
Detection and Differentiation of SARS-CoV-2, Influenza, and Respiratory Syncytial Viruses by CRISPR


Abstract
:1. Introduction
2. Materials and Methods
2.1. Reference RNA Standards of Viruses
2.2. Oligonucleotides and RT-Recombinase Polymerase Amplification Reaction (RT-RPA)
2.3. Detection of the Viruses by Using CRISPR-Cas12a with a Fluorescence Plate Reader
2.4. Visual Detection of the Viruses by Using CRISPR-Cas12a with a UV Light Illuminator
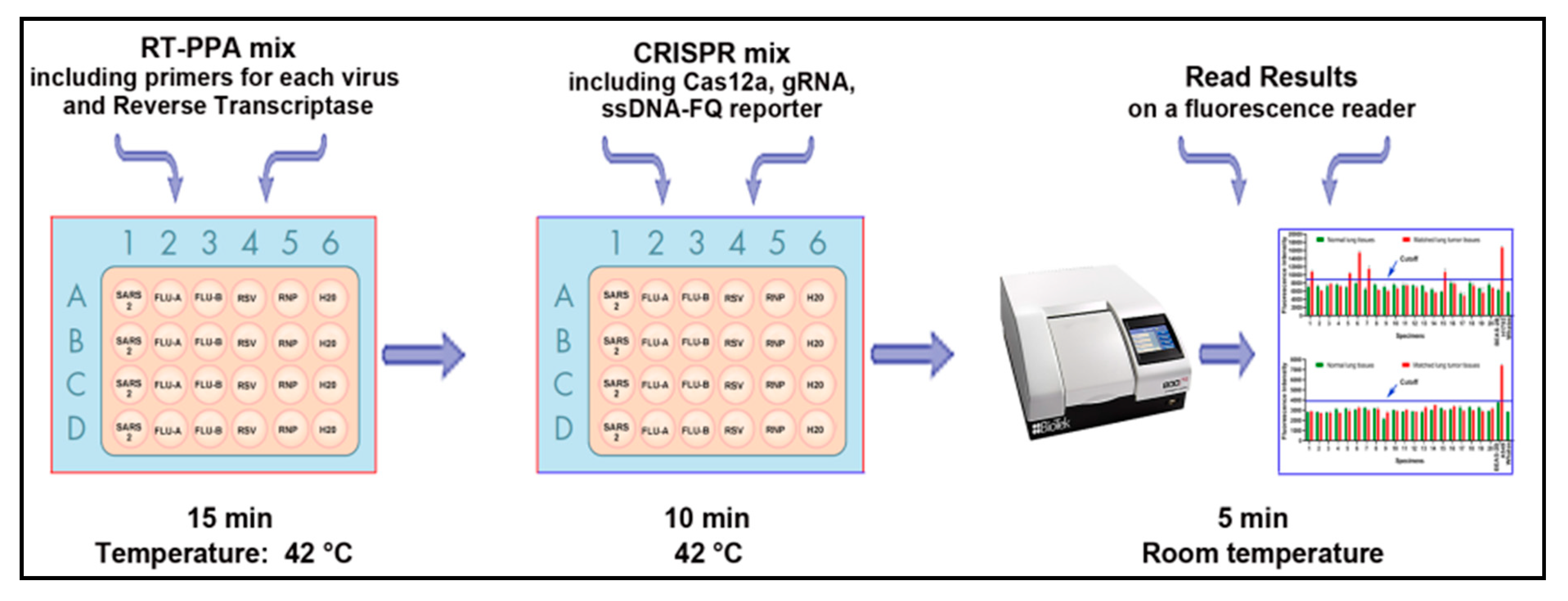
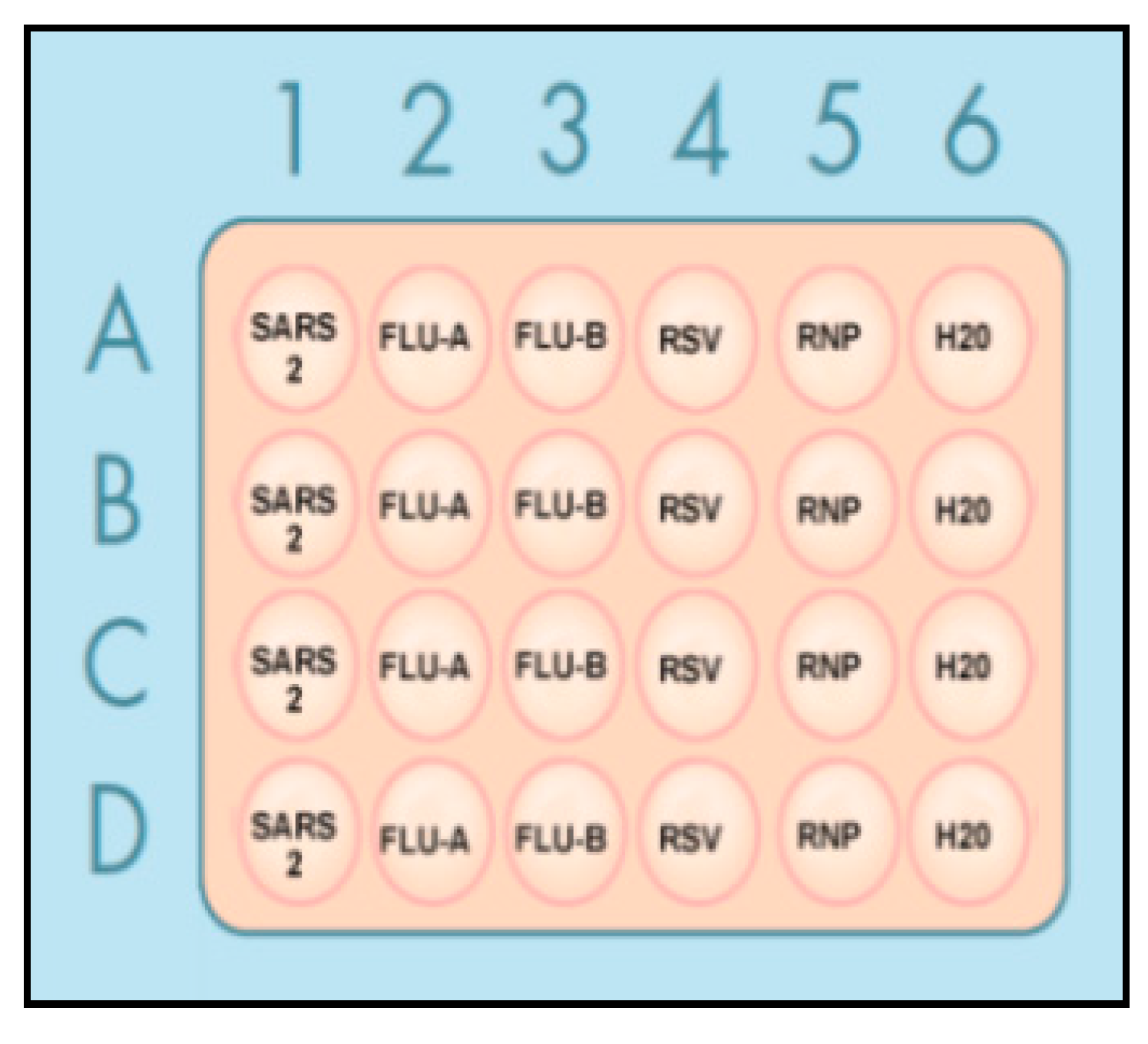
2.5. Simultaneous Detection of Multiple Viruses by CRISPR-Cas12a in a Single Plate
2.6. RT-PCR
2.7. Clinical Specimens and RNA Isolation
2.8. Statistical Analysis
3. Results
3.1. CRISPR-Cas12a Can Specifically Discriminate the Different Viruses
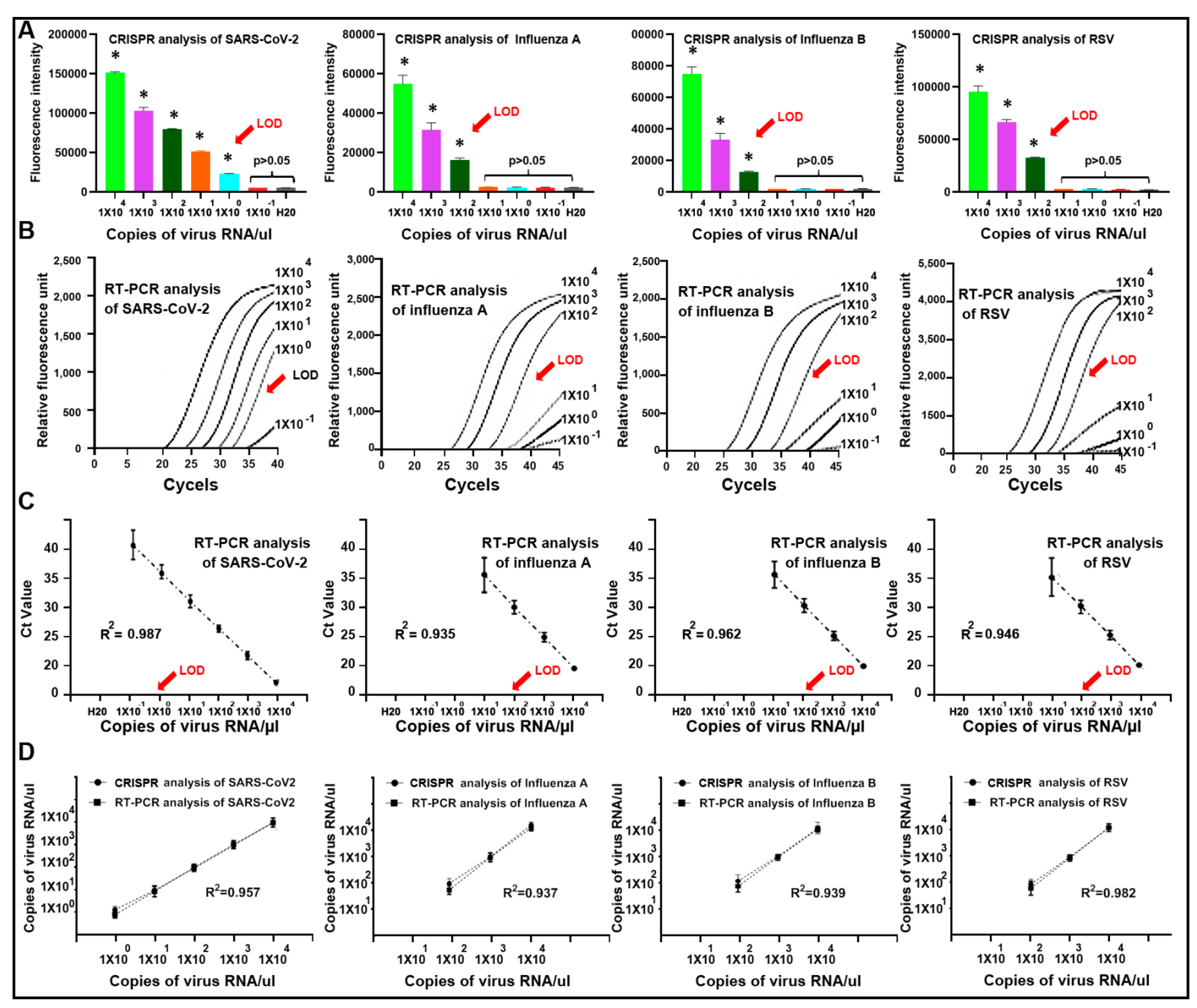
3.2. CRISPR-Cas12a Can Sensitively Detect SARS-CoV-2, Influenza A and B, and RSV
3.3. Diagnostic Performance of the Plate-Based CRISPR-Cas12a Assay for the Simultaneous Detection and Differentiation of SARS-CoV-2, Influenza, and RSV in Clinical Specimens
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Skegg, D.; Gluckman, P.; Boulton, G.; Hackmann, H.; Karim, S.S.A.; Piot, P.; Woopen, C. Future scenarios for the COVID-19 pandemic. Lancet 2021, 397, 777–778. [Google Scholar] [CrossRef]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Chiu, S.K.; Wang, Y.H.; Liao, S.J.; Li, S.Y.; et al. Novel dual multiplex real-time RT-PCR assays for the rapid detection of SARS-CoV-2, influenza A/B, and respiratory syncytial virus using the BD MAX open system. Emerg. Microbes Infect. 2021, 10, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Leung, E.C.; Chow, V.C.; Lee, M.K.; Tang, K.P.; Li, D.K.; Lai, R.W. Evaluation of the Xpert Xpress SARS-CoV-2/Flu/RSV assay for simultane-ous detection of SARS-CoV-2, Influenza A/B and Respiratory Syncytial Viruses in nasopharyngeal specimens. J. Clin. Microbiol. 2021, 59, e02965. [Google Scholar] [CrossRef]
- Udugama, B.; Kadhiresan, P.; Kozlowski, H.N.; Malekjahani, A.; Osborne, M.; Li, V.Y.C.; Chen, H.; Mubareka, S.; Gubbay, J.B.; Chan, W.C.W. Diagnosing COVID-19: The Disease and Tools for Detection. ACS Nano 2020, 14, 3822–3835. [Google Scholar] [CrossRef] [Green Version]
- Barrangou, R. The roles of CRISPR–Cas systems in adaptive immunity and beyond. Curr. Opin. Immunol. 2015, 32, 36–41. [Google Scholar] [CrossRef]
- Horvath, P.; Barrangou, R. CRISPR/Cas, the Immune System of Bacteria and Archaea. Science 2010, 327, 167–170. [Google Scholar] [CrossRef] [Green Version]
- Myhrvold, C.; Freije, C.A.; Gootenberg, J.S.; Abudayyeh, O.O.; Metsky, H.C.; Durbin, A.F.; Kellner, M.J.; Tan, A.L.; Paul, L.M.; Parham, L.A.; et al. Field-deployable viral diagnostics using CRISPR-Cas13. Science 2018, 360, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Gootenberg, J.S.; Abudayyeh, O.O.; Kellner, M.J.; Joung, J.; Collins, J.J.; Zhang, F. Multiplexed and portable nucleic acid detection platform with Cas13, Cas12a, and Csm6. Science 2018, 360, 439–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.S.; Ma, E.; Harrington, L.B.; Da Costa, M.; Tian, X.; Palefsky, J.M.; Doudna, J.A. CRISPR-Cas12a target binding unleashes indiscriminate single-stranded DNase activity. Science 2018, 360, 436–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abudayyeh, O.O.; Gootenberg, J.S.; Essletzbichler, P.; Han, S.; Joung, J.; Belanto, J.J.; Verdine, V.; Cox, D.B.T.; Kellner, M.J.; Regev, A.; et al. RNA targeting with CRISPR-Cas13. Nature 2017, 550, 280–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chertow, D.S. Next-generation diagnostics with CRISPR. Science 2018, 360, 381–382. [Google Scholar] [CrossRef]
- Tsou, J.-H.; Leng, Q.; Jiang, F. A CRISPR Test for Detection of Circulating Nuclei Acids. Transl. Oncol. 2019, 12, 1566–1573. [Google Scholar] [CrossRef]
- Tsou, J.-H.; Leng, Q.; Jiang, F. A CRISPR Test for Rapidly and Sensitively Detecting Circulating EGFR Mutations. Diagnostics 2020, 10, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Tsou, J.-H.; Leng, Q.; Jiang, F. Sensitive Detection of KRAS Mutations by Clustered Regularly Interspaced Short Palindromic Repeats. Diagnostics 2021, 11, 125. [Google Scholar] [CrossRef]
- Tsou, J.H.; Liu, H.; Stass, S.A.; Jiang, F. Rapid and Sensitive Detection of SARS-CoV-2 Using Clustered Regularly Interspaced Short Palindromic Repeats. Biomedicines 2021, 9, 239. [Google Scholar] [CrossRef]
- Kim, K. A bivariate cumulative probit regression model for ordered categorical data. Stat. Med. 1995, 14, 1341–1352. [Google Scholar] [CrossRef]
- Sanagi, M.M.; Ling, S.L.; Nasir, Z.; Hermawan, D.; Ibrahim, W.A.; Abu Naim, A. Comparison of signal-to-noise, blank determination, and linear regression methods for the estimation of detection and quantification limits for volatile organic compounds by gas chroma-tography. J. AOAC Int. 2009, 92, 1833–1838. [Google Scholar] [CrossRef] [Green Version]
- Hung, K.F.; Hung, C.H.; Hong, C.; Chen, S.C.; Sun, Y.C.; Wen, J.W.; Kuo, C.H.; Ko, C.H.; Cheng, C.M. Quantitative Spectrochip-Coupled Lateral Flow Immunoassay Demon-strates Clinical Potential for Overcoming Coronavirus Disease 2019 Pandemic Screening Challenges. Micromachines 2021, 12, 321. [Google Scholar] [CrossRef]
- Chen, L.; Eitenmiller, R. Single Laboratory Method Performance Evaluation for the Analysis of Total Food Folate by Trienzyme Extraction and Microplate Assay. J. Food Sci. 2007, 72, C243–C247. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, A.; Gupta, V.B. Methods for the determination of limit of detection and limit of quantitation of the analytical methods. Chronicles Young Sci. 2011, 2, 21. [Google Scholar] [CrossRef]
- Reed, G.F.; Lynn, F.; Meade, B.D. Use of Coefficient of Variation in Assessing Variability of Quantitative Assays. Clin. Vaccine Immunol. 2002, 9, 1235–1239. [Google Scholar] [CrossRef] [Green Version]
- Kevadiya, B.D.; Machhi, J.; Herskovitz, J.; Oleynikov, M.D.; Blomberg, W.R.; Bajwa, N.; Soni, D.; Das, S.; Hasan, M.; Patel, M.; et al. Diagnostics for SARS-CoV-2 infections. Nat. Mater. 2021, 20, 593–605. [Google Scholar] [CrossRef]
- Ni, M.; Xu, H.; Luo, J.; Liu, W.; Zhou, D. Simultaneous detection and differentiation of SARS-CoV-2, influenza A virus and in-fluenza B virus by one-step quadruplex real-time RT-PCR in patients with clinical manifestations. Int. J. Infect. Dis. 2021, 103, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.I.I.; Wong, A.H.; Lai, R.W.M. Comparison of the Cepheid Xpert Xpress Flu/RSV Assay to in-house Flu/RSV triplex real-time RT-PCR for rapid molecular detection of Influenza, A.; Influenza B and Respiratory Syncytial Virus in respiratory specimens. J. Med. Microbiol. 2018, 67, 1576–1580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Tanner, N.A. Development of multiplexed reverse-transcription loop-mediated isothermal amplifica-tion for detection of SARS-CoV-2 and influenza viral, R.N.A. Biotechniques 2021, 70, 167–174. [Google Scholar] [CrossRef]
- Ahn, S.J.; Baek, Y.H.; Lloren, K.K.S.; Choi, W.S.; Jeong, J.H.; Antigua, K.J.C.; Kwon, H.I.; Park, S.J.; Kim, E.H.; Kim, Y.I.; et al. Rapid and simple colorimetric detection of multiple influenza viruses in-fecting humans using a reverse transcriptional loop-mediated isothermal amplification (RT-LAMP) diagnostic platform. BMC Infect. Dis. 2019, 19, 676. [Google Scholar] [CrossRef] [Green Version]
- Broughton, J.P.; Deng, X.; Yu, G.; Fasching, C.L.; Servellita, V.; Singh, J.; Miao, X.; Streithorst, J.A.; Granados, A.; Sotomayor-Gonzalez, A.; et al. CRISPR-Cas12-based detection of SARS-CoV-2. Nat. Biotechnol. 2020, 38, 870–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.; Yin, K.; Li, Z.; Lalla, R.V.; Ballesteros, E.; Sfeir, M.M.; Liu, C. Ultrasensitive and visual detection of SARS-CoV-2 using all-in-one dual CRISPR-Cas12a assay. Nat. Commun. 2020, 11, 4711. [Google Scholar] [CrossRef]
- Joung, J.; Ladha, A.; Saito, M.; Kim, N.G.; Woolley, A.E.; Segel, M.; Barretto, R.P.J.; Ranu, A.; Macrae, R.K.; Faure, G.; et al. Detection of SARS-CoV-2 with SHERLOCK One-Pot Testing. N. Engl. J. Med. 2020, 383, 1492–1494. [Google Scholar] [CrossRef]
- Mayuramart, O.; Nimsamer, P.; Rattanaburi, S.; Chantaravisoot, N.; Khongnomnan, K.; Chansaenroj, J.; Puenpa, J.; Suntronwong, N.; Vichaiwattana, P.; Poovorawan, Y.; et al. Detection of severe acute respiratory syndrome coronavirus 2 and influenza viruses based on CRISPR-Cas12a. Exp. Biol. Med. 2021, 246, 400–405. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B.; et al. Tracking Changes in SARS-CoV-2 Spike: Evidence that D614G In-creases Infectivity of the COVID-19 Virus. Cell 2020, 182, 812–827.e819. [Google Scholar] [CrossRef] [PubMed]
- Weissman, D.; Alameh, M.-G.; De Silva, T.; Collini, P.; Hornsby, H.; Brown, R.; Labranche, C.C.; Edwards, R.J.; Sutherland, L.; Santra, S.; et al. D614G Spike Mutation Increases SARS CoV-2 Susceptibility to Neutralization. Cell Host Microbe 2021, 29, 23–31.e4. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primers for RT-RPA | |
|---|---|
| SARS-CoV2 N-F | TGATTACAAACATTGGCCGCAAATTGCACA |
| SARS-CoV2 N-R | AGGTCAACCACGTTCCCGAAGGTGTGACTT |
| Influenza A-F | CTCACTTTTCTAGCACGGT |
| Influenza A-R | CCACTGGCTACGGCAGGTC |
| Influenza B-F | GCCATTCGATTTATAGGAAGAGC |
| Influenza B-R | CACTTGATCAACTAGAGCCT |
| RSV-F | AGAAATGAAATTTGAAGTGT |
| RSV-R | GATTCTATCTCAATGTTGAT |
| RNase P gene-F | TGGAGCCAGAGACCGACACA |
| RNase P gene-R | ACATGGCTCTGGTCCGAGGT |
| Target | The Number of Specimens Tested | The Number of Positive Results | Sensitivity * | Specificity * |
|---|---|---|---|---|
| SARS-CoV-2 | 10 | 10 | 100.0% | 100.0% |
| Influenza A | 16 | 16 | 100.0% | 100.0% |
| Influenza B | 13 | 13 | 100.0% | 100.0% |
| RSV | 10 | 9 | 90.0% | 100.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, H.; Tsou, J.-H.; Chinthalapally, M.; Liu, H.; Jiang, F. Detection and Differentiation of SARS-CoV-2, Influenza, and Respiratory Syncytial Viruses by CRISPR. Diagnostics 2021, 11, 823. https://doi.org/10.3390/diagnostics11050823
Zhou H, Tsou J-H, Chinthalapally M, Liu H, Jiang F. Detection and Differentiation of SARS-CoV-2, Influenza, and Respiratory Syncytial Viruses by CRISPR. Diagnostics. 2021; 11(5):823. https://doi.org/10.3390/diagnostics11050823
Chicago/Turabian StyleZhou, Huifen, Jen-Hui Tsou, Molangur Chinthalapally, Hongjie Liu, and Feng Jiang. 2021. "Detection and Differentiation of SARS-CoV-2, Influenza, and Respiratory Syncytial Viruses by CRISPR" Diagnostics 11, no. 5: 823. https://doi.org/10.3390/diagnostics11050823