
Prognostic Factors Associated with 5-Year Overall Survival in Cervical Cancer Patients Treated with Radical Hysterectomy Followed by Adjuvant Concurrent Chemoradiation Therapy at a Tertiary Care Center in Eastern Europe



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Treatments
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
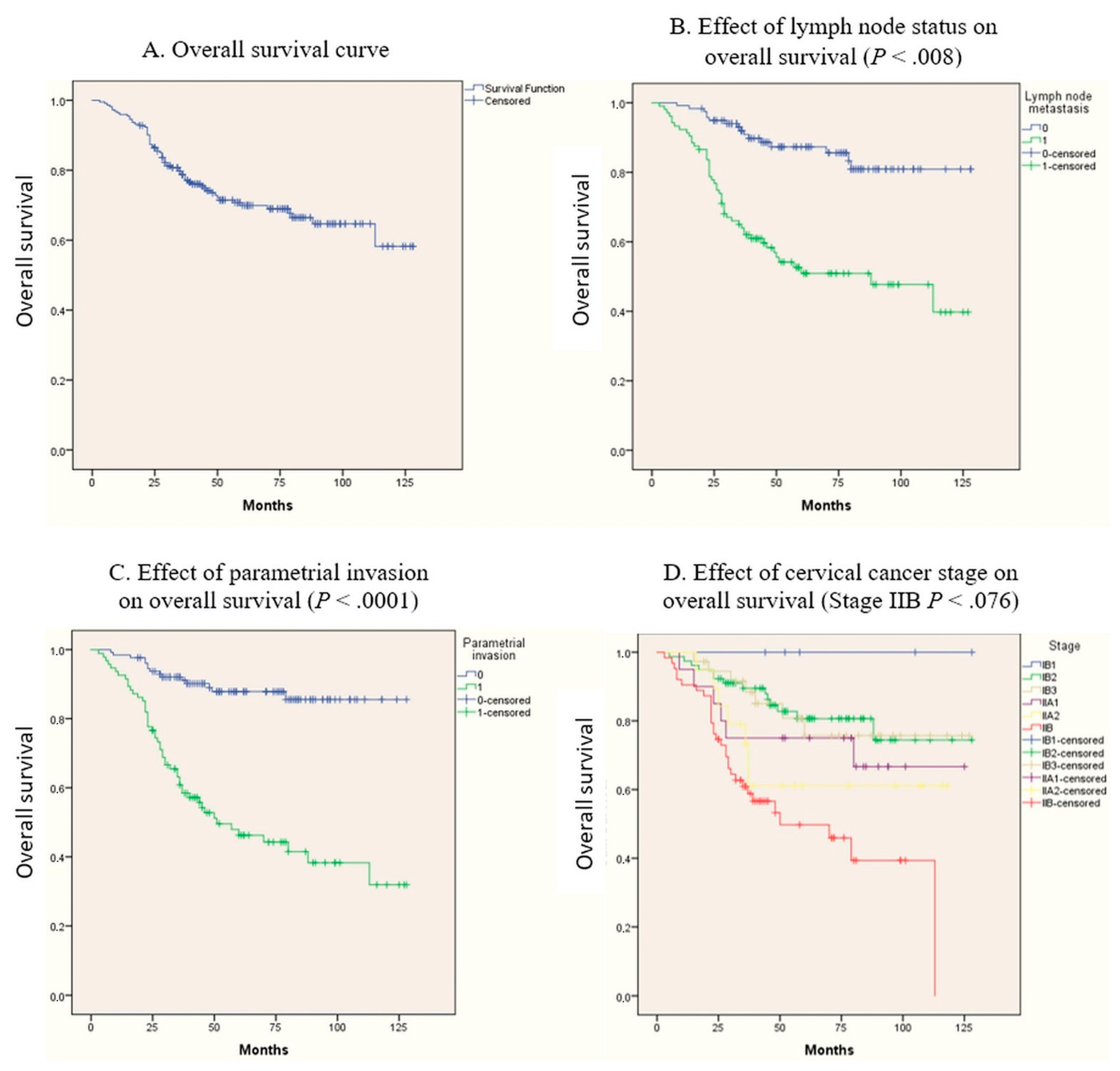
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaffney, D.K.; Hashibe, M.; Kepka, D.; Maurer, K.A.; Werner, T.L. Too many women are dying from cervix cancer: Problems and solutions. Gynecol. Oncol. 2018, 151, 547–554. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0090825818312800 (accessed on 23 March 2020). [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Pötter, R.; Planchamp, F.; Avall-Lundqvist, E.; Fischerova, D.; Meder, C.H.; Köhler, C.; Landoni, F.; Lax, S.; Lindegaard, J.C.; et al. The European Society of Gynaecological Oncology/European Society for Radiotherapy and Oncology/European Society of Pathology guidelines for the management of patients with cervical cancer. Radiother. Oncol. 2018, 127, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Berek, J.S.; Fredes, M.C.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S.T.; Konishi, I.; Olawaiye, A.B.; Prat, J.; et al. Revised FIGO staging for carcinoma of the cervix uteri. Int. J. Gynecol. Obstet. 2019, 145, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Guo, J.; Zhang, X.; Chen, M.; Xu, C.; Yao, L. Feasibility of radical hysterectomy in women with FIGO stage IIB cervical cancer: An observation study of 10-year experience in a tertiary center. OncoTargets Ther. 2018, 11, 5527–5533. [Google Scholar] [CrossRef] [Green Version]
- Keys, H.M.; Bundy, B.N.; Stehman, F.B.; Muderspach, L.I.; Chafe, W.E.; Suggs, C.L.; Walker, J.L.; Gersell, D. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N. Engl. J. Med. 1999, 340, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Peters, W.A.; Liu, P.Y.; Barrett, R.J.; Stock, R.J.; Monk, B.J.; Berek, J.S.; Souhami, L.; Grigsby, P.; Gordon, W., Jr.; Alberts, D.S. Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J. Clin. Oncol. 2000, 18, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- CNEPSS. Cancerul de Col Uterin. Available online: https://insp.gov.ro/sites/cnepss/cancerul-de-col-uterin/ (accessed on 14 February 2021).
- Căpîlna, M.E.; Szabo, B.; Rusu, S.C.; Becsi, J.; Moldovan, B.; Neagoe, R.M.; Muhlfay, G. Anatomical variations of the obturator veins and their surgical implications. Eur. J. Gynaecol. Oncol. 2017, 38, 263–265. [Google Scholar]
- Kasamatsu, T.; Onda, T.; Sawada, M.; Kato, T.; Ikeda, S.-I. Radical hysterectomy for FIGO stage IIB cervical cancer: Clinicopathological characteristics and prognostic evaluation. Gynecol. Oncol. 2009, 114, 69–74. [Google Scholar] [CrossRef]
- Kawagoe, T.; Kashimura, M.; Matsuura, Y.; Sugihara, K.; Toki, N.; Aoki, T. Clinical significance of tumor size in stage IB and II carcinoma of the uterine cervix. Int. J. Gynecol. Cancer 1999, 9, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Koh, W.J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Cohn, D.; Crispens, M.A.; DuPont, N.; Eifel, P.J.; et al. Cervical cancer, version 3.2019, NCCN Clinical Practice Guidelines in Oncology. JNCCN 2019, 17, 64–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv72–83. [Google Scholar] [CrossRef]
- Vale, C.; Tierney, J.F.; Stewart, L.A.; Brady, M.; Dinshaw, K.; Jakobsen, A.; Parmar, M.K.B.; Thomas, G.; Trimble, T.; Alberts, D.S.; et al. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: A systematic review and meta-analysis of individual patient data from 18 randomized trials. J. Clin. Oncol. 2008, 26, 5802–5812. [Google Scholar]
- Sedlis, A.; Bundy, B.N.; Rotman, M.Z.; Lentz, S.S.; Muderspach, L.I.; Zaino, R.J. A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A gynecologic oncology group study. Gynecol. Oncol. 1999, 73, 177–183. [Google Scholar] [CrossRef]
- Hale, R.J.; Wilcox, F.L.; Buckley, C.H.; Tindall, V.R.; Ryder, W.D.J.; Logueh, J.P. Prognostic factors in uterine cervical carcinoma: A clinicopathological analysis. Int. J. Gynecol. Cancer 1991, 1, 19–23. [Google Scholar] [CrossRef]
- Zaino, R.J.; Ward, S.; Delgado, G.; Bundy, B.; Gore, H.; Fetter, G.; Ganjei, P.; Frauenhofer, E. Histopathologic predictors of the behavior of surgically treated stage IB squamous cell carcinoma of the cervix a gynecologic oncology group study. Cancer 1992, 69, 1750–1758. [Google Scholar] [CrossRef]
- Matsuo, K.; Mandelbaum, R.S.; Machida, H.; Purushotham, S.; Grubbs, B.H.; Roman, L.D.; Wright, J.D. Association of tumor differentiation grade and survival of women with squamous cell carcinoma of the uterine cervix. J. Gynecol. Oncol. 2018, 29. [Google Scholar] [CrossRef] [PubMed]
- Ryu, S.Y.; Kim, M.H.; Nam, B.H.; Lee, T.S.; Song, E.S.; Park, C.Y.; Kim, J.W.; Kim, Y.B.; Ryu, H.S.; Park, S.Y.; et al. Intermediate-risk grouping of cervical cancer patients treated with radical hysterectomy: A Korean Gynecologic Oncology Group study. Br. J. Cancer 2014, 110, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, A.H.; Varia, M.A.; Moore, D.; Rao, G.G.; Gaffney, D.K.; Erickson-Wittmann, B.A.; Jhingran, A.; Mayr, N.A.; Puthawala, A.A.; Small, W., Jr.; et al. ACR Appropriateness Criteria® role of adjuvant therapy in the management of early stage cervical cancer. Gynecol. Oncol. 2012, 125, 256–262. Available online: https://pubmed.ncbi.nlm.nih.gov/22155418/ (accessed on 31 January 2021). [CrossRef]
- Lim, S.; Lee, S.-H.; Lee, K.B.; Park, C.-Y. The influence of number of high risk factors on clinical outcomes in patients with early-stage cervical cancer after radical hysterectomy and adjuvant chemoradiation. Obstet. Gynecol. Sci. 2016, 59, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Delgado, G.; Bundy, B.; Zaino, R.; Sevin, B.-U.; Creasman, W.T.; Major, F. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol. Oncol. 1990, 38, 352–357. [Google Scholar] [CrossRef]
- Aoki, Y.; Sasaki, M.; Watanabe, M.; Sato, T.; Tsuneki, I.; Aida, H.; Tanaka, K. High-risk group in node-positive patients with stage IB, IIA, and IIB cervical carcinoma after radical hysterectomy and postoperative pelvic irradiation. Gynecol. Oncol. 2000, 77, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Peccatori, F.A.; Azim, J.H.A.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. 6), vi160–vi170. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Choi, H.S.; Byun, J.S. Overall 5-year survival rate and prognostic factors in patients with stage IB and IIA cervical cancer treated by radical hysterectomy and pelvic lymph node dissection. Int. J. Gynecol. Cancer 2000, 10, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Casarin, J.; Bogani, G.; Papadia, A.; Ditto, A.; Pinelli, C.; Garzon, S.; Donadello, N.; Laganà, A.S.; Cromi, A.; Mueller, M.; et al. Preoperative conization and risk of recurrence in patients undergoing laparoscopic radical hysterectomy for early stage cervical cancer: A multicenter study. J. Minim. Invasive Gynecol. 2021, 28, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Sopracordevole, F.; Di Donato, V.; Ciavattini, A.; Ghelardi, A.; Lopez, S.; Simoncini, T.; Plotti, F.; Casarin, J.; Serati, M.; et al. High-risk HPV-positive and -negative high-grade cervical dysplasia: Analysis of 5-year outcomes. Gynecol. Oncol. 2021. [Google Scholar] [CrossRef]
- Yan, W.; Qiu, S.; Ding, Y.; Zhang, Q.; Si, L.; Lv, S.; Liu, L. Prognostic value of lymphovascular space invasion in patients with early stage cervical cancer in Jilin, China: A retrospective study. Medicine 2019, 98, e17301. [Google Scholar] [CrossRef]
- Căpîlna, M.E.; Moldovan, B.; Szabo, B. Pelvic exenteration--our initial experience in 15 cases. Eur. J. Gynaecol. Oncol. 2015, 36, 142–145. [Google Scholar] [PubMed]
- Gershon, A.S.; Jafarzadeh, S.R.; Wilson, K.C.; Walkey, A.J. Clinical knowledge from observational studies: Everything you wanted to know but were afraid to ask. Am. J. Respir. Crit. Care Med. 2018, 198, 859–867. Available online: https://pubmed.ncbi.nlm.nih.gov/29733678/ (accessed on 17 February 2021). [CrossRef]


{kind=link}
| Number (%) or Median (Range) | Overall Survival | Recurrences | |||||
|---|---|---|---|---|---|---|---|
| 5-Year Survival Rate | 95% CI | Mean Survival (Months) | P Value | Number | P Value | ||
| No. of Patients | 222 | 22 | |||||
| Age (Years) | 51.2 (28–76) | ||||||
| 30–40 | 62.7% | 61.9–63.5 | 90.5 | 0.740 | |||
| 41–50 | 66.4% | 65.6–67.1 | 95.9 | 0.940 | |||
| 51–60 | 67.8% | 67.1–68.4 | 93 | 0.909 | |||
| 61–70 | 65.3% | 64.3–66.2 | 90.4 | 0.876 | |||
| Provenance | |||||||
| Urban | 92 (41.4%) | 12 | |||||
| Rural | 130 (58.6%) | 10 | |||||
| Stage (FIGO 2018) | |||||||
| IB1 | 5 (2.3%) | 100% | 0.350 | ||||
| IB2 | 78 (35.1%) | 80% | 79.5–80.5 | 0.009 | 4 | 0.060 | |
| IB3 | 37 (16.7%) | 75.7% | 74.8–76.5 | 0.131 | 4 | 0.518 | |
| IIA1 | 20 (9.0%) | 66.7% | 65.5–67.8 | 0.802 | 2 | 0.615 | |
| IIA2 | 19 (8.6%) | 61.1% | 59.94–62.2 | 0.585 | 1 | 0.415 | |
| IIB | 63 (28.4%) | 39.3% | 38.4–40.2 | 0.001 | 11 | 0.020 | |
| Tumor size | 0.603 | .475 | |||||
| <4 cm | 167 (75.2%) | 70% | 69.6–70.3 | 16 | |||
| ≥4 cm | 55 (24.8%) | 68.3% | 67.5–69 | 6 | |||
| Histology | |||||||
| Squamous Cell Carcinoma | 179 (80.6%) | 78.6% | 78.2–78.9 | 94.6 | 0.856 | 18 | 0.572 |
| Adenocarcinoma | 25 (11.3%) | 68.5% | 67.5–69.5 | 96.6 | 0.896 | 2 | 0.537 |
| Other | 18 (8.1%) | 61.9% | 60.6–63 | 88.4 | 0.675 | 2 | 0.554 |
| Tumor Differentiation Grade | |||||||
| Grade 1 (Well-Differentiated) | 20 (9%) | 83.8% | 82.9–84.6 | 92.3 | 0.331 | 1 | 0.615 |
| Grade 2 (Moderately-Differentiated) | 82 (36.9%) | 71.6% | 71–72.1 | 96.8 | 0.931 | 11 | 0.135 |
| Grade 3 (Poorly-Differentiated) | 120 (54.1%) | 69.7% | 69.2–70.1 | 91.9 | 0.615 | 9 | 0.141 |
| Depth of Cervical Stromal Invasion | |||||||
| Inner 1/3 | 14 (6.3%) | 73% | 71.6–74.4 | 87.3 | 0.709 | 1 | 0.586 |
| Middle 1/3 | 26 (11.7%) | 66.8% | 65.5–66.9 | 98.5 | 0.749 | 1 | 0.238 |
| Outer 1/3 | 182 (82.0%) | 75.5% | 75.1–75.8 | 93.3 | 0.398 | 20 | 0.200 |
| Lymphovascular Space Invasion | 0.762 | 0.207 | |||||
| Positive | 171 (77.0%) | 77.4% | 77–77.7 | 94.2 | 19 | ||
| Negative | 51 (23.0%) | 68.4% | 67.7–69 | 94.7 | 3 | ||
| Parametrial Involvement | 0.0001 | 0.463 | |||||
| Positive | 94 (42.3%) | 46.3% | 45.7–46.8 | 69.9 | 10 | ||
| Negative | 128 (57.7%) | 87.8% | 87.4–88.1 | 114.7 | 12 | ||
| Resection Margin Status | 0.801 | 0.109 | |||||
| Positive | 52 (23%) | 69.6% | 68.9–70.5 | 94.3 | 8 | ||
| Negative | 170 (77%) | 70% | 69.6–70.3 | 94.1 | 14 | ||
| Pelvic Lymph Nodes Metastases | 0.0001 | 0.162 | |||||
| Positive | 104 (47%) | 58.3% | 57.8–58.8 | 76.1 | 13 | ||
| Negative | 118(53%) | 87.3% | 86.9–87.6 | 112.3 | 9 | ||
| Adjuvant Treatment | |||||||
| CCRT | 222 (100%) | ||||||
| Median Follow-Up Duration (Months) | 65.5 (3–128) | ||||||
| Status | |||||||
| Alive | 157 (70.07%) | 69.9% | 69.5–70.2 | 94.7 | |||
| Alive Free of Disease | 135 (61%) | ||||||
| Alive with Disease | 22 (9%) | ||||||
| Deceased | 65 (29.3%) | ||||||
| Variables | B | SE | Wald | P-Value | HR | 95.0% CI for OR | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| IIB | 0.535 | 0.301 | 3.145 | .076 | 1.707 | 0.945 | 3.082 |
| Parametrial Invasion | 1.200 | 0.333 | 12.979 | .0001 | 3.322 | 1.729 | 6.383 |
| Lymph Node Metastasis | 0.838 | 0.314 | 7.140 | .008 | 2.313 | 1.250 | 4.277 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanca, M.; Căpîlna, M.E. Prognostic Factors Associated with 5-Year Overall Survival in Cervical Cancer Patients Treated with Radical Hysterectomy Followed by Adjuvant Concurrent Chemoradiation Therapy at a Tertiary Care Center in Eastern Europe. Diagnostics 2021, 11, 570. https://doi.org/10.3390/diagnostics11030570
Stanca M, Căpîlna ME. Prognostic Factors Associated with 5-Year Overall Survival in Cervical Cancer Patients Treated with Radical Hysterectomy Followed by Adjuvant Concurrent Chemoradiation Therapy at a Tertiary Care Center in Eastern Europe. Diagnostics. 2021; 11(3):570. https://doi.org/10.3390/diagnostics11030570
Chicago/Turabian StyleStanca, Mihai, and Mihai Emil Căpîlna. 2021. "Prognostic Factors Associated with 5-Year Overall Survival in Cervical Cancer Patients Treated with Radical Hysterectomy Followed by Adjuvant Concurrent Chemoradiation Therapy at a Tertiary Care Center in Eastern Europe" Diagnostics 11, no. 3: 570. https://doi.org/10.3390/diagnostics11030570