
Enhance Portable Radiograph for Fast and High Accurate COVID-19 Monitoring


Abstract
:1. Introduction
- Firstly, we introduce a novel database collection of subject-pairs radiographs. For each subject, we collect a pair of samples which are from both portable machines (source domain) and conventional machines (target domain).
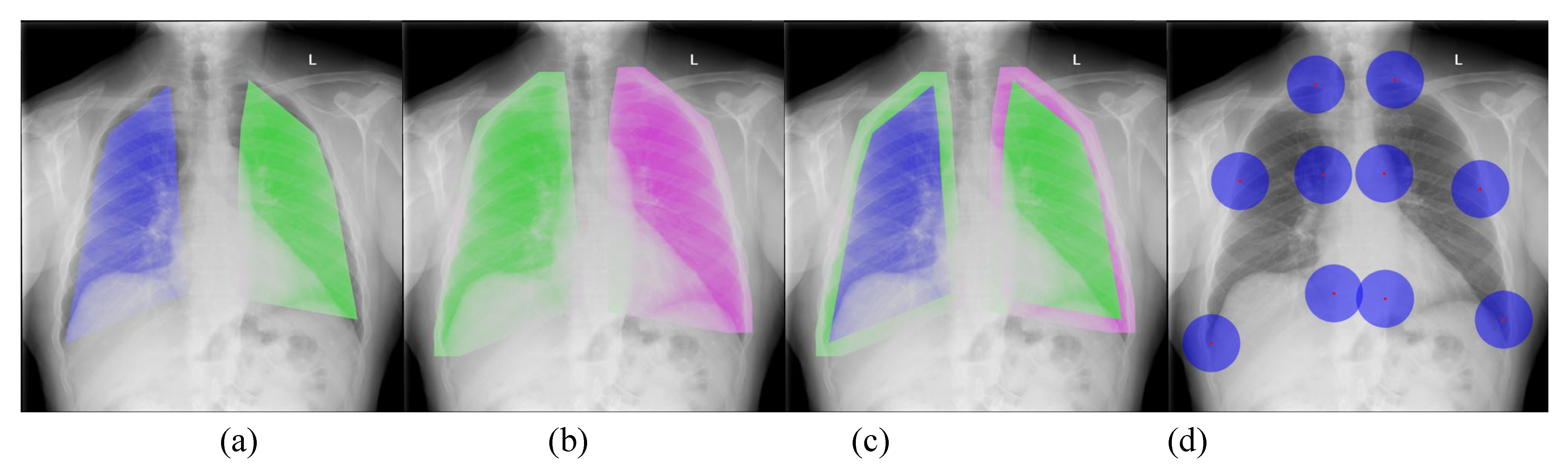
- Secondly, we introduce a new deep learning-based approach to align a subject-pairs dataset to obtain pixel-pairs dataset. In order to learn the knowledge correlation between two different domains, it is important to have a pixel-wise pair dataset. Thus, alignment is an important step that helps to perform knowledge transferring from the source domain to target domain.
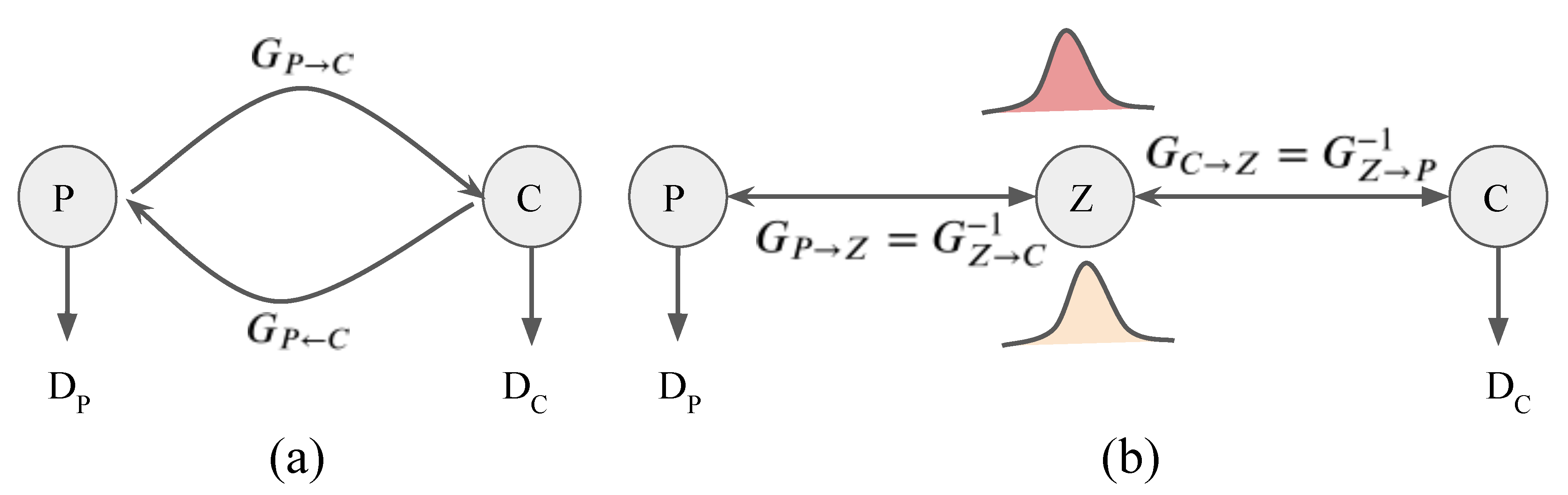
- Thirdly, we propose a new PairFlow approach, an end-to-end invertible transfer of a deep learning method, to enhance the degraded CXRs from the portable machine. High-quality knowledge is then transferred to a degraded domain to increase the portable CXRs quality.
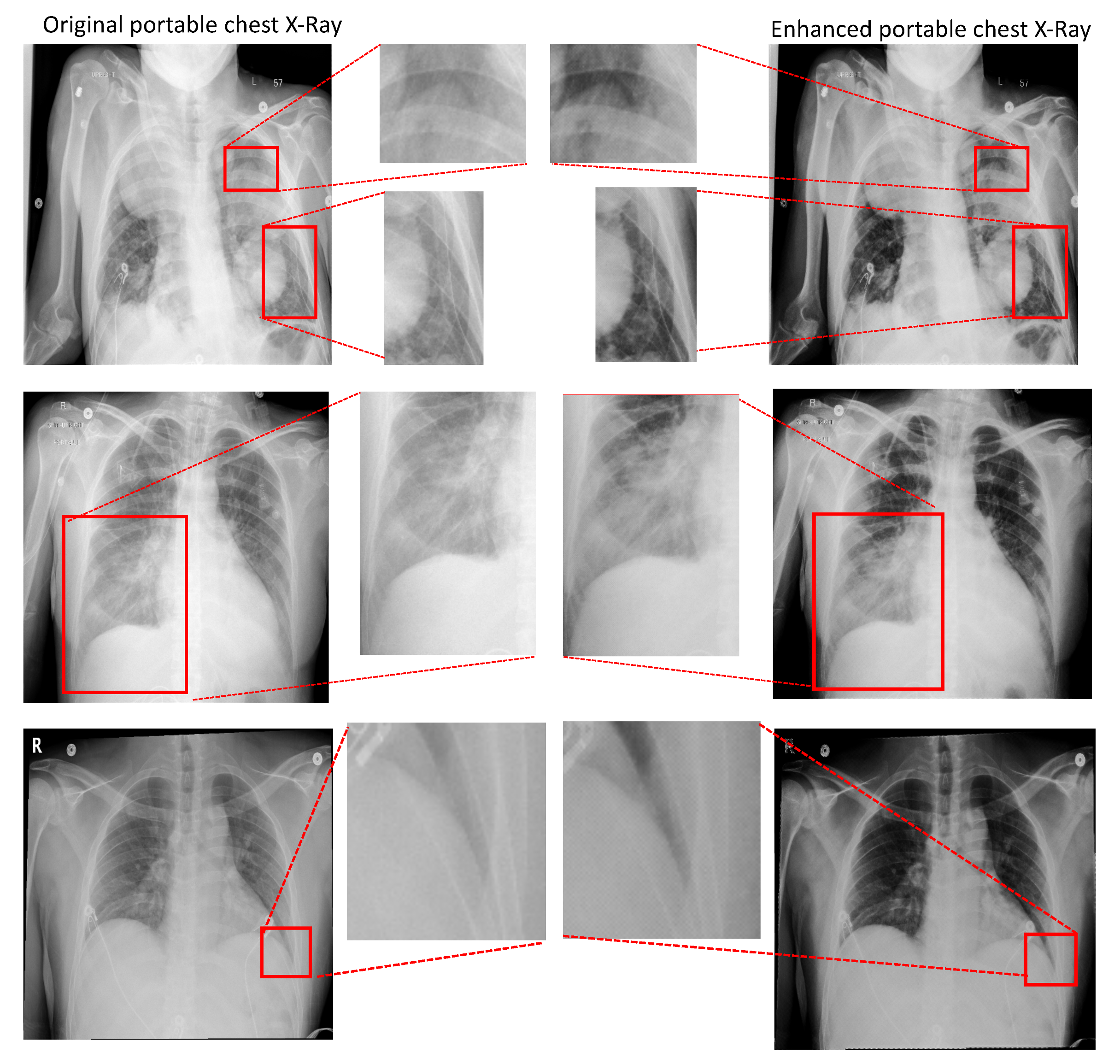
- Finally, we evaluate the system performance at both image-quality enhancement and topological properties.
2. Related Works and Background
2.1. Generative Adversarial Networks
2.2. Flow-Based Generative Networks
2.3. Comparison between GANs (cycleGAN) and Flow-Based Generative Networks
2.4. Deep Learning for COVID-19 on CXR
3. Our Proposed Method
- C: target domain—CXR from conventional machines;
- : each CXR in the target domain C;
- P: source domain—CXR from portable machines;
- : each CXR in the source domain.
3.1. Portable Radiograph Alignment
3.2. Portable Radiograph Quality Enhancement
3.2.1. Mapping Function via ResNet Layers
3.2.2. The Radiograph Enhancement Embedding
3.2.3. Enhancement Model Learning
4. Experimental Results
4.1. Database
4.2. Implementation Details
4.3. Results and Discussion
4.3.1. CXR Alignment Network
4.3.2. Portable Radiographs Quality Enhancement
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mossa-Basha, M.; Meltzer, C.C.; Kim, D.C.; Tuite, M.J.; Kolli, K.P.; Tan, B.S. Radiology department preparedness for COVID-19: Radiology scientific expert review panel. Radiology 2020, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooraki, S.; Hosseiny, M.; Myers, L.; Gholamrezanezhad, A. Coronavirus (COVID-19) Outbreak: What the Department of Radiology Should Know. J. Am. Coll. Radiol. 2020, 17, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Schluger, N.W.; Volpi, A.; Yim, J.J.; Martin, I.B.; et al. The role of chest imaging in patient management during the COVID-19 pandemic: A multinational consensus statement from the Fleischner Society. Chest 2020, 158, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Li, X. Mobile X-rays are highly valuable for critically ill COVID patients. Eur. Radiol. 2020, 30, 5217–5219. [Google Scholar] [CrossRef]
- Gaitan, D. Portable X-ray Services Becoming More Common. Available online: https://www.reuters.com/article/us-portable-xrays/portable-x-ray-services-becoming-more-common-idUSKBN0KW1ZN20150123 (accessed on 31 May 2021).
- Jensen, L.; Meyer, C. Reducing Errors in Portable Chest Radiography. Available online: https://appliedradiology.com/articles/reducing-errors-in-portable-chest-radiography (accessed on 31 May 2021).
- Portable versus Fixed X-ray Equipment: A Review of the Clinical Effectiveness, Cost-Effectiveness, and Guidelines; Canadian Agency for Drugs and Technologies in Health: Ottawa, ON, Canada, 22 February 2016. Available online: https://pubmed.ncbi.nlm.nih.gov/27030858/ (accessed on 31 May 2021).
- Sprawls, P. Scattered Radiation and Contrast. Available online: http://www.sprawls.org/ppmi2/SCATRAD/ (accessed on 31 May 2021).
- Barnes, G.T. Contrast and scatter in X-ray imaging. RadioGraphics 1991, 11, 307–323. [Google Scholar] [CrossRef] [Green Version]
- Barski, L.; Couwenhoven, M. Improving the Quality of Mobile Chest X-rays. Available online: https://www.carestream.com/blog/2019/02/12/improving-the-quality-of-mobile-chest-x-rays/ (accessed on 31 May 2021).
- Chen, X.; Lian, C.; Wang, L.; Deng, H.; Fung, S.H.; Nie, D.; Thung, K.H.; Yap, P.T.; Gateno, J.; Xia, J.J.; et al. One-Shot Generative Adversarial Learning for MRI Segmentation of Craniomaxillofacial Bony Structures. IEEE Trans. Med. Imaging 2019, 39, 787–796. [Google Scholar] [CrossRef]
- Welander, P.; Karlsson, S.; Eklund, A. Generative adversarial networks for image-to-image translation on multi-contrast MR images-A comparison of CycleGAN and UNIT. arXiv 2018, arXiv:1806.07777. [Google Scholar]
- Zhu, J.Y.; Park, T.; Isola, P.; Efros, A.A. Unpaired image-to-image translation using cycle-consistent adversarial networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2223–2232. [Google Scholar]
- Dinh, L.; Sohl-Dickstein, J.; Bengio, S. Density estimation using real nvp. arXiv 2016, arXiv:1605.08803. [Google Scholar]
- Grover, A.; Chute, C.; Shu, R.; Cao, Z.; Ermon, S. AlignFlow: Cycle Consistent Learning from Multiple Domains via Normalizing Flows. arXiv 2019, arXiv:1905.12892. [Google Scholar] [CrossRef]
- Kingma, D.P.; Dhariwal, P. Glow: Generative flow with invertible 1x1 convolutions. arXiv 2018, arXiv:1807.03039. [Google Scholar]
- van der Ouderaa, T.F.; Worrall, D.E. Reversible gans for memory-efficient image-to-image translation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 16–20 June 2019; pp. 4720–4728. [Google Scholar]
- Sun, H.; Mehta, R.; Zhou, H.H.; Huang, Z.; Johnson, S.C.; Prabhakaran, V.; Singh, V. DUAL-GLOW: Conditional Flow-Based Generative Model for Modality Transfer. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Seoul, Korea, 27 October–2 November 2019; pp. 10611–10620. [Google Scholar]
- Duong, C.N.; Truong, T.D.; Quach, K.G.; Bui, H.; Roy, K.; Luu, K. Vec2Face: Unveil Human Faces from their Blackbox Features in Face Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 14–18 June 2020. [Google Scholar]
- Duong, C.N.; Quach, K.G.; Luu, K.; Le, N.; Savvides, M. Temporal Non-Volume Preserving Approach to Facial Age-Progression and Age-Invariant Face Recognition. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar]
- Duong, C.N.; Quach, K.G.; Luu, K.; Le, T.H.N.; Savvides, M.; Bui, T.D. Learning from Longitudinal Face Demonstration—Where Tractable Deep Modeling Meets Inverse Reinforcement Learning. Int. J. Comput. Vis. 2019, 127, 957–971. [Google Scholar] [CrossRef] [Green Version]
- Bui, T.; Nguyen, M.; Le, N.T.; Luu, K. Flow-based Deformation Guidance for Unpaired Multi-Contrast MRI Image-to-Image Translation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020. [Google Scholar]
- Alam, N.A.; Ahsan, M.; Based, M.A.; Haider, J.; Kowalski, M. COVID-19 Detection from Chest X-ray Images Using Feature Fusion and Deep Learning. Sensors 2021, 21, 1480. [Google Scholar] [CrossRef]
- Li, X.; Li, C.; Zhu, D. Covid-mobilexpert: On-device COVID-19 screening using snapshots of chest X-ray. arXiv 2020, arXiv:2004.03042. [Google Scholar]
- Minaee, S.; Kafieh, R.; Sonka, M.; Yazdani, S.; Soufi, G.J. Deep-covid: Predicting COVID-19 from chest X-ray images using deep transfer learning. Med. Image Anal. 2020, 65, 101794. [Google Scholar] [CrossRef]
- Khobahi, S.; Agarwal, C.; Soltanalian, M. Coronet: A deep network architecture for semi-supervised task-based identification of COVID-19 from chest X-ray images. medRxiv 2020. [Google Scholar] [CrossRef]
- Ucar, F.; Korkmaz, D. COVIDiagnosis-Net: Deep Bayes-SqueezeNet based diagnosis of the coronavirus disease 2019 (COVID-19) from X-ray images. Med. Hypotheses 2020, 140, 109761. [Google Scholar] [CrossRef] [PubMed]
- Afshar, P.; Heidarian, S.; Naderkhani, F.; Oikonomou, A.; Plataniotis, K.N.; Mohammadi, A. Covid-caps: A capsule network-based framework for identification of COVID-19 cases from X-ray images. Pattern Recognit. Lett. 2020, 138, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Lin, Z.Q.; Wong, A. Covid-net: A tailored deep convolutional neural network design for detection of COVID-19 cases from chest X-ray images. Sci. Rep. 2020, 10, 1–12. [Google Scholar]
- Tartaglione, E.; Barbano, C.A.; Berzovini, C.; Calandri, M.; Grangetto, M. Unveiling COVID-19 from chest X-ray with deep learning: A hurdles race with small data. Int. J. Environ. Res. Public Health 2020, 17, 6933. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, A.; Mittal, S.; Majumdar, P.; Chhabra, S.; Thakral, K.; Vatsa, M.; Singh, R.; Chaudhury, S.; Pudrod, A.; Agrawal, A. Multi-Task Driven Explainable Diagnosis of COVID-19 using Chest X-ray Images. arXiv 2020, arXiv:2008.03205. [Google Scholar]
- Rahaman, M.M.; Li, C.; Yao, Y.; Kulwa, F.; Rahman, M.A.; Wang, Q.; Qi, S.; Kong, F.; Zhu, X.; Zhao, X. Identification of COVID-19 samples from chest X-ray images using deep learning: A comparison of transfer learning approaches. J. X-ray Sci. Technol. 2020, 28, 821–839. [Google Scholar] [CrossRef]
- Tsiknakis, N.; Trivizakis, E.; Vassalou, E.E.; Papadakis, G.Z.; Spandidos, D.A.; Tsatsakis, A.; Sánchez-García, J.; López-González, R.; Papanikolaou, N.; Karantanas, A.H.; et al. Interpretable artificial intelligence framework for COVID-19 screening on chest X-rays. Exp. Ther. Med. 2020, 20, 727–735. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Heidari, M.; Mirniaharikandehei, S.; Khuzani, A.Z.; Danala, G.; Qiu, Y.; Zheng, B. Improving the performance of CNN to predict the likelihood of COVID-19 using chest X-ray images with preprocessing algorithms. Int. J. Med. Inform. 2020, 144, 104284. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE International Conference on Computer Vision (CVPR), Santiago, Chile, 7–13 December 2015; pp. 770–778. [Google Scholar]
- Wang, Z.; Xiao, Y.; Li, Y.; Zhang, J.; Lu, F.; Hou, M.; Liu, X. Automatically discriminating and localizing COVID-19 from community-acquired pneumonia on chest X-rays. Pattern Recognit. 2021, 110, 107613. [Google Scholar] [CrossRef]
- Zhang, R.; Guo, Z.; Sun, Y.; Lu, Q.; Xu, Z.; Yao, Z.; Duan, M.; Liu, S.; Ren, Y.; Huang, L.; et al. COVID19XrayNet: A Two-Step Transfer Learning Model for the COVID-19 Detecting Problem Based on a Limited Number of Chest X-ray Images. Interdiscip. Sci. Comput. Life Sci. 2020, 12, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the 36th International Conference on Machine Learning, PMLR, Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar]
- Luz, E.; Silva, P.L.; Silva, R.; Silva, L.; Moreira, G.; Menotti, D. Towards an effective and efficient deep learning model for COVID-19 patterns detection in X-ray images. arXiv 2020, arXiv:2004.05717. [Google Scholar]
- Zhang, R.; Tie, X.; Qi, Z.; Bevins, N.B.; Zhang, C.; Griner, D.; Song, T.K.; Nadig, J.D.; Schiebler, M.L.; Garrett, J.W.; et al. Diagnosis of coronavirus disease 2019 pneumonia by using chest radiography: Value of artificial intelligence. Radiology 2021, 298, E88–E97. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, D.; Hassanien, A.E.; Ella, H.A. An optimized deep learning architecture for the diagnosis of COVID-19 disease based on gravitational search optimization. Appl. Soft Comput. 2020, 98, 106742. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.P.; Morrison, P.; Dao, L.; Roth, K.; Duong, T.Q.; Ghassemi, M. COVID-19 image data collection: Prospective predictions are the future. arXiv 2020, arXiv:2006.11988. [Google Scholar]
- Actualmed COVID-19 Chest X-ray Data Initiative. Available online: https://github.com/agchung/Actualmed-COVID-chestxray-dataset (accessed on 31 May 2021).
- Chowdhury, M.E.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Al Emadi, N.; et al. Can AI help in screening viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- RSNA Pneumonia Detection Challenge. Available online: https://www.kaggle.com/c/rsna-pneumonia-detection-challenge (accessed on 31 May 2021).
- Rocco, I.; Arandjelovic, R.; Sivic, J. Convolutional neural network architecture for geometric matching. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 6148–6157. [Google Scholar]
- Wang, Z.; Bovik, A.C.; Sheikh, H.R.; Simoncelli, E.P. Image Quality Assessment: From Error Visibility to Structural Similarity. IEEE Trans. Image Process. 2004, 13, 600–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Portable CXR vs. Conventional CXR | Aligned CXR vs. Conventional CXR | |
|---|---|---|
| Left Lung | 203.03 | 42.02 |
| Right Lung | 239.31 | 38.86 |
| Entire CXR | 221.17 | 40.44 |
| RoIs | PSNR ↑ | SSIM ↑ | ||
|---|---|---|---|---|
| Por.CXR vs. Con.CXR | Enh.CXR vs. Con.CXR | Por.CXR vs. Con.CXR | Enh.CXR vs. Con.CXR | |
| 28.019/0.245 | 30.273/1.798 | 0.936/0.018 | 0.960/0.011 | |
| 28.003/0.236 | 30.437/1.707 | 0.748/0.047 | 0.787/0.045 | |
| 29.009/0.229 | 30.474/1.724 | 0.919/0.021 | 0.955/0.013 | |
| 28.006/0.227 | 30.522/1.662 | 0.729/0.050 | 0.780/0.047 | |
| 28.011/0.205 | 30.407/1.670 | 0.873/0.035 | 0.920/0.021 | |
| 28.009/0.198 | 30.498/1.629 | 0.839/0.044 | 0.910/0.026 | |
| RoIs | PSNR ↑ | SSIM ↑ | ||
|---|---|---|---|---|
| Por.CXR vs. Con.CXR | Enh.CXR vs. B | Por.CXR vs. Con.CXR | Enh.CXR vs. Con.CXR | |
| P1 | 27.995/0.970 | 28.780/3.338 | 0.675/0.195 | 0.723/0.086 |
| P2 | 28.079/1.126 | 29.911/2.783 | 0.756/0.065 | 0.763/0.062 |
| P3 | 28.196/1.290 | 30.025/3.031 | 0.669/0.187 | 0.736/0.101 |
| P4 | 27.960/0.672 | 30.519/2.453 | 0.706/0.076 | 0.795/0.051 |
| P5 | 27.898/0.538 | 29.007/2.444 | 0.683/0.077 | 0.736/0.084 |
| P6 | 28.159/1.097 | 28.523/3.328 | 0.699/0.153 | 0.720/0.098 |
| P7 | 28.407/1.143 | 29.576/2.354 | 0.733/0.070 | 0.778/0.059 |
| P8 | 28.595/1.786 | 31.005/2.201 | 0.776/0.063 | 0.802/0.052 |
| P9 | 28.075/0.826 | 30.485/3.503 | 0.721/0.079 | 0.737/0.134 |
| P10 | 27.940/0.676 | 30.738/2.589 | 0.713/0.070 | 0.767/0.067 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, N.; Sorensen, J.; Bui, T.; Choudhary, A.; Luu, K.; Nguyen, H. Enhance Portable Radiograph for Fast and High Accurate COVID-19 Monitoring. Diagnostics 2021, 11, 1080. https://doi.org/10.3390/diagnostics11061080
Le N, Sorensen J, Bui T, Choudhary A, Luu K, Nguyen H. Enhance Portable Radiograph for Fast and High Accurate COVID-19 Monitoring. Diagnostics. 2021; 11(6):1080. https://doi.org/10.3390/diagnostics11061080
Chicago/Turabian StyleLe, Ngan, James Sorensen, Toan Bui, Arabinda Choudhary, Khoa Luu, and Hien Nguyen. 2021. "Enhance Portable Radiograph for Fast and High Accurate COVID-19 Monitoring" Diagnostics 11, no. 6: 1080. https://doi.org/10.3390/diagnostics11061080