
Motor Cortical Activation Assessment in Progressive Multiple Sclerosis Patients Enrolled in Gait Rehabilitation: A Secondary Analysis of the RAGTIME Trial Assisted by Functional Near-Infrared Spectroscopy

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Rehabilitation Treatments
2.3. Outcome Measures
2.3.1. Cortical Activation
2.3.2. Performance Parameters
2.4. Statistical Analysis
3. Results
3.1. Cortical Activation at Baseline
3.2. Cortical Activation Changes after Rehabilitation
3.3. Concomitant Variations in Cortical Activation and Functional Parameters
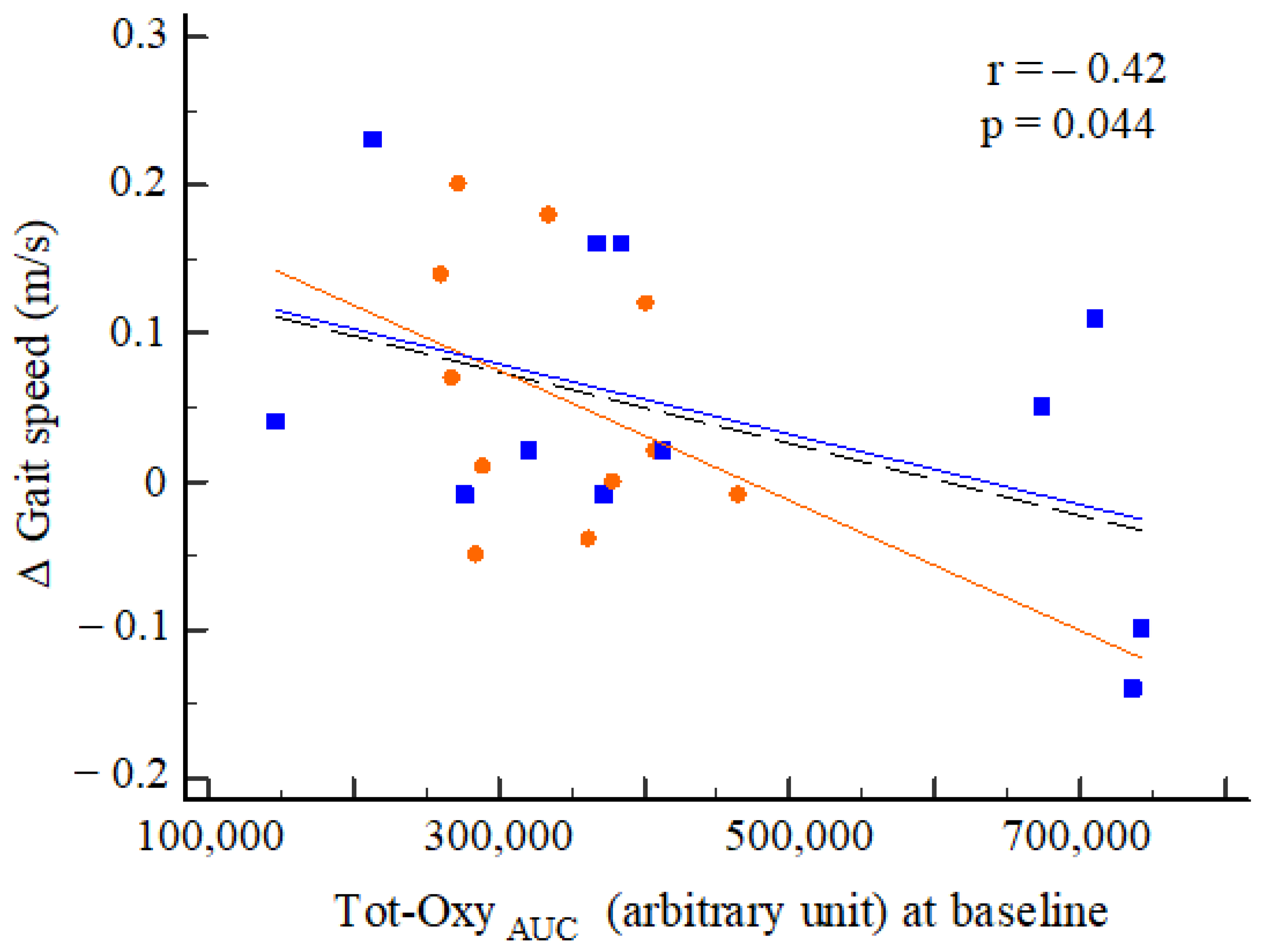
3.4. Baseline Cortical Activation and Rehabilitation Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amatya, B.; Khan, F.; Galea, M. Rehabilitation for people with multiple sclerosis: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2019, 1, CD012732. [Google Scholar] [CrossRef]
- Ontaneda, D.; Thompson, A.J.; Fox, R.J.; Cohen, J.A. Progressive multiple sclerosis: Prospects for disease therapy; repair; and restoration of function. Lancet 2017, 389, 1357–1366. [Google Scholar] [CrossRef]
- Barten, L.J.; Allington, D.R.; Procacci, K.A.; Rivey, M.P. New approaches in the management of multiple sclerosis. Drug Des. Dev. Ther. 2010, 4, 343–366. [Google Scholar]
- Heesen, C.; Böhm, J.; Reich, C.; Kasper, J.; Goebel, M.; Gold, S.M. Patient perception of bodily functions in multiple sclerosis: Gait and visual function are the most valuable. Mult. Scler. 2008, 14, 988–991. [Google Scholar] [CrossRef] [PubMed]
- Van Asch, P. Impact of mobility impairment in multiple sclerosis 2—Patients’ perspectives. Eur. Neurol. Rev. 2011, 6, 115–120. [Google Scholar] [CrossRef]
- Scalfari, A.; Neuhaus, A.; Degenhardt, A.; Rice, G.P.; Muraro, P.A.; Daumer, M.; Ebers, G.C. The natural history of multiple sclerosis, a geographically based study 10: Relapses and long-term disability. Brain 2010, 133, 1914–1929. [Google Scholar] [CrossRef]
- Kieseier, B.C.; Pozzilli, C. Assessing walking disability in multiple sclerosis. Mult. Scler. 2012, 18, 914–924. [Google Scholar] [CrossRef] [PubMed]
- Amatya, B.; Khan, F.; La Mantia, L.; Demetrios, M.; Wade, D.T. Non pharmacological interventions for spasticity in multiple sclerosis. Cochrane Database Syst. Rev. 2013, CD009974. [Google Scholar] [CrossRef] [PubMed]
- Beer, S.; Khan, F.; Kesselring, J. Rehabilitation interventions in multiple sclerosis: An overview. J. Neurol. 2012, 259, 1994–2008. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Pallant, J.F. Use of the International Classification of Functioning; Disability and Health (ICF) to identify preliminary comprehensive and brief core sets for multiple sclerosis. Disabil. Rehabil. 2007, 29, 205–213. [Google Scholar] [CrossRef]
- Wiles, C.M.; Newcombe, R.G.; Fuller, K.J.; Shaw, S.; Furnival-Doran, J.; Pickersgill, T.P.; Morgan, A. Controlled randomised crossover trial of the effects of physiotherapy on mobility in chronic multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2001, 70, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straudi, S.; Fanciullacci, C.; Martinuzzi, C.; Pavarelli, C.; Rossi, B.; Chisari, C.; Basaglia, N. The effects of robot-assisted gait training in progressive multiple sclerosis: A randomized controlled trial. Mult. Scler. 2016, 22, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Straudi, S.; Manfredini, F.; Lamberti, N.; Martinuzzi, C.; Maietti, E.; Basaglia, N. Robot-assisted gait training is not superior to intensive overground walking in multiple sclerosis with severe disability (the RAGTIME study): A randomized controlled trial. Mult. Scler. 2020, 26, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Bowman, T.; Gervasoni, E.; Amico, A.P.; Antenucci, R.; Benanti, P.; Boldrini, P.; Bonaiuti, D.; Burini, A.; Castelli, E.; Draicchio, F.; et al. What is the impact of robotic rehabilitation on balance and gait outcomes in people with multiple sclerosis? A systematic review of randomized control trials. Eur. J. Phys. Rehabil. Med. 2021, 57, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.W.; Lin, L.F.; Tam, K.W.; Tsai, C.P.; Hong, C.H.; Kuan, Y.C. Efficacy of robot-assisted gait training in multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2020, 41, 102034. [Google Scholar] [CrossRef] [PubMed]
- Tomassini, V.; Matthews, P.M.; Thompson, A.J.; Fuglø, D.; Geurts, J.J.; Johansen-Berg, H.; Jones, D.K.; Rocca, M.A.; Wise, R.G.; Barkhof, F.; et al. Neuroplasticity and functional recovery in multiple sclerosis. Nat. Rev. Neurol. 2012, 8, 635–646. [Google Scholar] [CrossRef]
- Bonilauri, A.; Sangiuliano Intra, F.; Pugnetti, L.; Baselli, G.; Baglio, F. A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases-Actual Applications and Future Perspectives. Diagnostics 2020, 10, 581. [Google Scholar] [CrossRef]
- Risacher, S.L.; Saykin, A.J. Neuroimaging biomarkers of neurodegenerative diseases and dementia. Semin. Neurol. 2013, 33, 386–416. [Google Scholar] [CrossRef] [Green Version]
- Prosperini, L.; Di Filippo, M. Beyond clinical changes: Rehabilitation-induced neuroplasticity in MS. Mult. Scler. 2019, 25, 1348–1362. [Google Scholar] [CrossRef] [PubMed]
- Yücel, M.A.; Selb, J.J.; Huppert, T.J.; Franceschini, M.A.; Boas, D.A. Functional Near Infrared Spectroscopy: Enabling Routine Functional Brain Imaging. Curr. Opin. Biomed. Eng. 2017, 4, 78–86. [Google Scholar] [CrossRef]
- Yang, R.; Dunn, J.F. Reduced cortical microvascular oxygenation in multiple sclerosis: A blinded; case-controlled study using a novel quantitative near-infrared spectroscopy method. Sci. Rep. 2015, 5, 16477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mihara, M.; Miyai, I. Review of functional near-infrared spectroscopy in neurorehabilitation. Neurophotonics 2016, 3, 031414. [Google Scholar] [CrossRef]
- Gramigna, V.; Pellegrino, G.; Cerasa, A.; Cutini, S.; Vasta, R.; Olivadese, G.; Martino, I.; Quattrone, A. Near-Infrared Spectroscopy in Gait Disorders: Is It Time to Begin? Neurorehabil. Neural Repair 2017, 31, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Broscheid, K.C.; Hamacher, D.; Lamprecht, J.; Sailer, M.; Schega, L. Inter-Session Reliability of Functional Near-Infrared Spectroscopy at the Prefrontal Cortex While Walking in Multiple Sclerosis. Brain Sci. 2020, 10, 643. [Google Scholar] [CrossRef] [PubMed]
- Bishnoi, A.; Holtzer, R.; Hernandez, M.E. Brain Activation Changes While Walking in Adults with and without Neurological Disease: Systematic Review and Meta-Analysis of Functional Near-Infrared Spectroscopy Studies. Brain Sci. 2021, 11, 291. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.C.; Sur, M.; Dobkin, B.H.; ’O’Brien, C.; Sanger, T.D.; Trojanowski, J.Q.; Rumsey, J.M.; Hicks, R.; Cameron, J.; Chen, D.; et al. Harnessing neuroplasticity for clinical applications. Brain 2011, 134, 1591–1609. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Izumiyama, M.; Koizumi, H.; Takahashi, A.; Itoyama, Y. Near-infrared spectroscopic topography as a tool to monitor motor reorganization after hemiparetic stroke: A comparison with functional MRI. Stroke 2002, 33, 2032–2036. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Yang, S.P.; Park, G.L.; Kim, E.J.; You, J.S. Best facilitated cortical activation during different stepping; treadmill; and robot-assisted walking training paradigms and speeds: A functional near-infrared spectroscopy neuroimaging study. NeuroRehabilitation 2016, 38, 171–178. [Google Scholar] [CrossRef]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Straudi, S.; Manfredini, F.; Lamberti, N.; Zamboni, P.; Bernardi, F.; Marchetti, G.; Pinton, P.; Bonora, M.; Secchiero, P.; Tisato, V.; et al. The effectiveness of Robot-Assisted Gait Training versus conventional therapy on mobility in severely disabled progressIve MultiplE sclerosis patients (RAGTIME): Study protocol for a randomized controlled trial. Trials 2017, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, F.; Malagoni, A.M.; Felisatti, M.; Mandini, S.; Mascoli, F.; Manfredini, R.; Basaglia, N.; Zamboni, P. A dynamic objective evaluation of peripheral arterial disease by near-infrared spectroscopy. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 441–448. [Google Scholar] [CrossRef] [Green Version]
- Manfredini, F.; Malagoni, A.M.; Mandini, S.; Felisatti, M.; Mascoli, F.; Basaglia, N.; Manfredini, R.; Mikhailidis, D.P.; Zamboni, P. Near-infrared spectroscopy assessment following exercise training in patients with intermittent claudication and in untrained healthy participants. Vasc. Endovasc. Surg. 2012, 46, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, F.; Lamberti, N.; Ficarra, V.; Tsolaki, E.; Straudi, S.; Zamboni, P.; Basaglia, N.; Gasbarro, V. Biomarkers of Muscle Metabolism in Peripheral Artery Disease: A Dynamic NIRS-Assisted Study to Detect Adaptations Following Revascularization and Exercise Training. Diagnostics 2020, 10, 312. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, F.; Straudi, S.; Lamberti, N.; Patergnani, S.; Tisato, V.; Secchiero, P.; Bernardi, F.; Ziliotto, N.; Marchetti, G.; Basaglia, N.; et al. Rehabilitation Improves Mitochondrial Energetics in Progressive Multiple Sclerosis: The Significant Role of Robot-Assisted Gait Training and of the Personalized Intensity. Diagnostics 2020, 10, 834. [Google Scholar] [CrossRef] [PubMed]
- Quaresima, V.; Sacco, S.; Totaro, R.; Ferrari, M. Noninvasive measurement of cerebral hemoglobin oxygen saturation using two near infrared spectroscopy approaches. J. Biomed. Opt. 2000, 5, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.D.; Marrie, R.A.; Cohen, J.A. Evaluation of the six-minute walk in multiple sclerosis subjects and healthy controls. Mult. Scler. 2008, 14, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, D.; Regola, A.; Meotti, M. Validity of six balance disorders scales in persons with multiple sclerosis. Disabil. Rehabil. 2006, 28, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Miyai, I.; Tanabe, H.C.; Sase, I.; Eda, H.; Oda, I.; Konishi, I.; Tsunazawa, Y.; Suzuki, T.; Yanagida, T.; Kubota, K. Cortical mapping of gait in humans: A near-infrared spectroscopic topography study. NeuroImage 2001, 14, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S. The clinical course of multiple sclerosis. Handb. Clin. Neurol. 2014, 122, 343–369. [Google Scholar] [CrossRef]
- Stuart, S.; Vitorio, R.; Morris, R.; Martini, D.N.; Fino, P.C.; Mancini, M. Cortical activity during walking and balance tasks in older adults and in people with Parkinson’s disease: A structured review. Maturitas 2018, 113, 53–72. [Google Scholar] [CrossRef] [Green Version]
- Miyai, I.; Yagura, H.; Hatakenaka, M.; Oda, I.; Konishi, I.; Kubota, K. Longitudinal optical imaging study for locomotor recovery after stroke. Stroke 2003, 34, 2866–2870. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.E.; Holtzer, R.; Chaparro, G.; Jean, K.; Balto, J.M.; Sandroff, B.M.; Izzetoglu, M.; Motl, R.W. Brain activation changes during locomotion in middle-aged to older adults with multiple sclerosis. J. Neurol. Sci. 2016, 370, 277–283. [Google Scholar] [CrossRef]
- Saleh, S.; Sandroff, B.M.; Vitiello, T.; Owoeye, O.; Hoxha, A.; Hake, P.; Goverover, Y.; Wylie, G.; Yue, G.; DeLuca, J. The Role of Premotor Areas in Dual Tasking in Healthy Controls and Persons with Multiple Sclerosis: An fNIRS Imaging Study. Front. Behav. Neurosci. 2018, 12, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jimenez, J.J.; Yang, R.; Nathoo, N.; Varshney, V.P.; Golestani, A.M.; Goodyear, B.G.; Metz, L.M.; Dunn, J.F. Detection of reduced interhemispheric cortical communication during task execution in multiple sclerosis patients using functional near-infrared spectroscopy. J. Biomed. Opt. 2014, 19, 076008. [Google Scholar] [CrossRef] [PubMed]
- Reddy, H.; Narayanan, S.; Arnoutelis, R.; Jenkinson, M.; Antel, J.; Matthews, P.M.; Arnold, D.L. Evidence for adaptive functional changes in the cerebral cortex with axonal injury from multiple sclerosis. Brain 2000, 123, 2314–2320. [Google Scholar] [CrossRef] [Green Version]
- Manson, S.C.; Palace, J.; Frank, J.A.; Matthews, P.M. Loss of interhemispheric inhibition in patients with multiple sclerosis is related to corpus callosum atrophy. Exp. Brain Res. 2006, 174, 728–733. [Google Scholar] [CrossRef]
- Lenzi, D.; Conte, A.; Mainero, C.; Frasca, V.; Fubelli, F.; Totaro, P.; Caramia, F.; Inghilleri, M.; Pozzilli, C.; Pantano, P. Effect of corpus callosum damage on ipsilateral motor activation in patients with multiple sclerosis: A functional and anatomical study. Hum. Brain Mapp. 2007, 28, 636–644. [Google Scholar] [CrossRef]
- Mezzapesa, D.M.; Rocca, M.A.; Rodegher, M.; Comi, G.; Filippi, M. Functional cortical changes of the sensorimotor network are associated with clinical recovery in multiple sclerosis. Hum. Brain Mapp. 2008, 29, 562–573. [Google Scholar] [CrossRef]
- Lefeber, N.; Swinnen, E.; Kerckhofs, E. The immediate effects of robot-assistance on energy consumption and cardiorespiratory load during walking compared to walking without robot-assistance: A systematic review. Disabil. Rehabil. Assist. Technol. 2017, 12, 657–671. [Google Scholar] [CrossRef] [PubMed]
- Lefeber, N.; De Keersmaecker, E.; Henderix, S.; Michielsen, M.; Kerckhofs, E.; Swinnen, E. Physiological Responses and Perceived Exertion During Robot-Assisted and Body Weight-Supported Gait After Stroke. Neurorehabil. Neural Repair 2018, 32, 1043–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassmann, H. Hypoxia-like tissue injury as a component of multiple sclerosis lesions. J. Neurol. Sci. 2003, 206, 187–191. [Google Scholar] [CrossRef]
- Adkins, D.L.; Boychuk, J.; Remple, M.S.; Kleim, J.A. Motor training induces experience-specific patterns of plasticity across motor cortex and spinal cord. J. Appl. Physiol. 2006, 101, 1776–1782. [Google Scholar] [CrossRef] [Green Version]
- Sandroff, B.M.; Jones, C.D.; Baird, J.F.; Motl, R.W. Systematic Review on Exercise Training as a Neuroplasticity-Inducing Behavior in Multiple Sclerosis. Neurorehabil. Neural Repair 2020, 34, 575–588. [Google Scholar] [CrossRef] [PubMed]
- Ksiazek-Winiarek, D.J.; Szpakowski, P.; Glabinski, A. Neural Plasticity in Multiple Sclerosis: The Functional and Molecular Background. Neural Plast. 2015, 2015, 307175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tachtsidis, I.; Scholkmann, F. False positives and false negatives in functional near-infrared spectroscopy: Issues; challenges, and the way forward. Neurophotonics 2016, 3, 031405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RAGT (n = 12) | OW (n = 12) | p | |
|---|---|---|---|
| Age, years | 56 ± 10 | 57 ± 11 | 0.88 |
| Male sex, n (%) | 5 (42) | 8 (67) | 0.22 |
| MS duration, years | 12 ± 9 | 20 ± 13 | 0.12 |
| EDSS | 6.3 ± 0.3 | 6.3 ± 0.3 | 1 |
| Primary progressive, n (%) | 6 (50) | 4 (33) | 0.22 |
| Secondary progressive, n (%) | 6 (50) | 8 (67) | 0.22 |
| T25FW speed, m/s | 0.50 ± 0.20 | 0.65 ± 0.40 | 0.37 |
| 6MWT, m | 118 ± 55 | 171 ± 124 | 0.18 |
| BBS | 32 ± 13 | 36 ± 14 | 0.43 |
| PwMS (n = 24) | Healthy (n = 5) | p | |
|---|---|---|---|
| Tot-OxyAUC (a.u.) | 382,434 ± 174,813 | 41,971 ± 8549 | <0.001 |
| MAff-OxyAUC (a.u.) | 218,637 ± 162,874 | 26,428 ± 7488 | 0.015 |
| LAff-OxyAUC (a.u.) | 163,797 ± 104,461 | 15,543 ± 2075 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lamberti, N.; Manfredini, F.; Baroni, A.; Crepaldi, A.; Lavezzi, S.; Basaglia, N.; Straudi, S. Motor Cortical Activation Assessment in Progressive Multiple Sclerosis Patients Enrolled in Gait Rehabilitation: A Secondary Analysis of the RAGTIME Trial Assisted by Functional Near-Infrared Spectroscopy. Diagnostics 2021, 11, 1068. https://doi.org/10.3390/diagnostics11061068
Lamberti N, Manfredini F, Baroni A, Crepaldi A, Lavezzi S, Basaglia N, Straudi S. Motor Cortical Activation Assessment in Progressive Multiple Sclerosis Patients Enrolled in Gait Rehabilitation: A Secondary Analysis of the RAGTIME Trial Assisted by Functional Near-Infrared Spectroscopy. Diagnostics. 2021; 11(6):1068. https://doi.org/10.3390/diagnostics11061068
Chicago/Turabian StyleLamberti, Nicola, Fabio Manfredini, Andrea Baroni, Anna Crepaldi, Susanna Lavezzi, Nino Basaglia, and Sofia Straudi. 2021. "Motor Cortical Activation Assessment in Progressive Multiple Sclerosis Patients Enrolled in Gait Rehabilitation: A Secondary Analysis of the RAGTIME Trial Assisted by Functional Near-Infrared Spectroscopy" Diagnostics 11, no. 6: 1068. https://doi.org/10.3390/diagnostics11061068