
Shear Wave Elastography and Shear Wave Dispersion Imaging in the Assessment of Liver Disease in Alpha1-Antitrypsin Deficiency

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. 2D-SWE and SWD
2.2. ATI
2.3. TE/CAP
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the Cohort
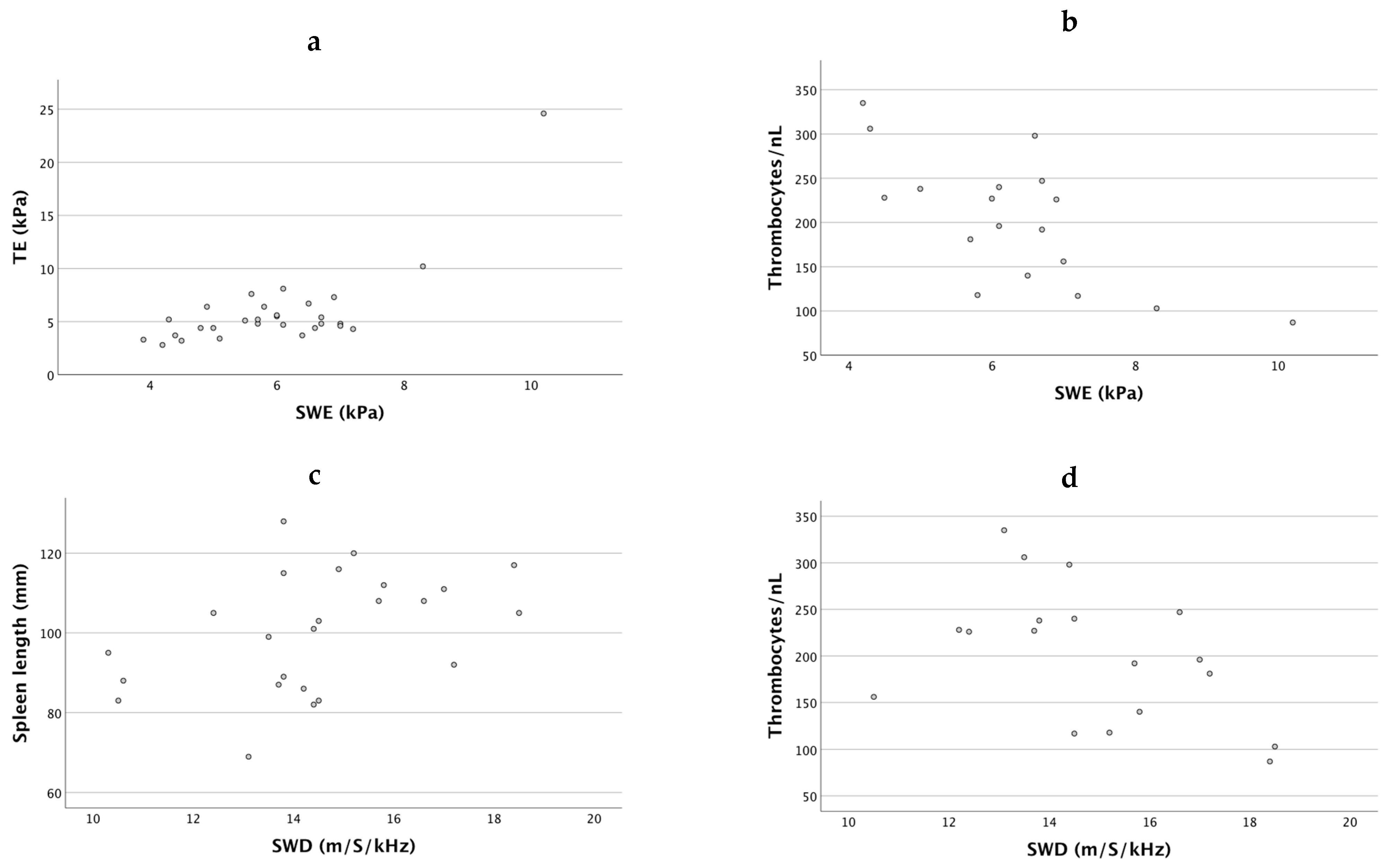
3.2. 2D-SWE Measurements in Patients with AATD Is Correlated with Established Predictors of Liver Fibrosis
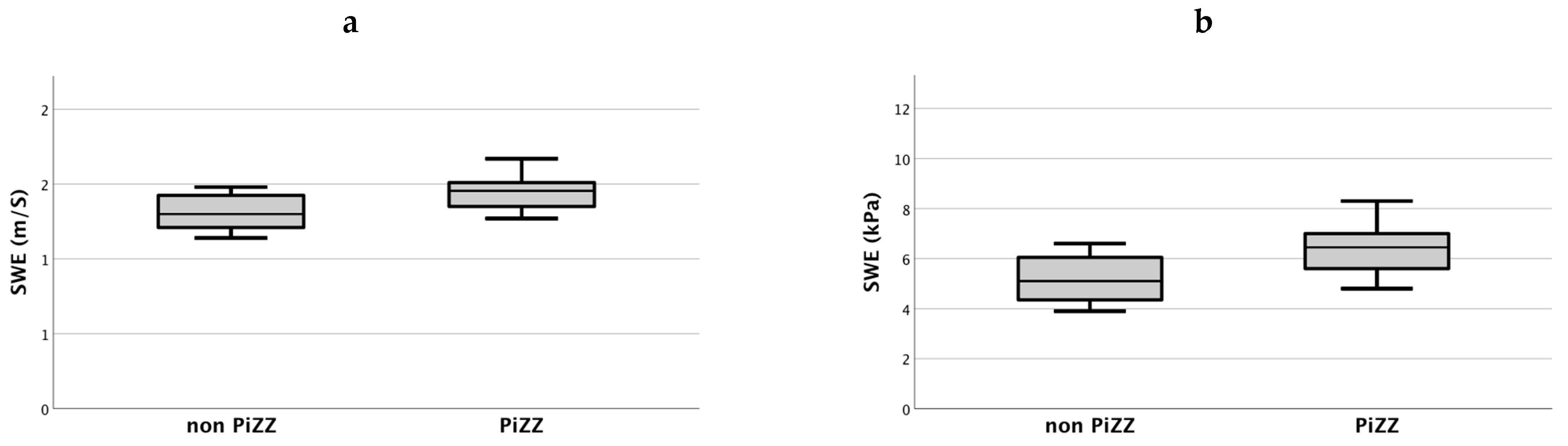
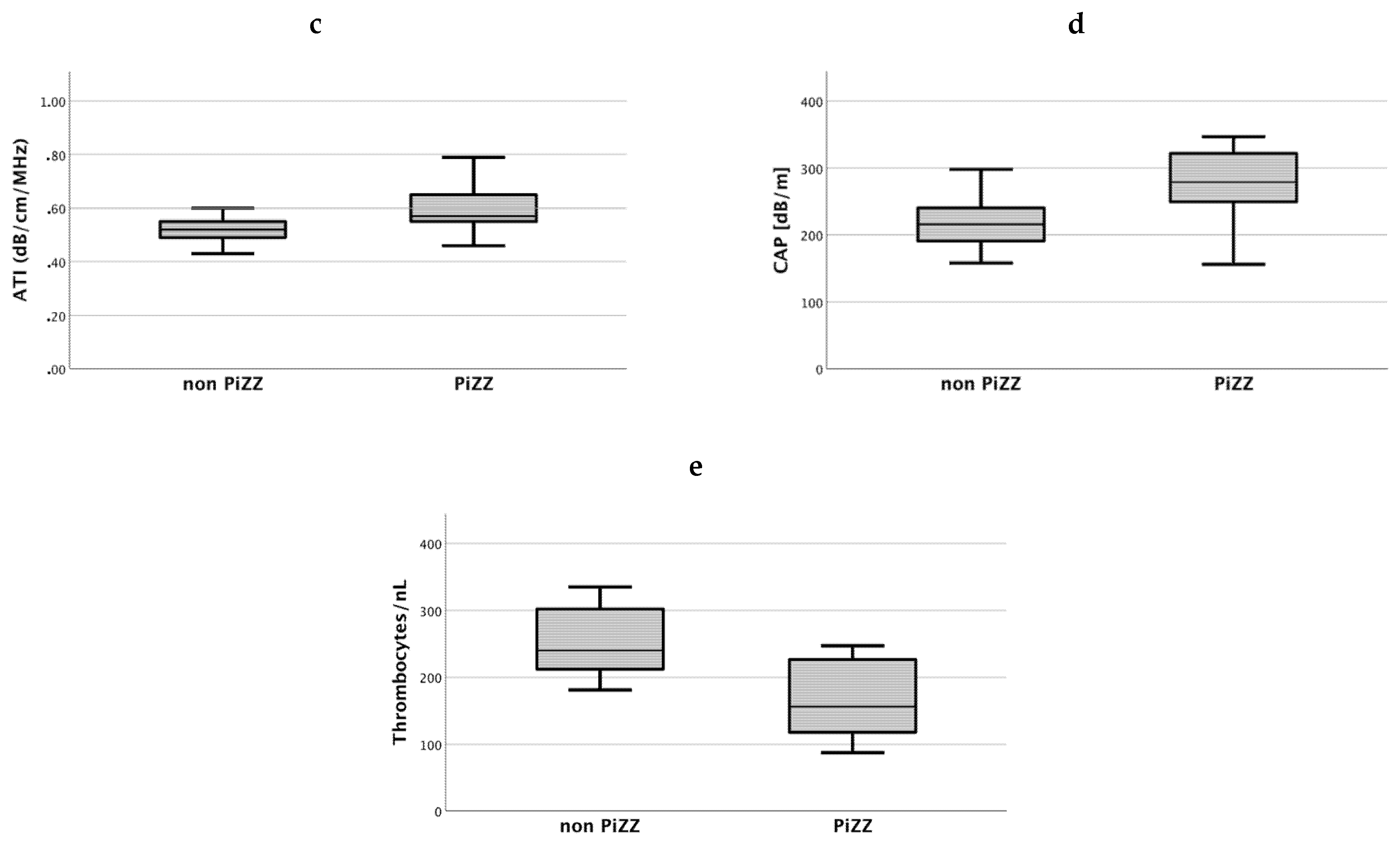
3.3. AATD Patients with PiZZ Genotype Show Increased Ultrasound-Based Liver Injury Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tanash, H.A.; Piitulainen, E. Liver disease in adults with severe alpha-1-antitrypsin deficiency. J. Gastroenterol. 2019, 54, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Strnad, P.; McElvaney, N.G.; Lomas, D.A. Alpha(1)-Antitrypsin Deficiency. N. Engl. J. Med. 2020, 382, 1443–1455. [Google Scholar] [CrossRef]
- Manne, V.; Kowdley, K.V. Alpha1-Antitrypsin Deficiency: A Cause of Chronic Liver Disease. Clin. Liver Dis. 2020, 24, 483–492. [Google Scholar] [CrossRef]
- Clark, V.C.; Dhanasekaran, R.; Brantly, M.; Rouhani, F.; Schreck, P.; Nelson, D.R. Liver test results do not identify liver disease in adults with α(1)-antitrypsin deficiency. Clin. Gastroenterol. Hepatol. 2012, 10, 1278–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, M.; Tacke, F. Identifying High-Risk NASH Patients: What We Know so Far. Hepatic Med. 2020, 12, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M.; Giuricin, M.; Bonazza, D.; Rosso, N.; Giraudi, P.J.; Masutti, F.; Palmucci, S.; Basile, A.; Zanconati, F.; de Manzini, N.; et al. Optimization of Point-Shear Wave Elastography by Skin-to-Liver Distance to Assess Liver Fibrosis in Patients Undergoing Bariatric Surgery. Diagnostics 2020, 10, 795. [Google Scholar] [CrossRef] [PubMed]
- Giuffrè, M.; Fouraki, S.; Comar, M.; Masutti, F.; Crocè, L.S. The Importance of Transaminases Flare in Liver Elastography: Characterization of the Probability of Liver Fibrosis Overestimation by Hepatitis C Virus-Induced Cytolysis. Microorganisms 2020, 8, 348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giuffrè, M.; Bedogni, G.; Abazia, C.; Masutti, F.; Tiribelli, C.; Crocè, L.S. Spleen stiffness can be employed to assess the efficacy of spontaneous portosystemic shunts in relieving portal hypertension. Ann. Hepatol. 2020, 19, 691–693. [Google Scholar] [CrossRef]
- Giuffrè, M.; Macor, D.; Masutti, F.; Abazia, C.; Tinè, F.; Patti, R.; Buonocore, M.R.; Colombo, A.; Visintin, A.; Campigotto, M.; et al. Evaluation of spleen stiffness in healthy volunteers using point shear wave elastography. Ann. Hepatol. 2019, 18, 736–741. [Google Scholar] [CrossRef]
- Giuffrè, M.; Fouraki, S.; Campigotto, M.; Colombo, A.; Visintin, A.; Buonocore, M.R.; Aversano, A.; Budel, M.; Tinè, F.; Abazia, C.; et al. Alanine aminotransferase and spleno-portal dynamics affect spleen stiffness measured by point shear-wave elastography in patients with chronic hepatitis C in the absence of significant liver fibrosis. J. Ultrasound 2021, 24, 67–73. [Google Scholar] [CrossRef]
- Giuffrè, M.; Macor, D.; Masutti, F.; Abazia, C.; Tinè, F.; Bedogni, G.; Tiribelli, C.; Crocè, L.S. Spleen Stiffness Probability Index (SSPI): A simple and accurate method to detect esophageal varices in patients with compensated liver cirrhosis. Ann. Hepatol. 2020, 19, 53–61. [Google Scholar] [CrossRef]
- Piccinni, R.; Rodrigues, S.G.; Montani, M.; Murgia, G.; Delgado, M.G.; Casu, S.; Stirnimann, G.; Semmo, N.; De Gottardi, A.; Dufour, J.F.; et al. Controlled attenuation parameter reflects steatosis in compensated advanced chronic liver disease. Liver Int. 2019, 40, 1151–1158. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi Burgio, M.; Ronot, M.; Reizine, E.; Rautou, P.E.; Castera, L.; Paradis, V.; Garteiser, P.; Van Beers, B.; Vilgrain, V. Quantification of hepatic steatosis with ultrasound: Promising role of attenuation imaging coefficient in a biopsy-proven cohort. Eur. Radiol. 2020, 30, 2293–2301. [Google Scholar] [CrossRef] [PubMed]
- Tada, T.; Iijima, H.; Kobayashi, N.; Yoshida, M.; Nishimura, T.; Kumada, T.; Kondo, R.; Yano, H.; Kage, M.; Nakano, C.; et al. Usefulness of Attenuation Imaging with an Ultrasound Scanner for the Evaluation of Hepatic Steatosis. Ultrasound Med. Biol. 2019, 45, 2679–2687. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Abe, M.; Yoshimasu, Y.; Kasai, Y.; Sakamaki, K.; Hara, T.; Itoi, T. The Role of Multiparametric US of the Liver for the Evaluation of Nonalcoholic Steatohepatitis. Radiology 2020, 296, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Moriyasu, F.; Oshiro, H.; Takeuchi, H.; Yoshimasu, Y.; Kasai, Y.; Itoi, T. Clinical utilization of shear wave dispersion imaging in diffuse liver disease. Ultrasonography 2020, 39, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Clark, V.C.; Marek, G.; Liu, C.; Collinsworth, A.; Shuster, J.; Kurtz, T.; Nolte, J.; Brantly, M. Clinical and histologic features of adults with alpha-1 antitrypsin deficiency in a non-cirrhotic cohort. J. Hepatol. 2018, 69, 1357–1364. [Google Scholar] [CrossRef]
- Hamesch, K.; Mandorfer, M.; Pereira, V.M.; Moeller, L.S.; Pons, M.; Dolman, G.E.; Reichert, M.C.; Schneider, C.V.; Woditsch, V.; Voss, J.; et al. Liver Fibrosis and Metabolic Alterations in Adults With alpha-1-antitrypsin Deficiency Caused by the Pi*ZZ Mutation. Gastroenterology 2019, 157, 705–719.e718. [Google Scholar] [CrossRef]
- Diaz, S.; Mostafavi, B.; Tanash, H.A.; Piitulainen, E. Acoustic radiation force impulse (ARFI) elastography in a cohort of alpha-1 antitrypsin-deficient individuals and healthy volunteers. Acta Radiol. Open 2018, 7, 2058460118768363. [Google Scholar] [CrossRef] [Green Version]
- Reiter, R.; Wetzel, M.; Hamesch, K.; Strnad, P.; Asbach, P.; Haas, M.; Siegmund, B.; Trautwein, C.; Hamm, B.; Klatt, D.; et al. Comparison of non-invasive assessment of liver fibrosis in patients with alpha1-antitrypsin deficiency using magnetic resonance elastography (MRE), acoustic radiation force impulse (ARFI) Quantification, and 2D-shear wave elastography (2D-SWE). PLoS ONE 2018, 13, e0196486. [Google Scholar] [CrossRef] [Green Version]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basic principles and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietrich, C.F.; Bamber, J.; Berzigotti, A.; Bota, S.; Cantisani, V.; Castera, L.; Cosgrove, D.; Ferraioli, G.; Friedrich-Rust, M.; Gilja, O.H.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Liver Ultrasound Elastography, Update 2017 (Long Version). Ultraschall Med. 2017, 38, e48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.H.; Lee, E.S.; Lee, J.Y.; Bae, J.S.; Kim, H.; Lee, K.B.; Yu, S.J.; Cho, E.J.; Lee, J.H.; Cho, Y.Y.; et al. Two-Dimensional-Shear Wave Elastography with a Propagation Map: Prospective Evaluation of Liver Fibrosis Using Histopathology as the Reference Standard. Korean J. Radiol. 2020, 21, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.S.; Lee, D.H.; Lee, J.Y.; Kim, H.; Yu, S.J.; Lee, J.H.; Cho, E.J.; Lee, Y.B.; Han, J.K.; Choi, B.I. Assessment of hepatic steatosis by using attenuation imaging: A quantitative, easy-to-perform ultrasound technique. Eur. Radiol. 2019, 29, 6499–6507. [Google Scholar] [CrossRef]
- Friedrich-Rust, M.; Poynard, T.; Castera, L. Critical comparison of elastography methods to assess chronic liver disease. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 402–411. [Google Scholar] [CrossRef]
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.G.; Mi, Y.Q.; de Ledinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.H.; Cardoso, A.C.; et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J. Hepatol. 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- Fromme, M.; Schneider, C.V.; Pereira, V.; Hamesch, K.; Pons, M.; Reichert, M.C.; Benini, F.; Ellis, P.; Thorhauge, K.; Mandorfer, M.; et al. Hepatobiliary phenotypes of adults with alpha-1 antitrypsin deficiency. Gut 2021. online ahead of print. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 29) |
|---|---|
| Genotype | 18 PiZZ |
| 8 PiMZ | |
| 2 PiSZ | |
| 1 PiZP-Lowell | |
| Gender | 15 Female (51.7%) |
| 14 Male (48.3%) | |
| Age | Median 66.5 Years, Range 22–80 Years |
| Laboratory Findings: | |
| Total Bilirubin | 0.49 mg/dL, Range 0.1–1.16 mg/dL |
| ALT | 23 U/L, Range 6–87 U/L |
| AST | 25 U/L, Range 15–94 U/L |
| GGT | 24 U/L, Range 10–155 U/L |
| Platelet Count | 211/nL, Range 87–335 U/L |
| US Findings: | |
| PV Maximum Velocity | 20.9 cm/S |
| Spleen Length | 102 mm |
| 2D-SWE | 1.42 m/S, Range 1.14–1.83 m/S |
| 6 kPa, Range 3.9–10.2 kPa | |
| SWD | 14.2 m/S/kHz, Range 10.3–18.5 m/S/kHz |
| TE | 4.8 kPa, Range 2.8–24.6 kPa |
| ATI | 0.56 dB/cm/MHz, Range 0.43–0.96 dB/cm/MHz |
| CAP | 249.5 dB/m, Range 156–347 dB/m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, M.; Kleinjans, M.; Strnad, P.; Demir, M.; Holtmann, T.M.; Tacke, F.; Wree, A. Shear Wave Elastography and Shear Wave Dispersion Imaging in the Assessment of Liver Disease in Alpha1-Antitrypsin Deficiency. Diagnostics 2021, 11, 629. https://doi.org/10.3390/diagnostics11040629
Schulz M, Kleinjans M, Strnad P, Demir M, Holtmann TM, Tacke F, Wree A. Shear Wave Elastography and Shear Wave Dispersion Imaging in the Assessment of Liver Disease in Alpha1-Antitrypsin Deficiency. Diagnostics. 2021; 11(4):629. https://doi.org/10.3390/diagnostics11040629
Chicago/Turabian StyleSchulz, Marten, Moritz Kleinjans, Pavel Strnad, Münevver Demir, Theresa M. Holtmann, Frank Tacke, and Alexander Wree. 2021. "Shear Wave Elastography and Shear Wave Dispersion Imaging in the Assessment of Liver Disease in Alpha1-Antitrypsin Deficiency" Diagnostics 11, no. 4: 629. https://doi.org/10.3390/diagnostics11040629