
Chronic Kidney Disease Is Associated with High Mortality Risk in Patients with Diabetes after Primary Shoulder Arthroplasty: A Nationwide Population-Based Cohort Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Covariates
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. In-Hospital Outcomes
3.3. Late Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwartz, B.E.; Savin, D.D.; Youderian, A.R.; Mossad, D.; Goldberg, B.A. National trends and perioperative outcomes in primary and revision total shoulder arthroplasty: Trends in total shoulder arthroplasty. Int. Orthop. 2015, 39, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Godeneche, A.; Boulahia, A.; Noel, E.; Boileau, P.; Walch, G. Total shoulder arthroplasty in chronic inflammatory and degenerative disease. Rev. Rhum. Engl. Ed. 1999, 66, 560–570. [Google Scholar] [PubMed]
- Schoch, B.S.; Barlow, J.D.; Schleck, C.; Cofield, R.H.; Sperling, J.W. Shoulder arthroplasty for atraumatic osteonecrosis of the humeral head. J. Shoulder Elb. Surg. 2016, 25, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Churchill, J.L.; Garrigues, G.E. Current Controversies in Reverse Total Shoulder Arthroplasty. JBJS Rev. 2016, 4, e4. [Google Scholar] [CrossRef] [PubMed]
- Dezfuli, B.; King, J.J.; Farmer, K.W.; Struk, A.M.; Wright, T.W. Outcomes of reverse total shoulder arthroplasty as primary versus revision procedure for proximal humerus fractures. J. Shoulder Elb. Surg. 2016, 25, 1133–1137. [Google Scholar] [CrossRef] [PubMed]
- Sebastia-Forcada, E.; Lizaur-Utrilla, A.; Cebrian-Gomez, R.; Miralles-Munoz, F.A.; Lopez-Prats, F.A. Outcomes of Reverse Total Shoulder Arthroplasty for Proximal Humeral Fractures: Primary Arthroplasty Versus Secondary Arthroplasty After Failed Proximal Humeral Locking Plate Fixation. J. Orthop. Trauma 2017, 31, e236–e240. [Google Scholar] [CrossRef] [PubMed]
- Bohsali, K.I.; Bois, A.J.; Wirth, M.A. Complications of Shoulder Arthroplasty. J. Bone Joint Surg. Am. 2017, 99, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Cancienne, J.M.; Kew, M.E.; Deasey, M.J.; Brockmeier, S.F.; Werner, B.C. Dialysis dependence and modality impact complication rates after shoulder arthroplasty. J. Shoulder Elb. Surg. 2019, 28, e71–e77. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.J.; Toor, A.S.; Shi, L.L.; Koh, J.L. Analysis of perioperative complications in patients after total shoulder arthroplasty and reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Lung, B.E.; Bisogno, M.; Kanjiya, S.; Komatsu, D.E.; Wang, E.D. Early postoperative complications and discharge time in diabetic patients undergoing total shoulder arthroplasty. J. Orthop. Surg. Res. 2019, 14, 9. [Google Scholar] [CrossRef]
- Menendez, M.E.; Baker, D.K.; Fryberger, C.T.; Ponce, B.A. Predictors of extended length of stay after elective shoulder arthroplasty. J. Shoulder Elb. Surg. 2015, 24, 1527–1533. [Google Scholar] [CrossRef] [PubMed]
- Ponce, B.A.; Menendez, M.E.; Oladeji, L.O.; Soldado, F. Diabetes as a risk factor for poorer early postoperative outcomes after shoulder arthroplasty. J. Shoulder Elb. Surg. 2014, 23, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Anastasio, A.T.; Farley, K.X.; Boden, S.; Wagner, E.R.; Gottschalk, M.B. Complications and Mortality in Patients with Chronic Kidney Disease Undergoing Total Shoulder Arthroplasty. Semin. Arthroplast. JSES 2020, 30, 96–103. [Google Scholar] [CrossRef]
- Villar, E.; Chang, S.H.; McDonald, S.P. Incidences, treatments, outcomes, and sex effect on survival in patients with end-stage renal disease by diabetes status in Australia and New Zealand (1991–2005). Diabetes Care 2007, 30, 3070–3076. [Google Scholar] [CrossRef] [Green Version]
- Collins, A.J.; Foley, R.N.; Gilbertson, D.T.; Chen, S.C. United States Renal Data System public health surveillance of chronic kidney disease and end-stage renal disease. Kidney Int. Suppl. 2015, 5, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Hsing, A.W.; Ioannidis, J.P. Nationwide Population Science: Lessons from the Taiwan National Health Insurance Research Database. JAMA Intern. Med. 2015, 175, 1527–1529. [Google Scholar] [CrossRef]
- Lin, L.Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.C. Data resource profile: The National Health Insurance Research Database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Kao Yang, Y.H.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.C.; Lai, M.S.; Syu, C.Y.; Chang, S.C.; Tseng, F.Y. Accuracy of diabetes diagnosis in health insurance claims data in Taiwan. J. Formos. Med. Assoc. 2005, 104, 157–163. [Google Scholar]
- Wu, C.S.; Lai, M.S.; Gau, S.S.; Wang, S.C.; Tsai, H.J. Concordance between patient self-reports and claims data on clinical diagnoses, medication use, and health system utilization in Taiwan. PLoS ONE 2014, 9, e112257. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.-H.; Lee, Y.-C.; Tsai, C.-T.; Chang, S.-N.; Chung, Y.-H.; Lin, M.-S.; Lin, J.-W.; Lai, M.-S. Continuation of statin therapy and a decreased risk of atrial fibrillation/flutter in patients with and without chronic kidney disease. Atherosclerosis 2014, 232, 224–230. [Google Scholar] [CrossRef]
- Lin, S.J.; Chen, T.H.; Kuo, L.T.; Yu, P.A.; Chen, C.L.; Hsu, W.H. Effects of Chronic Kidney Disease on Hemiarthroplasty Outcomes for Fragility Hip Fracture in Diabetic Patients: A Nationwide Population-Based Observational Study. J. Arthroplast. 2020, 35, 477–484. [Google Scholar] [CrossRef]
- Winkelmayer, W.C.; Schneeweiss, S.; Mogun, H.; Patrick, A.R.; Avorn, J.; Solomon, D.H. Identification of individuals with CKD from Medicare claims data: A validation study. Am. J. Kidney Dis. 2005, 46, 225–232. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Wu, C.Y.; Chen, Y.J.; Ho, H.J.; Hsu, Y.C.; Kuo, K.N.; Wu, M.S.; Lin, J.T. Association between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1914. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Loberiza, F.R.; Klein, J.P.; Zhang, M.J. A SAS macro for estimation of direct adjusted survival curves based on a stratified Cox regression model. Comput. Methods Prog. Biomed. 2007, 88, 95–101. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, M.J. SAS macros for estimation of direct adjusted cumulative incidence curves under proportional subdistribution hazards models. Comput. Methods Prog. Biomed. 2011, 101, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Deegan, B.F.; Richard, R.D.; Bowen, T.R.; Perkins, R.M.; Graham, J.H.; Foltzer, M.A. Impact of Chronic Kidney Disease Stage on Lower-extremity Arthroplasty. Orthopedics 2014, 37, e613–e618. [Google Scholar] [CrossRef]
- Warth, L.C.; Pugely, A.J.; Martin, C.T.; Gao, Y.; Callaghan, J.J. Total Joint Arthroplasty in Patients with Chronic Renal Disease: Is It Worth the Risk? J. Arthroplast. 2015, 30, 51–54. [Google Scholar] [CrossRef]
- Himmelfarb, J. Hemodialysis complications. Am. J. Kidney Dis. 2005, 45, 1122–1131. [Google Scholar] [CrossRef]
- Suh, Y.S.; Won, S.H.; Choi, H.S.; Lee, J.C.; Chun, D.I.; Nho, J.H.; Lee, H.W.; Kim, J.H. Survivorship and Complications after Hip Fracture Surgery in Patients with Chronic Kidney Disease. J. Korean Med. Sci. 2017, 32, 2035–2041. [Google Scholar] [CrossRef] [Green Version]
- Singh, J.A.; Sperling, J.W.; Schleck, C.; Harmsen, W.S.; Cofield, R.H. Periprosthetic infections after total shoulder arthroplasty: A 33-year perspective. J. Shoulder Elb. Surg. 2012, 21, 1534–1541. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.; Inacio, M.C.; Beckett, M.; Navarro, R.A.; Singh, A.; Dillon, M.T.; Sodl, J.F.; Yian, E.H. Patient and procedure-specific risk factors for deep infection after primary shoulder arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 2809–2815. [Google Scholar] [CrossRef] [Green Version]
- Daratha, K.B.; Short, R.A.; Corbett, C.F.; Ring, M.E.; Alicic, R.; Choka, R.; Tuttle, K.R. Risks of subsequent hospitalization and death in patients with kidney disease. Clin. J. Am. Soc. Nephrol. 2012, 7, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Kose, E.; An, T.; Kikkawa, A.; Matsumoto, Y.; Hayashi, H. Analysis of factors affecting rehospitalization of patients with chronic kidney disease after educational hospitalization. Clin. Pharmacol. 2014, 6, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Kuo, L.T.; Lin, S.J.; Chen, C.L.; Yu, P.A.; Hsu, W.H.; Chen, T.H. Chronic kidney disease is associated with a risk of higher mortality following total knee arthroplasty in diabetic patients: A nationwide population-based study. Oncotarget 2017, 8, 100288–100295. [Google Scholar] [CrossRef] [Green Version]
- Jamsa, P.; Jamsen, E.; Huhtala, H.; Eskelinen, A.; Oksala, N. Moderate to Severe Renal Insufficiency Is Associated with High Mortality After Hip and Knee Replacement. Clin. Orthop. Relat. Res. 2018, 476, 1284–1292. [Google Scholar] [CrossRef]
- Nagoya, S.; Nagao, M.; Takada, J.; Kuwabara, H.; Kaya, M.; Yamashita, T. Efficacy of Cementless Total Hip Arthroplasty in Patients on Long-Term Hemodialysis. J. Arthroplast. 2005, 20, 66–71. [Google Scholar] [CrossRef]
- Ponnusamy, K.E.; Jain, A.; Thakkar, S.C.; Sterling, R.S.; Skolasky, R.L.; Khanuja, H.S. Inpatient Mortality and Morbidity for Dialysis-Dependent Patients Undergoing Primary Total Hip or Knee Arthroplasty. J. Bone Joint Surg. Am. 2015, 97, 1326–1332. [Google Scholar] [CrossRef]
- Shadman, R.; Allison, M.A.; Criqui, M.H. Glomerular Filtration Rate and N-terminal Pro-Brain Natriuretic Peptide as Predictors of Cardiovascular Mortality in Vascular Patients. J. Am. Coll. Cardiol. 2007, 49, 2172–2181. [Google Scholar] [CrossRef] [Green Version]
- Ryan, T.P.; Fisher, S.G.; Elder, J.L.; Winters, P.C.; Beckett, W.; Tacci, J.; Sloand, J.A. Increased cardiovascular risk associated with reduced kidney function. Am. J. Nephrol. 2009, 29, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soleymanian, T.; Kokabeh, Z.; Ramaghi, R.; Mahjoub, A.; Argani, H. Clinical outcomes and quality of life in hemodialysis diabetic patients versus non-diabetics. J. Nephropathol. 2017, 6, 81–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Non-CKD (n = 3042) | Non-Dialysis CKD (n = 1174) | Dialysis (n = 227) | p-Value |
|---|---|---|---|---|
| Age (years) | 69.6 ± 11.9 | 71.8 ± 10.6 a | 65.4 ± 10.3 a,b | <0.001 |
| Age group | ||||
| <60 yrs. | 682 (22.4) | 173 (14.7) a | 83 (36.6) a,b | <0.001 |
| 60–80 yrs. | 1766 (58.1) | 745 (63.5) a | 125 (55.1) | |
| >80 yrs. | 594 (19.5) | 256 (21.8) | 19 (8.4) b | |
| Female sex | 2112 (69.4) | 831 (70.8) | 144 (63.4) | 0.088 |
| Hospital level | ||||
| Medical center | 1134 (37.3) | 411 (35.0) | 91 (40.1) | 0.041 |
| Region hospital | 1268 (41.7) | 537 (45.7) | 102 (44.9) | |
| District hospital or clinics | 640 (21.0) | 226 (19.3) | 34 (15.0) | |
| Hospital volume (surgeries) | 0.013 | |||
| Q1 (1–130) | 764 (25.1) | 287 (24.4) | 46 (20.3) | |
| Q2 (132–262) | 772 (25.4) | 278 (23.7) | 58 (25.6) | |
| Q3 (281–544) | 762 (25.0) | 313 (26.7) | 81 (35.7) b | |
| Q4 (598–1427) | 744 (24.5) | 296 (25.2) | 42 (18.5) | |
| Monthly income, USD | 0.130 | |||
| ≤$596 | 1095 (36.0) | 414 (35.3) | 70 (30.8) | |
| $597–$760 | 1236 (40.6) | 510 (43.4) | 94 (41.4) | |
| >$760 | 711 (23.4) | 250 (21.3) | 63 (27.8) | |
| Urbanization level | 0.401 | |||
| Low | 437 (14.4) | 192 (16.4) | 33 (14.5) | |
| Moderate | 1002 (32.9) | 366 (31.2) | 77 (33.9) | |
| High | 917 (30.1) | 333 (28.4) | 60 (26.4) | |
| Very high | 686 (22.6) | 283 (24.1) | 57 (25.1) | |
| Duration of surgery | 0.133 | |||
| ≤4 h | 880 (28.9) | 362 (30.8) | 77 (33.9) | |
| >4 h | 2162 (71.1) | 812 (69.2) | 150 (66.1) | |
| Comorbidity | ||||
| Stroke | 463 (15.2) | 253 (21.6) a | 56 (24.7) a | <0.001 |
| COPD | 264 (8.7) | 158 (13.5) a | 18 (7.9) | <0.001 |
| Heart failure | 534 (17.6) | 323 (27.5) a | 85 (37.4) a,b | <0.001 |
| Coronary heart disease | 556 (18.3) | 380 (32.4) a | 76 (33.5) a | <0.001 |
| Hyperlipidemia | 706 (23.2) | 353 (30.1) a | 46 (20.3) b | <0.001 |
| Cardiac dysrhythmia | 212 (7.0) | 113 (9.6) a | 22 (9.7) | 0.009 |
| Myocardial infarction | 175 (5.8) | 117 (10.0) a | 30 (13.2) a | <0.001 |
| Hypertension | 2026 (66.6) | 933 (79.5) a | 187 (82.4) a | <0.001 |
| Dementia | 221 (7.3) | 113 (9.6) a | 11 (4.8) | 0.009 |
| Osteoporosis | 1426 (46.9) | 577 (49.1) | 142 (62.6) b | <0.001 |
| CCI score | 2.0 ± 2.0 | 3.0 ± 2.0 a | 5.0 ± 2.0 a,b | <0.001 |
| Follow up duration (years) | 5.5 ± 3.9 | 3.8 ± 3.0 a | 2.7 ± 2.3 a,b | <0.001 |
| Number of Events (%) | Adjusted OR or β ‡ | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | Non-CKD (n = 3042) | Non-Dialysis CKD (n = 1174) | Dialysis (n = 227) | Non-Dialysis CKD vs. Non-CKD | Dialysis vs. Non-CKD | Dialysis vs. Non-Dialysis CKD | |||
| OR or β (95% CI) | p-Value | OR or β (95% CI) | p-Value | OR or β (95% CI) | p-Value | ||||
| Categorical | |||||||||
| Newly-onset VTE | 7 (0.23) | 4 (0.34) | 0 (0) | 1.68 (0.46–6.20) | 0.436 | NA | NA | NA | NA |
| Delirium | 5 (0.16) | 4 (0.34) | 0 (0) | 1.76 (0.40–7.78) | 0.455 | NA | NA | NA | NA |
| Debridement | 44 (1.45) | 16 (1.36) | 0 (0) | 1.02 (0.56–1.86) | 0.949 | NA | NA | NA | NA |
| Infection | 76 (2.5) | 23 (2.0) | 2 (0.88) | 0.87 (0.53–1.42) | 0.573 | 0.39 (0.09–1.63) | 0.196 | 0.45 (0.10–1.96) | 0.284 |
| UTI | 106 (3.5) | 56 (4.8) | 5 (2.2) | 1.16 (0.82–1.64) | 0.391 | 0.58 (0.23–1.49) | 0.258 | 0.50 (0.20–1.29) | 0.153 |
| Pneumonia | 50 (1.6) | 28 (2.4) | 2 (0.88) | 1.19 (0.73–1.94) | 0.492 | 0.66 (0.15–2.82) | 0.569 | 0.55 (0.13–2.40) | 0.428 |
| Transfusion | 1922 (63.2) | 897 (76.4) | 186 (81.9) | 1.87 (1.59–2.21) | <0.001 | 2.98 (2.07–4.30) | <0.001 | 1.59 (1.09–2.33) | 0.016 |
| ICU stay | 106 (3.5) | 83 (7.1) | 15 (6.6) | 1.68 (1.23–2.29) | 0.001 | 1.79 (0.98–3.26) | 0.058 | 1.07 (0.58–1.95) | 0.833 |
| In-hospital death | 9 (0.29) | 17 (1.4) | 3 (1.3) | 4.69 (2.02–10.89) | <0.001 | 6.71 (1.63–27.73) | 0.009 | 1.43 (0.38–5.35) | 0.595 |
| Continuous | |||||||||
| Hospital days | 10.0 ± 9.0 | 12.0 ± 11.0 | 12.0 ± 10.0 | 1.79 (1.13–2.45) | <0.001 | 2.29 (0.96–3.61) | 0.001 | 0.50 (−0.89–1.88) | 0.481 |
| Cost (USD × 103) | 3.6 ± 2.4 | 4.2 ± 4.0 | 4.5 ± 2.4 | 0.47 (0.27, 0.67) | <0.001 | 0.85 (0.45, 1.26) | <0.001 | 0.38 (−0.04, 0.80) | 0.077 |
| Number of Events (%) | Adjusted Hazard Ratio and 95% CI ‡ | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | Non-CKD (n = 3042) | Non-Dialysis CKD (n = 1174) | Dialysis (n = 227) | Non-Dialysis CKD vs. Non-CKD | Dialysis vs. Non-CKD | Dialysis vs. Non-Dialysis CKD | |||
| HR or SHR (95% CI) | p-Value | HR or SHR (95% CI) | p-Value | HR or SHR (95% CI) | p-Value | ||||
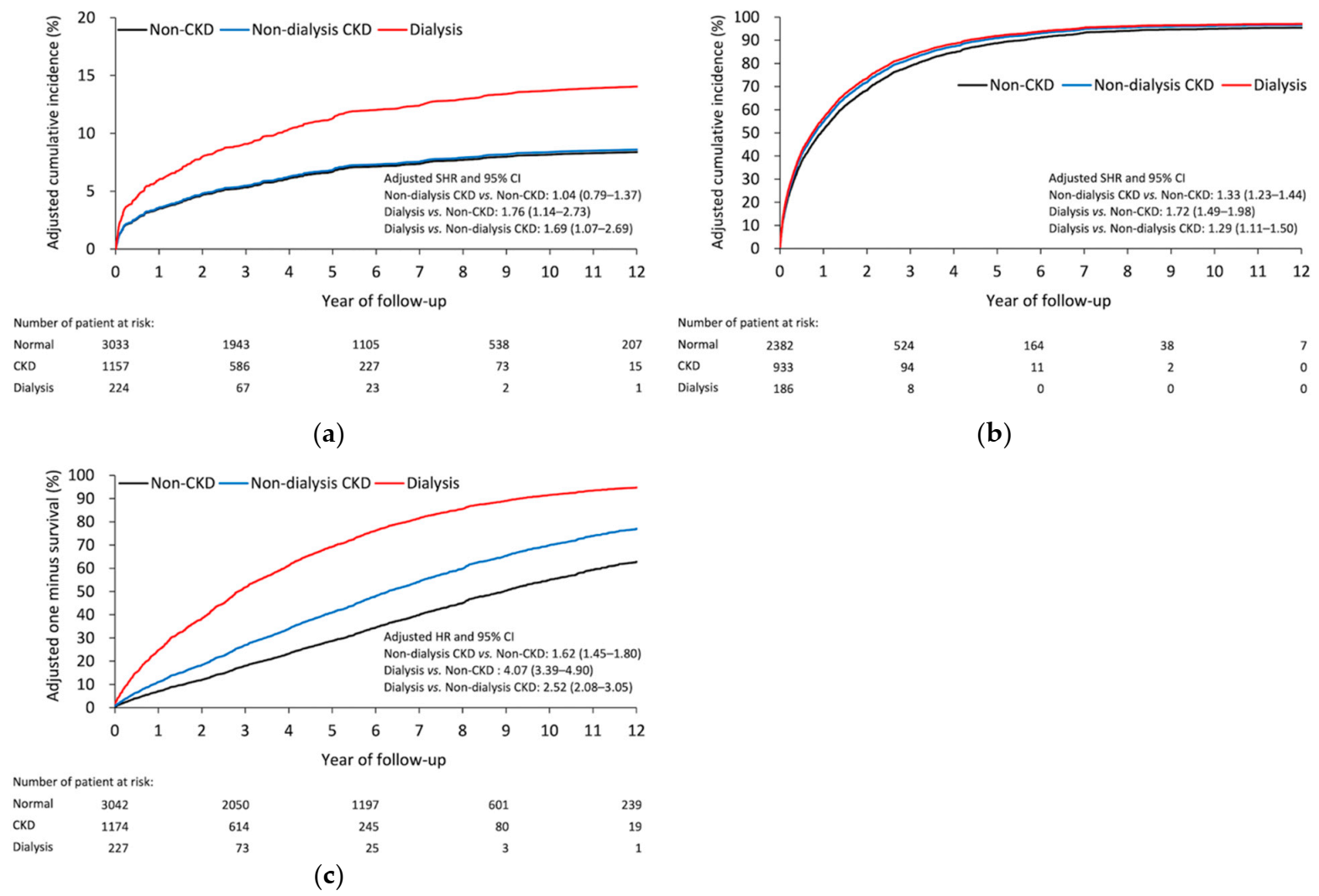
| Infection | |||||||||
| Superficial infection | 169 (5.6) | 61 (5.3) | 18 (8.0) | 1.14 (0.83–1.56) | 0.416 | 1.63 (0.97–2.75) | 0.067 | 1.43 (0.83–2.47) | 0.197 |
| Debridement | 59 (1.9) | 16 (1.4) | 6 (2.7) | 0.94 (0.52–1.70) | 0.842 | 1.43 (0.59–3.50) | 0.431 | 1.52 (0.58–4.02) | 0.398 |
| Implant removal | 72 (2.4) | 23 (2.0) | 6 (2.7) | 1.09 (0.67–1.75) | 0.738 | 1.34 (0.58–3.10) | 0.501 | 1.23 (0.51–2.96) | 0.642 |
| Any infection | 228 (7.5) | 75 (6.5) | 26 (11.6) | 1.04 (0.79–1.37) | 0.780 | 1.76 (1.14–2.73) | 0.011 | 1.69 (1.07–2.69) | 0.025 |
| All-cause readmission | |||||||||
| At 30 days | 293 (9.7) | 170 (14.7) | 30 (13.4) | 1.39 (1.15–1.70) | 0.001 | 1.28 (0.85–1.92) | 0.234 | 0.92 (0.61–1.38) | 0.679 |
| At 90 days | 565 (18.6) | 306 (26.4) | 76 (33.9) | 1.33 (1.15–1.54) | <0.001 | 1.62 (1.27–2.09) | <0.001 | 1.22 (0.95–1.58) | 0.125 |
| At 1 year | 1138 (37.5) | 609 (52.6) | 141 (62.9) | 1.42 (1.29–1.58) | <0.001 | 1.74 (1.46–2.08) | <0.001 | 1.22 (1.02–1.47) | 0.031 |
| At the end | 2382 (78.5) | 933 (80.6) | 186 (83.0) | 1.33 (1.23–1.44) | <0.001 | 1.72 (1.49–1.98) | <0.001 | 1.29 (1.11–1.50) | 0.001 |
| All-cause mortality | |||||||||
| At 30 days | 24 (0.79) | 33 (2.8) | 7 (3.1) | 3.33 (1.93–5.75) | <0.001 | 4.82 (1.95–11.89) | 0.001 | 1.45 (0.61–3.43) | 0.402 |
| At 90 days | 62 (2.0) | 58 (4.9) | 18 (7.9) | 2.22 (1.53–3.21) | <0.001 | 4.74 (2.69–8.36) | <0.001 | 2.14 (1.22–3.76) | 0.008 |
| At 1 year | 199 (6.5) | 148 (12.6) | 43 (18.9) | 1.83 (1.47–2.28) | <0.001 | 3.56 (2.50–5.06) | <0.001 | 1.95 (1.36–2.78) | 0.000 |
| At the end | 1191 (39.2) | 555 (47.3) | 143 (63.0) | 1.62 (1.45–1.80) | <0.001 | 4.07 (3.39–4.90) | <0.001 | 2.52 (2.08–3.05) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, M.-H.; Lin, S.-J.; Kuo, L.-T.; Chen, T.-H.; Chen, C.-L.; Yu, P.-A.; Tsai, Y.-H.; Hsu, W.-H. Chronic Kidney Disease Is Associated with High Mortality Risk in Patients with Diabetes after Primary Shoulder Arthroplasty: A Nationwide Population-Based Cohort Study. Diagnostics 2021, 11, 822. https://doi.org/10.3390/diagnostics11050822
Lin M-H, Lin S-J, Kuo L-T, Chen T-H, Chen C-L, Yu P-A, Tsai Y-H, Hsu W-H. Chronic Kidney Disease Is Associated with High Mortality Risk in Patients with Diabetes after Primary Shoulder Arthroplasty: A Nationwide Population-Based Cohort Study. Diagnostics. 2021; 11(5):822. https://doi.org/10.3390/diagnostics11050822
Chicago/Turabian StyleLin, Meng-Hao, Su-Ju Lin, Liang-Tseng Kuo, Tien-Hsing Chen, Chi-Lung Chen, Pei-An Yu, Yao-Hung Tsai, and Wei-Hsiu Hsu. 2021. "Chronic Kidney Disease Is Associated with High Mortality Risk in Patients with Diabetes after Primary Shoulder Arthroplasty: A Nationwide Population-Based Cohort Study" Diagnostics 11, no. 5: 822. https://doi.org/10.3390/diagnostics11050822