
A Novel Deep Learning Method for Recognition and Classification of Brain Tumors from MRI Images

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
- The proposed method can precisely segment and classify the brain tumors from MRI images under the presence of blurring, noise, and bias field-effect variations in input images.
- We have created the annotations which are essential for the training of the proposed model because available datasets do not have a bounding box and mask ground truths (GTs).
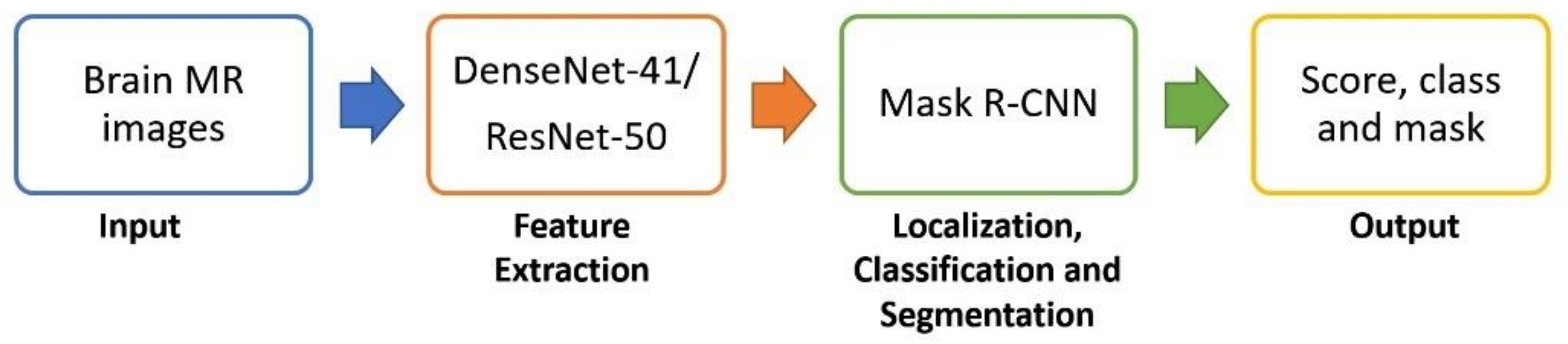
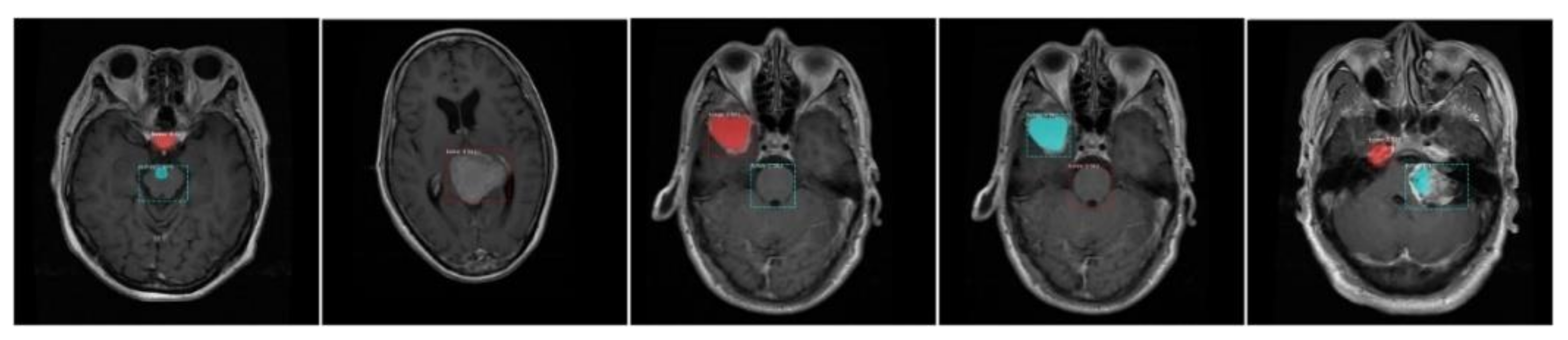
- The accurate localization and segmentation of tumor regions due to an effective region proposal network of DenseNet-41-based Mask-RCNN as it works in an end-to-end manner.
- Extensive experiments are performed using two different datasets to show the robustness of the presented framework and compared obtained results with the existing state-of-the-art methods.
2. Related Work
3. Proposed Methodology
3.1. Preprocessing
3.2. Annotations
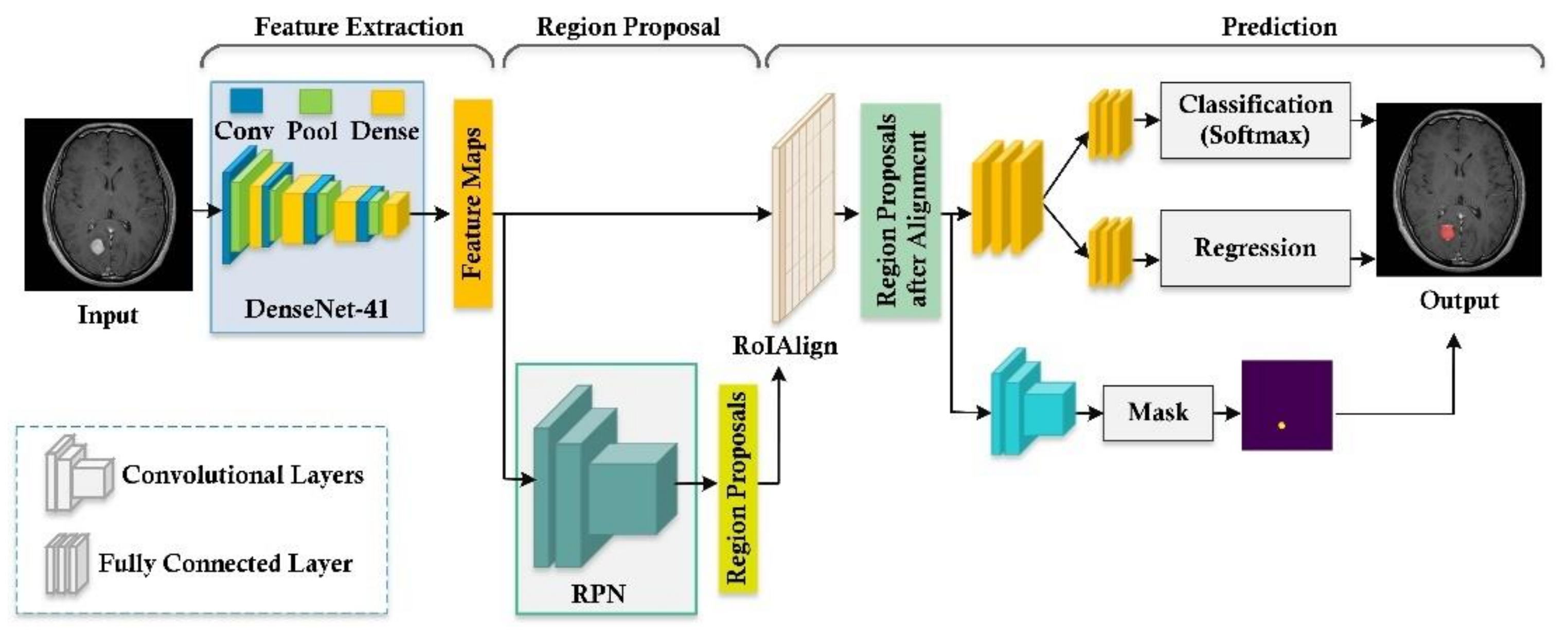
3.3. Tumor Localization and Segmentation Using Mask-RCNN
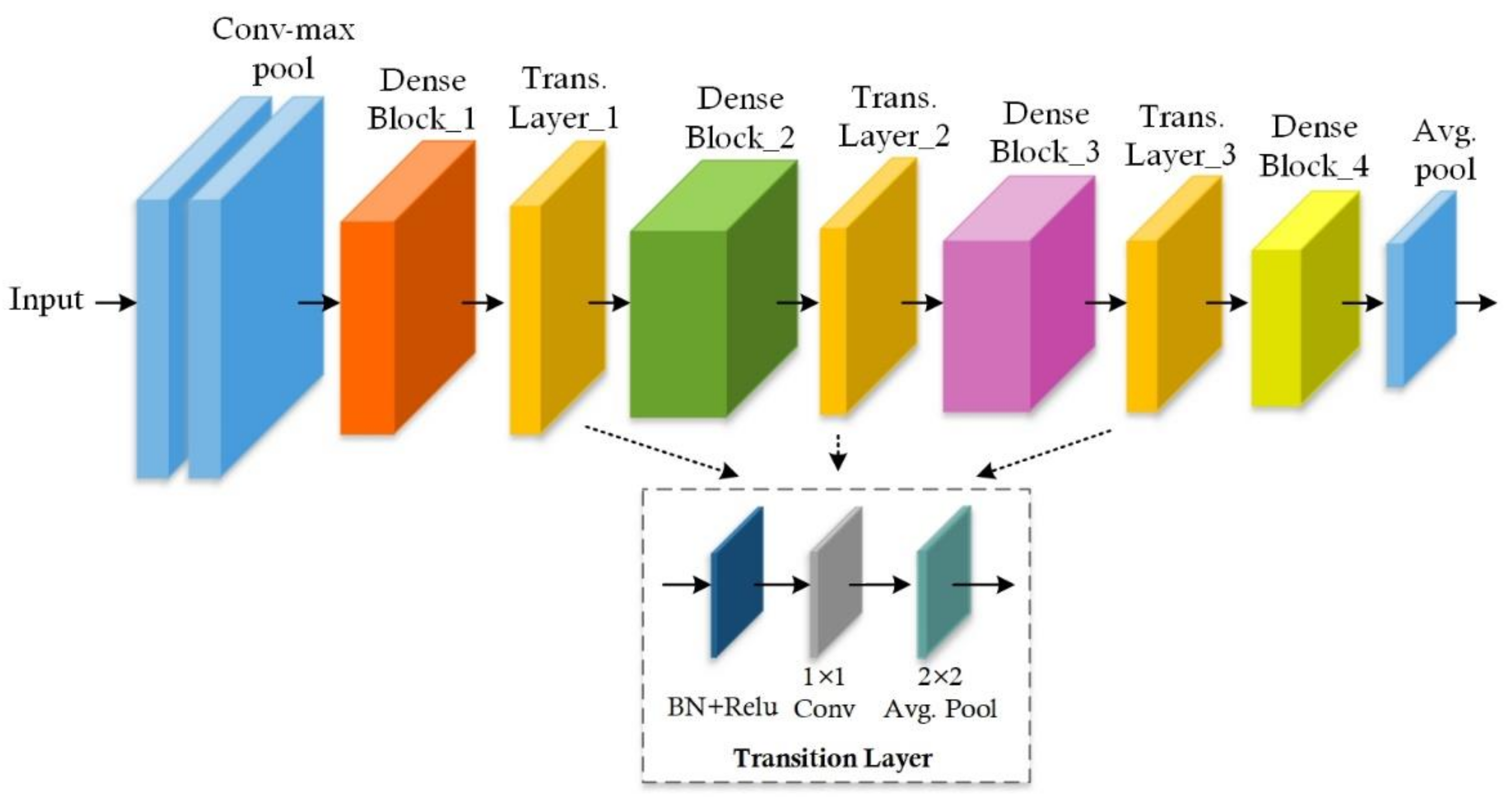
3.3.1. Feature Extraction
3.3.2. Region Proposal Network
3.3.3. RoI Classification and Bounding Box Regression
3.3.4. Segmentation Mask Acquisition
3.4. Loss Function
4. Performance Evaluation
4.1. Experimental Setup
4.2. Dataset
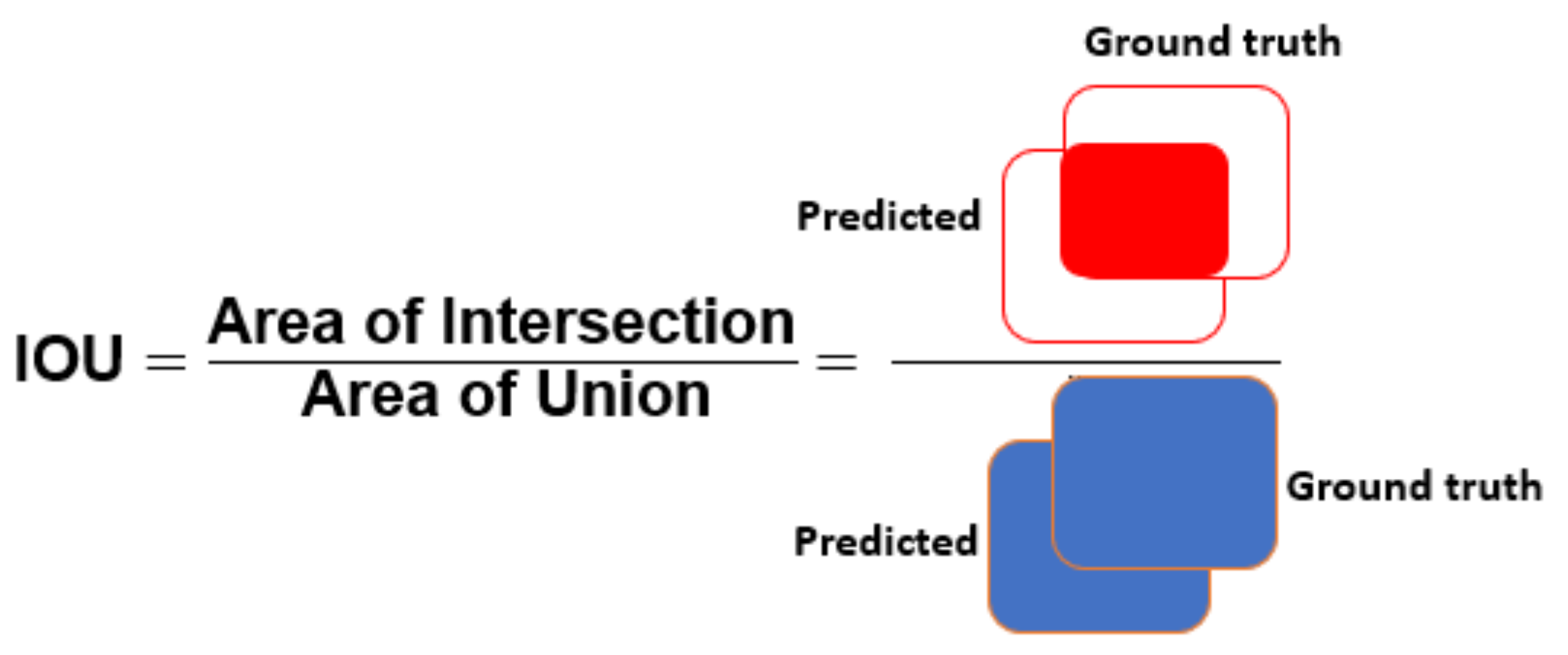
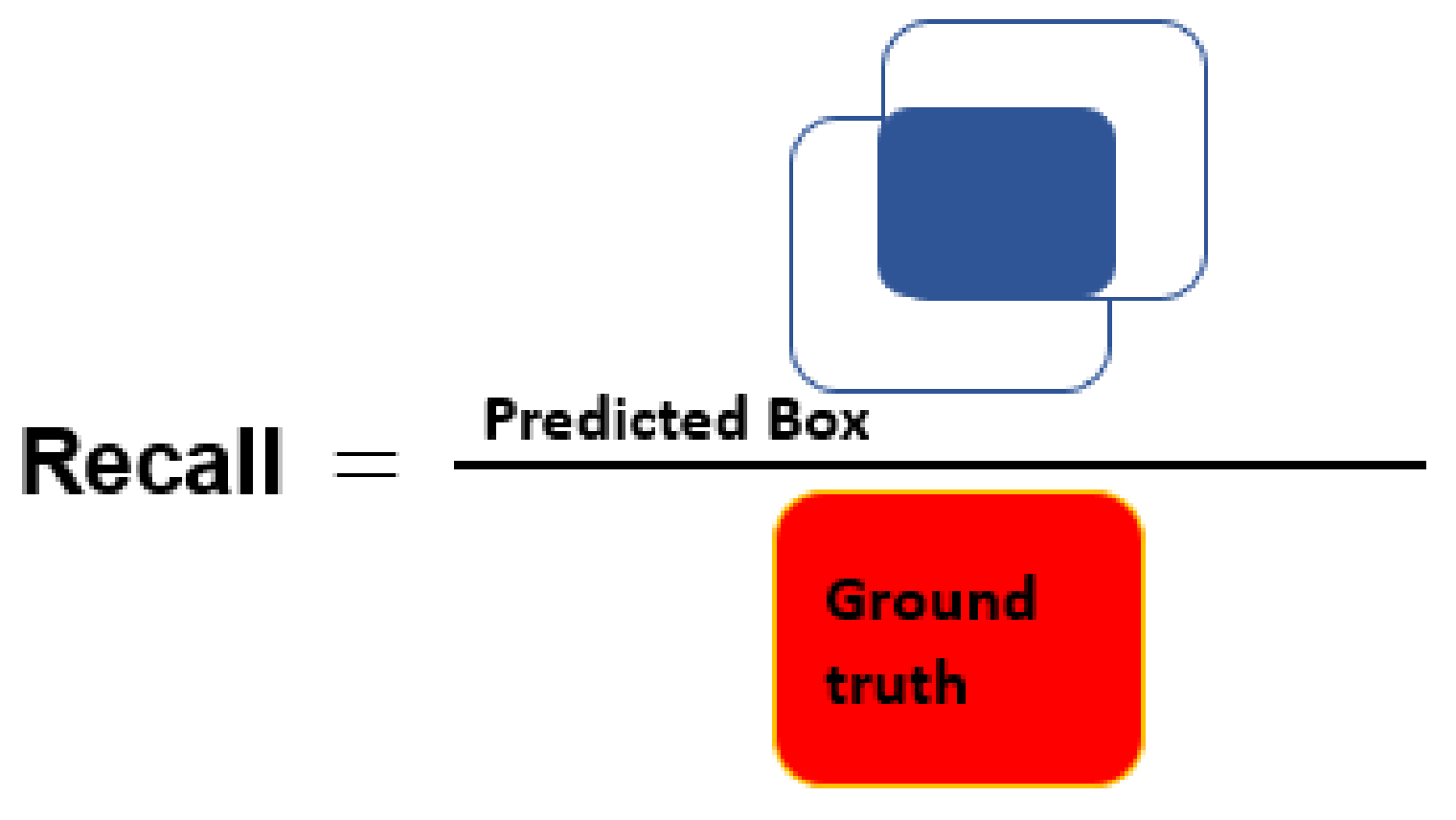
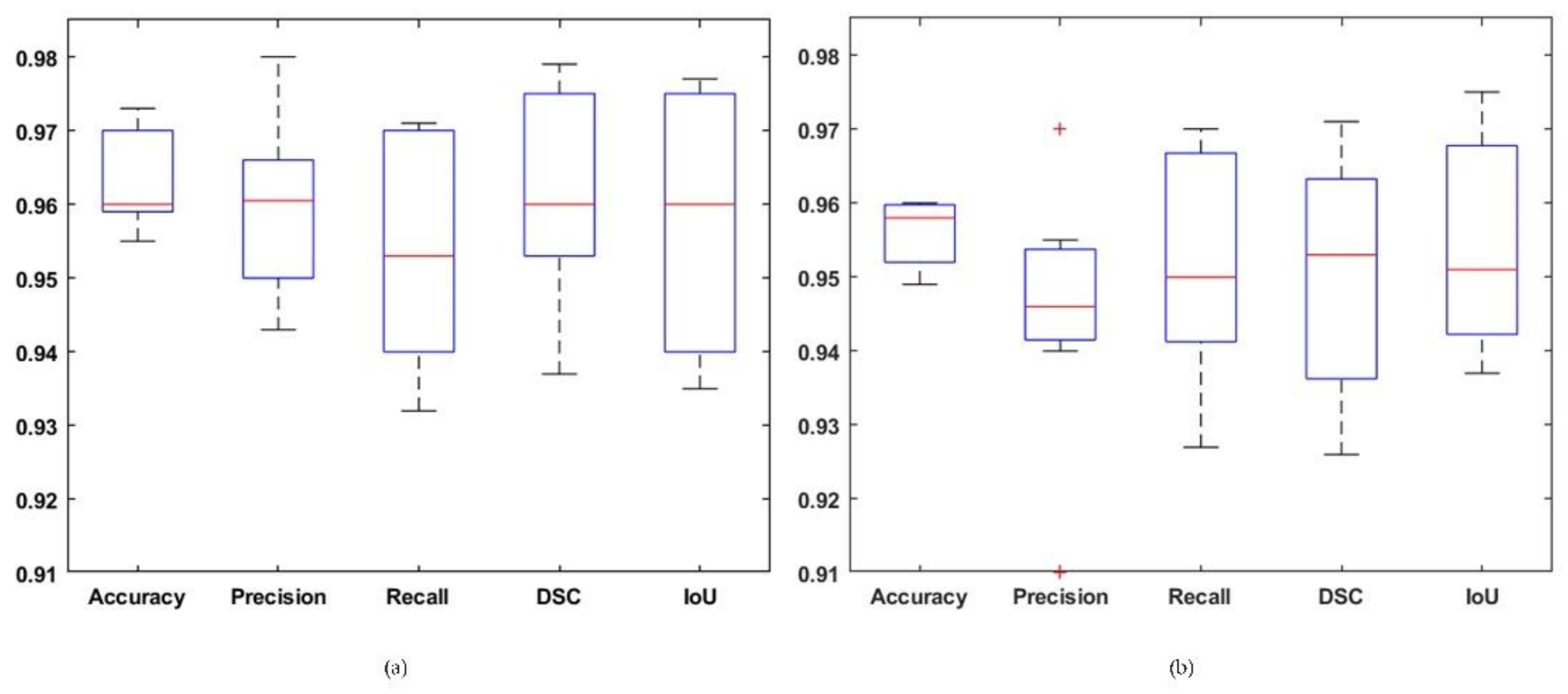
4.3. Evaluation Metrics
4.4. Experimental Results and Discussion
4.4.1. Comparison with RCNN-Based Methods
4.4.2. Comparison with Other Segmentation Techniques
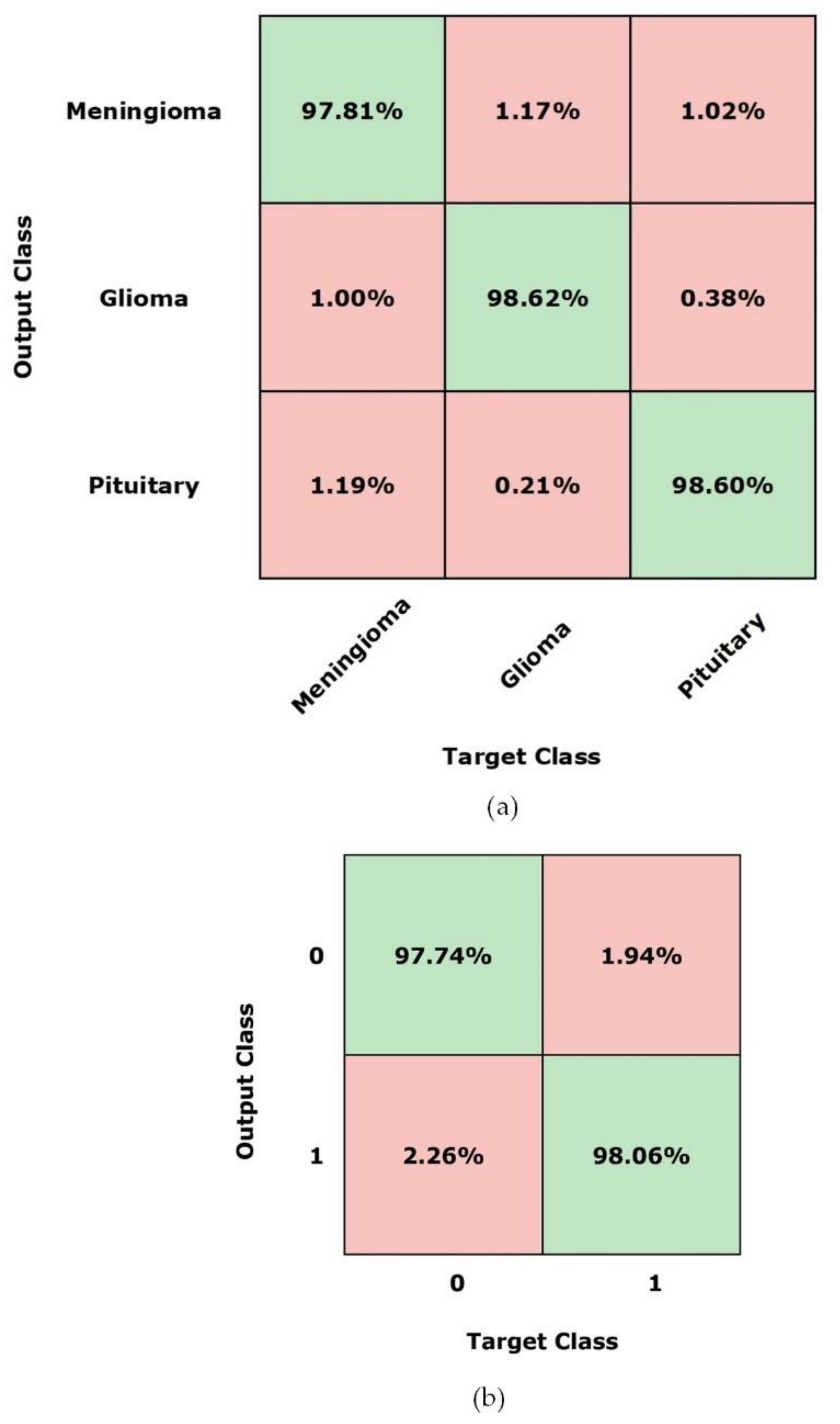
4.4.3. Comparison with Other Classification Techniques
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeAngelis, L.M. Brain tumors. N. Engl. J. Med. 2001, 344, 114–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultan, H.H.; Salem, N.M.; Al-Atabany, W. Multi-classification of Brain Tumor Images using Deep Neural Network. IEEE Access 2019, 7, 69215–69225. [Google Scholar] [CrossRef]
- Behin, A.; Hoang-Xuan, K.; Carpentier, A.F.; Delattre, J.-Y. Primary brain tumours in adults. Lancet 2003, 361, 323–331. [Google Scholar] [CrossRef]
- Akil, M.; Saouli, R.; Kachouri, R. Fully automatic brain tumor segmentation with deep learning-based selective attention using overlapping patches and multi-class weighted cross-entropy. Med. Image Anal. 2020, 63, 101692. [Google Scholar]
- Maharjan, S.; Alsadoon, A.; Prasad, P.; Al-Dalain, T.; Alsadoon, O.H. A novel enhanced softmax loss function for brain tumour detection using deep learning. J. Neurosci. Methods 2020, 330, 108520. [Google Scholar] [CrossRef] [PubMed]
- Smoll, N.R.; Schaller, K.; Gautschi, O.P. Long-term survival of patients with glioblastoma multiforme (GBM). J. Clin. Neurosci. 2013, 20, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, P.B.; Robinson, A.G.; Martinez, J.A. Metastatic tumor of the pituitary gland. Neurosurgery 1987, 21, 941–944. [Google Scholar] [CrossRef] [PubMed]
- Komninos, J.; Vlassopoulou, V.; Protopapa, D.; Korfias, S.; Kontogeorgos, G.; Sakas, D.E.; Thalassinos, N.C. Tumors metastatic to the pituitary gland: Case report and literature review. J. Clin. Endocrinol. Metab. 2004, 89, 574–580. [Google Scholar] [CrossRef] [Green Version]
- Ullah, M.N.; Park, Y.; Kim, G.B.; Kim, C.; Park, C.; Choi, H.; Yeom, J.-Y. Simultaneous Acquisition of Ultrasound and Gamma Signals with a Single-Channel Readout. Sensors 2021, 21, 1048. [Google Scholar] [CrossRef]
- Bauer, S.; Wiest, R.; Nolte, L.-P.; Reyes, M. A survey of MRI-based medical image analysis for brain tumor studies. Phys. Med. Biol. 2013, 58, R97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olabarriaga, S.D.; Smeulders, A.W. Interaction in the segmentation of medical images: A survey. Med. Image Anal. 2001, 5, 127–142. [Google Scholar] [CrossRef]
- Asa, S.L. Tumors of the Pituitary Gland; Amer Registry of Pathology: Washington, DC, USA, 1998. [Google Scholar]
- Işın, A.; Direkoğlu, C.; Şah, M. Review of MRI-based brain tumor image segmentation using deep learning methods. Procedia Comput. Sci. 2016, 102, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Goetz, M.; Weber, C.; Binczyk, F.; Polanska, J.; Tarnawski, R.; Bobek-Billewicz, B.; Koethe, U.; Kleesiek, J.; Stieltjes, B.; Maier-Hein, K.H. DALSA: Domain adaptation for supervised learning from sparsely annotated MR images. IEEE Trans. Med. Imaging 2015, 35, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Yao, J. Image processing in tumor imaging. In New Techniques in Oncologic Imaging; Routledge: Abingdon, UK, 2006; pp. 79–102. [Google Scholar]
- Ding, Y.; Zhang, C.; Lan, T.; Qin, Z.; Zhang, X.; Wang, W. Classification of Alzheimer's disease based on the combination of morphometric feature and texture feature. In Proceedings of the 2015 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Washington, DC, USA, 9–12 November 2015; pp. 409–412. [Google Scholar]
- Ding, Y.; Dong, R.; Lan, T.; Li, X.; Shen, G.; Chen, H.; Qin, Z. Multi-modal brain tumor image segmentation based on SDAE. Int. J. Imaging Syst. Tech. 2018, 28, 38–47. [Google Scholar] [CrossRef]
- Bauer, S.; Nolte, L.-P.; Reyes, M. Fully automatic segmentation of brain tumor images using support vector machine classification in combination with hierarchical conditional random field regularization. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Toronto, ON, Canada, 18–22 September 2011; pp. 354–361. [Google Scholar]
- Tustison, N.J.; Shrinidhi, K.; Wintermark, M.; Durst, C.R.; Kandel, B.M.; Gee, J.C.; Grossman, M.C.; Avants, B.B. Optimal symmetric multimodal templates and concatenated random forests for supervised brain tumor segmentation (simplified) with ANTsR. Neuroinformatics 2015, 13, 209–225. [Google Scholar] [CrossRef]
- Zikic, D.; Glocker, B.; Konukoglu, E.; Criminisi, A.; Demiralp, C.; Shotton, J.; Thomas, O.M.; Das, T.; Jena, R.; Price, S.J. Decision forests for tissue-specific segmentation of high-grade gliomas in multi-channel MR. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nice, France, 1–5 October 2012; pp. 369–376. [Google Scholar]
- Kaya, I.E.; Pehlivanlı, A.Ç.; Sekizkardeş, E.G.; Ibrikci, T. PCA based clustering for brain tumor segmentation of T1w MRI images. Comput. Meth. Prog. Bio. 2017, 140, 19–28. [Google Scholar] [CrossRef]
- Hooda, H.; Verma, O.P.; Singhal, T. Brain tumor segmentation: A performance analysis using K-Means, Fuzzy C-Means and Region growing algorithm. In Proceedings of the 2014 IEEE International Conference on Advanced Communications, Control and Computing Technologies, Ramanathapuram, India, 8–10 May 2014; pp. 1621–1626. [Google Scholar]
- Khalid, S.; Khalil, T.; Nasreen, S. A survey of feature selection and feature extraction techniques in machine learning. In Proceedings of the 2014 Science and Information Conference, London, UK, 27–29 August 2014; pp. 372–378. [Google Scholar]
- Riaz, H.; Park, J.; Choi, H.; Kim, H.; Kim, J. Deep and Densely Connected Networks for Classification of Diabetic Retinopathy. Diagnostics 2020, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Mehmood, A.; Iqbal, M.; Mehmood, Z.; Irtaza, A.; Nawaz, M.; Nazir, T.; Masood, M. Prediction of Heart Disease Using Deep Convolutional Neural Networks. Arab. J. Sci. Eng. 2021, 46, 3409–3422. [Google Scholar] [CrossRef]
- Nazir, T.; Irtaza, A.; Javed, A.; Malik, H.; Hussain, D.; Naqvi, R.A. Retinal Image Analysis for Diabetes-Based Eye Disease Detection Using Deep Learning. Appl. Sci. 2020, 10, 6185. [Google Scholar] [CrossRef]
- Hu, K.; Gan, Q.; Zhang, Y.; Deng, S.; Xiao, F.; Huang, W.; Cao, C.; Gao, X. Brain Tumor Segmentation Using Multi-Cascaded Convolutional Neural Networks and Conditional Random Field. IEEE Access 2019, 7, 92615–92629. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; Van Der Laak, J.A.; Van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, S.; Pinto, A.; Alves, V.; Silva, C.A. Brain tumor segmentation using convolutional neural networks in MRI images. IEEE Trans. Med. Imaging 2016, 35, 1240–1251. [Google Scholar] [CrossRef]
- Havaei, M.; Davy, A.; Warde-Farley, D.; Biard, A.; Courville, A.; Bengio, Y.; Pal, C.; Jodoin, P.-M.; Larochelle, H. Brain tumor segmentation with deep neural networks. Med. Image Anal. 2017, 35, 18–31. [Google Scholar] [CrossRef] [Green Version]
- Kamnitsas, K.; Ledig, C.; Newcombe, V.F.; Simpson, J.P.; Kane, A.D.; Menon, D.K.; Rueckert, D.; Glocker, B. Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmentation. Med. Image Anal. 2017, 36, 61–78. [Google Scholar] [CrossRef]
- Zhao, X.; Wu, Y.; Song, G.; Li, Z.; Zhang, Y.; Fan, Y. A deep learning model integrating FCNNs and CRFs for brain tumor segmentation. Med. Image Anal. 2018, 43, 98–111. [Google Scholar] [CrossRef]
- Dong, H.; Yang, G.; Liu, F.; Mo, Y.; Guo, Y. Automatic brain tumor detection and segmentation using U-Net based fully convolutional networks. In Proceedings of the Annual Conference on Medical Image Understanding and Analysis, Edinburgh, UK, 11–13 July 2017; pp. 506–517. [Google Scholar]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R.B. Mask R-CNN. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2980–2988. [Google Scholar]
- Cheng, J. Brain tumor dataset. Available online: https://figshare.com/articles/brain_tumor_dataset/1512427 (accessed on 21 December 2020).
- Brain MRI Images for Brain Tumor Detection. Available online: https://www.kaggle.com/navoneel/brain-mri-images-for-brain-tumor-detection (accessed on 1 April 2021).
- Jeong, J.; Lei, Y.; Kahn, S.; Liu, T.; Curran, W.J.; Shu, H.-K.; Mao, H.; Yang, X. Brain tumor segmentation using 3D Mask R-CNN for dynamic susceptibility contrast enhanced perfusion imaging. Phys. Med. Biol. 2020, 65, 185009. [Google Scholar] [CrossRef]
- Anantharaman, R.; Velazquez, M.; Lee, Y. Utilizing Mask R-CNN for Detection and Segmentation of Oral Diseases. In Proceedings of the 2018 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 3–6 December 2018; pp. 2197–2204. [Google Scholar]
- Chiao, J.-Y.; Chen, K.-Y.; Liao, K.Y.-K.; Hsieh, P.-H.; Zhang, G.; Huang, T.-C. Detection and classification the breast tumors using mask R-CNN on sonograms. Medicine 2019, 98, e15200. [Google Scholar] [CrossRef]
- Kopelowitz, E.; Englehard, G. Lung Nodules Detection and Segmentation using 3D Mask-RCNN. arXiv preprint 2019, arXiv:1907.07676. [Google Scholar]
- Ismael, S.A.A.; Mohammed, A.; Hefny, H. An enhanced deep learning approach for brain cancer MRI images classification using residual networks. Artif. Intell. Med. 2020, 102, 101779. [Google Scholar] [CrossRef]
- Kleesiek, J.; Biller, A.; Urban, G.; Kothe, U.; Bendszus, M.; Hamprecht, F. Ilastik for multi-modal brain tumor segmentation. In Proceedings of the MICCAI BraTS (Brain Tumor Segmentation Challenge), Boston, MA, USA, 14 September 2014; pp. 12–17. [Google Scholar]
- Kamnitsas, K.; Ferrante, E.; Parisot, S.; Ledig, C.; Nori, A.V.; Criminisi, A.; Rueckert, D.; Glocker, B. DeepMedic for brain tumor segmentation. In Proceedings of the International workshop on Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Athens, Greece, 17 October 2016; pp. 138–149. [Google Scholar]
- Zhang, W.; Li, R.; Deng, H.; Wang, L.; Lin, W.; Ji, S.; Shen, D. Deep convolutional neural networks for multi-modality isointense infant brain image segmentation. NeuroImage 2015, 108, 214–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, X.; Tustison, N.; Meyer, C. Brain tumor segmentation using an ensemble of 3d u-nets and overall survival prediction using radiomic features. In Proceedings of the International MICCAI Brainlesion Workshop, Granada, Spain, 16 September 2018; pp. 279–288. [Google Scholar]
- Qasem, S.N.; Nazar, A.; Attia Qamar, S. A Learning Based Brain Tumor Detection System. Comput. Mater. Contin. 2019, 59, 713–727. [Google Scholar] [CrossRef]
- Rehman, A.; Naz, S.; Naseem, U.; Razzak, I.; Hameed, I.A. Deep AutoEncoder-Decoder Framework for Semantic Segmentation of Brain Tumor. Aust. J. Intell. Inf. Process. Syst. 2019, 15, 53. [Google Scholar]
- Rayhan, F. FR-MRInet: A Deep Convolutional Encoder-Decoder for Brain Tumor Segmentation with Relu-RGB and Sliding-window. Int. J. Comput. Appl. 2018, 975, 8887. [Google Scholar]
- Gispert, J.D.; Reig, S.; Pascau, J.; Vaquero, J.J.; García-Barreno, P.; Desco, M. Method for bias field correction of brain T1-weighted magnetic resonance images minimizing segmentation error. Hum. Brain Mapp. 2004, 22, 133–144. [Google Scholar] [CrossRef] [Green Version]
- Zhan, T.; Zhang, J.; Xiao, L.; Chen, Y.; Wei, Z. An improved variational level set method for MR image segmentation and bias field correction. Magn. Reson. Imaging 2013, 31, 439–447. [Google Scholar] [CrossRef]
- Hwang, H.; Haddad, R.A. Adaptive median filters: New algorithms and results. IEEE Trans. Image Process. 1995, 4, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Dutta, A.; Gupta, A.; Zisserman, A. Vgg Image Annotator (VIA). Available online: http://www.robots.ox.ac.uk/˜vgg/software/via (accessed on 12 December 2020).
- Ren, S.; He, K.; Girshick, R.B.; Sun, J. Faster R-CNN: Towards Real-Time Object Detection with Region Proposal Networks. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 1137–1149. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Albahli, S.; Nazir, T.; Irtaza, A.; Javed, A. Recognition and Detection of Diabetic Retinopathy Using Densenet-65 Based Faster-RCNN. Comput. Mater. Contin. 2021, 67, 1333–1351. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Mask-RCNN. Available online: https://github.com/matterport/Mask_RCNN (accessed on 12 December 2020).
- Sheela, C.J.J.; Suganthi, G. Brain tumor segmentation with radius contraction and expansion based initial contour detection for active contour model. Multimed. Tools. Appl. 2020, 79, 23793–23819. [Google Scholar] [CrossRef]
- Sobhaninia, Z.; Rezaei, S.; Karimi, N.; Emami, A.; Samavi, S. Brain Tumor Segmentation by Cascaded Deep Neural Networks Using Multiple Image Scales. In Proceedings of the 2020 28th Iranian Conference on Electrical Engineering (ICEE), Tabriz, Iran, 4–6 August 2020; pp. 1–4. [Google Scholar]
- Gunasekara, S.R.; Kaldera, H.; Dissanayake, M.B. A Systematic Approach for MRI Brain Tumor Localization and Segmentation Using Deep Learning and Active Contouring. J. Healthc. Eng. 2021, 2021. [Google Scholar] [CrossRef]
- Díaz-Pernas, F.J.; Martínez-Zarzuela, M.; Antón-Rodríguez, M.; González-Ortega, D. A Deep Learning Approach for Brain Tumor Classification and Segmentation Using a Multiscale Convolutional Neural Network. Healthcare 2021, 9, 153. [Google Scholar] [CrossRef]
- Masood, M.; Nazir, T.; Nawaz, M.; Javed, A.; Iqbal, M.; Mehmood, A. Brain Tumor Localization and Segmentation using Mask RCNN. Front. Comput. Sci. 2020. (accepted). Preprint version. Available online: https://journal.hep.com.cn/fcs/EN/article/downloadArticleFile.do?attachType=PDF&id=28181 (accessed on 20 April 2021). [CrossRef]
- Deepak, S.; Ameer, P. Brain tumor classification using deep CNN features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef]
- Swati, Z.N.K.; Zhao, Q.; Kabir, M.; Ali, F.; Ali, Z.; Ahmed, S.; Lu, J. Brain tumor classification for MR images using transfer learning and fine-tuning. Comput. Med. Imaging Graph. 2019, 75, 34–46. [Google Scholar] [CrossRef]
- Huang, Z.; Du, X.; Chen, L.; Li, Y.; Liu, M.; Chou, Y.; Jin, L. Convolutional Neural Network Based on Complex Networks for Brain Tumor Image Classification with a Modified Activation Function. IEEE Access 2020, 8, 89281–89290. [Google Scholar] [CrossRef]
- Gumaei, A.; Hassan, M.M.; Hassan, M.R.; Alelaiwi, A.; Fortino, G. A hybrid feature extraction method with regularized extreme learning machine for brain tumor classification. IEEE Access 2019, 7, 36266–36273. [Google Scholar] [CrossRef]
- Toğaçar, M.; Ergen, B.; Cömert, Z. Tumor type detection in brain MR images of the deep model developed using hypercolumn technique, attention modules, and residual blocks. Med. Biol. Eng. Comput. 2021, 59, 57–70. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Value |
|---|---|
| Epochs | 45 |
| Learning rate | 0.001 |
| IoU Threshold | 0.70 |
| Method | Evaluation Metrics | ||||
|---|---|---|---|---|---|
| Accuracy | mAP | Dice | Sensitivity | Time(s) | |
| RCNN [51] | 0.920 | 0.910 | 0.870 | 0.950 | 0.47 |
| Faster RCNN [56] | 0.940 | 0.940 | 0.910 | 0.940 | 0.25 |
| Proposed (Resnet-50) | 0.959 | 0.946 | 0.955 | 0.953 | 0.20 |
| Proposed (Densenet-41) | 0.963 | 0.949 | 0.959 | 0.953 | 0.20 |
| Technique | Segmentation Method | Evaluation Metrics | ||
|---|---|---|---|---|
| Mean IoU | Dice | Accuracy | ||
| Sobhaninia et al. [62] | Cascaded CNN | 0.907 | 0.800 | - |
| Gunasekara et al. [63] | Faster RCNN and ChanVese active contour | - | 0.920 | 94.6 |
| Sheela et al. [61] | Active Contour and Fuzzy-C-Means | - | 0.665 | 91.0 |
| Díaz-Pernas et al. [64] | Multi-scale CNN | - | 0.828 | - |
| Masood et al. [65] | Traditional Mask-RCNN | 0.950 | 0.950 | 95.1 |
| Proposed method | Mask-RCNN (ResNet-50) | 0.951 | 0.955 | 95.9 |
| Mask-RCNN(DenseNet-41) | 0.957 | 0.959 | 96.3 | |
| Technique | Classification Method | Acc (%) |
|---|---|---|
| Deepak et al. [66] | GoogLeNet and SVM | 97.10 |
| Swati et al. [67] | VGG19 | 94.82 |
| Huang et al. [68] | CCN based on complex networks | 95.49 |
| Gumaei et al. [69] | GIST descriptor and ELM | 94.93 |
| BrainMRNet [70] | Attention module, Hypercolumn technique, and Residual block | 97.69 |
| Proposed method | Custom Mask-RCNN | 98.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masood, M.; Nazir, T.; Nawaz, M.; Mehmood, A.; Rashid, J.; Kwon, H.-Y.; Mahmood, T.; Hussain, A. A Novel Deep Learning Method for Recognition and Classification of Brain Tumors from MRI Images. Diagnostics 2021, 11, 744. https://doi.org/10.3390/diagnostics11050744
Masood M, Nazir T, Nawaz M, Mehmood A, Rashid J, Kwon H-Y, Mahmood T, Hussain A. A Novel Deep Learning Method for Recognition and Classification of Brain Tumors from MRI Images. Diagnostics. 2021; 11(5):744. https://doi.org/10.3390/diagnostics11050744
Chicago/Turabian StyleMasood, Momina, Tahira Nazir, Marriam Nawaz, Awais Mehmood, Junaid Rashid, Hyuk-Yoon Kwon, Toqeer Mahmood, and Amir Hussain. 2021. "A Novel Deep Learning Method for Recognition and Classification of Brain Tumors from MRI Images" Diagnostics 11, no. 5: 744. https://doi.org/10.3390/diagnostics11050744