
Cost-Effectiveness Analysis of 68Ga DOTA-TATE PET/CT, 111In-Pentetreotide SPECT/CT and CT for Diagnostic Workup of Neuroendocrine Tumors

 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Model Structure
2.2. Input Parameters
2.3. Efficacy of Treatment Modalities
2.4. Costs and Utilities
2.5. Transition Probabilities
2.6. Cost-Effectiveness Analysis
2.7. Sensitivity Analysis
3. Results
3.1. Estimated Outcomes and Corresponding Costs
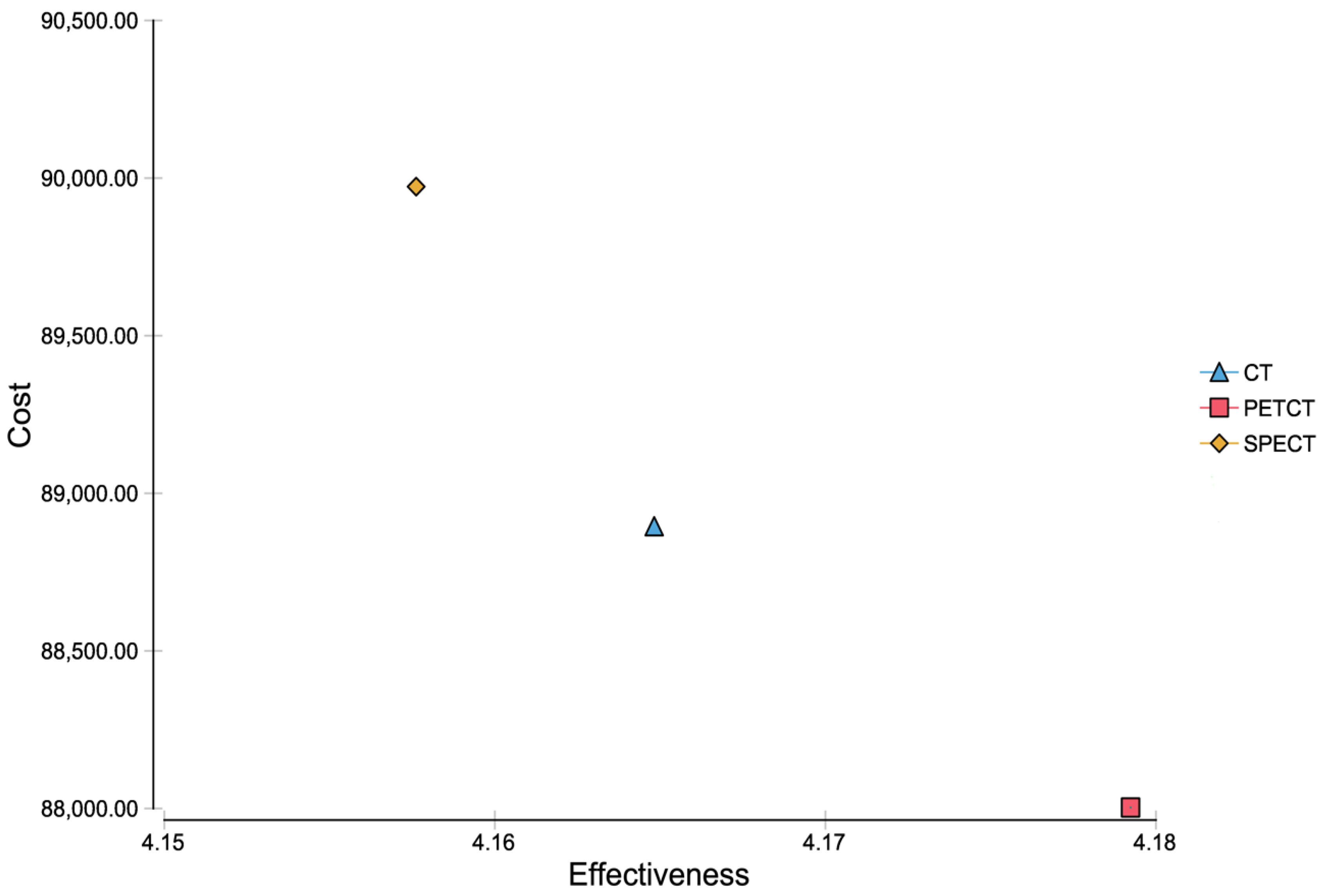
3.2. Cost-Effectiveness Analysis
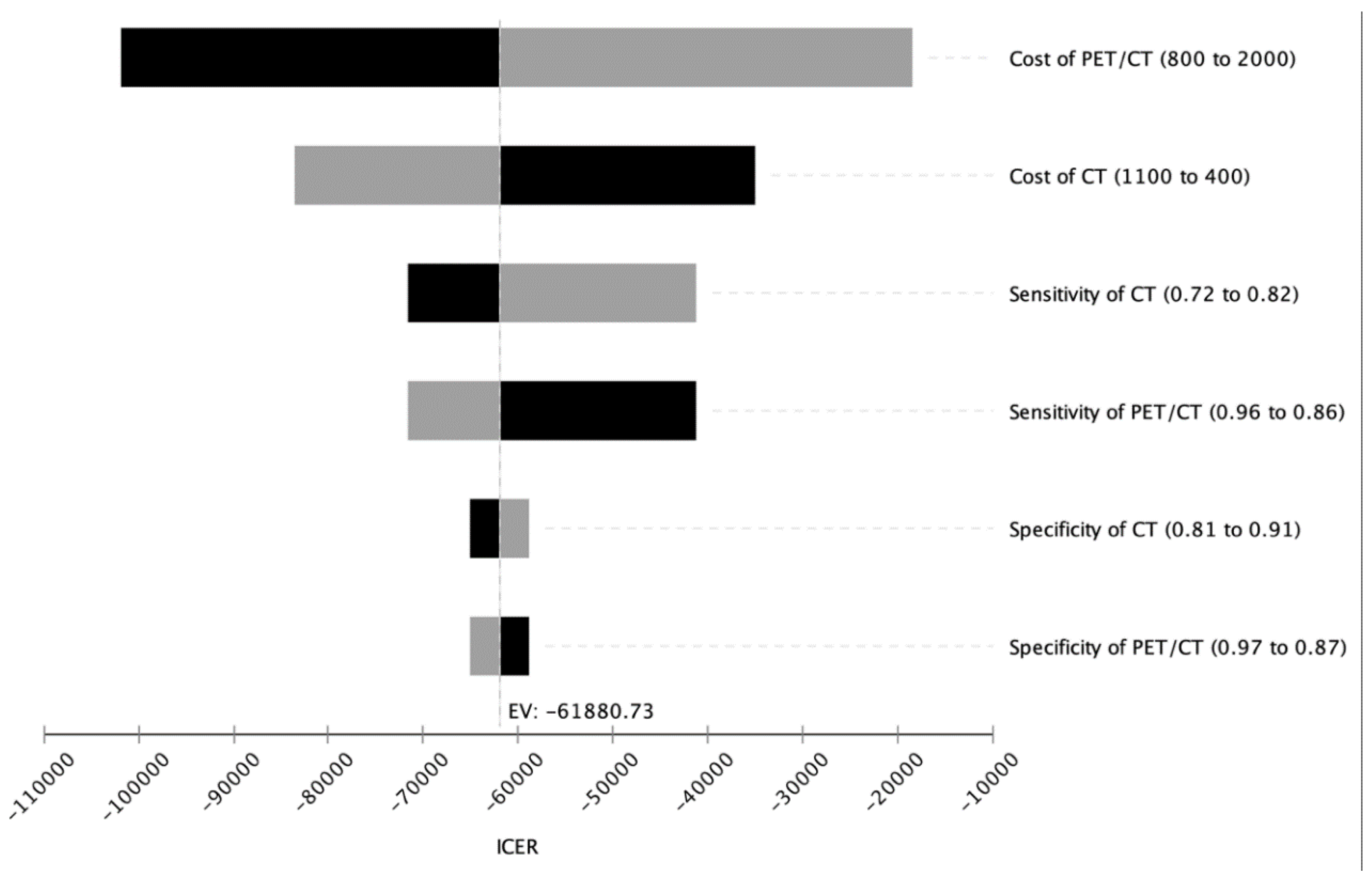
3.3. Deterministic Sensitivity Analysis
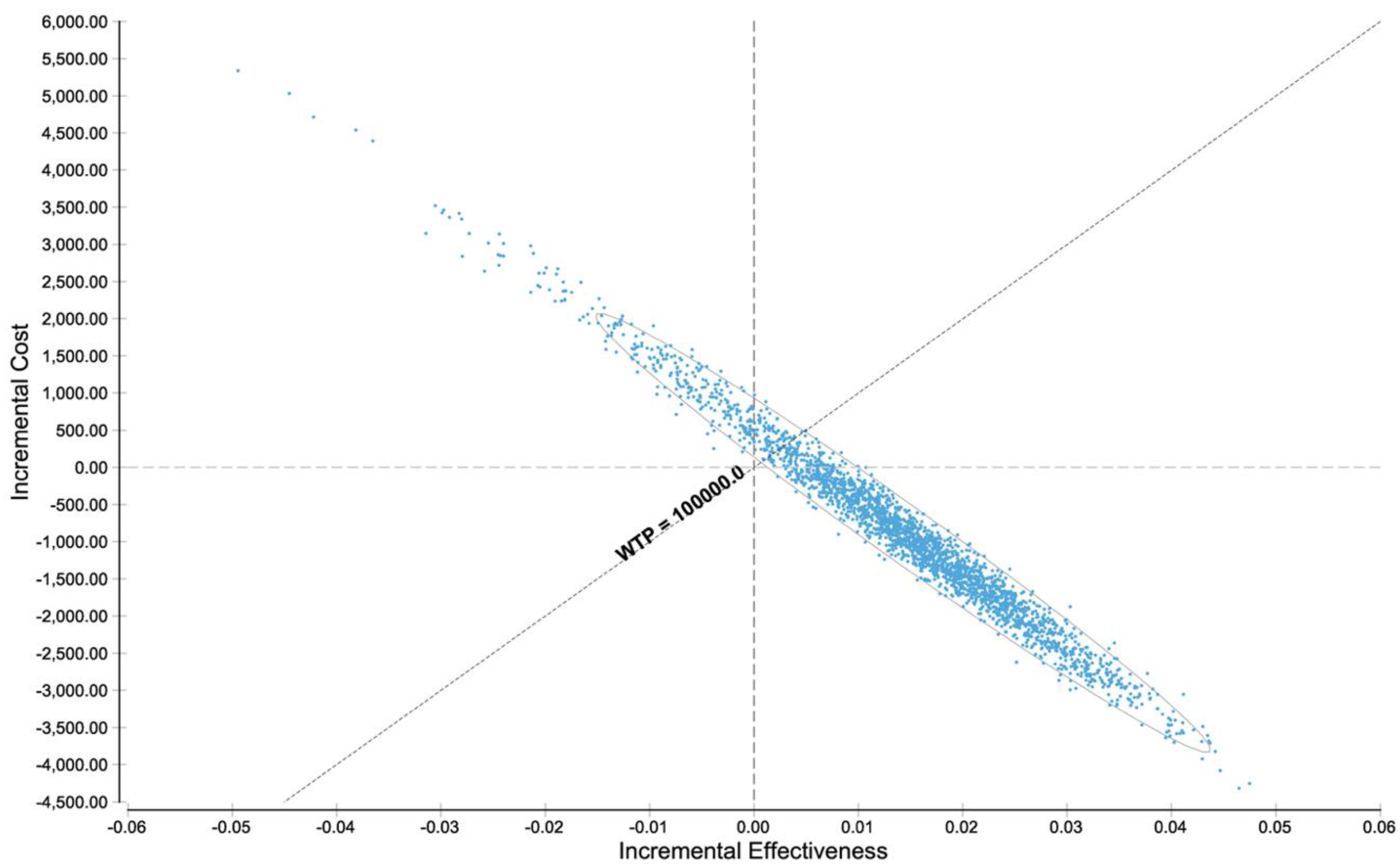
3.4. Probabilistic Sensitivity Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beaumont, J.L.; Cella, D.; Phan, A.T.; Choi, S.; Liu, Z.; Yao, J.C. Comparison of health-related quality of life in patients with neuroendocrine tumors with quality of life in the general US population. Pancreas 2012, 41, 461–466. [Google Scholar] [CrossRef]
- Man, D.; Wu, J.; Shen, Z.; Zhu, X. Prognosis of patients with neuroendocrine tumor: A SEER database analysis. Cancer Manag. Res. 2018, 10, 5629–5638. [Google Scholar] [CrossRef] [Green Version]
- Fallahi, B.; Manafi-Farid, R.; Eftekhari, M.; Fard-Esfahani, A.; Emami-Ardekani, A.; Geramifar, P.; Akhlaghi, M.; Hashemi Taheri, A.P.; Beiki, D. Diagnostic fficiency of (68)Ga-DOTATATE PET/CT as ompared to (99m)Tc-Octreotide SPECT/CT andonventional orphologic odalities in euroendocrine umors. Asia Ocean. J. Nucl. Med. Biol. 2019, 7, 129–140. [Google Scholar] [CrossRef]
- Spolverato, G.; Vitale, A.; Ejaz, A.; Kim, Y.; Cosgrove, D.; Schlacter, T.; Geschwind, J.F.; Pawlik, T.M. Net health benefit of hepatic resection versus intraarterial therapies for neuroendocrine liver metastases: A Markov decision model. Surgery 2015, 158, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Clift, A.K.; Kidd, M.; Bodei, L.; Toumpanakis, C.; Baum, R.P.; Oberg, K.; Modlin, I.M.; Frilling, A. Neuroendocrine Neoplasms of the Small Bowel and Pancreas. Neuroendocrinology 2020, 110, 444–476. [Google Scholar] [CrossRef]
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [Green Version]
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Delle Fave, G.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef]
- Sundin, A.; Arnold, R.; Baudin, E.; Cwikla, J.B.; Eriksson, B.; Fanti, S.; Fazio, N.; Giammarile, F.; Hicks, R.J.; Kjaer, A.; et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology 2017, 105, 212–244. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Lee, L.; Jensen, R.T. Carcinoid-syndrome: Recent advances, current status and controversies. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Grande, E.; Diaz, A.; Lopez, C.; Munarriz, J.; Reina, J.J.; Vera, R.; Bernardez, B.; Aller, J.; Capdevila, J.; Garcia-Carbonero, R.; et al. Economics of gastroenteropancreatic neuroendocrine tumors: A systematic review. Adv. Endocrinol. Metab. 2019, 10, 2042018819828217. [Google Scholar] [CrossRef]
- Rindi, G.; Inzani, F. Neuroendocrine neoplasm update: Toward universal nomenclature. Endocr. Relat. Cancer 2020, 27, R211–R218. [Google Scholar] [CrossRef] [PubMed]
- Pearman, T.P.; Beaumont, J.L.; Cella, D.; Neary, M.P.; Yao, J. Health-related quality of life in patients with neuroendocrine tumors: An investigation of treatment type, disease status, and symptom burden. Support. Care Cancer 2016, 24, 3695–3703. [Google Scholar] [CrossRef]
- Bhargava, P.; He, G.; Samarghandi, A.; Delpassand, E.S. Pictorial review of SPECT/CT imaging applications in clinical nuclear medicine. Am. J. Nucl. Med. Mol. Imaging 2012, 2, 221–231. [Google Scholar] [PubMed]
- Chowdhury, F.U.; Scarsbrook, A.F. The role of hybrid SPECT-CT in oncology: Current and emerging clinical applications. Clin. Radiol. 2008, 63, 241–251. [Google Scholar] [CrossRef]
- Klausen, T.L.; Mortensen, J.; de Nijs, R.; Andersen, F.L.; Hojgaard, L.; Beyer, T.; Holm, S. Intravenous contrast-enhanced CT can be used for CT-based attenuation correction in clinical (111)In-octreotide SPECT/CT. Ejnmmi Phys. 2015, 2, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuclear Medicine. Available online: https://www.nibib.nih.gov/science-education/science-topics/nuclear-medicine (accessed on 11 February 2021).
- Hoyer, D.; Bell, G.I.; Berelowitz, M.; Epelbaum, J.; Feniuk, W.; Humphrey, P.P.; O’Carroll, A.M.; Patel, Y.C.; Schonbrunn, A.; Taylor, J.E.; et al. Classification and nomenclature of somatostatin receptors. Trends Pharm. Sci. 1995, 16, 86–88. [Google Scholar] [CrossRef]
- Xu, J.; Li, Y.; Xu, X.; Zhang, J.; Zhang, Y.; Yu, X.; Huang, D. Clinical application of (99m)Tc-HYNIC-TOC SPECT/CT in diagnosing and monitoring of pancreatic neuroendocrine neoplasms. Ann. Nucl. Med. 2018, 32, 446–452. [Google Scholar] [CrossRef]
- Johnbeck, C.B.; Knigge, U.; Loft, A.; Berthelsen, A.K.; Mortensen, J.; Oturai, P.; Langer, S.W.; Elema, D.R.; Kjaer, A. Head-to-Head Comparison of (64)Cu-DOTATATE and (68)Ga-DOTATOC PET/CT: A Prospective Study of 59 Patients with Neuroendocrine Tumors. J. Nucl. Med. 2017, 58, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Pollard, J.; McNeely, P.; Menda, Y. Nuclear Imaging of Neuroendocrine Tumors. Surg. Oncol. Clin. N. Am. 2020, 29, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177)Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Krausz, Y.; Freedman, N.; Rubinstein, R.; Lavie, E.; Orevi, M.; Tshori, S.; Salmon, A.; Glaser, B.; Chisin, R.; Mishani, E.; et al. 68Ga-DOTA-NOC PET/CT imaging of neuroendocrine tumors: Comparison with (1)(1)(1)In-DTPA-octreotide (OctreoScan(R)). Mol. Imaging Biol. 2011, 13, 583–593. [Google Scholar] [CrossRef] [PubMed]
- Morgat, C.; Velayoudom-Cephise, F.L.; Schwartz, P.; Guyot, M.; Gaye, D.; Vimont, D.; Schulz, J.; Mazere, J.; Nunes, M.L.; Smith, D.; et al. Evaluation of (68)Ga-DOTA-TOC PET/CT for the detection of duodenopancreatic neuroendocrine tumors in patients with MEN1. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1258–1266. [Google Scholar] [CrossRef]
- Kowalski, J.; Henze, M.; Schuhmacher, J.; Macke, H.R.; Hofmann, M.; Haberkorn, U. Evaluation of positron emission tomography imaging using [68Ga]-DOTA-D Phe(1)-Tyr(3)-Octreotide in comparison to [111In]-DTPAOC SPECT. First results in patients with neuroendocrine tumors. Mol. Imaging Biol. 2003, 5, 42–48. [Google Scholar] [CrossRef]
- Tolomeo, A.; Lopopolo, G.; Dimiccoli, V.; Perioli, L.; Modoni, S.; Scilimati, A. Impact of 68Ga-DOTATOC PET/CT in comparison to 111In-Octreotide SPECT/CT in management of neuro-endocrine tumors: A case report. Medicine 2020, 99, e19162. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Paeng, J.C.; Lee, S.J.; Shin, C.S.; Jang, J.Y.; Cheon, G.J.; Lee, D.S.; Chung, J.K.; Kang, K.W. Comparison of Diagnostic Sensitivity and Quantitative Indices Between (68)Ga-DOTATOC PET/CT and (111)In-Pentetreotide SPECT/CT in Neuroendocrine Tumors: A Preliminary Report. Nucl. Med. Mol. Imaging 2015, 49, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Sanders, G.D.; Neumann, P.J.; Basu, A.; Brock, D.W.; Feeny, D.; Krahn, M.; Kuntz, K.M.; Meltzer, D.O.; Owens, D.K.; Prosser, L.A.; et al. Recommendations for Conduct, Methodological Practices, and Reporting of Cost-effectiveness Analyses: Second Panel on Cost-Effectiveness in Health and Medicine. JAMA 2016, 316, 1093–1103. [Google Scholar] [CrossRef]
- Chua, A.; Perrin, A.; Ricci, J.F.; Neary, M.P.; Thabane, M. Cost-effectiveness of everolimus for the treatment of advanced neuroendocrine tumours of gastrointestinal or lung origin in Canada. Curr. Oncol. 2018, 25, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef]
- Casciano, R.; Chulikavit, M.; Perrin, A.; Liu, Z.; Wang, X.; Garrison, L.P. Cost-effectiveness of everolimus vs sunitinib in treating patients with advanced, progressive pancreatic neuroendocrine tumors in the United States. J. Med. Econ. 2012, 15 (Suppl. 1), 55–64. [Google Scholar] [CrossRef]
- Teunissen, J.J.; Kwekkeboom, D.J.; Krenning, E.P. Quality of life in patients with gastroenteropancreatic tumors treated with [177Lu-DOTA0,Tyr3]octreotate. J. Clin. Oncol. 2004, 22, 2724–2729. [Google Scholar] [CrossRef]
- Korse, C.M.; Taal, B.G.; van Velthuysen, M.L.; Visser, O. Incidence and survival of neuroendocrine tumours in The Netherlands according to histological grade: Experience of two decades of cancer registry. Eur. J. Cancer 2013, 49, 1975–1983. [Google Scholar] [CrossRef]
- Keizer, A.; Korse, C.M.; Meijer, F.J. The effect of delay in diagnosis in patients with neuroendocrine tumors. Int. J. Endocr. Oncol. 2016, 3, 33–39. [Google Scholar] [CrossRef]
- Low, S.K.; Giannis, D.; Bahaie, N.S.; Trong, B.L.H.; Moris, D.; Huy, N.T. Competing Mortality in Patients with Neuroendocrine Tumors. Am. J. Clin. Oncol. 2019, 42, 668–674. [Google Scholar] [CrossRef]
- Ter-Minassian, M.; Chan, J.A.; Hooshmand, S.M.; Brais, L.K.; Daskalova, A.; Heafield, R.; Buchanan, L.; Qian, Z.R.; Fuchs, C.S.; Lin, X.; et al. Clinical presentation, recurrence, and survival in patients with neuroendocrine tumors: Results from a prospective institutional database. Endocr. Relat. Cancer 2013, 20, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMJ 2013, 346, f1049. [Google Scholar] [CrossRef] [Green Version]
- Woods, B.; Revill, P.; Sculpher, M.; Claxton, K. Country-Level Cost-Effectiveness Thresholds: Initial Estimates and the Need for Further Research. Value Health 2016, 19, 929–935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, W.; van Baal, P.; van Exel, J.; Versteegh, M. When is it too expensive? Cost-effectiveness thresholds and health care decision-making. Eur. J. Health Econ. 2019, 20, 175–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, I.; McIver, S.; Moore, D.; Bryan, S. The use of economic evaluations in NHS decision-making: A review and empirical investigation. Health Technol. Assess. 2008, 12, 1–175. [Google Scholar] [CrossRef]
- Hall Dykgraaf, S.; Barnard, A. The role of cost-effectiveness analyses in investment decision making by primary health networks. Med. J. Aust. 2020, 213, 72–73. [Google Scholar] [CrossRef]
- Scholte, M.; Barentsz, J.O.; Sedelaar, J.P.M.; Gotthardt, M.; Grutters, J.P.C.; Rovers, M.M. Modelling Study with an Interactive Model Assessing the Cost-effectiveness of (68)Ga Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography and Nano Magnetic Resonance Imaging for the Detection of Pelvic Lymph Node Metastases in Patients with Primary Prostate Cancer. Eur. Urol. Focus 2020, 6, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Peng, L.; Tan, C.; Wang, Y. Cost-effectiveness analysis of positron-emission tomography-computed tomography in preoperative staging for nonsmall-cell lung cancer with resected monometastatic disease. Medicine 2019, 98, e16843. [Google Scholar] [CrossRef]
- Schreiter, N.F.; Brenner, W.; Nogami, M.; Buchert, R.; Huppertz, A.; Pape, U.F.; Prasad, V.; Hamm, B.; Maurer, M.H. Cost comparison of 111In-DTPA-octreotide scintigraphy and 68Ga-DOTATOC PET/CT for staging enteropancreatic neuroendocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Segard, T.; Morandeau, L.M.; Geelhoed, E.A.; Francis, R.J. (68) Ga-somatostatin analogue PET-CT: Analysis of costs and benefits in a public hospital setting. J. Med. Imaging Radiat. Oncol. 2018, 62, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Verde, F.; Galatola, R.; Romeo, V.; Perillo, T.; Liuzzi, R.; Camera, L.; Klain, M.; Modica, R.; Faggiano, A.; Napolitano, V.; et al. Pancreatic Neuroendocrine Tumors in patients with Multiple Endocrine Neoplasia Type 1: Diagnostic Value of Different MRI Sequences. Neuroendocrinology 2020. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Estimate | Distribution | Source |
|---|---|---|---|
| Pre-test probability of NET | 5% | β | Dasari et al. 2017 [29] |
| Expected age at diagnosis | 30 | Dasari et al. 2017 [29] | |
| Assumed WTP/ QALY | $100,000.00 | Sanders et al. 2016 [27] | |
| Discount rate | 3.00% | Sanders et al. 2016 [27] | |
| Diagnostic test performances | |||
| CT sensitivity | 77% | β | Sundin et al. 2017 [8] |
| CT specificity | 86% | β | Sundin et al. 2017 [8] |
| SPECT/CT sensitivity | 70% | β | Sundin et al. 2017 [8] |
| SPECT/CT specificity | 96% | β | Sundin et al. 2017 [8] |
| PET-CT sensitivity | 91% | β | Sundin et al. 2017 [8] |
| PET-CT specificity | 92% | β | Sundin et al. 2017 [8] |
| Costs (Acute) | |||
| CT | $787 | γ | Medicare (74,177 + 71,260 + 70,491) |
| PET/CT | $1375.00 | γ | Medicare (78814) |
| SPECT/CT | $1242.00 | γ | Medicare (78,803 + 74,177 + 71,260 + 70,491) |
| Biopsy | $1375.00 | γ | Medicare (48,102) |
| Timely surgery + treatment (true positive) | $85,068.00 | γ | Medicare/Expert opinion |
| Delayed surgery + treatment (false negative) | $127,602.00 | γ | Medicare/Expert opinion |
| Unnecessary biopsy (false positive) | $1375.00 | γ | Medicare (36,246) |
| No further action required (true negative) | $0.00 | γ | Assumption |
| Costs (long term) | |||
| Yearly costs without relevant tumor burden | $0.00 | γ | Assumption |
| Yearly costs with/after treated NET | $2107.00 | γ | Spolverato et al. 2015 [4] |
| Yearly costs with/after treated NET (clinically relevant) | $61,375.00 | γ | Spolverato et al. 2015 [4] |
| Utilities | |||
| Health state utility values of NET patients without relevant tumor burden | 1 | β | Assumption |
| Health state utility values of NET patients (no clinically relevant tumor burden) | 0.779 | β | Chua et al. 2018 [28] |
| Health state utility values of NET patients (clinically relevant tumor burden) | 0.768 | β | Casciano et al. 2012 [30] |
| Health state utility values of NET patients with disease progression | 0.612 | β | Casciano et al. 2012 [30] |
| Health state utility values of NET patients without treatment | 0.690 | β | Teunissen et al. 2004 [31] |
| Death | 0 | Assumption | |
| Transition probabilities | |||
| Risk of death with timely treatment | 4.00% | β | Korse et al. 2013 [32] |
| Risk of death with delayed treatment | 4.50% | β | Keizer et al. 2016 [33] |
| Risk of death with no treatment | 12.12% | β | Man et al. 2018 [2] |
| Risk of death for a competitive cause | 2.50% | β | Low et al. 2019 [34] |
| Risk of disease progression/recurrence | 8.80% | β | Ter-Minassian et al.2013 [35] |
| Risk of death for other reason | Life Table x relative Risk | β | US Life Table |
| Clinical rel w/o treatment to clin rel with treatment | 1 | β | Assumption |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Froelich, M.F.; Schnitzer, M.L.; Holzgreve, A.; Gassert, F.G.; Gresser, E.; Overhoff, D.; Schwarze, V.; Fabritius, M.P.; Nörenberg, D.; von Münchhausen, N.; et al. Cost-Effectiveness Analysis of 68Ga DOTA-TATE PET/CT, 111In-Pentetreotide SPECT/CT and CT for Diagnostic Workup of Neuroendocrine Tumors. Diagnostics 2021, 11, 334. https://doi.org/10.3390/diagnostics11020334
Froelich MF, Schnitzer ML, Holzgreve A, Gassert FG, Gresser E, Overhoff D, Schwarze V, Fabritius MP, Nörenberg D, von Münchhausen N, et al. Cost-Effectiveness Analysis of 68Ga DOTA-TATE PET/CT, 111In-Pentetreotide SPECT/CT and CT for Diagnostic Workup of Neuroendocrine Tumors. Diagnostics. 2021; 11(2):334. https://doi.org/10.3390/diagnostics11020334
Chicago/Turabian StyleFroelich, Matthias Frank, Moritz Ludwig Schnitzer, Adrien Holzgreve, Felix Gerhard Gassert, Eva Gresser, Daniel Overhoff, Vincent Schwarze, Matthias Philipp Fabritius, Dominik Nörenberg, Niklas von Münchhausen, and et al. 2021. "Cost-Effectiveness Analysis of 68Ga DOTA-TATE PET/CT, 111In-Pentetreotide SPECT/CT and CT for Diagnostic Workup of Neuroendocrine Tumors" Diagnostics 11, no. 2: 334. https://doi.org/10.3390/diagnostics11020334