
BatchBMD as an Efficient and Accurate Dual-Energy X-ray Absorptiometry Report Generator

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
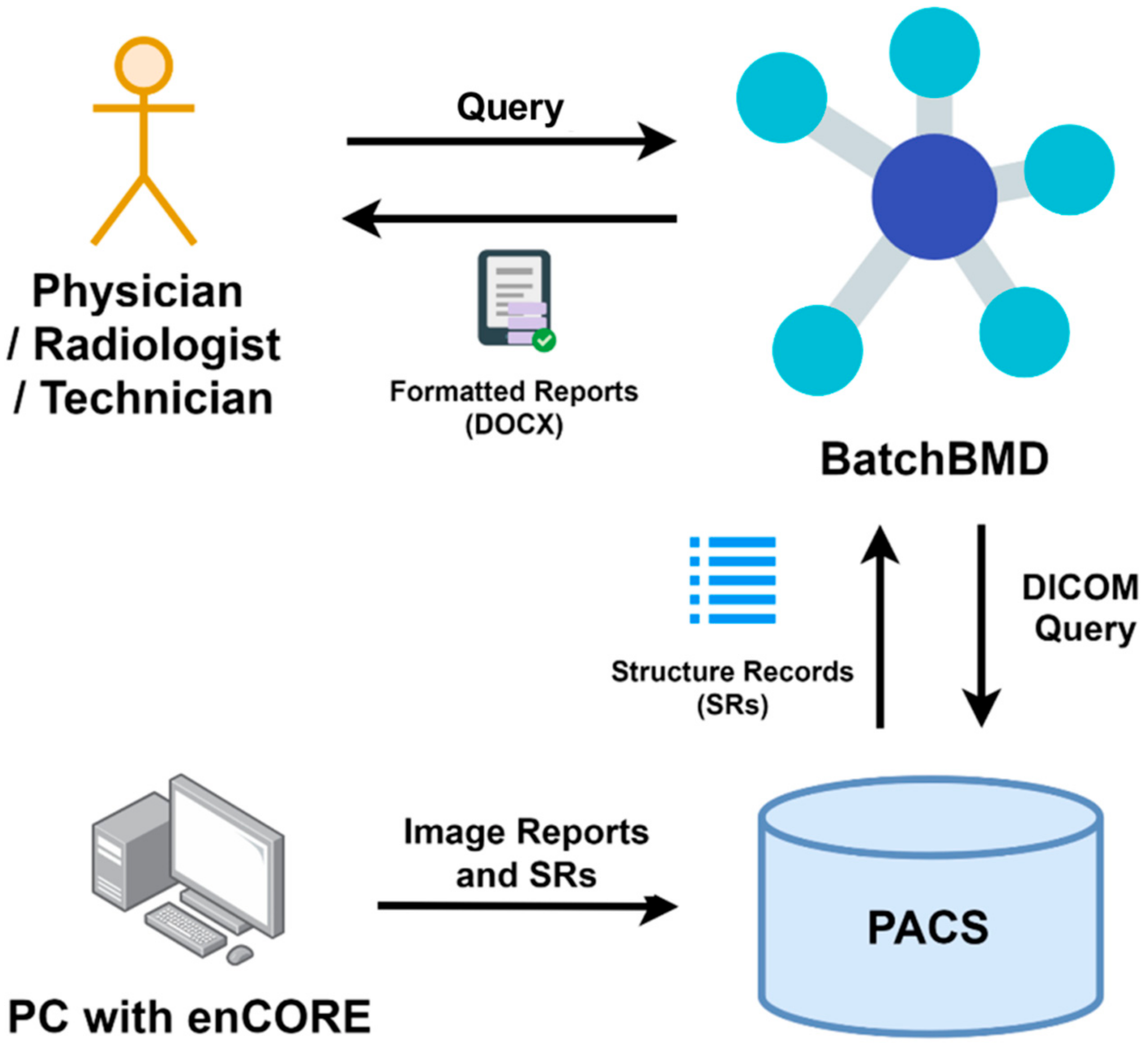
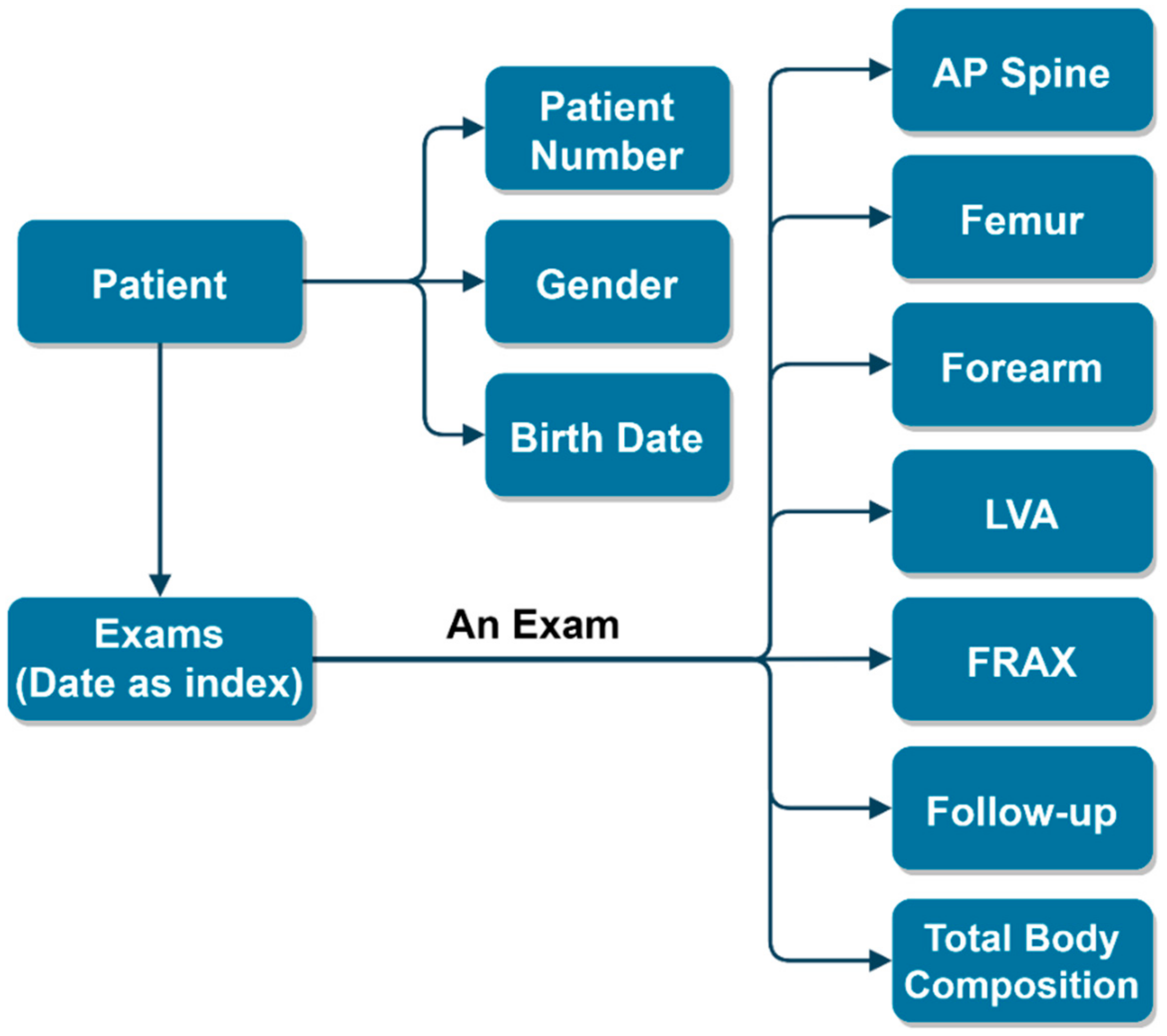
2.1. Software Design
2.2. Data Acquisition
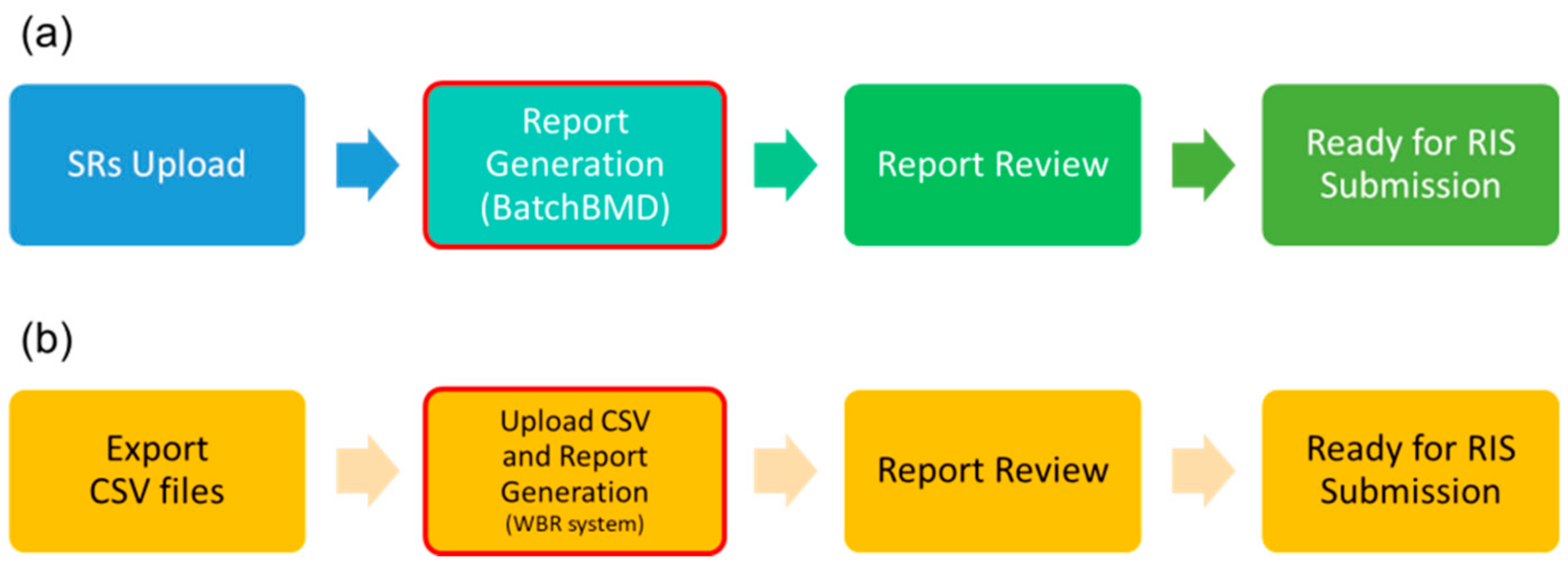
2.3. Software Evaluation
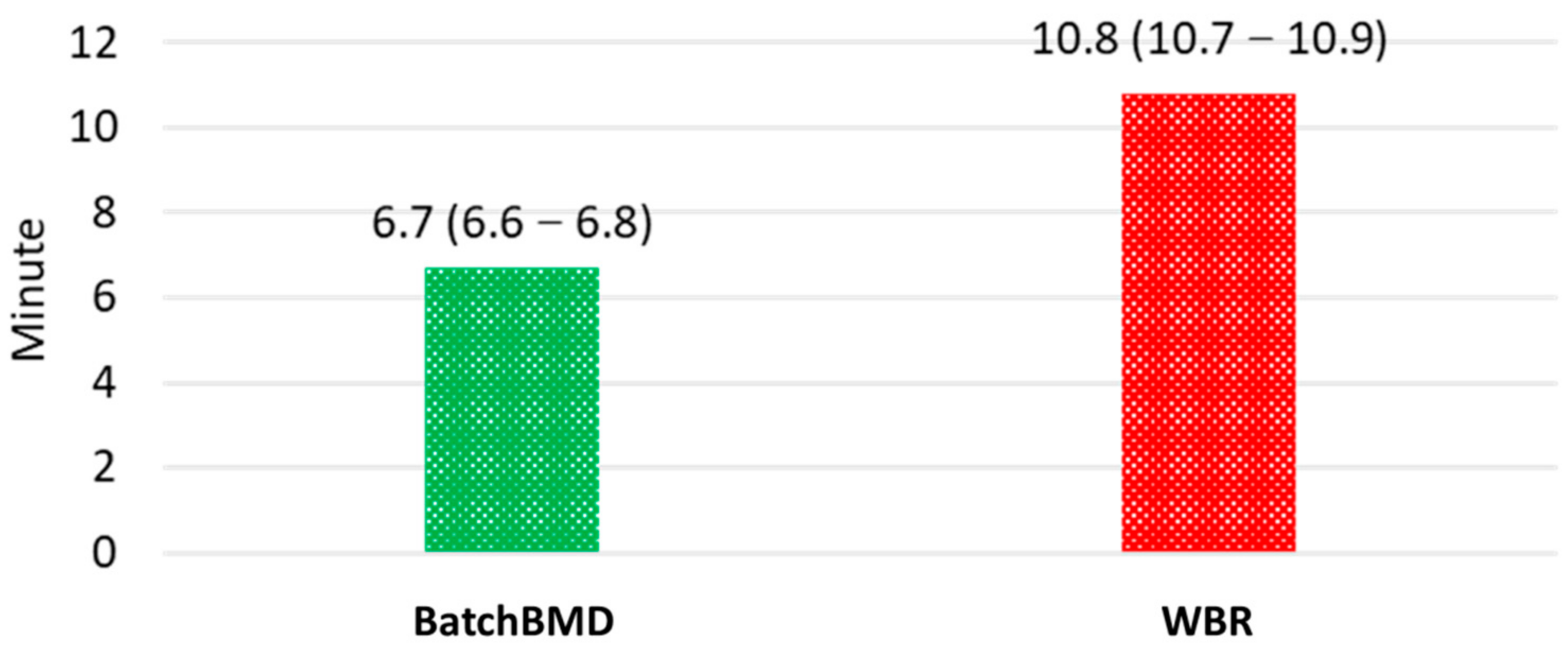
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMD | Bone Mineral Density |
| WBR | Web-based Reporting |
| DXA | Dual-energy X-ray Absorptiometry |
| ISCD | International Society for Clinical Densitometry |
| LVA | Lateral Vertebral Assessment |
| PACS | Picture Archiving and Communication System |
| DICOM | Digital Imaging and Communications in Medicine |
| SR | Structure Report |
| AP | Anteroposterior |
| FRAX | Fracture Risk Assessment Tool |
| RIS | Radiological Information System |
| ASMI | Appendicular Skeletal Muscle Index |
References
- Miller, P.D. The history of bone densitometry. Bone 2017, 104, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Dimai, H.P. Use of dual-energy X-ray absorptiometry (DXA) for diagnosis and fracture risk assessment; WHO-criteria, T- and Z-score, and reference databases. Bone 2017, 104, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.A.; Ng, B.K.; Sommer, M.J.; Heymsfield, S.B. Body composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.J.; Stewart, A.; Torgerson, D.J.; Reid, D.M. Population screening for osteoporosis risk: A randomised control trial of medication use and fracture risk. Osteoporos. Int. 2010, 21, 561–568. [Google Scholar] [CrossRef]
- Burge, R.; Dawson-Hughes, B.; Solomon, D.H.; Wong, J.B.; King, A.; Tosteson, A. Incidence and Economic Burden of Osteoporosis-Related Fractures in the United States, 2005–2025. J. Bone Miner. Res. 2007, 22, 465–475. [Google Scholar] [CrossRef]
- Kern, L.M.; Powe, N.R.; Levine, M.A.; Fitzpatrick, A.L.; Harris, T.B.; Robbins, J.; Fried, L.P. Association between Screening for Osteoporosis and the Incidence of Hip Fracture. Ann. Intern. Med. 2005, 142, 173–181. [Google Scholar] [CrossRef]
- Wang, L.; Yu, W.; Yin, X.; Cui, L.; Tang, S.; Jiang, N.; Cui, L.; Zhao, N.; Lin, Q.; Chen, L.; et al. Prevalence of Osteoporosis and Fracture in China: The China Osteoporosis Prevalence Study. JAMA Netw. Open 2021, 4, e2121106. [Google Scholar] [CrossRef]
- ISCD. Adult Official Positions. 2019. Available online: https://iscd.org/learn/official-positions/adult-positions/ (accessed on 22 August 2021).
- Tsai, I.T.; Tsai, M.-Y.; Wu, M.-T.; Chen, C.K.-H. Development of an Automated Bone Mineral Density Software Application: Facilitation Radiologic Reporting and Improvement of Accuracy. J. Digit. Imaging 2016, 29, 380–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachsmann, J.; Blain, K.; Thompson, M.; Cherian, S.; Oz, O.K.; Browning, T. Electronic Medical Record Integration for Streamlined DXA Reporting. J. Digit. Imaging 2018, 31, 159–166. [Google Scholar] [CrossRef] [Green Version]
- Morgan, S.L.; Prater, G.L. Quality in dual-energy X-ray absorptiometry scans. Bone 2017, 104, 13–28. [Google Scholar] [CrossRef]
- Promma, S.; Sritara, C.; Wipuchwongsakorn, S.; Chuamsaamarkkee, K.; Utamakul, C.; Chamroonrat, W.; Kositwattanarerk, A.; Anongpornjossakul, Y.; Thamnirat, K.; Ongphiphadhanakul, B. Errors in Patient Positioning for Bone Mineral Density Assessment by Dual X-Ray Absorptiometry: Effect of Technologist Retraining. J. Clin. Densitom. 2018, 21, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Messina, C.; Bandirali, M.; Sconfienza, L.M.; D’Alonzo, N.K.; Di Leo, G.; Papini, G.D.E.; Ulivieri, F.M.; Sardanelli, F. Prevalence and type of errors in dual-energy x-ray absorptiometry. Eur. Radiol. 2015, 25, 1504–1511. [Google Scholar] [CrossRef]
- Çetin, A.; Özgüçlü, E.; Özçakar, L.; Akıncı, A. Evaluation of the patient positioning during DXA measurements in daily clinical practice. Clin. Rheumatol. 2008, 27, 713–715. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.J.; Robbins, J.A.; Amarnath, A.L.D.; Franks, P. Osteoporosis Overtreatment in a Regional Health Care System. JAMA Intern. Med. 2016, 176, 391–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorasani, R. Can Health IT Tools Enable Improved Documentation of Quality, Safety Measures, and Regulatory Requirements in Radiology Reports? J. Am. Coll. Radiol. 2013, 10, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, H.-T.; Suh, J.-S. Quantitative Computed Tomography (QCT) as a Radiology Reporting Tool by Using Optical Character Recognition (OCR) and Macro Program. J. Digit. Imaging 2012, 25, 815–818. [Google Scholar] [CrossRef] [Green Version]
- Iv, M.; Patel, M.R.; Santos, A.; Kang, Y.S. Informatics in Radiology: Use of a Macro Scripting Editor to Facilitate Transfer of Dual-Energy X-ray Absorptiometry Reports into an Existing Departmental Voice Recognition Dictation System. RadioGraphics 2011, 31, 1181–1189. [Google Scholar] [CrossRef]
- Kanis, J.A.; WHO Study Group. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. Osteoporos. Int. 1994, 4, 368–381. [Google Scholar] [CrossRef]
- Martineau, P.; Morgan, S.L.; Leslie, W.D. Bone Mineral Densitometry Reporting: Pearls and Pitfalls. Can. Assoc. Radiol. J. 2021, 72, 490–504. [Google Scholar] [CrossRef] [Green Version]
- Baker, B.S.; Li, J.; Leary, E.V. DXA2: An Automated Program for Extraction of Dual-Energy X-Ray Absorptiometry Data. J. Clin. Densitom. 2021, 24, 658–662. [Google Scholar] [CrossRef]
- Abujudeh, H.H.; Govindan, S.; Narin, O.; Johnson, J.O.; Thrall, J.H.; Rosenthal, D.I. Automatically Inserted Technical Details Improve Radiology Report Accuracy. J. Am. Coll. Radiol. 2011, 8, 635–637. [Google Scholar] [CrossRef]
- Zimmerman, S.L.; Kim, W.; Boonn, W.W. Informatics in Radiology: Automated Structured Reporting of Imaging Findings Using the AIM Standard and XML. RadioGraphics 2011, 31, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Sobez, L.M.; Spiro, J.E.; Curta, A.; Ceelen, F.; Kampmann, E.; Goepfert, M.; Bodensohn, R.; Meinel, F.G.; Sommer, W.H.; et al. Structured reporting has the potential to reduce reporting times of dual-energy x-ray absorptiometry exams. BMC Musculoskelet Disord. 2020, 21, 248. [Google Scholar] [CrossRef] [PubMed]
- Krueger, D.; Shives, E.; Siglinsky, E.; Libber, J.; Buehring, B.; Hansen, K.E.; Binkley, N. DXA Errors Are Common and Reduced by Use of a Reporting Template. J. Clin. Densitom. 2019, 22, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Schoeppe, F.; Sommer, W.H.; Haack, M.; Havel, M.; Rheinwald, M.; Wechtenbruch, J.; Fischer, M.R.; Meinel, F.G.; Sabel, B.O.; Sommer, N.N. Structured reports of videofluoroscopic swallowing studies have the potential to improve overall report quality compared to free text reports. Eur. Radiol. 2018, 28, 308–315. [Google Scholar] [CrossRef]
- Schoeppe, F.; Sommer, W.H.; Nörenberg, D.; Verbeek, M.; Bogner, C.; Westphalen, C.B.; Dreyling, M.; Rummeny, E.J.; Fingerle, A.A. Structured reporting adds clinical value in primary CT staging of diffuse large B-cell lymphoma. Eur. Radiol. 2018, 28, 3702–3709. [Google Scholar] [CrossRef]
- Weiss, D.L.; Langlotz, C.P. Structured Reporting: Patient Care Enhancement or Productivity Nightmare? Radiology 2008, 249, 739–747. [Google Scholar] [CrossRef]
- Bosmans, J.M.L.; Peremans, L.; Menni, M.; De Schepper, A.M.; Duyck, P.O.; Parizel, P.M. Structured reporting: If, why, when, how—and at what expense? Results of a focus group meeting of radiology professionals from eight countries. Insights Imaging 2012, 3, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Kanis, J.A.; Oden, A.; Johansson, H.; Borgström, F.; Ström, O.; McCloskey, E. FRAX® and its applications to clinical practice. Bone 2009, 44, 734–743. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Auto-Filled Item Type (Number of Items) | Report Accuracy | |
|---|---|---|
| BatchBMD | WBR | |
| Patient profile (6) | 100.0% | 100.0% |
| Lumbar spine BMD info (4) | 100.0% | 99.8% |
| Femur BMD info (4) | 100.0% | 100.0% |
| Forearm BMD (2) | 100.0% | 100.0% |
| LVA, vertebral compression fractures (1) | 100.0% | 98.2% |
| Lowest T-score (1) | 100.0% | 99.8% |
| Densitometric assessment (1) | 100.0% | 98.2% |
| Fracture risk analysis (2) | 100.0% | N/A |
| BMD Follow-up (2) | 100.0% | N/A |
| Body composition (11) | 99.4% | 100.0% |
| Body composition assessment (7) | 100.0% | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, C.-H.; Huang, W.-C.; Lu, Y.-C.; Hsiao, H.-F.; Chan, W.P. BatchBMD as an Efficient and Accurate Dual-Energy X-ray Absorptiometry Report Generator. Diagnostics 2021, 11, 2403. https://doi.org/10.3390/diagnostics11122403
Chan C-H, Huang W-C, Lu Y-C, Hsiao H-F, Chan WP. BatchBMD as an Efficient and Accurate Dual-Energy X-ray Absorptiometry Report Generator. Diagnostics. 2021; 11(12):2403. https://doi.org/10.3390/diagnostics11122403
Chicago/Turabian StyleChan, Chun-Hsiang, Wen-Chi Huang, Yi-Chien Lu, Hsing-Fen Hsiao, and Wing P. Chan. 2021. "BatchBMD as an Efficient and Accurate Dual-Energy X-ray Absorptiometry Report Generator" Diagnostics 11, no. 12: 2403. https://doi.org/10.3390/diagnostics11122403