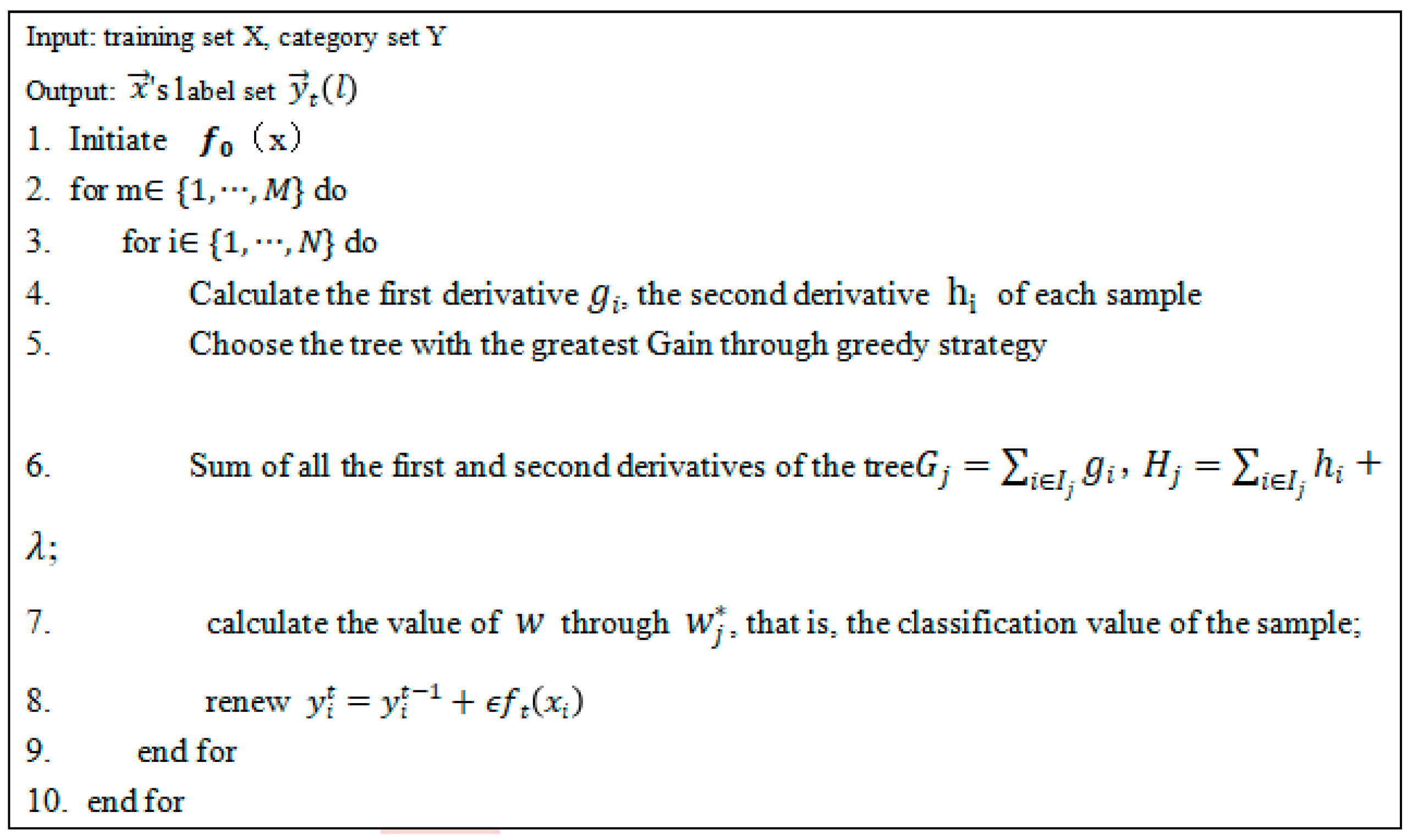
2.3. Algorithms
2.4. Performance Analysis
2.4.1. Tenfold Validation
2.4.2. Statistical Analyses
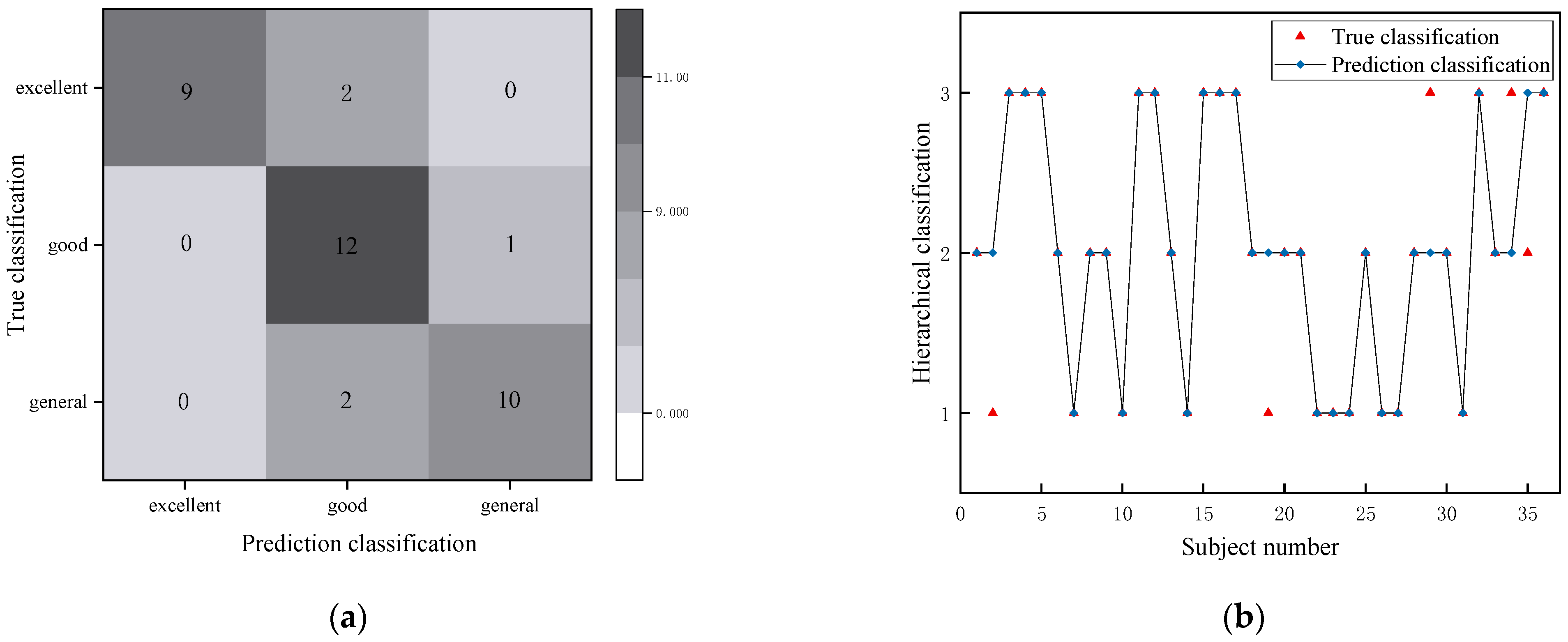
2.4.3. Confusion Matrix
3. Results
3.1. Performance of Classifying Models
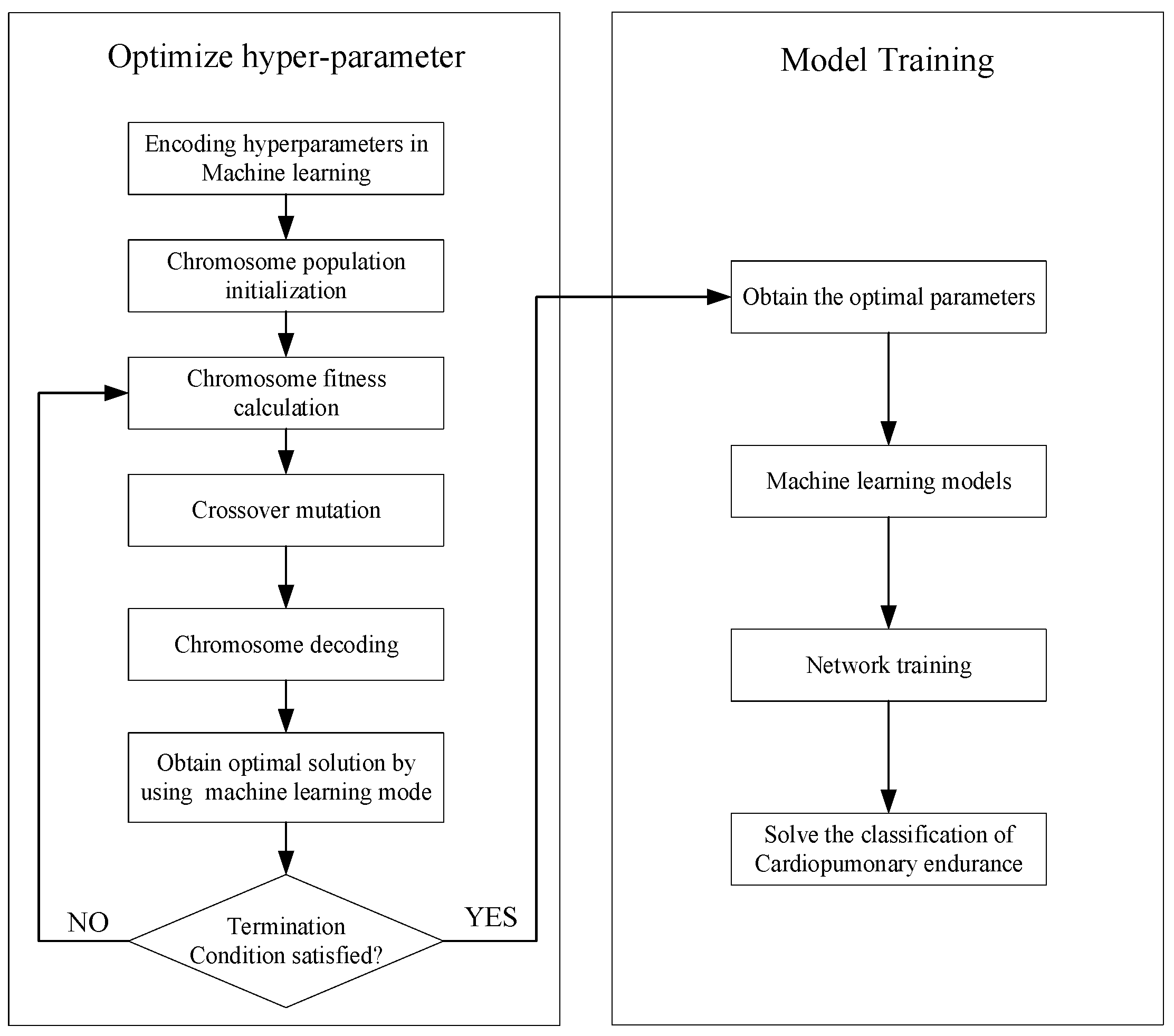
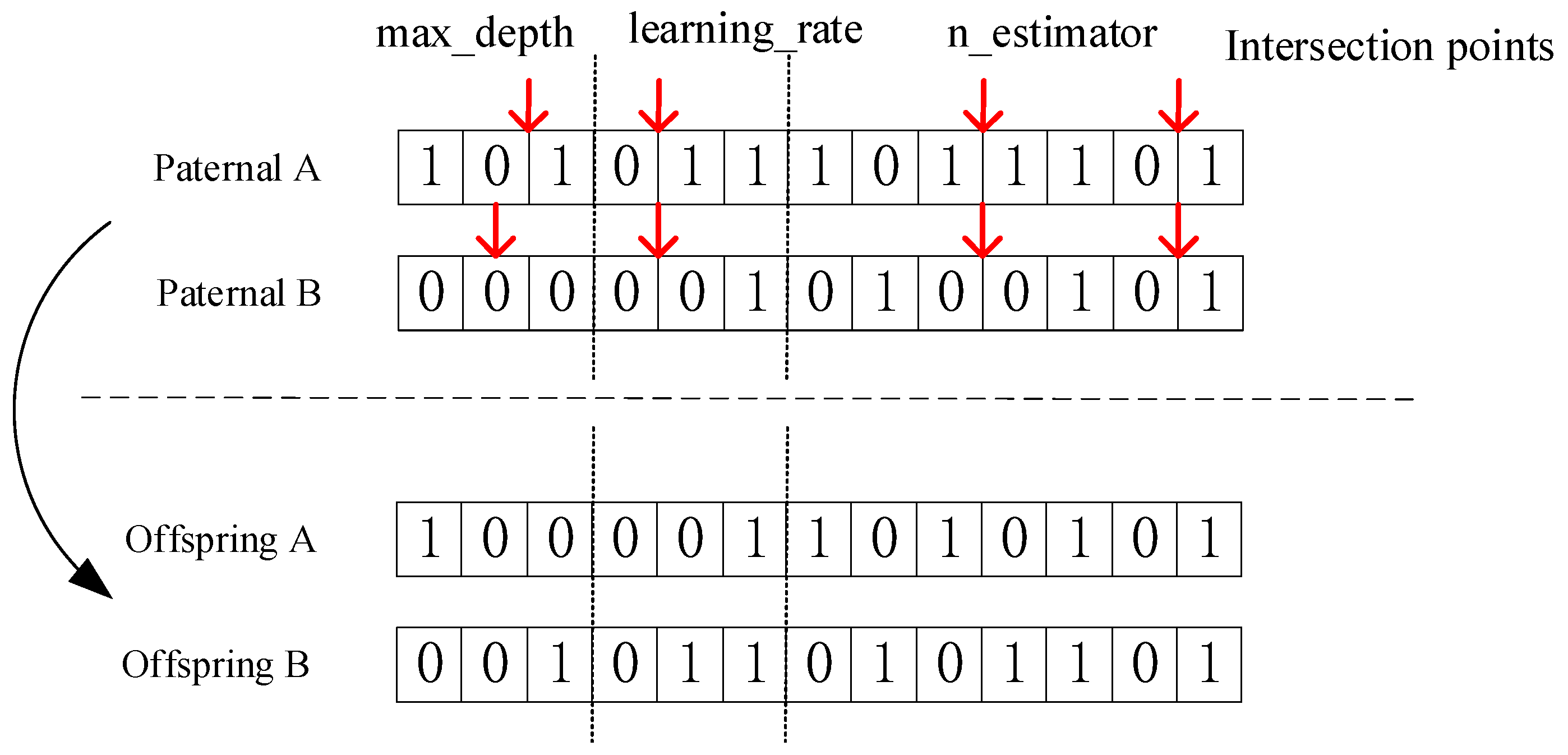
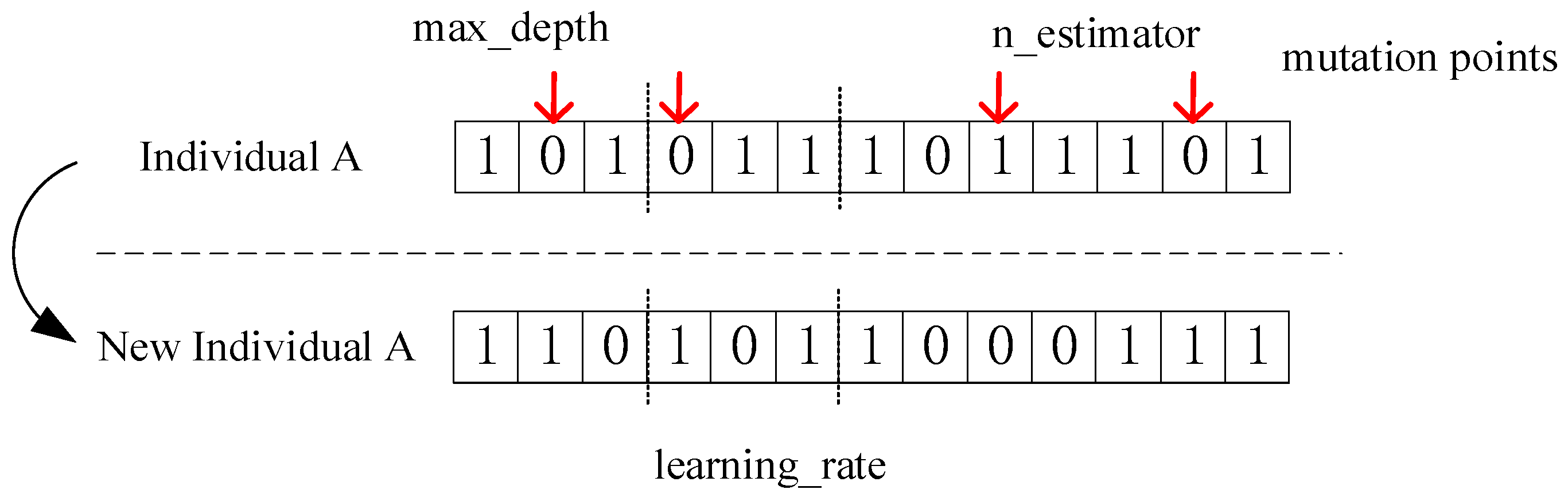
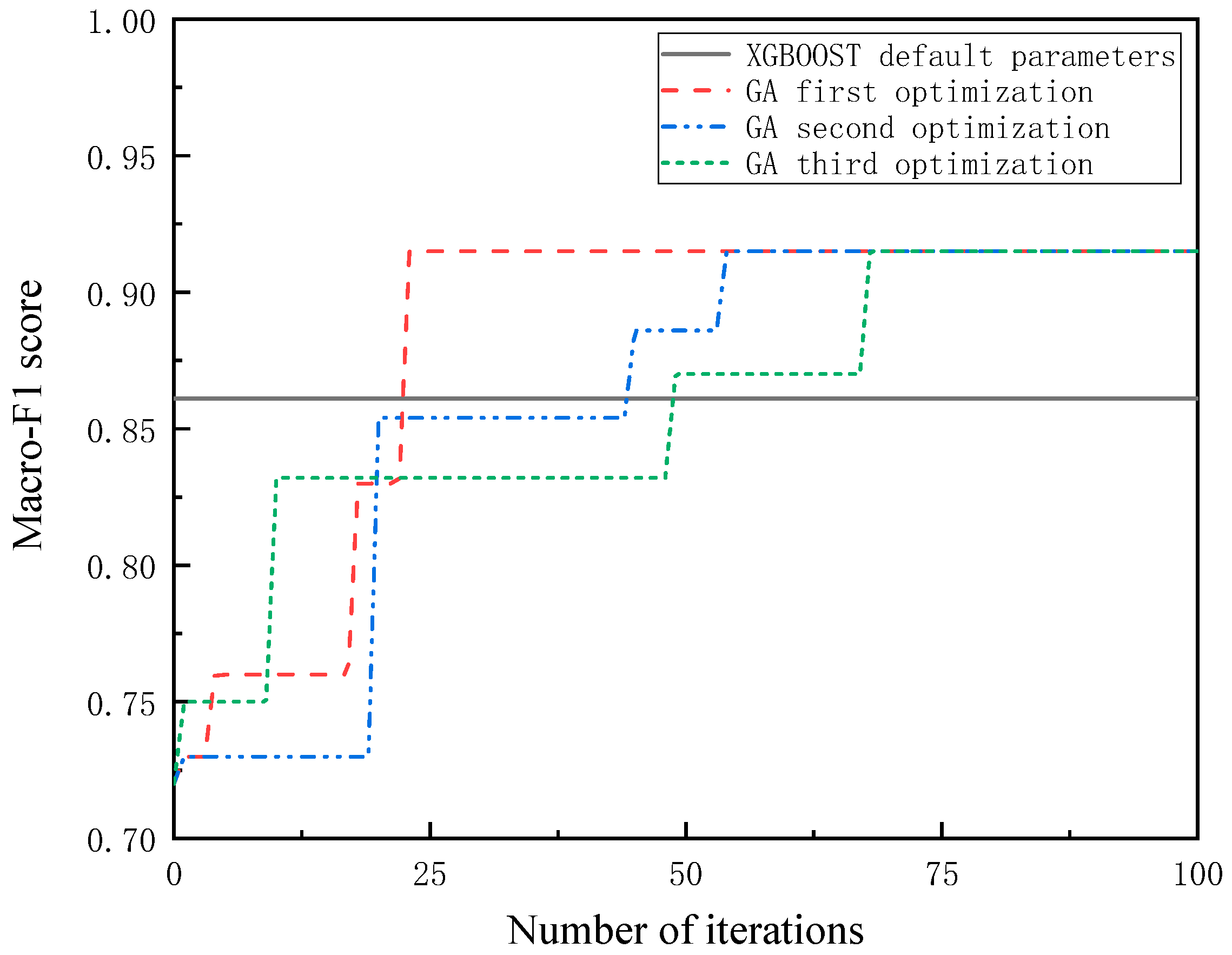
3.2. Hyperparameter Optimization of XGBOOST Based on Genetic Algorithm
- Step 1: Set genetic algorithm parameters
- Step 2: Determine genetic operators
- Step 3: Determine fitness function
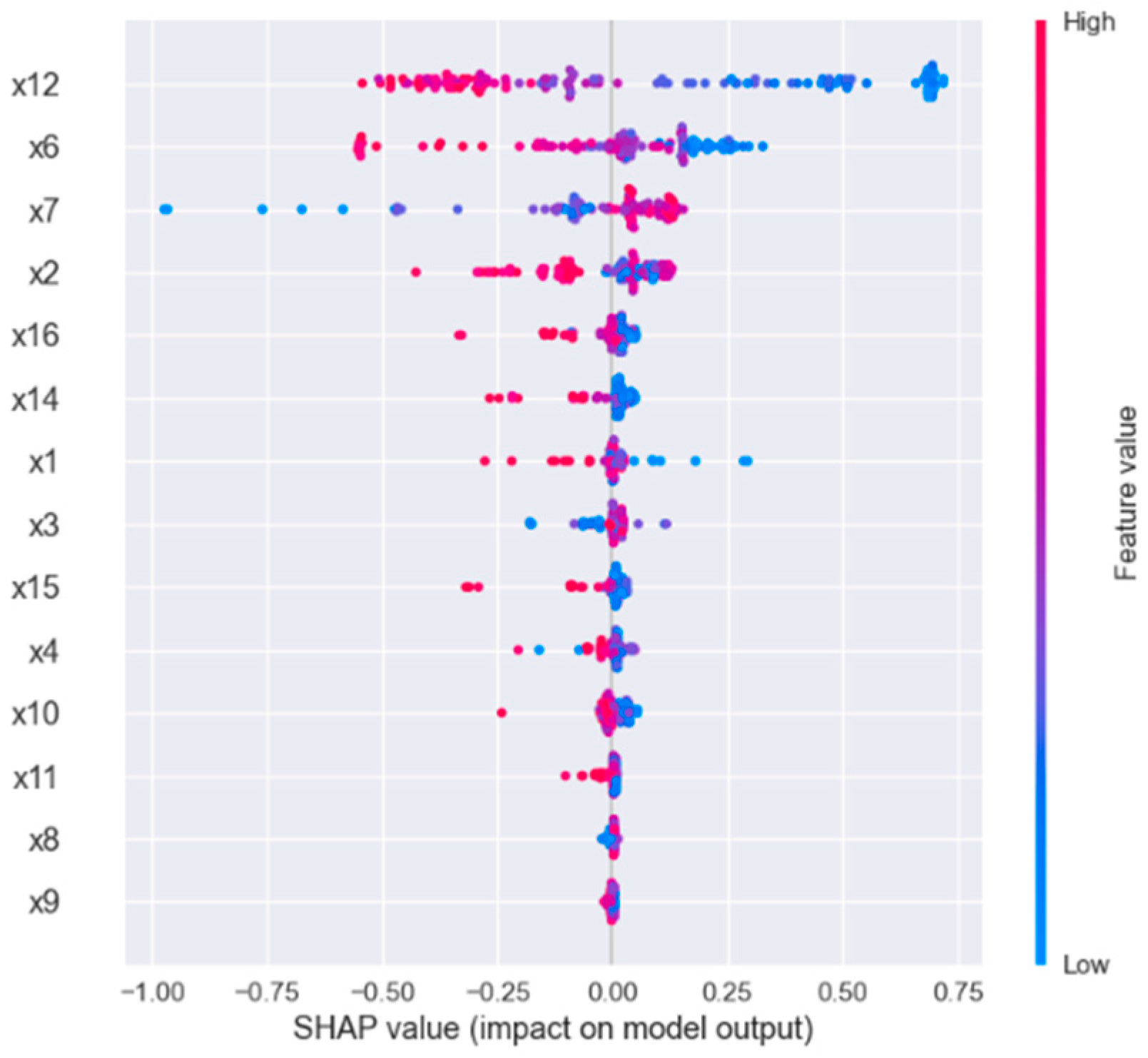
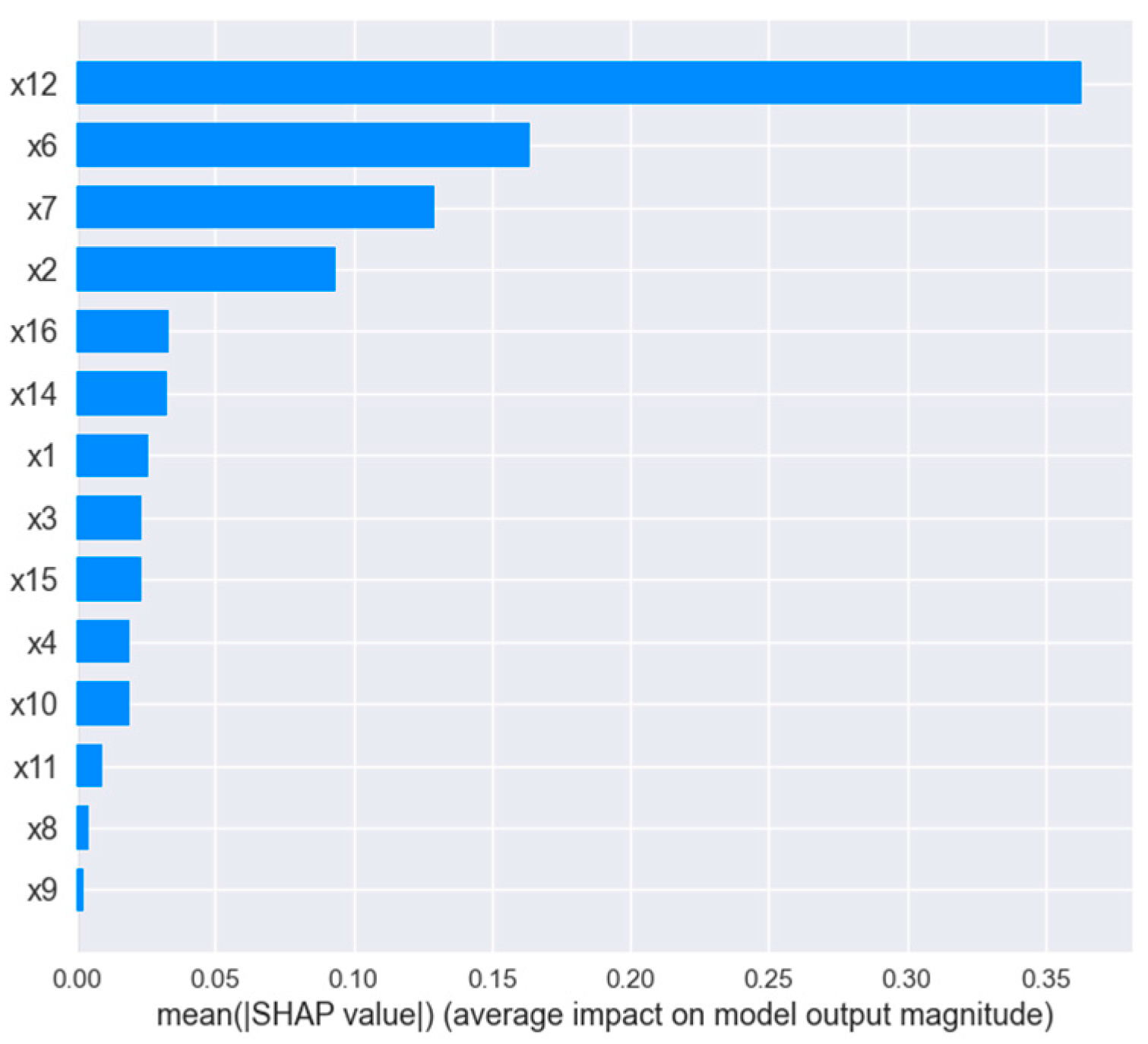
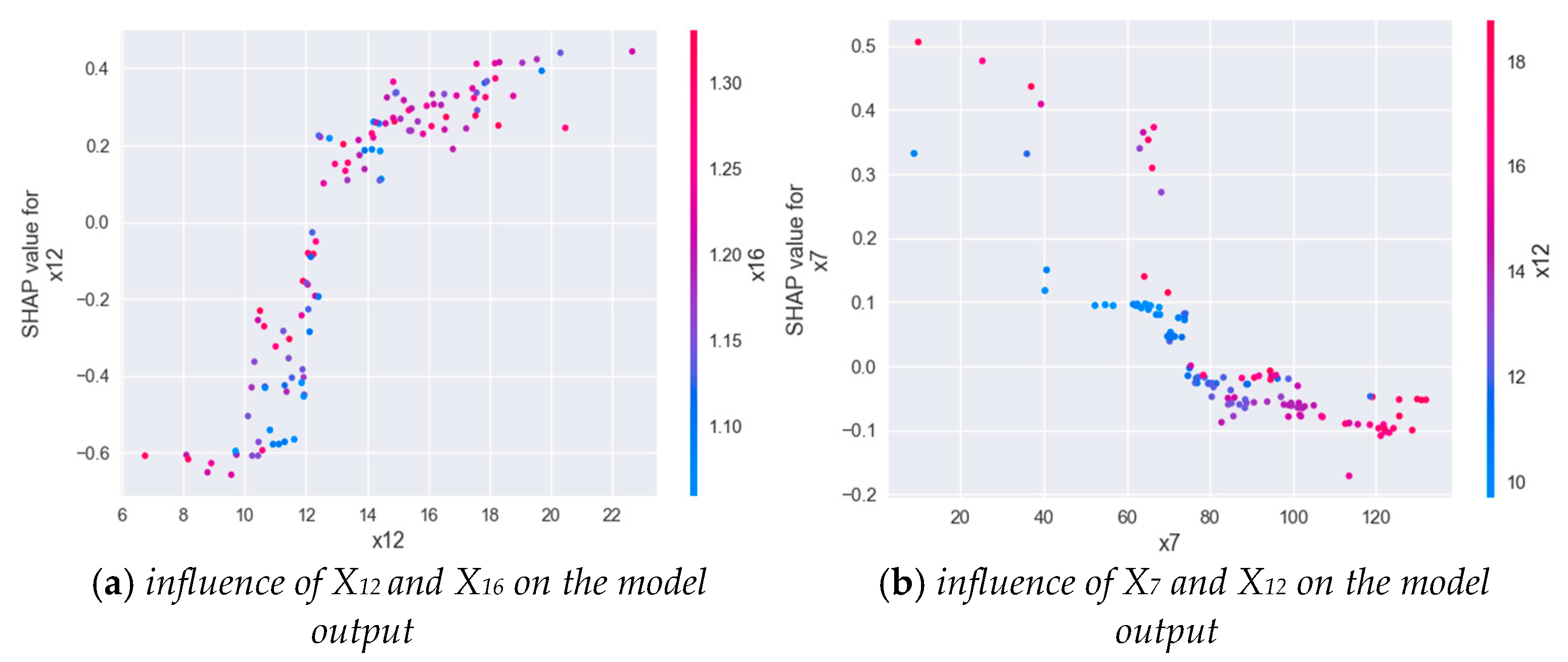
3.3. Interpretability of GA-XGBOOST Output
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amelchugov, S.; Inzhutov, I.; Nikitina, O.; Berseneva, M. On the issue of personnel management in high-latitude construction. MATEC Web Conf. 2018, 245, 03021. [Google Scholar] [CrossRef]
- Huang, B. Analysis and Comprehensive Evaluation of Core Elements of Physical Fitness of Young Male at Different Altitudes. Ph.D thesis, Tianjin Institute of Physical Education, Tianjin, China, 2020. [Google Scholar]
- Balady, G.J.; Arena, R.; Sietsema, K.; Myers, J.; Coke, L.; Fletcher, G.F.; Forman, D.; Franklin, B.; Guazzi, M.; Gulati, M.; et al. Clinician’s guide to cardiopulmonary exercise testing in adults: A scientific statement from the American Heart Association. Circulation 2010, 122, 191–225. [Google Scholar] [CrossRef] [Green Version]
- Hill, D.W.; Rowell, A.L. Running velocity at VO2max. Med. Sci. Sport. Exerc. 1996, 28, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sport. 2015, 25, 1–72. [Google Scholar] [CrossRef] [Green Version]
- Mezzani, A.; Guazzi, M. Balancing the evidence on the cardiovascular determinants of oxygen uptake improvement after endurance training in the elderly: What are the next steps? Eur. J. Prev. Cardiol. 2016, 23, 730–732. [Google Scholar] [CrossRef] [Green Version]
- Jones, L.W.; Eves, N.D.; Hayowsky, M.; Joy, A.A.; Douglas, P.S. Cardiorespiratory exercise testing in clinical oncology research: Systematic review and practice recommendations. Lancet Oncol. 2008, 9, 757–765. [Google Scholar] [CrossRef]
- Svedahl, K.; MacIntosh, B.R. Anaerobic threshold: The concept and methods of measurement. Can. J. Appl. Physiol. 2003, 28, 299–323. [Google Scholar] [CrossRef] [Green Version]
- Braga AC, M.; Pinto, A.; Pinto, S.; de Carvalho, M. The role of moderate aerobic exercise as determined by cardiopulmonary exercise testing in ALS. Neurol. Res. Int. 2018, 2018, 8218697. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.M.; Carter, H. The effect of endurance training on parameters of aerobic fitness. Sport. Med. 2000, 29, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.; Tartibian, B. Prediction and comparison of maximum O2 pulse in male adolescents. Facta Univ.-Ser. Phys. Educ. Sport 2006, 4, 81–92. [Google Scholar]
- Laukkanen, J.A.; Kurl, S.; Salonen, J.T.; Lakka, T.; Rauramaa, R. Peak oxygen pulse during exercise as a predictor for coronary heart disease and all cause death. Heart 2006, 92, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Petek, B.J.; Churchill, T.W.; Sawalla Guseh, J.; Loomer, G.; Gustus, S.K.; Lewis, G.D.; Weiner, R.B.; Baggish, A.L.; Wasfy, M.M. Utility of the oxygen pulse in the diagnosis of obstructive coronary artery disease in physically fit patients. Physiol. Rep. 2021, 9, e15105. [Google Scholar] [CrossRef] [PubMed]
- Carriere, C.; Corrà, U.; Piepoli, M.; Bonomi, A.; Merlo, M.; Barbieri, S.; Salvioni, E.; Binno, S.; Mapelli, M.; Righini, F.; et al. Anaerobic threshold and respiratory compensation point identification during cardiopulmonary exercise tests in chronic heart failure. Chest 2019, 156, 338–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biccard, B.M. Improving the evidence-base for preoperative cardiopulmonary exercise testing. Br. J. Anaesth. 2018, 120, 419–421. [Google Scholar] [CrossRef] [Green Version]
- Stringer, W.; Marciniuk, D. The role of cardiopulmonary exercise testing (CPET) in pulmonary rehabilitation (PR) of chronic obstructive pulmonary disease (COPD) patients. COPD J. Chronic Obstr. Pulm. Dis. 2018, 15, 621–631. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.; Agostoni, P.; Arena, R.; Belardinelli, R.; Dumitrescu, D.; Hager, A.; Myers, J.; Rauramaa, R.; Riley, M.; Takken, T.; et al. The role of gas exchange variables in cardiopulmonary exercise testing for risk stratification and management of heart failure with reduced ejection fraction. Am. Heart J. 2018, 202, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Remington, H.E. Aortic Stiffness and Cardiopulmonary Exercise Test Variables. Master’s Thesis, School of Kinesiology, Ann Arbor, MI, USA, 2020. [Google Scholar]
- Duceppe, E.; Parlow, J.; MacDonald, P.; Lyons, K.; McMullen, M.; Srinathan, S.; Graham, M.; Tandon, V.; Styles, K.; Bessissow, A.; et al. Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. Can. J. Cardiol. 2017, 33, 17–32. [Google Scholar] [CrossRef] [Green Version]
- Leopold, E.; Navot-Mintzer, D.; Shargal, E.; Tsuk, S.; Tuller, T.; Scheinowitz, M. Prediction of the Wingate anaerobic mechanical power outputs from a maximal incremental cardiopulmonary exercise stress test using machine-learning approach. PLoS ONE 2019, 14, e0212199. [Google Scholar] [CrossRef]
- Braccioni, F.; Bottigliengo, D.; Ermolao, A.; Schiavon, M.; Loy, M.; Marchi, M.R.; Gregori, D.; Rea, F.; Vianello, A. Dyspnea, effort and muscle pain during exercise in lung transplant recipients: An analysis of their association with cardiopulmonary function parameters using machine learning. Respir. Res. 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Inbar, O.; Inbar, O.; Reuveny, R.; Segel, M.J.; Greenspan, H.; Scheinowitz, M. A Machine Learning Approach to the Interpretation of Cardiopulmonary Exercise Tests: Development and Validation. Pulm. Med. 2021, 2021, 5516248. [Google Scholar] [CrossRef] [PubMed]
- Li, H.L.; Xia, Y.Y.; Zou, J.C. Selection method of middle and long distance endurance athletes based onCPET time series clustering. Comput. Eng. 2022, 48, 262–268. [Google Scholar]
- Deak, G.; Miron, R.; Astilean, A.; Domuţa, C. Fuzzy based method for assessing the training level of nonathletes and athletes. In Proceedings of the 2010 IEEE International Conference on Automation, Quality and Testing, Robotics (AQTR), IEEE, Cluj-Napoca, Romania, 28–30 May 2010; Volume 2, pp. 1–5. [Google Scholar]
- Chen, W.; Zheng, L.; Li, K.; Wang, Q.; Liu, G.; Jiang, Q. A novel and effective method for congestive heart failure detection and quantification using dynamic heart rate variability measurement. PLoS ONE 2016, 11, e0165304. [Google Scholar] [CrossRef] [PubMed]
- Bellos, C.; Papadopoulos, A.; Rosso, R.; Fotiadis, D.I.; Papadopoulos, A. Categorization of patients’ health status in COPD disease using a wearable platform and random forests methodology. In Proceedings of the 2012 IEEE-EMBS International Conference on Biomedical and Health Informatics, IEEE, Hong Kong, China, 5–7 January 2012; pp. 404–407. [Google Scholar]
- Song, K.; Yan, F.; Ding, T.; Gao, L.; Lu, S. A steel property optimization model based on the XGBoost algorithm and improved PSO. Comput. Mater. Sci. 2020, 174, 109472. [Google Scholar] [CrossRef]
- Pan, B. Application of XGBoost algorithm in hourly PM2. 5 concentration prediction. In IOP Conference Series: Earth and Environmental Science; IOP Publishing: Bristol, UK, 2018; Volume 113, p. 012127. [Google Scholar]
- Ogunleye, A.; Wang, Q.G. XGBoost model for chronic kidney disease diagnosis. IEEE/ACM Trans. Comput. Biol. Bioinform. 2019, 17, 2131–2140. [Google Scholar] [CrossRef]
- Qi, L. Research and Application of the Intelligent Evaluation Method of Cardiopulmonary Endurance. Master’s thesis, Huazhong University of Science and Technology, Wuhan, China, 2020. [Google Scholar]
- Winter, E. The shapley value. In Handbook of game theory with economic applications; Elsevier: Amsterdam, The Netherland, 2002; Volume 3, pp. 2025–2054. [Google Scholar]
- Hui, G. Development of Self-Evaluation Method for Adult Cardiopulmonary Endurance and Establishment of Reference Grade. Ph.D. Thesis, Beijing Sport University, Beijing, China, 2016. [Google Scholar]
- Yuri, F.; Meir, M. ACSM’s Health-Related Physical Fitness Assessment Manual; American College of Sports Medicine: Baltimore, MD, USA, 2021. [Google Scholar]
- Ong, K.C.; Ong, Y.Y. Cardiopulmonary exercise testing in patients with chronic obstructive pulmonary disease. Ann. Acad. Med. Singap. 2000, 29, 648–652. [Google Scholar] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Weights | |
|---|---|---|
| Cardiovascular Capacity | ) | 0.078 |
| 0.058 | ||
| 0.073 | ||
| 0.048 | ||
| 0.075 | ||
| Respiratory Metabolic Capacity | 0.096 | |
| 0.064 | ||
| 0.075 | ||
| 0.087 | ||
| Metabolic Capacity | 0.064 | |
| 0.111 | ||
| 0.053 | ||
| 0.054 | ||
| 0.066 |
| Model | Accuracy | Macro-Recall | Macro-Precision | Macro-F1 Score |
|---|---|---|---|---|
| RF | 0.810 | 0.810 | 0.886 | 0.812 |
| SVM | 0.843 | 0.843 | 0.876 | 0.841 |
| XGBOOST | 0.861 | 0.861 | 0.879 | 0.864 |
| Parameter Name | Meaning | Default Value | Optimal Value |
|---|---|---|---|
| max_depth | The maximum depth of number | 10 | 221 |
| learning_rate | Learning rate | 0.1 | 0.285 |
| n_estimator | Number of iterators | 100 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, J.; Fu, Y.; Liu, Q.; Chang, L.; Li, H.; Liu, S. Automatic Cardiopulmonary Endurance Assessment: A Machine Learning Approach Based on GA-XGBOOST. Diagnostics 2022, 12, 2538. https://doi.org/10.3390/diagnostics12102538
Deng J, Fu Y, Liu Q, Chang L, Li H, Liu S. Automatic Cardiopulmonary Endurance Assessment: A Machine Learning Approach Based on GA-XGBOOST. Diagnostics. 2022; 12(10):2538. https://doi.org/10.3390/diagnostics12102538
Chicago/Turabian StyleDeng, Jia, Yan Fu, Qi Liu, Le Chang, Haibo Li, and Shenglin Liu. 2022. "Automatic Cardiopulmonary Endurance Assessment: A Machine Learning Approach Based on GA-XGBOOST" Diagnostics 12, no. 10: 2538. https://doi.org/10.3390/diagnostics12102538