
Cerebral [18F]-FDOPA Uptake in Autism Spectrum Disorder and Its Association with Autistic Traits

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Autism Spectrum Quotient
2.3. MRI and PET/CT Acquisition and Processing
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. ROI Analyses
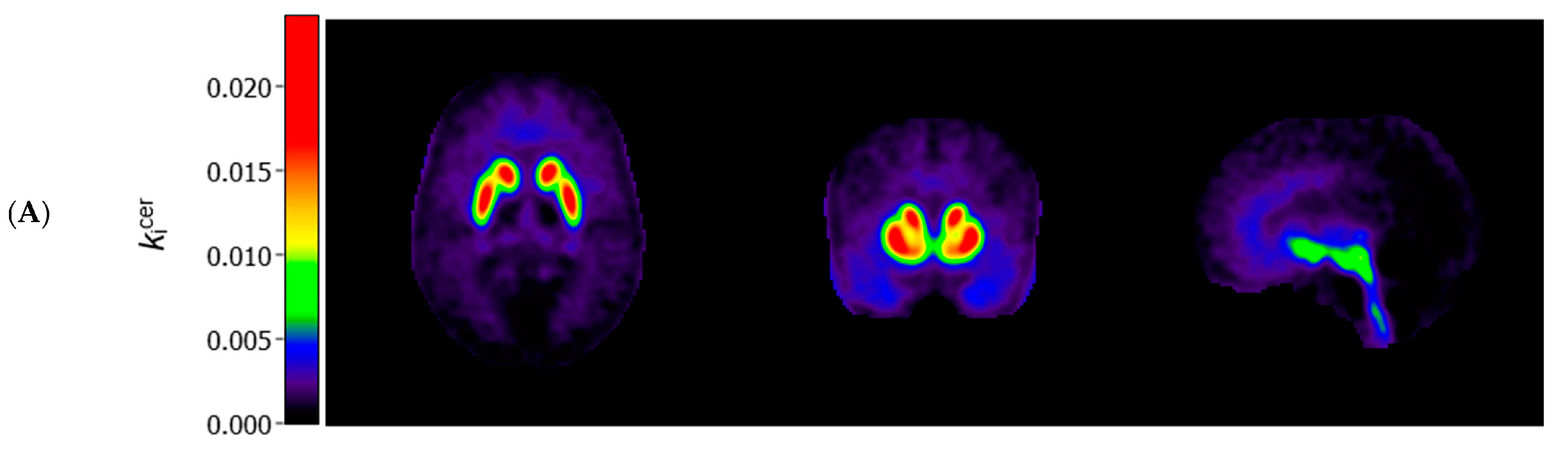
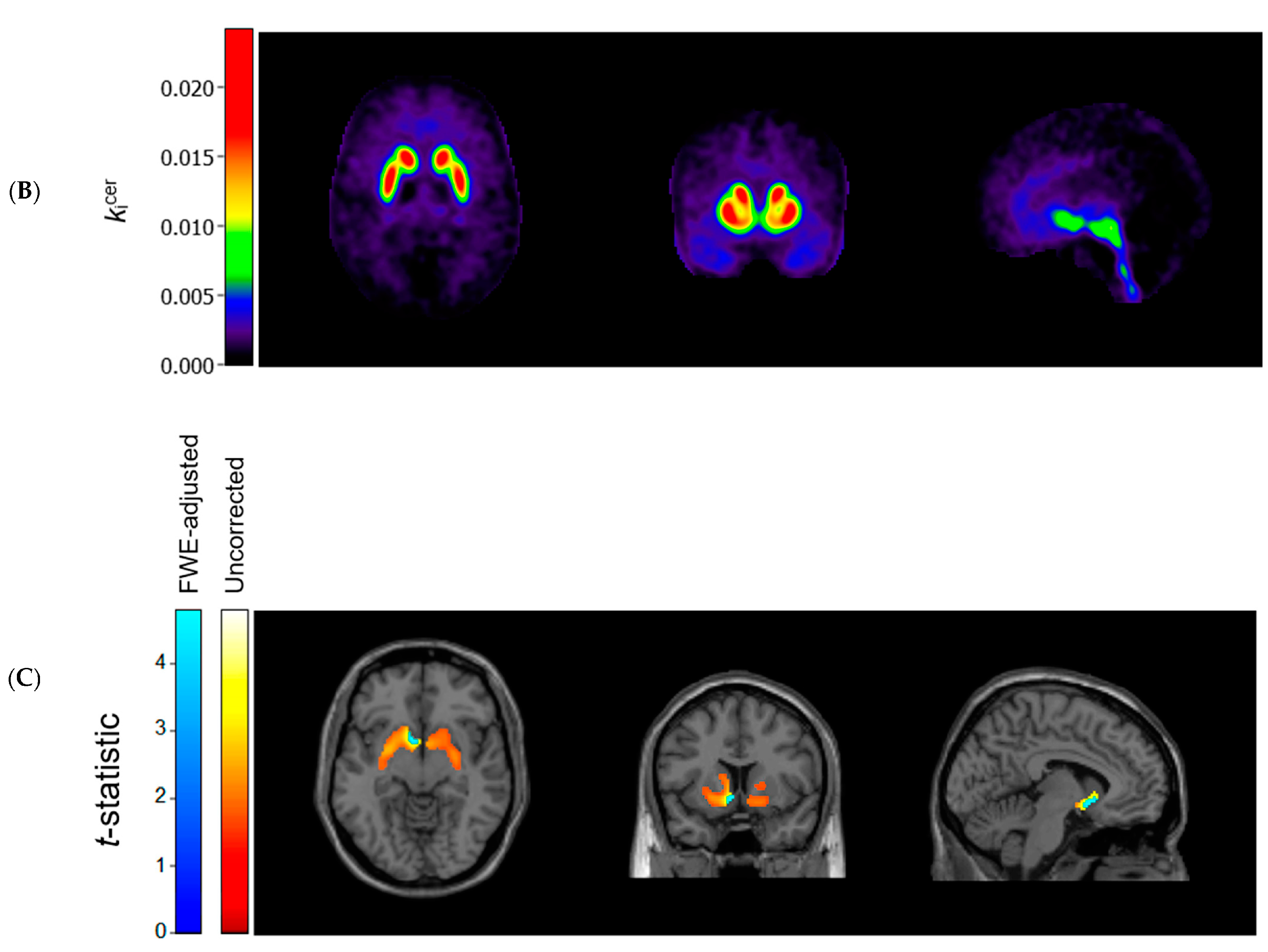
3.3. Voxel-Based Comparisons
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.D.; Taylor, M.; Roberts, A.D.; Oakes, T.R.; Schueller, M.; Holden, J.E.; Malischke, L.; DeJesus, O.T.; Nickles, R.J. FluoroDOPA PET shows the nondopaminergic as well as dopaminergic destinations of levodopa. Neurology 1999, 53, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Cauda, F.; Geda, E.; Sacco, K.; D’Agata, F.; Duca, S.; Geminiani, G.; Keller, R. Grey matter abnormality in autism spectrum disorder: An activation likelihood estimation meta-analysis study. J. Neurol. Neurosurg. Psychiatry 2011, 82, 1304–1313. [Google Scholar] [CrossRef] [PubMed]
- Cools, R.; D’Esposito, M. Inverted-U–shaped dopamine actions on human working memory and cognitive control. Biol. Psychiatry 2011, 69, e113–e125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damasio, A.R.; Maurer, R.G. A neurological model for childhood autism. Arch. Neurol. 1978, 35, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Egerton, A.; Demjaha, A.; McGuire, P.; Mehta, M.A.; Howes, O.D. The test–retest reliability of 18F-DOPA PET in assessing striatal and extrastriatal presynaptic dopaminergic function. Neuroimage 2010, 50, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Ernst, M.; Zametkin, A.; Matochik, J.; Pascualvaca, D.; Cohen, R. Low medial prefrontal dopaminergic activity in autistic children. Lancet 1997, 350, 638. [Google Scholar] [CrossRef]
- Fuccillo, M.V. Striatal circuits as a common node for autism pathophysiology. Front. Neurosci. 2016, 10, 27. [Google Scholar] [CrossRef] [Green Version]
- Hammers, A.; Allom, R.; Koepp, M.J.; Free, S.L.; Myers, R.; Lemieux, L.; Mitchell, T.N.; Brooks, D.J.; Duncan, J.S. Three-dimensional maximum probability atlas of the human brain, with particular reference to the temporal lobe. Hum. Brain Mapp. 2003, 19, 224–247. [Google Scholar] [CrossRef]
- Hoekstra, R.A.; Bartels, M.; Cath, D.C.; Boomsma, D.I. Factor structure, reliability and criterion validity of the Autism-Spectrum Quotient (AQ): A study in Dutch population and patient groups. J. Autism Dev. Disord. 2008, 38, 1555–1566. [Google Scholar] [CrossRef] [Green Version]
- Hus, V.; Lord, C. The autism diagnostic observation schedule, module 4: Revised algorithm and standardized severity scores. J. Autism Dev. Disord. 2014, 44, 1996–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JASP Team. JASP (Version 0.16); University of Amsterdam: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Kapur, S.; Mizrahi, R.; Li, M. From dopamine to salience to psychosis—Linking biology, pharmacology and phenomenology of psychosis. Schizophr. Res. 2005, 79, 59–68. [Google Scholar] [CrossRef]
- Kubota, M.; Fujino, J.; Tei, S.; Takahata, K.; Matsuoka, K.; Tagai, K.; Sano, Y.; Yamamoto, Y.; Shimada, H.; Takado, Y. Binding of Dopamine D1 receptor and noradrenaline transporter in individuals with autism spectrum disorder: A PET study. Cereb. Cortex 2020, 30, 6458–6468. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Lord, C.; Petkova, E.; Hus, V.; Gan, W.; Lu, F.; Martin, D.M.; Ousley, O.; Guy, L.; Bernier, R.; Gerdts, J. A multisite study of the clinical diagnosis of different autism spectrum disorders. Arch. Gen. Psychiatry 2012, 69, 306–313. [Google Scholar] [CrossRef]
- Moore, R.Y.; Whone, A.L.; McGowan, S.; Brooks, D.J. Monoamine neuron innervation of the normal human brain: An 18F-DOPA PET study. Brain Res. 2003, 982, 137–145. [Google Scholar] [CrossRef]
- Nieminen-von Wendt, T.S.; Metsähonkala, L.; Kulomäki, T.A.; Aalto, S.; Autti, T.H.; Vanhala, R.; Eskola, O.; Bergman, J.; Hietala, J.A.; von Wendt, L.O. Increased presynaptic dopamine function in Asperger syndrome. Neuroreport 2004, 15, 757–760. [Google Scholar] [CrossRef]
- Patlak, C.S.; Blasberg, R.G. Graphical evaluation of blood-to-brain transfer constants from multiple-time uptake data. Generalizations. J. Cereb. Blood Flow Metab. 1985, 5, 584–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavăl, D. A dopamine hypothesis of autism spectrum disorder. Dev. Neurosci. 2017, 39, 355–360. [Google Scholar] [CrossRef]
- Pavăl, D.; Micluția, I.V. The dopamine hypothesis of autism spectrum disorder revisited: Current status and future prospects. Dev. Neurosci. 2021, 43, 73–83. [Google Scholar] [CrossRef]
- Pavese, N.; Simpson, B.; Metta, V.; Ramlackhansingh, A.; Chaudhuri, K.R.; Brooks, D.J. [18F]FDOPA uptake in the raphe nuclei complex reflects serotonin transporter availability. A combined [18F]FDOPA and [11C]DASB PET study in Parkinson’s disease. Neuroimage 2012, 59, 1080–1084. [Google Scholar] [CrossRef]
- Quarantelli, M.; Berkouk, K.; Prinster, A.; Landeau, B.; Svarer, C.; Balkay, L.; Alfano, B.; Brunetti, A.; Baron, J.-C.; Salvatore, M. Integrated software for the analysis of brain PET/SPECT studies with partial-volume-effect correction. J. Nucl. Med. 2004, 45, 192–201. [Google Scholar]
- Radua, J.; Via, E.; Catani, M.; Mataix-Cols, D. Voxel-based meta-analysis of regional white-matter volume differences in autism spectrum disorder versus healthy controls. Psychol. Med. 2011, 41, 1539–1550. [Google Scholar] [CrossRef] [PubMed]
- Salgado, S.; Kaplitt, M.G. The nucleus accumbens: A comprehensive review. Stereotact. Funct. Neurosurg. 2015, 93, 75–93. [Google Scholar] [CrossRef]
- Schalbroeck, R.; van Velden, F.H.P.; de Geus-Oei, L.-F.; Yaqub, M.; van Amelsvoort, T.; Booij, J.; Selten, J.-P. Striatal dopamine synthesis capacity in autism spectrum disorder and its relation with social defeat: An [18F]-FDOPA PET/CT study. Transl. Psychiatry 2021, 11, 47. [Google Scholar] [CrossRef]
- Selten, J.-P.; Booij, J.; Buwalda, B.; Meyer-Lindenberg, A. Biological mechanisms whereby social exclusion may contribute to the etiology of psychosis: A narrative review. Schizophr. Bull. 2017, 43, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Svarer, C.; Madsen, K.; Hasselbalch, S.G.; Pinborg, L.H.; Haugbøl, S.; Frøkjær, V.G.; Holm, S.; Paulson, O.B.; Knudsen, G.M. MR-based automatic delineation of volumes of interest in human brain PET images using probability maps. Neuroimage 2005, 24, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Verwer, E.E.; Golla, S.; Kaalep, A.; Lubberink, M.; van Velden, F.; Bettinardi, V.; Yaqub, M.; Sera, T.; Rijnsdorp, S.; Lammertsma, A.A.; et al. Harmonisation of PET/CT contrast recovery performance for brain studies. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2856–2870. [Google Scholar] [CrossRef]
- Wong, A.Y.; Hsia, Y.; Chan, E.W.; Murphy, D.G.; Simonoff, E.; Buitelaar, J.K.; Wong, I.C. The variation of psychopharmacological prescription rates for people with autism spectrum disorder (ASD) in 30 countries. Autism Res. 2014, 7, 543–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zürcher, N.R.; Bhanot, A.; McDougle, C.J.; Hooker, J.M. A systematic review of molecular imaging (PET and SPECT) in autism spectrum disorder: Current state and future research opportunities. Neurosci. Biobehav. Rev. 2015, 52, 56–73. [Google Scholar] [CrossRef]
- Zürcher, N.R.; Walsh, E.C.; Phillips, R.D.; Cernasov, P.M.; Tseng, C.-E.J.; Dharanikota, A.; Smith, E.; Li, Z.; Kinard, J.L.; Bizzell, J.C. A simultaneous [11C]raclopride positron emission tomography and functional magnetic resonance imaging investigation of striatal dopamine binding in autism. Transl. Psychiatry 2021, 11, 33. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | ASD (n = 44) | Controls (n = 22) |
|---|---|---|
| Male, no. (%) | 28 (64%) | 14 (64%) |
| Age in years, mean (SD) | 23.74 (2.64) | 23.47 (2.48) |
| IQ, mean (SD) | 103.75 (5.19) | 105.05 (4.90) |
| Smoker, no. (%) | 2 (5%) | 1 (5%) |
| Scanned on Vereos PET/CT scanner, no. (%) | 31 (70%) | 13 (59%) |
| Approximate injected [18F]-FDOPA dose in MBq, mean (SD) | 161.55 (7.26) | 157.24 (8.57) |
| AQ total score, mean (SD) | 132.41 (20.05) | 91.73 (12.01) |
| AQ social interaction subscale, mean (SD) | 105.25 (17.65) | 71.27 (10.22) |
| AQ attention to detail subscale, mean (SD) | 27.16 (4.94) | 20.45 (4.19) |
| Association Between kicer Value and AQ Scores | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| kicer, Mean (SD) | ASD | Controls | Combined Sample | |||||||||
| ROI | ASD | Controls | p-value | Total | Social | Detail | Total | Social | Detail | Total | Social | Detail |
| Whole striatum | 0.0145 (0.0023) a | 0.0143 (0.0024) a | 0.87 a | β = −0.04, p = 0.81 | β = 0.04, p = 0.80 | β = −0.35, p = 0.04 | β = 0.08, p = 0.74 | β = 0.08, p = 0.74 | β = 0.03, p = 0.90 | β = 0.02, p = 0.87 | β = 0.06, p = 0.65 | β = −0.14, p = 0.28 |
| Putamen | 0.0157 (0.0025) | 0.0153 (0.0026) | 0.61 | β = 0.03, p = 0.86 | β = 0.12, p = 0.46 | β = −0.36, p = 0.04 | β = 0.10, p = 0.67 | β = 0.06, p = 0.80 | β = 0.13, p = 0.56 | β = 0.10, p = 0.43 | β = 0.14, p = 0.28 | β = −0.08, p = 0.52 |
| Nucleus accumbens | 0.0114 (0.0024) | 0.0108 (0.0024) | 0.38 | β = −0.09, p = 0.58 | β = 0.00, p = 0.99 | β = −0.43, p = 0.01 | β = 0.13, p = 0.59 | β = 0.14, p = 0.57 | β = 0.04, p = 0.85 | β = 0.09, p = 0.49 | β = 0.12, p = 0.33 | β = −0.10, p = 0.45 |
| Caudate nucleus | 0.0135 (0.0022) | 0.0137 (0.0025) | 0.69 | β = −0.12, p = 0.48 | β = −0.06, p = 0.72 | β = −0.29, p = 0.09 | β = 0.05, p = 0.84 | β = 0.10, p = 0.69 | β = −0.09, p = 0.72 | β = −0.09, p = 0.48 | β = −0.05, p = 0.66 | β = −0.19, p = 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schalbroeck, R.; de Geus-Oei, L.-F.; Selten, J.-P.; Yaqub, M.; Schrantee, A.; van Amelsvoort, T.; Booij, J.; van Velden, F.H.P. Cerebral [18F]-FDOPA Uptake in Autism Spectrum Disorder and Its Association with Autistic Traits. Diagnostics 2021, 11, 2404. https://doi.org/10.3390/diagnostics11122404
Schalbroeck R, de Geus-Oei L-F, Selten J-P, Yaqub M, Schrantee A, van Amelsvoort T, Booij J, van Velden FHP. Cerebral [18F]-FDOPA Uptake in Autism Spectrum Disorder and Its Association with Autistic Traits. Diagnostics. 2021; 11(12):2404. https://doi.org/10.3390/diagnostics11122404
Chicago/Turabian StyleSchalbroeck, Rik, Lioe-Fee de Geus-Oei, Jean-Paul Selten, Maqsood Yaqub, Anouk Schrantee, Therese van Amelsvoort, Jan Booij, and Floris H. P. van Velden. 2021. "Cerebral [18F]-FDOPA Uptake in Autism Spectrum Disorder and Its Association with Autistic Traits" Diagnostics 11, no. 12: 2404. https://doi.org/10.3390/diagnostics11122404