
Performance Analysis of Self-Collected Nasal and Oral Swabs for Detection of SARS-CoV-2
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Inclusion and Exclusion Criteria
2.2. Collection and Experimental Protocol
2.3. Multiplex Reverse Transcription Quantitative Real-Time Polymerase Chain Reaction (mRT-qPCR) Analysis
2.4. Viral RNA Load Standard
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
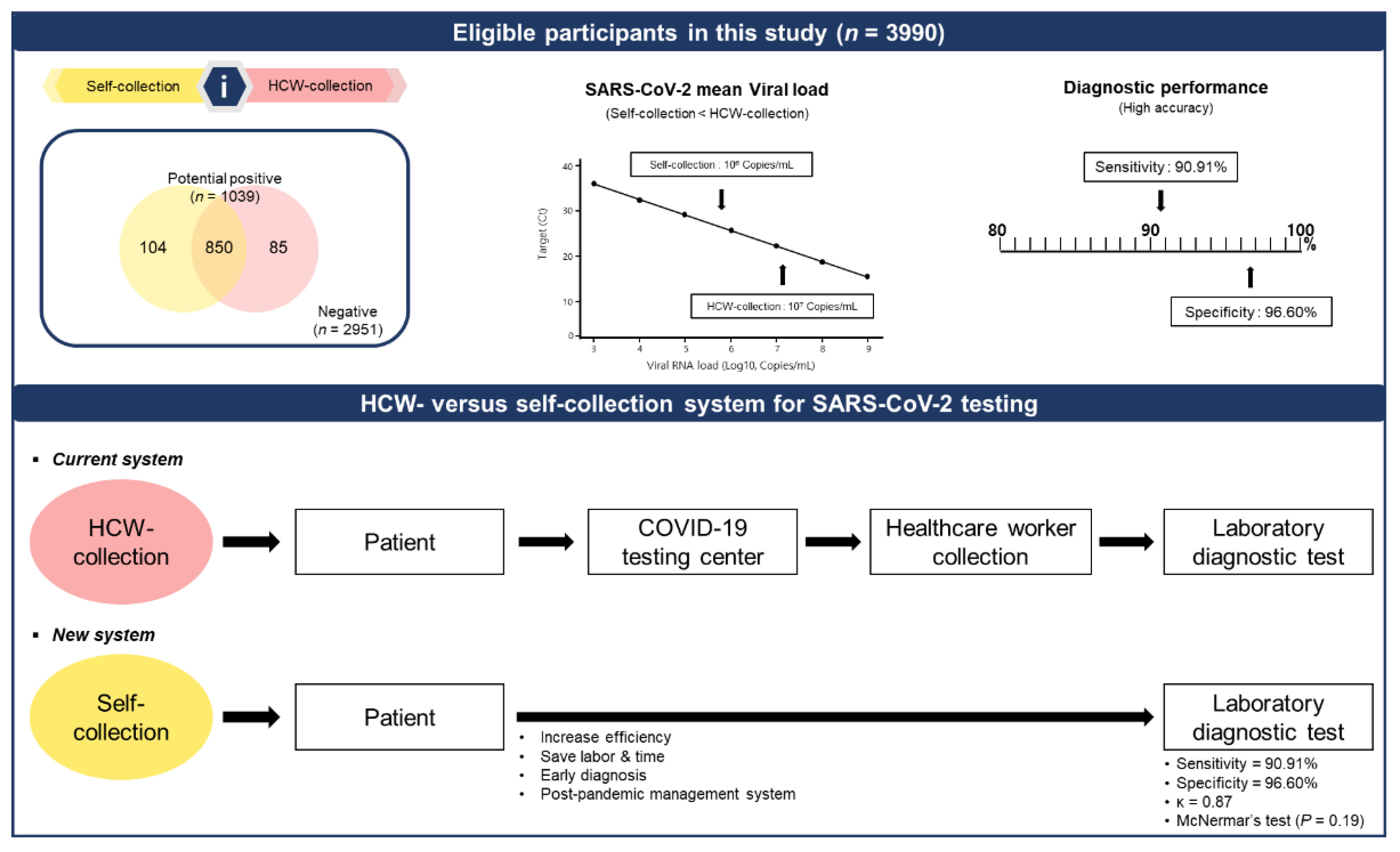
3.2. Comparison of the Clinical Diagnosis Performance between the HCW- and Self-Collected Samples
3.3. Clinical Performance of the HCW- and Self-Collection Methods
3.4. Viral Load Detected Using the HCW- and Self-Collection Methods
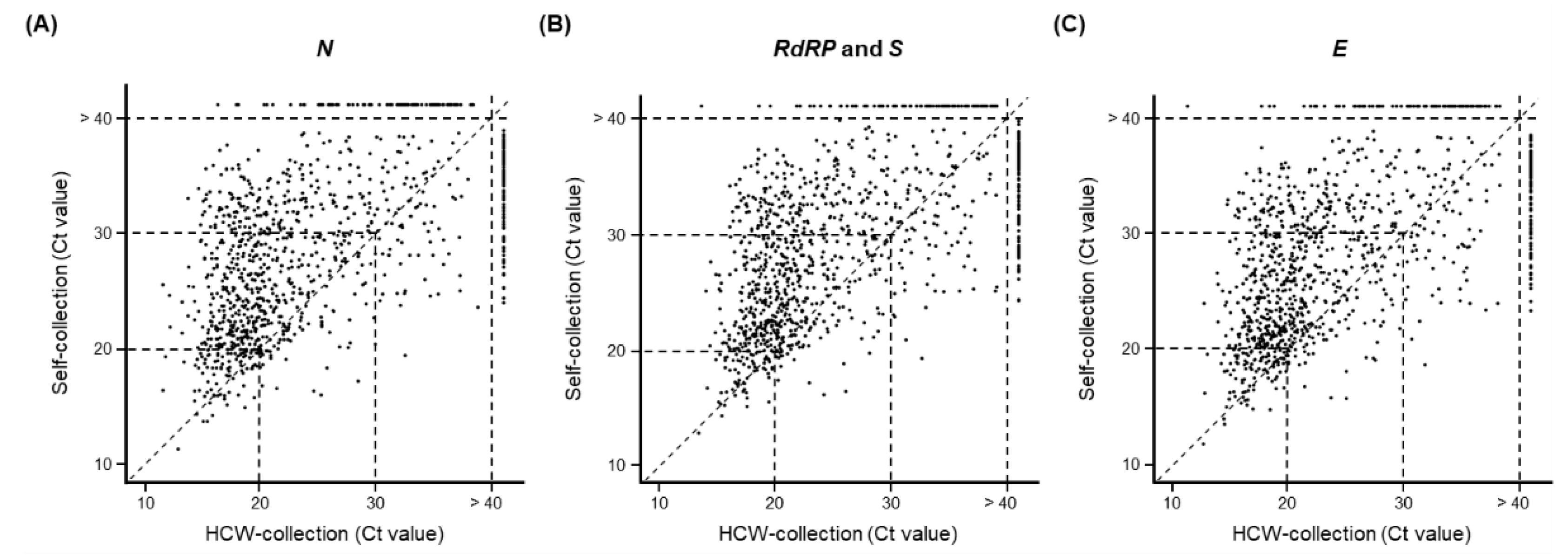
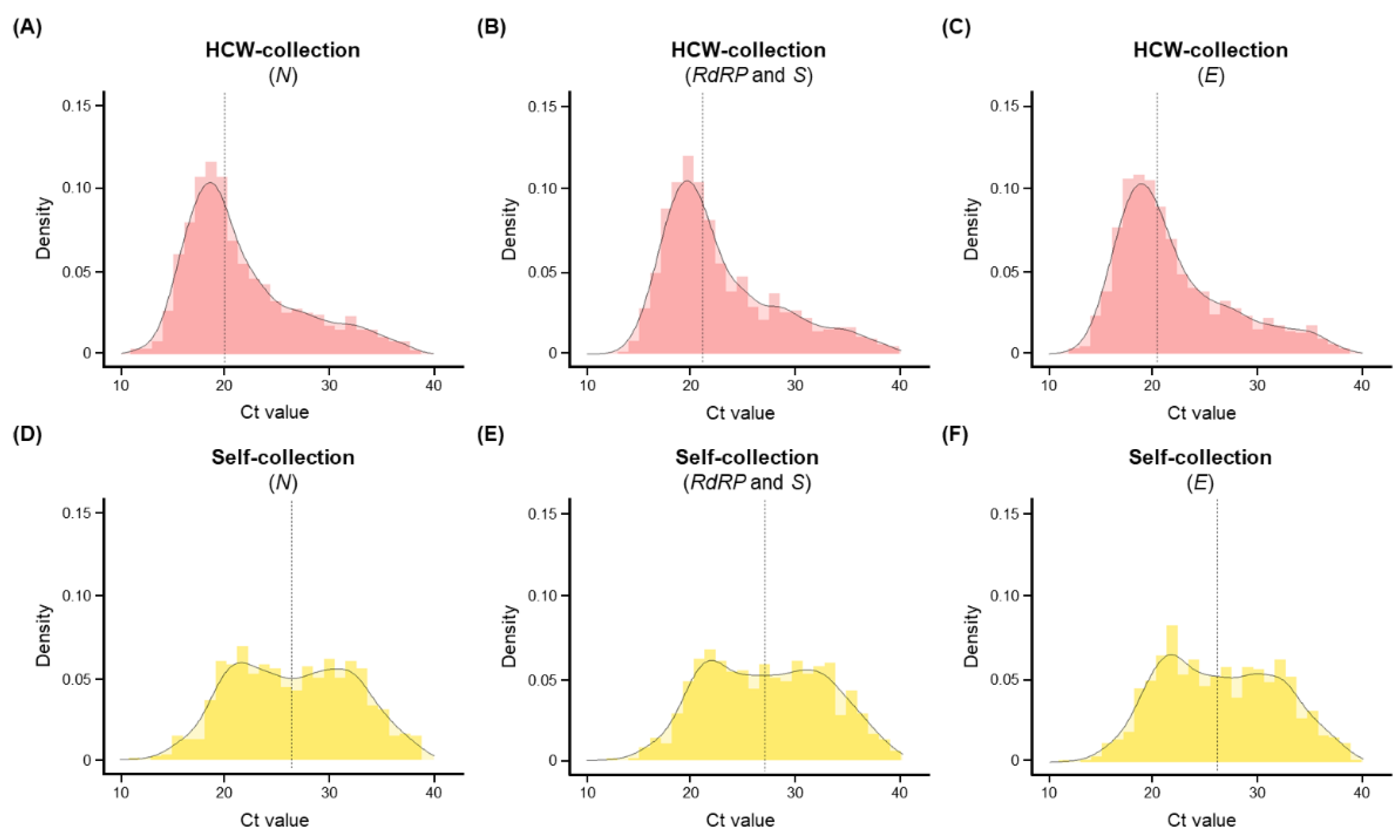
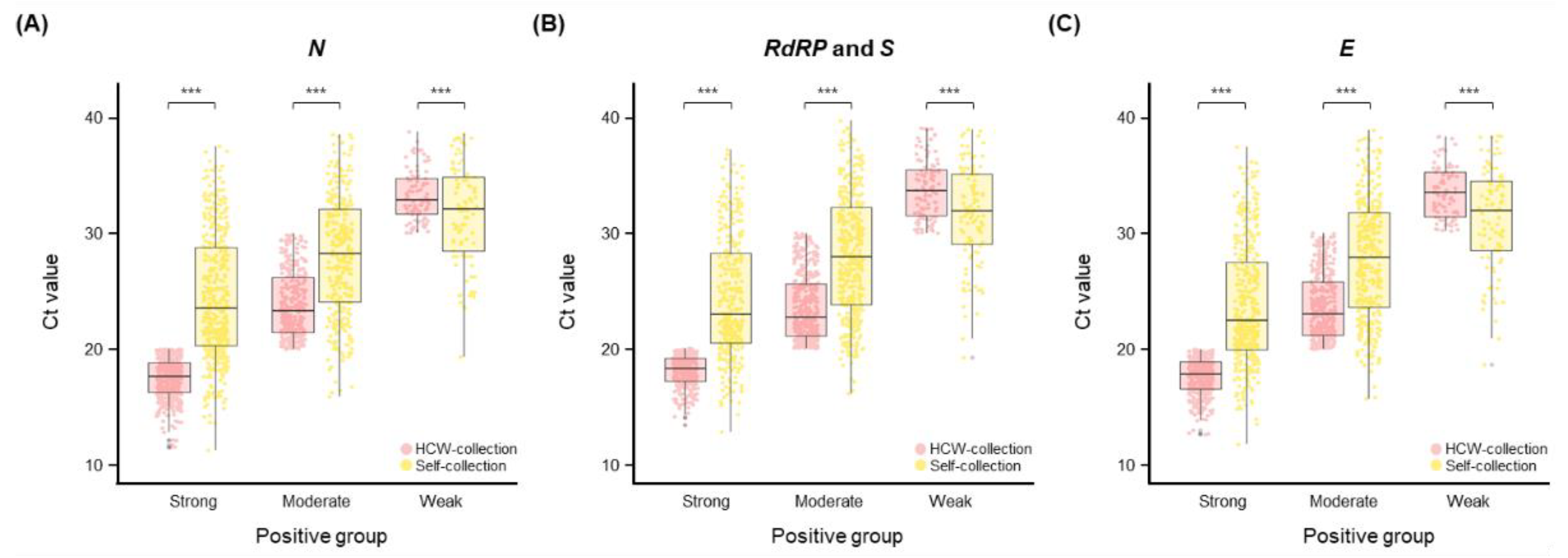
3.5. Comparison of Ct Values in the HCW-Collection and Self-Collection Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef]
- Gisondi, P.; PIaserico, S.; Bordin, C.; Alaibac, M.; Girolomoni, G.; Naldi, L. Cutaneous manifestations of SARS-CoV-2 infection: A clinical update. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 2499–2504. [Google Scholar] [CrossRef]
- World Health Organization. Strategy to Achieve Global COVID-19 Vaccination by mid-2022. Available online: https://www.who.int/publications/m/item/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022 (accessed on 25 May 2022).
- Hsu, L.; Hurrass, J.; Kossow, A.; Klobucnik, J.; Niessen, J.; Wiesmuller, G.A.; Grune, B.; Joisten, C. Breakthrough infections with the SARS-CoV-2 Delta variant: Vaccinations halved transmission risk. Public Health 2022, 204, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Mohapatra, R.K.; Tiwari, R.; Sarangi, A.K.; Sharma, S.K.; Khandia, R.; Saikumar, G.; Dhama, K. Twin combination of Omicron and Delta variants triggering a tsunami wave of ever high surges in COVID-19 cases: A challenging global threat with a special focus on the Indian subcontinent. J. Med. Virol. 2022, 94, 1761–1765. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 11 July 2021).
- Almadhi, M.A.; Abdulrahman, A.; Sharaf, S.A.; AlSaad, D.; Stevenson, N.J.; Atkin, S.L.; AlQahtani, M.M. The high prevalence of asymptomatic SARS-CoV-2 infection reveals the silent spread of COVID-19. Int J. Infect. Dis. 2021, 105, 656–661. [Google Scholar] [CrossRef]
- Hswen, Y.; Brownstein, J.S.; Xu, X.; Yom-Tov, E. Early detection of COVID-19 in China and the USA: Summary of the implementation of a digital decision-support and disease surveillance tool. BMJ Open 2020, 10, e041004. [Google Scholar] [CrossRef]
- Sharma, K.; Aggarwala, P.; Gandhi, D.; Mathias, A.; Singh, P.; Sharma, S.; Negi, S.S.; Bhargava, A.; Das, P.; Gaikwad, U.; et al. Comparative analysis of various clinical specimens in detection of SARS-CoV-2 using rRT-PCR in new and follow up cases of COVID-19 infection: Quest for the best choice. PLoS ONE 2021, 16, e0249408. [Google Scholar] [CrossRef]
- Gertler, M.; Krause, E.; van Loon, W.; Krug, N.; Kausch, F.; Rohardt, C.; Rossig, H.; Michel, J.; Nitsche, A.; Mall, M.A.; et al. Self-collected oral, nasal and saliva samples yield sensitivity comparable to professionally collected oro-nasopharyngeal swabs in SARS-CoV-2 diagnosis among symptomatic outpatients. Int. J. Infect. Dis. 2021, 110, 261–266. [Google Scholar] [CrossRef]
- Hong, K.H.; Kim, G.J.; Roh, K.H.; Sung, H.; Lee, J.; Kim, S.Y.; Kim, T.S.; Park, J.S.; Huh, H.J.; Park, Y.; et al. Update of Guidelines for Laboratory Diagnosis of COVID-19 in Korea. Ann. Lab. Med. 2022, 42, 391–397. [Google Scholar] [CrossRef]
- Mathews, S.S.; Varghese, L.; Trupthi, M.C.; Naomi, N.; Varghese, A.M. COVID-19 Pandemic-Training of Healthcare Workers in Obtaining a Nasopharyngeal Swab: Our Experience. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–5. [Google Scholar] [CrossRef]
- Gadenstaetter, A.J.; Mayer, C.D.; Landegger, L.D. Nasopharyngeal versus nasal swabs for detection of SARS-CoV-2: A systematic review. Rhinology 2021, 59, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Lincango-Naranjo, E.; Espinoza-Suarez, N.; Solis-Pazmino, P.; Vinueza-Moreano, P.; Rodriguez-Villafuerte, S.; Lincango-Naranjo, J.; Barberis-Barcia, G.; Ruiz-Sosa, C.; Rojas-Velasco, G.; Gravholt, D.; et al. Paradigms about the COVID-19 pandemic: Knowledge, attitudes and practices from medical students. BMC Med. Educ. 2021, 21, 128. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Coronavirus (COVID-19) Update: FDA Authorizes An-tigen Test as First Over-the-Counter Fully At-Home Diagnostic Test for COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-antigen-test-first-over-counter-fully-home-diagnostic (accessed on 20 June 2022).
- Brihn, A.; Chang, J.; OYong, K.; Balter, S.; Terashita, D.; Rubin, Z.; Yeganeh, N. Diagnostic Performance of an Antigen Test with RT-PCR for the Detection of SARS-CoV-2 in a Hospital Setting–Los Angeles County, California, June-August 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Chen, Q.Y.; Li, Y.Y.; Wang, Y.F.; Yang, Z.F.; Zhong, N.S. Comparison among nasopharyngeal swab, nasal wash, and oropharyngeal swab for respiratory virus detection in adults with acute pharyngitis. BMC Infect. Dis. 2013, 13, 281. [Google Scholar] [CrossRef]
- Péré, H.; Podglajen, I.; Wack, M.; Flamarion, E.; Mirault, T.; Goudot, G.; Hauw-Berlemont, C.; Le, L.; Caudron, E.; Carrabin, S.; et al. Nasal Swab Sampling for SARS-CoV-2: A Convenient Alternative in Times of Nasopharyngeal Swab Shortage. J. Clin. Microbiol. 2020, 58, e00721-20. [Google Scholar] [CrossRef]
- Hanson, K.E.; Barker, A.P.; Hillyard, D.R.; Gilmore, N.; Barrett, J.W.; Orlandi, R.R.; Shakir, S.M. Self-Collected Anterior Nasal and Saliva Specimens versus Health Care Worker-Collected Nasopharyngeal Swabs for the Molecular Detection of SARS-CoV-2. J. Clin. Microbiol 2020, 58, e01824-20. [Google Scholar] [CrossRef]
- Wurstle, S.; Spinner, C.D.; Voit, F.; Hoffmann, D.; Hering, S.; Weidlich, S.; Schneider, J.; Zink, A.; Treiber, M.; Iakoubov, R.; et al. Self-sampling versus health care professional-guided swab collection for SARS-CoV-2 testing. Infection 2021, 49, 927–934. [Google Scholar] [CrossRef]
- Kojima, N.; Turner, F.; Slepnev, V.; Bacelar, A.; Deming, L.; Kodeboyina, S.; Klausner, J.D. Self-Collected Oral Fluid and Nasal Swabs Demonstrate Comparable Sensitivity to Clinician Collected Nasopharyngeal Swabs for Coronavirus Disease 2019 Detection. Clin. Infect. Dis. 2021, 73, e3106–e3109. [Google Scholar] [CrossRef]
- Nacher, M.; Mergeay-Fabre, M.; Blanchet, D.; Benoit, O.; Pozl, T.; Mesphoule, P.; Sainte-Rose, V.; Vialette, V.; Toulet, B.; Moua, A.; et al. Prospective Comparison of Saliva and Nasopharyngeal Swab Sampling for Mass Screening for COVID-19. Front. Med. 2021, 8, 621160. [Google Scholar] [CrossRef]
- Lim, H.J.; Jung, H.S.; Park, M.Y.; Baek, Y.H.; Kannappan, B.; Park, J.Y.; Yang, J.H.; Seol, J.H.; Lee, M.W.; Jung, S.K.; et al. Evaluation of Three Automated Extraction Systems for the Detection of SARS-CoV-2 from Clinical Respiratory Specimens. Life 2022, 12, 68. [Google Scholar] [CrossRef]
- Di Pilato, V.; Morecchiato, F.; Rizzato, C.; Quaranta, G.; Fais, R.; Gandolfo, C.; Antonelli, A.; Cusi, M.G.; Pistello, M.; Rossolini, G.M.; et al. Validation of Two Commercial Multiplex Real-Time PCR Assays for Detection of SARS-CoV-2 in Stool Donors for Fecal Microbiota Transplantation. Microorganisms 2022, 10, 284. [Google Scholar] [CrossRef] [PubMed]
- Hong, K.H.; Lee, S.W.; Kim, T.S.; Huh, H.J.; Lee, J.; Kim, S.Y.; Park, J.S.; Kim, G.J.; Sung, H.; Roh, K.H.; et al. Guidelines for Laboratory Diagnosis of Coronavirus Disease 2019 (COVID-19) in Korea. Ann. Lab. Med. 2020, 40, 351–360. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Tiiti, T.A.; Mashishi, T.L.; Nkwinika, V.V.; Benoy, I.; Selabe, S.G.; Bogers, J.; Lebelo, R.L. High-risk human papillomavirus detection in self-collected vaginal samples compared with healthcare worker collected cervical samples among women attending gynecology clinics at a tertiary hospital in Pretoria, South Africa. Virol. J. 2021, 18, 192. [Google Scholar] [CrossRef] [PubMed]
- Hossain, A.; Trishna, S.A.; Rashid, A.A.; Khair, S.; Alam, A. Unique mutations in SARS-CoV-2 omicron subvariants’ non-spike proteins: Potential impact on viral pathogenesis and host immune evasion. Microb. Pathog. 2022, 170, 105699. [Google Scholar] [CrossRef]
- Alexiev, I.; Giovanetti, M.; Cella, E.; Ivanov, I.; Stoikov, I.; Donchev, D.; Grigorova, L.; Gancheva, A.; Dimitrova, R.; Korsun, N.; et al. Initial Introduction and Spread of the SARS-CoV-2 AY.4.2.1 Delta Variant in Bulgaria, a Genomic Insight. J. Med. Virol. 2022, 1–5. [Google Scholar] [CrossRef]
- Nora, M.; Deri, D.; Veres, D.S.; Kis, Z.; Barcsay, E.; Palyi, B. Evaluating the field performance of multiple SARS-Cov-2 antigen rapid tests using nasopharyngeal swab samples. PLoS ONE 2022, 17, e0262399. [Google Scholar] [CrossRef]
- Otelea, M.R.; Rascu, A.; Staicu, C.; Calugareanu, L.; Ipate, M.; Teodorescu, S.; Perseca, O.; Voinoiu, A.; Neamtu, A.; Calota, V.; et al. Exhaustion in Healthcare Workers after the First Three Waves of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 8871. [Google Scholar] [CrossRef]
- Caixeta, D.C.; Oliveira, S.W.; Cardoso-Sousa, L.; Cunha, T.M.; Goulart, L.R.; Martins, M.M.; Marin, L.M.; Jardim, A.C.G.; Siqueira, W.L.; Sabino-Silva, R. One-Year Update on Salivary Diagnostic of COVID-19. Front. Public Health 2021, 9, 589564. [Google Scholar] [CrossRef]
- O’Laughlin, K.; Espinosa, C.C.; Smith-Jeffcoat, S.E.; Koh, M.; Khalil, G.M.; Hoffman, A.; Rebolledo, P.A.; Schechter, M.C.; Stewart, R.J.; da Silva, J.; et al. Specimen self-collection for SARS-CoV-2 testing: Patient performance and preferences-Atlanta, Georgia, August-October 2020. PLoS ONE 2022, 17, e0264085. [Google Scholar] [CrossRef]
- Ursic, T.; Kogoj, R.; Sikonja, J.; Roskaric, D.; Jevsnik Virant, M.; Bogovic, P.; Petrovec, M. Performance of nasopharyngeal swab and saliva in detecting Delta and Omicron SARS-CoV-2 variants. J. Med. Virol. 2022, 94, 4704–4711. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Chen, S.; Yang, Z.; Guan, W.; Liu, D.; Lin, Z.; Zhang, Y.; Xu, Z.; Liu, X.; Li, Y. SARS-CoV-2 Viral Load in Clinical Samples from Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2020, 201, 1435–1438. [Google Scholar] [CrossRef]
- Savela, E.S.; Viloria Winnett, A.; Romano, A.E.; Porter, M.K.; Shelby, N.; Akana, R.; Ji, J.; Cooper, M.M.; Schlenker, N.W.; Reyes, J.A.; et al. Quantitative SARS-CoV-2 Viral-Load Curves in Paired Saliva Samples and Nasal Swabs Inform Appropriate Respiratory Sampling Site and Analytical Test Sensitivity Required for Earliest Viral Detection. J. Clin. Microbiol. 2022, 60, e0178521. [Google Scholar] [CrossRef]
- Kohmer, N.; Eckermann, L.; Boddinghaus, B.; Gotsch, U.; Berger, A.; Herrmann, E.; Kortenbusch, M.; Tinnemann, P.; Gottschalk, R.; Hoehl, S.; et al. Self-Collected Samples to Detect SARS-CoV-2: Direct Comparison of Saliva, Tongue Swab, Nasal Swab, Chewed Cotton Pads and Gargle Lavage. J. Clin. Med. 2021, 10, 5751. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.W.; Kim, S.M.; Kim, H.S.; Kim, Y.I.; Kim, J.H.; Cho, J.Y.; Kim, S.H.; Kang, H.; Kim, S.G.; Park, S.J.; et al. Viable SARS-CoV-2 in various specimens from COVID-19 patients. Clin. Microbiol. Infect. 2020, 26, 1520–1524. [Google Scholar] [CrossRef] [PubMed]
- Badu, K.; Oyebola, K.; Zahouli, J.Z.B.; Fagbamigbe, A.F.; de Souza, D.K.; Dukhi, N.; Amankwaa, E.F.; Tolba, M.F.; Sylverken, A.A.; Mosi, L.; et al. SARS-CoV-2 Viral Shedding and Transmission Dynamics: Implications of WHO COVID-19 Discharge Guidelines. Front. Med. 2021, 8, 648660. [Google Scholar] [CrossRef]
- Michel, W.; Farber, J.; Dilas, M.; Heuft, H.G.; Tammer, I.; Baar, J.; Kaasch, A.J. A combined oro-nasopharyngeal swab is more sensitive than mouthwash in detecting SARS-CoV-2 by a high-throughput PCR assay. Infection 2021, 49, 527–531. [Google Scholar] [CrossRef]
- McCulloch, D.J.; Kim, A.E.; Wilcox, N.C.; Logue, J.K.; Greninger, A.L.; Englund, J.A.; Chu, H.Y. Comparison of Unsupervised Home Self-collected Midnasal Swabs With Clinician-Collected Nasopharyngeal Swabs for Detection of SARS-CoV-2 Infection. JAMA Netw. Open 2020, 3, e2016382. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demography/Characteristics | Self-Collection (n = 3990) | HCW-Collection (n = 3990) | ||
|---|---|---|---|---|
| Positive | Negative | Positive | Negative | |
| Collected sample, n | 954 | 3036 | 935 | 3055 |
| Demography | ||||
| Age, years | 22 (20–26) | 24 (21–30) | 22 (20–26) | 24 (21–30) |
| Ct value | ||||
| N | 27.6 (22.3–32.1) | N/A | 20.3 (17.9–26.3) | N/A |
| RdRP and S | 27.9 (22.6–32.5) | N/A | 21.6 (19.1–27.7) | N/A |
| E | 27.0 (22.0–31.9) | N/A | 20.8 (18.2–26.6) | N/A |
| HCW-Collection | |||
|---|---|---|---|
| Positive | Negative | Total | |
| Self-collection | |||
| Positive, n | 850 | 104 | 954 |
| Negative, n | 85 | 2951 | 3036 |
| Total, n | 935 | 3055 | 3990 |
| Sensitivity, % (95% CI) | 90.9 (88.9–92.7) | ||
| Specificity, % (95% CI) | 96.6 (95.9–97.2) | ||
| Cohen’s kappa | 0.87 | ||
| McNemar’s test p-value | 0.19 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.-J.; Baek, Y.-H.; Park, M.-Y.; Yang, J.-H.; Kim, M.-J.; Sung, N.; Sohn, Y.-H.; Lee, S.-H.; Park, J.-E.; Yang, Y.-J. Performance Analysis of Self-Collected Nasal and Oral Swabs for Detection of SARS-CoV-2. Diagnostics 2022, 12, 2279. https://doi.org/10.3390/diagnostics12102279
Lim H-J, Baek Y-H, Park M-Y, Yang J-H, Kim M-J, Sung N, Sohn Y-H, Lee S-H, Park J-E, Yang Y-J. Performance Analysis of Self-Collected Nasal and Oral Swabs for Detection of SARS-CoV-2. Diagnostics. 2022; 12(10):2279. https://doi.org/10.3390/diagnostics12102279
Chicago/Turabian StyleLim, Ho-Jae, Young-Hyun Baek, Min-Young Park, Jae-Hyun Yang, Min-Jin Kim, Nackmoon Sung, Yong-Hak Sohn, Sun-Hwa Lee, Jung-Eun Park, and Yong-Jin Yang. 2022. "Performance Analysis of Self-Collected Nasal and Oral Swabs for Detection of SARS-CoV-2" Diagnostics 12, no. 10: 2279. https://doi.org/10.3390/diagnostics12102279