
Choroidal Vascularity Map in Unilateral Central Serous Chorioretinopathy: A Comparison with Fellow and Healthy Eyes

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
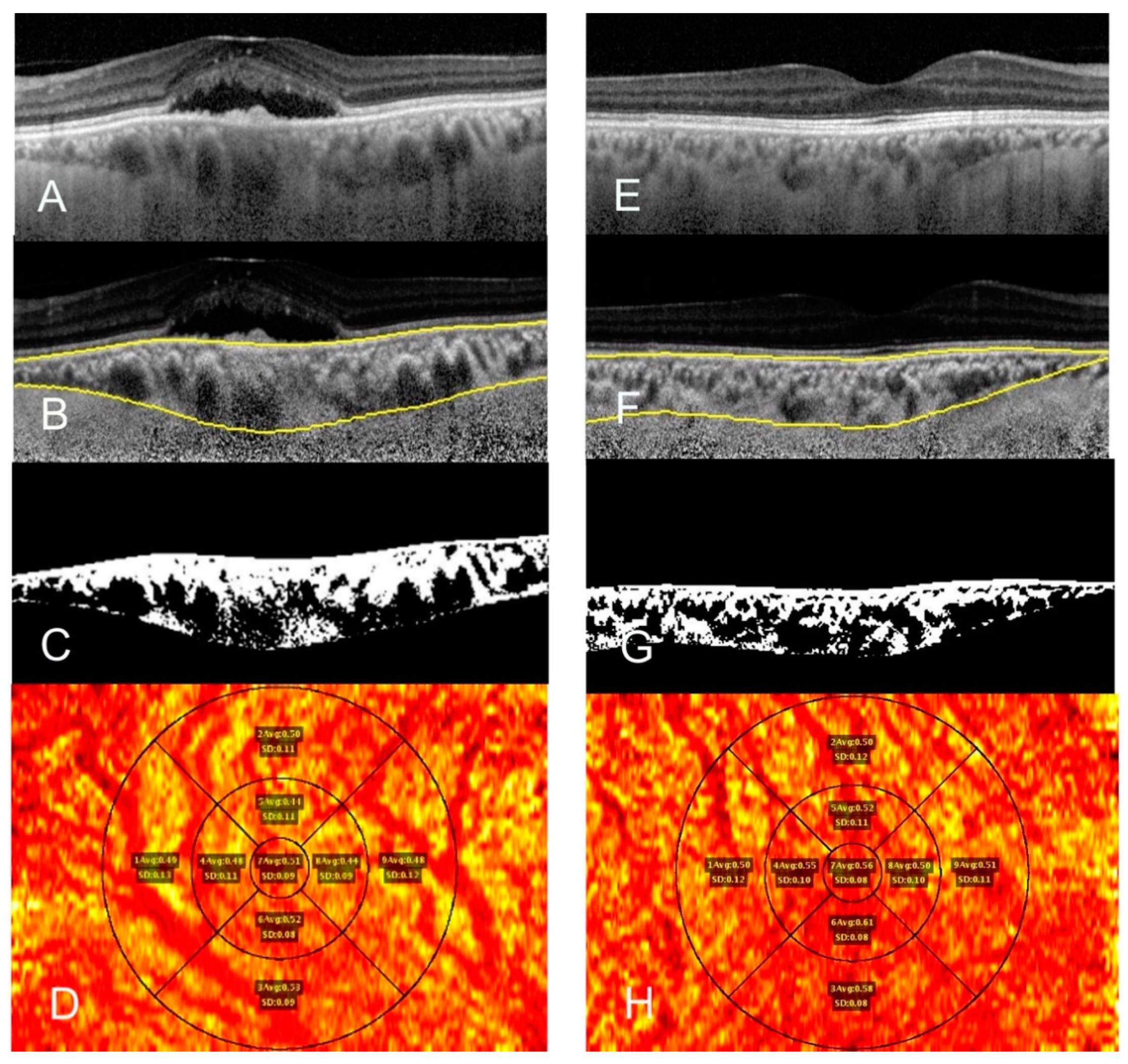
OCT Parameters
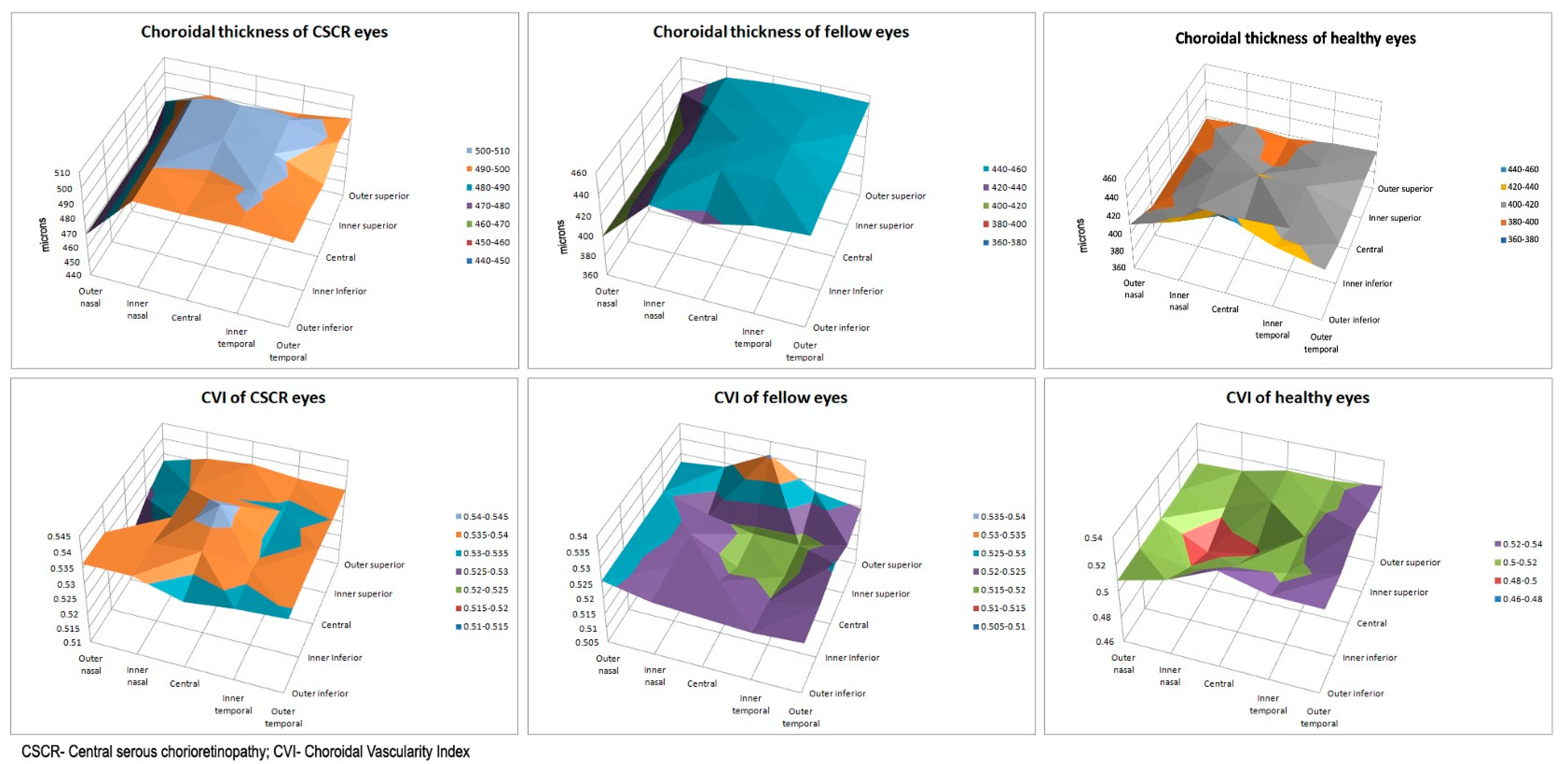
3. Results
3.1. Within Group Comparison
3.1.1. CSCR Eyes
3.1.2. Fellow Eyes
3.1.3. Healthy Controls
3.2. Between Group Comparison
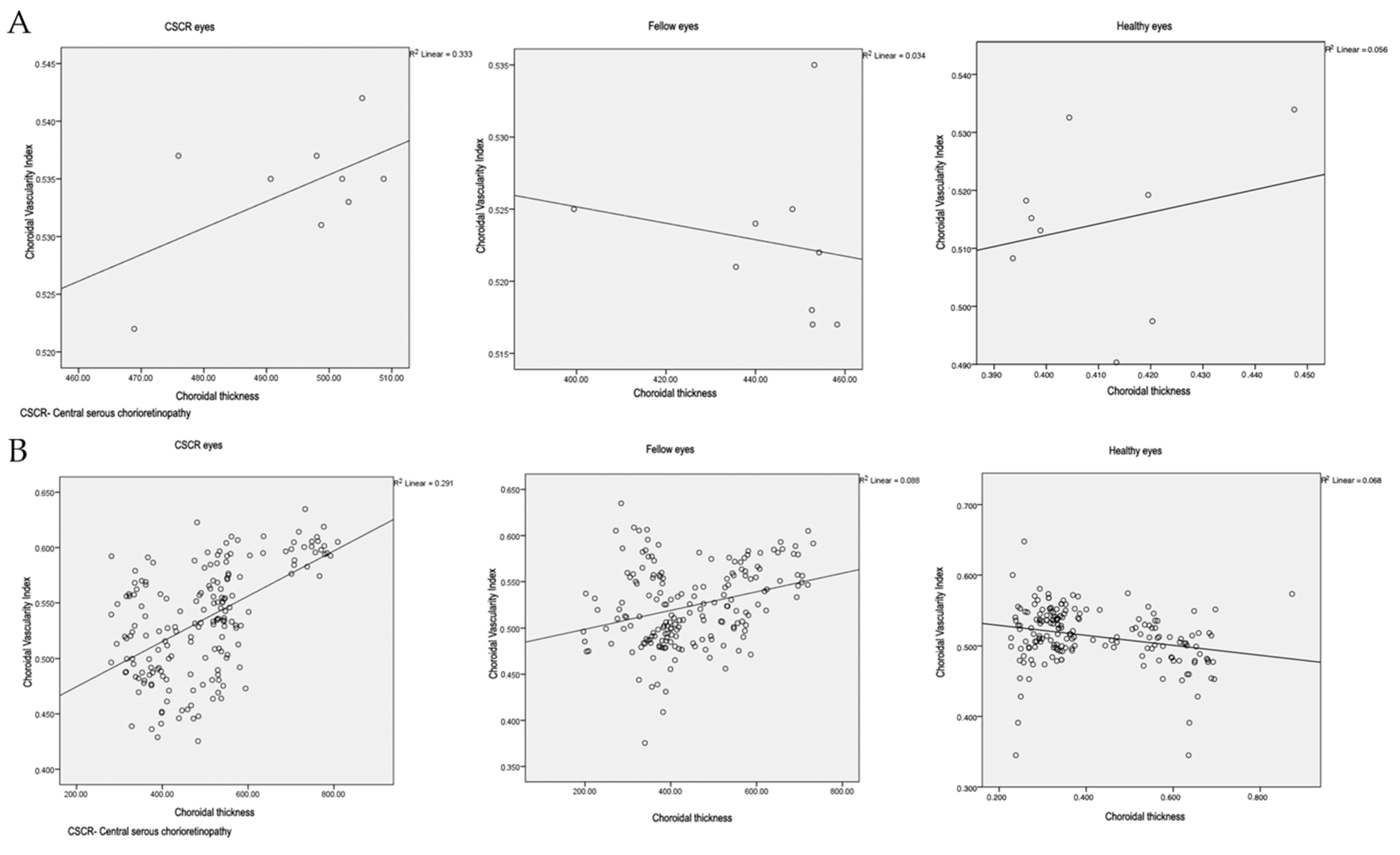
3.3. Co-Relation between CT and CVI
3.3.1. Comparison of Average of Regions
3.3.2. Comparison of Individual Values
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mrejen, S.; Spaide, R.F. Optical coherence tomography: Imaging of the choroid and beyond. Surv. Ophthalmol. 2013, 58, 387–429. [Google Scholar] [CrossRef] [PubMed]
- Daruich, A.; Matet, A.; Dirani, A.; Bousquet, E.; Zhao, M.; Farman, N.; Jaisser, F.; Behar-Cohen, F. Central serous chorioretinopathy: Recent findings and new physiopathology hypothesis. Prog. Retin. Eye Res. 2015, 48, 82–118. [Google Scholar] [CrossRef] [Green Version]
- Gajdzik-Gajdecka, U.; Dorecka, M.; Nita, E.; Michalska, A.; Miniewicz-Kurowska, J.; Romaniuk, W. Indocyanine green angiography in chronic central serous chorioretinopathy. Med. Sci. Monit. 2012, 18, CR51–CR57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costanzo, E.; Cohen, S.Y.; Miere, A.; Querques, G.; Capuano, V.; Semoun, O.; El Ameen, A.; Oubraham, H.; Souied, E.H. Optical Coherence Tomography Angiography in Central Serous Chorioretinopathy. J. Ophthalmol. 2015, 2015, 134783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, R.; Dogra, M.; Mulkutkar, S.; Katoch, D.; Singh, R.; Gupta, V.; Dogra, M.; Gupta, A. Optical coherence tomography angiography versus fluorescein angiography in diagnosing choroidal neovascularization in chronic central serous chorioretinopathy. Ind. J. Ophthalmol. 2019, 67, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Teussink, M.M.; Breukink, M.B.; van Grinsven, M.J.; Hoyng, C.B.; Klevering, B.J.; Boon, C.J.; de Jong, E.K.; Theelen, T. OCT angiography compared to fluorescein and indocyanine green angiography in chronic central serous chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2015, 56, 5229–5237. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Gupta, P.; Tan, K.A.; Cheung, C.M.; Wong, T.Y.; Cheng, C.Y. Choroidal vascularity index as a measure of vascular status of the choroid: Measurements in healthy eyes from a population-based study. Sci. Rep. 2016, 6, 21090. [Google Scholar] [CrossRef] [PubMed]
- Goud, A.; Singh, S.R.; Sahoo, N.K.; Rasheed, M.A.; Vupparaboina, K.K.; Ankireddy, S.; Lupidi, M.; Chhablani, J. New insights on choroidal vascularity: A comprehensive topographic approach. Investig. Ophthalmol. Vis. Sci. 2019, 60, 3563–3569. [Google Scholar] [CrossRef]
- Kim, Y.T.; Kang, S.W.; Bai, K.H. Choroidal thickness in both eyes of patients with unilaterally active central serous chorioretinopathy. Eye 2011, 25, 1635–1640. [Google Scholar] [CrossRef] [Green Version]
- Sahoo, N.K.; Maltsev, D.S.; Goud, A.; Kulikov, A.N.; Chhablani, J. Choroidal changes at the leakage site in acute central serous chorioretinopathy. Semin. Ophthalmol. 2019, 34, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Pyare, R.; Sridharan, P.; Arora, T.; Thakar, M.; Ghosh, B. Choroidal thickness evaluation of healthy eyes, central serous chorioretinopathy, and fellow eyes using spectral domain optical coherence tomography in Indian population. Ind. J. Ophthalmol. 2016, 64, 747. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.-R.; Kim, J.W.; Kim, S.W.; Lee, K. Choroidal thickness in patients with central serous chorioretinopathy: Assessment of Haller and Sattler layers. Retina 2016, 36, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, M.A.; Singh, S.R.; Invernizzi, A.; Cagini, C.; Goud, A.; Sahoo, N.K.; Cozzi, M.; Lupidi, M.; Chhablani, J. Wide-field choroidal thickness profile in healthy eyes. Sci. Rep. 2018, 8, 17166. [Google Scholar] [CrossRef] [PubMed]
- Woodman-Pieterse, E.C.; Read, S.A.; Collins, M.J.; Alonso-Caneiro, D. Regional changes in choroidal thickness associated with accommodation. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6414–6422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, C.A. Non-vascular smooth muscle cells in the human choroid: Distribution, development and further characterization. J. Anat. 2005, 207, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Nickla, D.L.; Wallman, J. The multifunctional choroid. Prog. Retin. Eye Res. 2010, 29, 144–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tewari, H.K.; Gadia, R.; Kumar, D.; Venkatesh, P.; Garg, S.P. Sympathetic–parasympathetic activity and reactivity in central serous chorioretinopathy: A case–control study. Investig. Ophthalmol. Vis. Sci. 2006, 47, 3474–3478. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Célérier, I.; Bousquet, E.; Jeanny, J.-C.; Jonet, L.; Savoldelli, M.; Offret, O.; Curan, A.; Farman, N.; Jaisser, F. Mineralocorticoid receptor is involved in rat and human ocular chorioretinopathy. J. Clin. Investig. 2012, 122, 2672–2679. [Google Scholar] [CrossRef] [PubMed]
- Maltsev, D.S.; Kulikov, A.N.; Chhablani, J. Topography-guided identification of leakage point in central serous chorioretinopathy: A base for fluorescein angiography-free focal laser photocoagulation. Br. J. Ophthalmol. 2018, 102, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Hoshino, J.; Mukai, R.; Nakamura, K.; Kikuchi, Y.; Kishi, S.; Akiyama, H. Vortex vein anastomosis at the watershed in pachychoroid spectrum diseases. Ophthalmol. Retina 2020, 4, 938–945. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| CSCR | Fellow | p-Value | Normal | |||
|---|---|---|---|---|---|---|
| CT (µm) | Region | Central | 505.27 ± 124.22 | 452.76 ± 127.52 | 0.02 | 420.32 ± 139.47 |
| Inner Superior | 508.7 ± 126.74 | 452.6 ± 124.82 | 0.03 | 397.15 ± 127.13 | ||
| Inner Temporal | 503.1 ± 133.16 | 458.25 ± 126.88 | 0.02 | 419.53 ± 147.31 | ||
| Inner Nasal | 502.08 ± 121.71 | 439.99 ± 120.51 | <0.01 | 413.42 ± 145.16 | ||
| Inner Inferior | 498 ± 132.73 | 454.21 ± 146.87 | 0.04 | 398.87 ± 145.09 | ||
| Outer Superior | 475.94 ± 139.48 | 453.15 ± 136.94 | 0.26 | 396.14 ± 138.61 | ||
| Outer Temporal | 490.66 ± 149.43 | 448.25 ± 129.12 | 0.01 | 404.40 ± 151.91 | ||
| Outer Nasal | 468.89 ± 124.58 | 399.44 ± 115.23 | <0.01 | 393.59 ± 158.89 | ||
| Outer Inferior | 498.74 ± 132.62 | 435.64 ± 124.23 | <0.01 | 447.50 ± 181.11 | ||
| Ring | Inner ring | 502.97 ± 126.36 | 451.26 ± 121.97 | <0.01 | 407.24 ± 135.23 | |
| Outer ring | 483.56 ± 132.51 | 434.12 ± 119.79 | <0.01 | 410.41 ± 144.37 | ||
| Quadrant | Superior | 492.32 ± 130.9 | 452.87 ± 122.76 | 0.05 | 396.64 ± 128.45 | |
| Temporal | 496.88 ± 140.71 | 453.25 ± 126.63 | 0.01 | 411.96 ± 148.86 | ||
| Nasal | 485.49 ± 122.1 | 419.71 ± 115.87 | <0.01 | 403.51 ± 151.42 | ||
| Inferior | 498.37 ± 129.77 | 444.93 ± 123.99 | <0.01 | 423.19 ± 147.97 | ||
| Overall average | 494.6 ± 128.14 | 443.81 ± 120.26 | 0.03 | 410.10 ± 148.29 | ||
| CVI | Region | Central | 0.542 ± 0.05 | 0.517 ± 0.046 | 0.06 | 0.497 ± 0.019 |
| Inner Superior | 0.535 ± 0.051 | 0.518 ± 0.046 | 0.18 | 0.515 ± 0.028 | ||
| Inner Temporal | 0.533 ± 0.052 | 0.517 ± 0.042 | 0.20 | 0.516 ± 0.031 | ||
| Inner Nasal | 0.535 ± 0.056 | 0.524 ± 0.042 | 0.41 | 0.490 ± 0.029 | ||
| Inner Inferior | 0.537 ± 0.051 | 0.522 ± 0.05 | 0.24 | 0.513 ± 0.047 | ||
| Outer Superior | 0.537 ± 0.046 | 0.535 ± 0.033 | 0.79 | 0.518 ± 0.047 | ||
| Outer Temporal | 0.535 ± 0.051 | 0.525 ± 0.041 | 0.33 | 0.533 ± 0.023 | ||
| Outer Nasal | 0.522 ± 0.045 | 0.525 ± 0.046 | 0.79 | 0.508 ± 0.042 | ||
| Outer Inferior | 0.531 ± 0.041 | 0.521 ± 0.04 | 0.19 | 0.530 ± 0.032 | ||
| Ring | Inner ring | 0.535 ± 0.045 | 0.52 ± 0.032 | 0.11 | 0.509 ± 0.028 | |
| Outer ring | 0.531 ± 0.038 | 0.527 ± 0.032 | 0.48 | 0.523 ± 0.037 | ||
| Quadrant | Superior | 0.536 ± 0.043 | 0.527 ± 0.034 | 0.27 | 0.517 ± 0.042 | |
| Temporal | 0.534 ± 0.05 | 0.521 ± 0.04 | 0.23 | 0.526 ± 0.025 | ||
| Nasal | 0.529 ± 0.047 | 0.525 ± 0.04 | 0.67 | 0.499 ± 0.032 | ||
| Inferior | 0.534 ± 0.043 | 0.522 ± 0.037 | 0.14 | 0.522 ± 0.036 | ||
| Overall average | 0.534 ± 0.041 | 0.523 ± 0.031 | 0.78 | 0.514 ± 0.035 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sahoo, N.K.; Singh, S.R.; Beale, O.; Nkrumah, G.; Rasheed, M.A.; Jabeen, A.; Vupparaboina, K.K.; Ibrahim, M.N.; Tatti, F.; Chandra, K.; et al. Choroidal Vascularity Map in Unilateral Central Serous Chorioretinopathy: A Comparison with Fellow and Healthy Eyes. Diagnostics 2021, 11, 861. https://doi.org/10.3390/diagnostics11050861
Sahoo NK, Singh SR, Beale O, Nkrumah G, Rasheed MA, Jabeen A, Vupparaboina KK, Ibrahim MN, Tatti F, Chandra K, et al. Choroidal Vascularity Map in Unilateral Central Serous Chorioretinopathy: A Comparison with Fellow and Healthy Eyes. Diagnostics. 2021; 11(5):861. https://doi.org/10.3390/diagnostics11050861
Chicago/Turabian StyleSahoo, Niroj Kumar, Sumit Randhir Singh, Oliver Beale, Gideon Nkrumah, Mohammed Abdul Rasheed, Asiya Jabeen, Kiran Kumar Vupparaboina, Mohammed Nasar Ibrahim, Filippo Tatti, Khushboo Chandra, and et al. 2021. "Choroidal Vascularity Map in Unilateral Central Serous Chorioretinopathy: A Comparison with Fellow and Healthy Eyes" Diagnostics 11, no. 5: 861. https://doi.org/10.3390/diagnostics11050861