
Physiological Offset Parameters of the Adult Shoulder Joint—A MRI Study of 800 Patients
 ,
,  , , ,
, , ,
Abstract
:Highlights
- 800 shoulder MRIs were retrospectively evaluated for humeral, glenoidal and latero-glenoidal humeral offset, as well as cortical and humeral shaft axis offset.
- Significantly higher values for all analysed offset parameters were found in male shoulder joints compared to female shoulder joints.
- Significant side-specific differences were found for humeral, glenoidal and latero-glenoidal humeral offset.
- A correlation of the offset parameters with age or the osteoarthritis grade exist only for cortical offset.
- These results should be considered in shoulder diagnostics and surgery.
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion Criteria
2.3. Exclusion Criteria
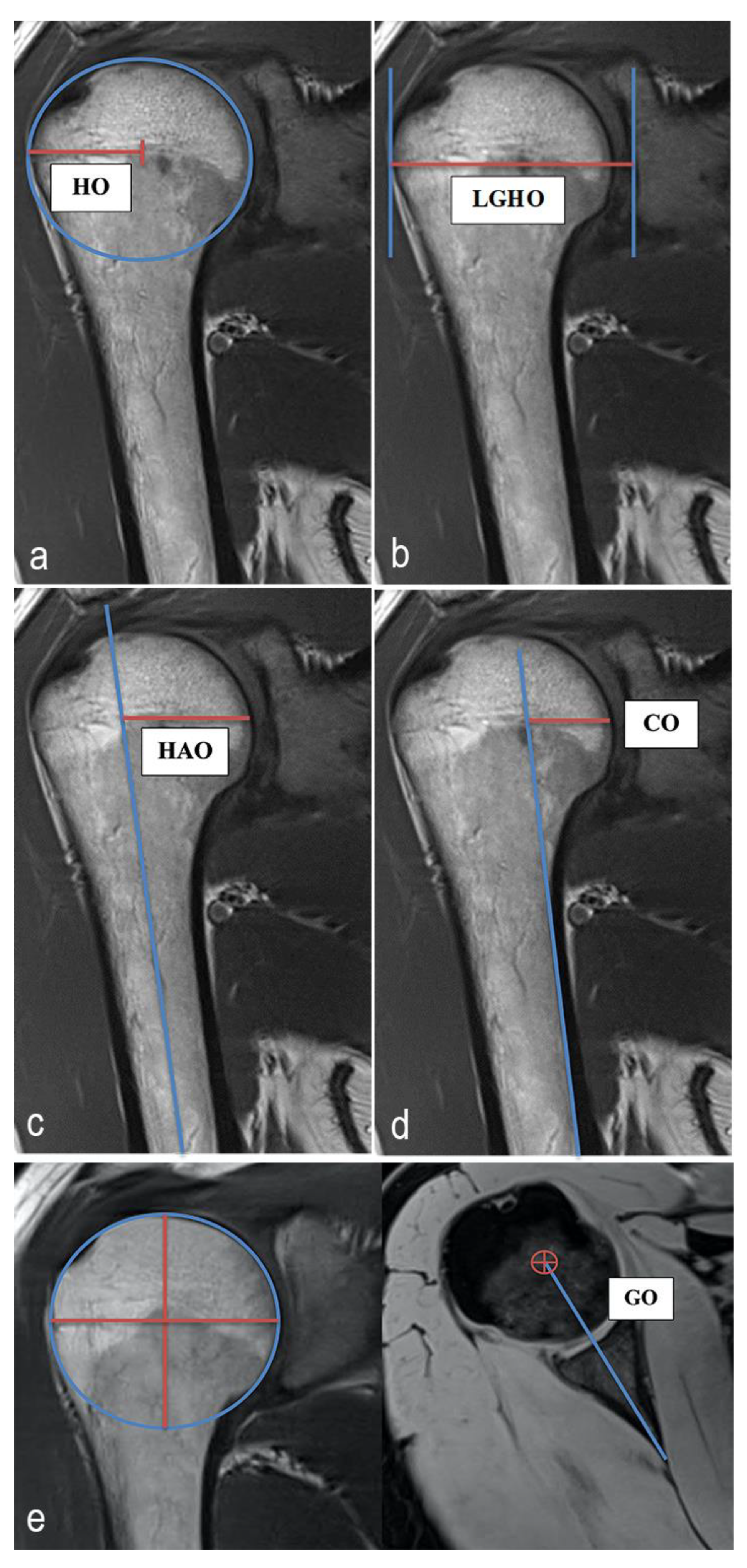
2.4. MRI Analysis, Parameters and Methods of Measurement
2.5. Statistics
3. Results
3.1. Characteristics of the Study Population
3.2. Analysis of the Shoulder Offset Parameters
3.2.1. Humeral Offset
3.2.2. Glenoidal Offset
3.2.3. Lateral Glenoidal Humeral Offset
3.2.4. Humeral Shaft Axis Offset
3.2.5. Cortical Offset
3.3. Analysis of Side Specific Differences for SOPs
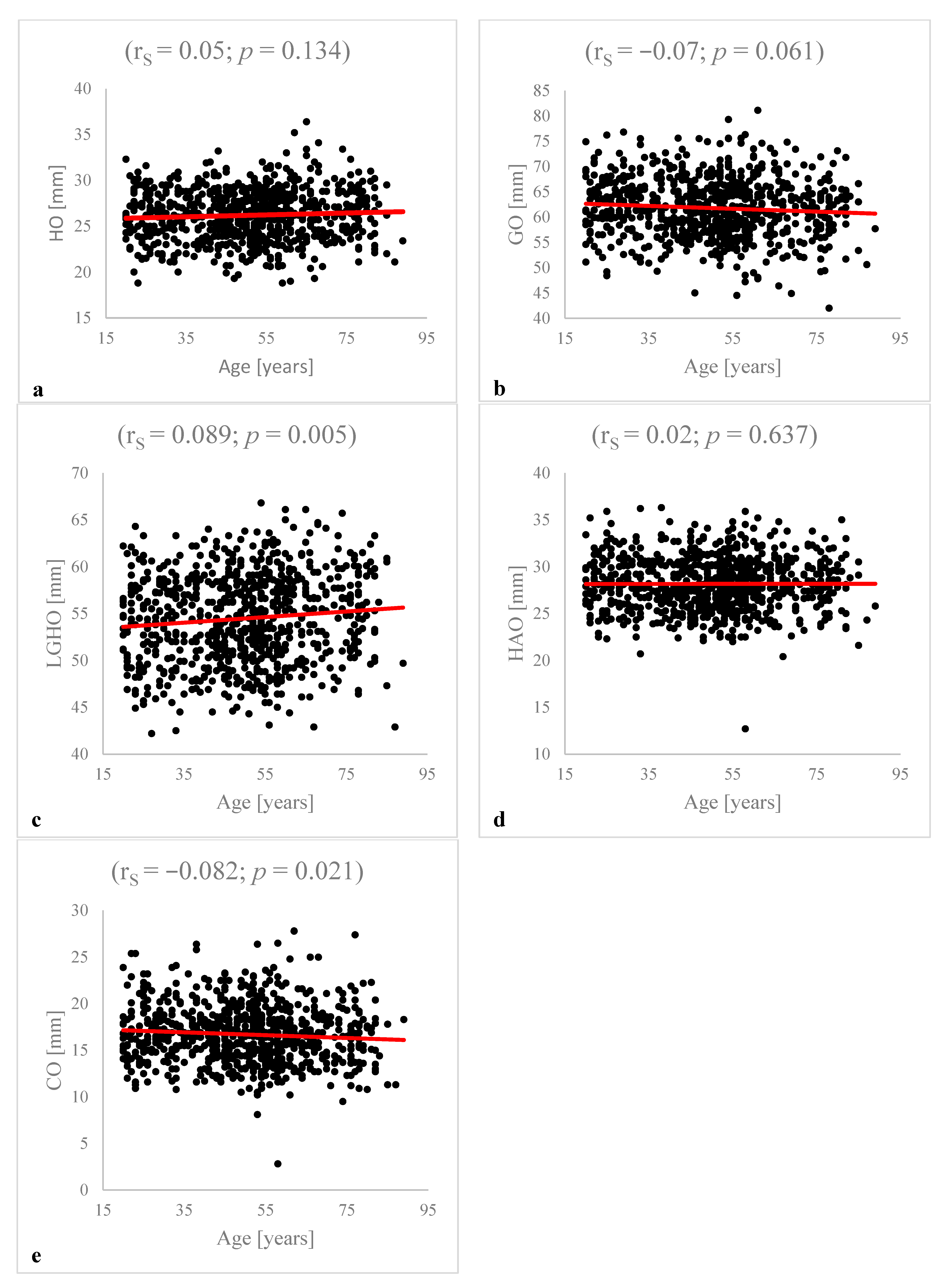
3.4. Analysis of Age-Specific Differences and Age Dependent Correlation Analysis for SOPs
3.5. Analysis of Gender-Specific Differences for SOPs
3.6. Analysis between SOPs and Grade of Osteoarthritis
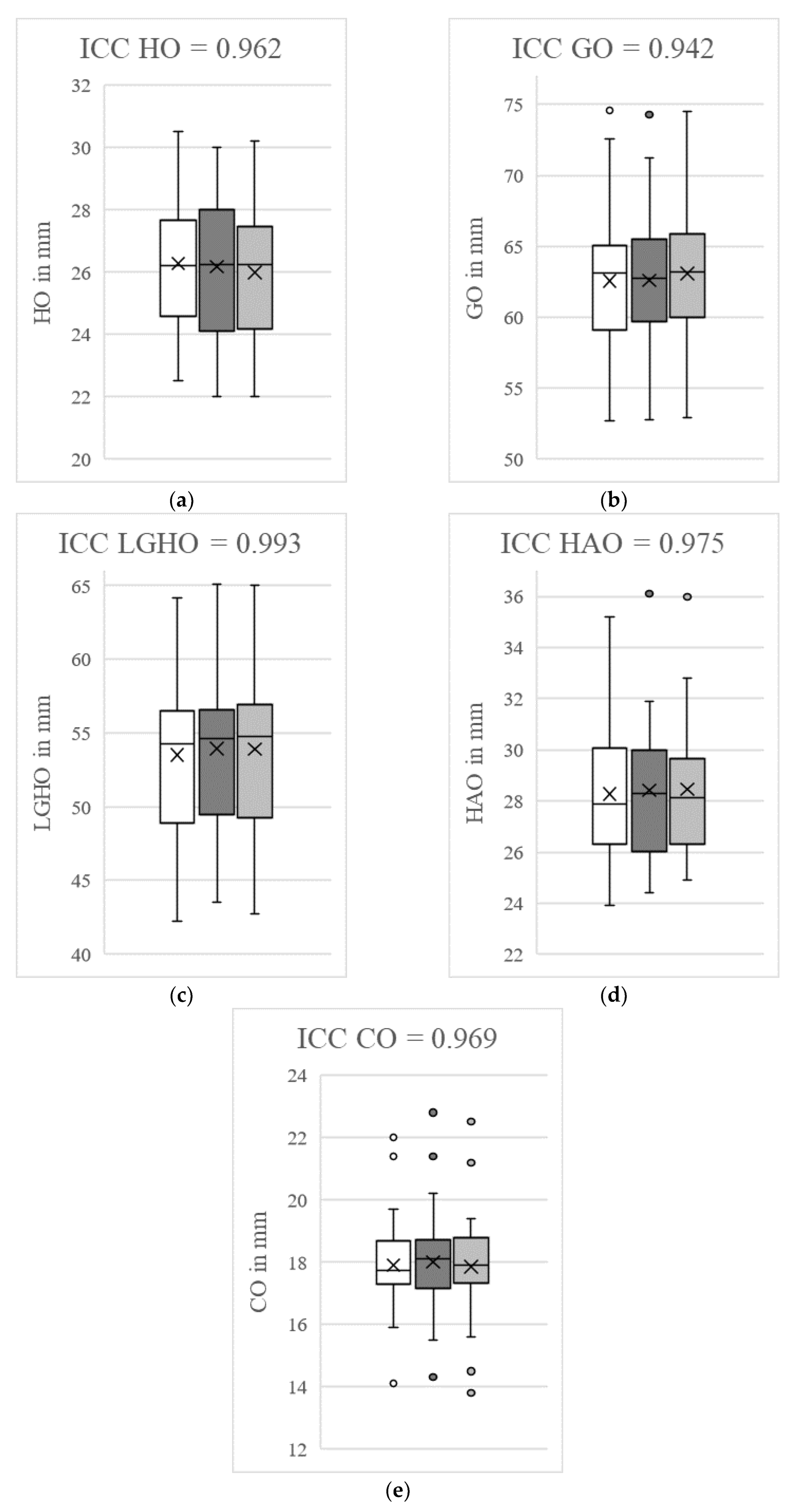
3.7. Analysis of Intraobserver and Interobserver Reliability
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Thelen, S.; Grassmann, J.P.; Schneider, M.; Jaekle, C.; Meier, D.M.; Betsch, M.; Hakimi, M.; Wild, M. The influence of fracture severity on postoperative outcome and quality of life after locking plate fixation of proximal humeral fractures. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2022, 11, 3. [Google Scholar] [CrossRef]
- Xiang, H.; Wang, Y.; Yang, Y.; Liu, F.; Lu, Q.; Kong, L.; Li, M.; Han, Y.; Wang, F. Anatomical study for the treatment of proximal humeral fracture through the medial approach. J. Orthop. Surg. Res. 2022, 17, 35. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt. Gesundheit: Fallpauschalenbezogene Krankenhausstatistik (DRG-Statistik) Operationen und Prozeduren der Vollstationären Patientinnen und Patienten in Krankenhäusern 2019; Statistisches Bundesamt: Wiesbaden, Germany, 2020.
- Ahrend, M.D.; Kühle, L.; Riedemann, S.; Bahrs, S.D.; Bahrs, C.; Ziegler, P. Radiographic parameter(s) influencing functional outcomes following angular stable plate fixation of proximal humeral fractures. Int. Orthop. 2021, 45, 1845–1852. [Google Scholar] [CrossRef]
- Athwal, G.S.; Wiater, J.M. Shoulder Joint Replacement. OrthoInfo. 2021. Available online: https://orthoinfo.aaos.org/ (accessed on 12 July 2022).
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Partial Knee Arthroplasty: Supplementary Report, in Hip, Knee & Shoulder Arthroplasty: 2020 Annual Report; AOA: Adelaide, Australia, 2020; pp. 1–27. Available online: https://aoanjrr.sahmri.com/annual-reports-2020/supplementary (accessed on 12 July 2022).
- Patzer, T. Schultergelenkersatz bei jungen Patienten. Arthroskopie 2020, 33, 336–347. [Google Scholar] [CrossRef]
- Sharma, G.B.; McMahon, P.J.; Robertson, D.D. Structure modeling of the glenoid: Relevance to shoulder arthroplasty. J. Orthop. Res. 2014, 32, 1471–1478. [Google Scholar] [CrossRef]
- Mizuno, N.; Nonaka, S.; Ozaki, R.; Yoshida, M.; Yoneda, M.; Walch, M. Three-dimensional assessment of the normal Japanese glenoid and comparison with the normal French glenoid. Orthop. Traumatol. Surg. Res. 2017, 103, 1271–1275. [Google Scholar] [CrossRef]
- Daggett, M.; Werner, B.; Gauci, M.O.; Chaoui, J.; Walch, G. Comparison of glenoid inclination angle using different clinical imaging modalities. J. Shoulder Elbow Surg. 2016, 25, 180–185. [Google Scholar] [CrossRef]
- Moineau, G.; Levigne, C.; Boileau, P.; Young, A.; Walch, G. Three-dimensional measurement method of arthritic glenoid cavity morphology: Feasibility and reproducibility. Orthop. Traumatol. Surg. Res. 2012, 98, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Tomanek, F.; Ulrich, L. Schulterinstabilität beim Überkopfsportler. Arthroskopie 2021, 34, 420–426. [Google Scholar] [CrossRef]
- Walton, J.; Paxinos, A.; Tzannes, A.; Callanan, M.; Hayes, K.; Murell, G.A.C. The unstable shoulder in the adolescent athlete. Am. J. Sports Med. 2002, 30, 758–767. [Google Scholar] [CrossRef]
- Bodrogi, A.; Athwal, G.S.; Howard, L.; Zhang, T.; Lapner, P. A reliable method of determining glenohumeral offset in anatomic total shoulder arthroplasty. J. Shoulder Elbow Surg. 2019, 28, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.R.; Houdek, M.T.; Schleck, C.D.; Harmsen, W.S.; Sánchez-Sotelo, J.; Cofield, R.; Elhassan, B.T.; Sperling, J.W. The role age plays in the outcomes and complications of shoulder arthroplasty. J. Shoulder Elbow Surg. 2017, 26, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.A.; Murthi, A.M. Offset in Reverse Shoulder Arthroplasty: Where, When, and How Much. J. Am. Acad. Orthop. Surg. 2021, 29, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Collotte, P.; Gauci, M.O.; Vieira, T.D.; Walch, G. Bony increased-offset reverse total shoulder arthroplasty (BIO-RSA) associated with an eccentric glenosphere and an onlay 135° humeral component: Clinical and radiological outcomes at a minimum 2-year follow-up. JSES Int. 2022, 28, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Middleton, C.; Uri, O.; Phillips, S.; Barmpagiannis, K.; Higgs, D.; Falworth, M.; Bayley, I.; Lambert, S. A reverse shoulder arthroplasty with increased offset for the treatment of cuff-deficient shoulders with glenohumeral arthritis. Bone Jt. J. 2014, 96, 936–942. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werthel, J.D.; Walch, G.; Vegehan, E.; Deransart, P.; Sanchez-Sotelo, J.; Valentin, P. Lateralization in reverse shoulder arthroplasty: A descriptive analysis of different implants in current practice. Int. Orthop. 2019, 43, 2349–2360. [Google Scholar] [CrossRef]
- Walker, D.R.; Kinney, A.L.; Wright, T.W.; Banks, S.A. How sensitive is the deltoid moment arm to humeral offset changes with reverse total shoulder arthroplasty? J. Shoulder Elbow Surg. 2016, 25, 998–1004. [Google Scholar] [CrossRef]
- Routman, H.D.; Flurin, P.H.; Wright, T.W.; Zuckerman, J.D.; Hamilton, M.A.; Roche, C.P. Reverse Shoulder Arthroplasty Prosthesis Design Classification System. Bull. Hosp. Jt. Dis. 2015, 73, 5–14. [Google Scholar]
- Harrold, F.; Wigderowitz, C. Humeral head arthroplasty and its ability to restore original humeral head geometry. J. Shoulder Elbow Surg. 2013, 22, 115–121. [Google Scholar] [CrossRef]
- Papadatou-Pastou, M.; Ntolka, E.; Schmitz, J.; Martin, M.; Munafò, M.R.; Ocklenburg, S.; Paracchini, S. Human handedness: A meta-analysis. Psychol. Bull. 2020, 146, 481–524. [Google Scholar] [CrossRef] [PubMed]
- Scharoun, S.M.; Bryden, P.J. Hand preference, performance abilities, and hand selection in children. Front. Psychol. 2014, 5, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandolini, M.; Bruzini, A.; Facco, G.; Mazzoli, A.; Forcellesse, A.; Gigante, A. Comparison of Three 3D Segmentation Software Tools for Hip Surgical Planning. Sensors 2022, 13, 5242. [Google Scholar] [CrossRef]
- Cao, Z.; Yang, W.; Yang, M.; Kong, X.; Wang, Y.; Guo, R.; Chen, J.; Chai, W. Application of preoperative digital-template planning in total hip arthroplasty via direct anterior approach. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2019, 15, 1374–1378. [Google Scholar] [CrossRef]
- Knowles, N.K.; Caroll, M.J.; Keener, J.D.; Ferreira, L.M.; Athwal, G.S. A comparison of normal and osteoarthritic humeral head size and morphology. J. Shoulder Elbow Surg. 2016, 25, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Piponov, I.H.; Savin, D.; Shah, N.; Esposito, D.; Schwartz, B.; Moretti, V.; Goldberg, B. Glenoid version and size: Does gender, ethnicity, or body size play a role? Int. Orthop. 2016, 40, 2347–2353. [Google Scholar] [CrossRef]
- Mathews, S.; Burkhard, M.; Serrano, N.; Link, K.; Häusler, M.; Frater, N.; Franke, I.; Bischofberger, H.; Buck, F.M.; Gaucho, D.; et al. Glenoid morphology in light of anatomical and reverse total shoulder arthroplasty: A dissection- and 3D-CT-based study in male and female body donors. BMC Musculoskelet. Disord. 2017, 10, 9. [Google Scholar] [CrossRef] [Green Version]
- Cagle, P.J., Jr.; Werner, B.; Shukla, D.R.; London, D.A.; Parsons, B.O.; Millar, N.L. Interobserver and intraobserver comparison of imaging glenoid morphology, glenoid version and humeral head subluxation. Shoulder Elbow 2019, 11, 204–209. [Google Scholar] [CrossRef]
- Kadum, B.; Sayed-Noor, A.S.; Perisynakis, N.; Baea, S.; Sjödén, G.O. Radiologic assessment of glenohumeral relationship: Reliability and reproducibility of lateral humeral offset. Surg. Radiol. Anat. 2015, 37, 363–367. [Google Scholar] [CrossRef]
- Bouacida, S.; Gauci, M.O.; Coulet, B.; Lazerges, C.; Cyteval, C.; Boileau, P.; Chammas, M. Interest in the glenoid hull method for analyzing humeral subluxation in primary glenohumeral osteoarthritis. J. Shoulder Elbow Surg. 2017, 26, 1128–1136. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 800) | Left (n = 371) | Right (n = 429) | p-Value | ||
|---|---|---|---|---|---|
| HO | [mm] | 26.19 (±2.70) | 25.45 (±2.62) | 26.83 (±2.59) | <0.001 ***,1 |
| GO | [mm] | 61.79 (±5.67) | 60.67 (±5.29) | 62.75 (±5.81) | <0.001 ***1 |
| LGHO | [mm] | 54.49 (±4.69) | 53.74 (±4.54) | 55.13 (±4.72) | <0.001 ***1 |
| HAO | [mm] | 28.17 (±2.82) | 28.14 (±2.93) | 28.20 (±2.73) | 0.609 1 |
| CO | [mm] | 16.70 (±3.08) | 16.74 (±3.21) | 16.67 (±2.97) | 0.843 1 |
| Total (n = 800) | 20–50 y. (n = 384) | >50 y. (n = 416) | p-Value | ||
|---|---|---|---|---|---|
| HO | [mm] | 26.19 (±2.70) | 26.07 (±2.61) | 26.31 (±2.77) | 0.363 1 |
| GO | [mm] | 61.79 (±5.67) | 62.13 (±5.41) | 61.47 (±5.89) | 0.124 1 |
| LGHO | [mm] | 54.49 (±4.69) | 54.16 (±4.62) | 54.79 (±4.73) | 0.081 1 |
| HAO | [mm] | 28.17 (±2.82) | 28.17 (±2.80) | 28.17 (±2.85) | 0.756 1 |
| CO | [mm] | 16.70 (±3.08) | 16.99 (±2.96) | 16.44 (±3.17) | 0.011 *1 |
| Total (n = 800) | Females (n = 351) | Males (n = 449) | p-Value | ||
|---|---|---|---|---|---|
| HO | [mm] | 26.19 (±2.70) | 24.17 (±2.01) | 27.77 (±2.03) | <0.001 ***1 |
| GO | [mm] | 61.79 (±5.67) | 58.14 (±4.52) | 64.64 (±4.78) | <0.001 ***1 |
| LGHO | [mm] | 54.49 (±4.69) | 50.56 (±3.14) | 57.56 (±3.15) | <0.001 ***1 |
| HAO | [mm] | 28.17 (±2.82) | 26.34 (±2.14) | 29.60 (±2.44) | <0.001 ***1 |
| CO | [mm] | 16.70 (±3.08) | 15.92 (±2.80) | 17.31 (±3.16) | <0.001 ***1 |
| Total (n = 800) | KL 0–2 (n = 777) | KL 3–4 (n = 23) | p-Value | ||
|---|---|---|---|---|---|
| HO | [mm] | 26.19 (±2.70) | 26.19 (±2.68) | 26.14 (±3.10) | 0.941 1 |
| GO | [mm] | 61.79 (±5.67) | 61.85 (±5.63) | 59.58 (±6.51) | 0.148 1 |
| LGHO | [mm] | 54.49 (±4.69) | 54.51 (±4.66) | 53.65 (±5.59) | 0.386 1 |
| HAO | [mm] | 28.17 (±2.82) | 28.19 (±2.77) | 27.55 (±4.31) | 0.571 1 |
| CO | [mm] | 16.70 (±3.08) | 16.75 (±3.04) | 15.09 (±3.92) | 0.049 *1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meier, M.-P.; Brandt, L.E.; Saul, D.; Roch, P.J.; Klockner, F.S.; Hosseini, A.S.A.; Lehmann, W.; Hawellek, T. Physiological Offset Parameters of the Adult Shoulder Joint—A MRI Study of 800 Patients. Diagnostics 2022, 12, 2507. https://doi.org/10.3390/diagnostics12102507
Meier M-P, Brandt LE, Saul D, Roch PJ, Klockner FS, Hosseini ASA, Lehmann W, Hawellek T. Physiological Offset Parameters of the Adult Shoulder Joint—A MRI Study of 800 Patients. Diagnostics. 2022; 12(10):2507. https://doi.org/10.3390/diagnostics12102507
Chicago/Turabian StyleMeier, Marc-Pascal, Lars Erik Brandt, Dominik Saul, Paul Jonathan Roch, Friederike Sophie Klockner, Ali Seif Amir Hosseini, Wolfgang Lehmann, and Thelonius Hawellek. 2022. "Physiological Offset Parameters of the Adult Shoulder Joint—A MRI Study of 800 Patients" Diagnostics 12, no. 10: 2507. https://doi.org/10.3390/diagnostics12102507