
The Patent Ductus Arteriosus in Adults with Special Focus on Role of CT

Abstract
:1. Introduction
2. Basic Embryology of PDA
3. Clinical Features of PDA
3.1. Small PDA
3.2. Moderate to Large PDA
4. Chest Radiographic and Echocardiographic Findings of PDA
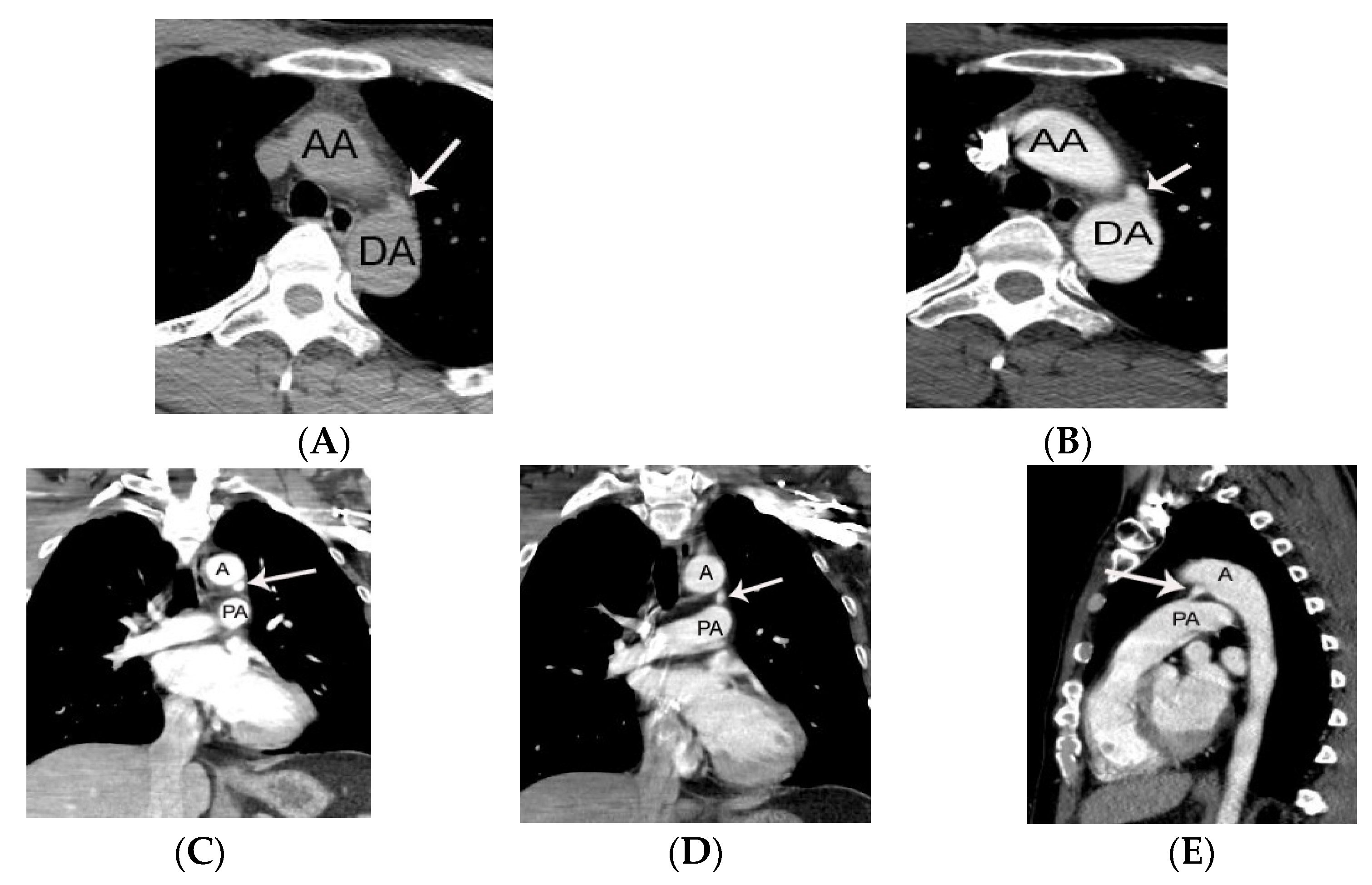
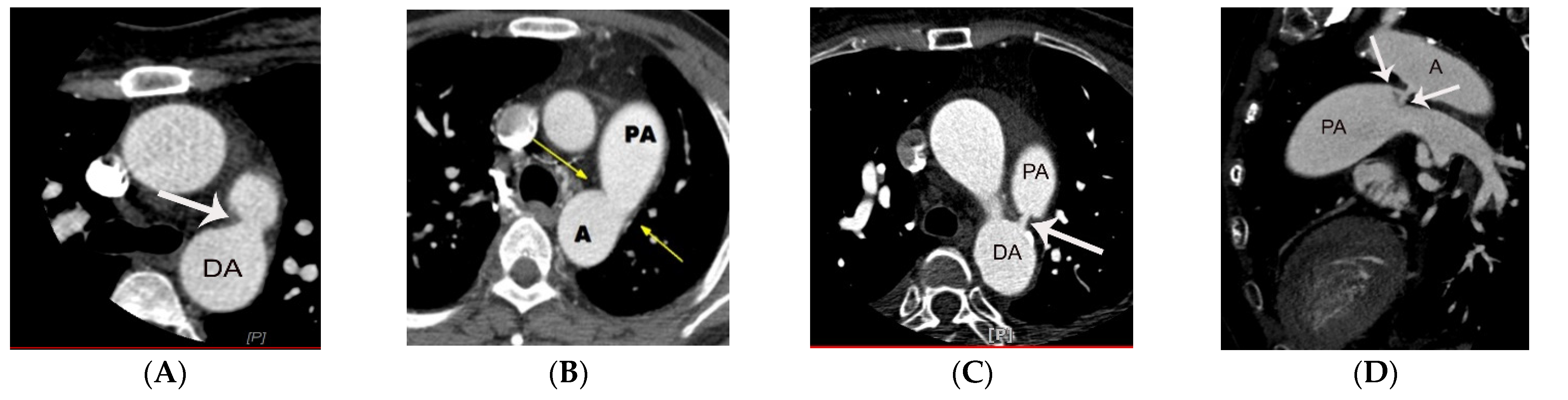
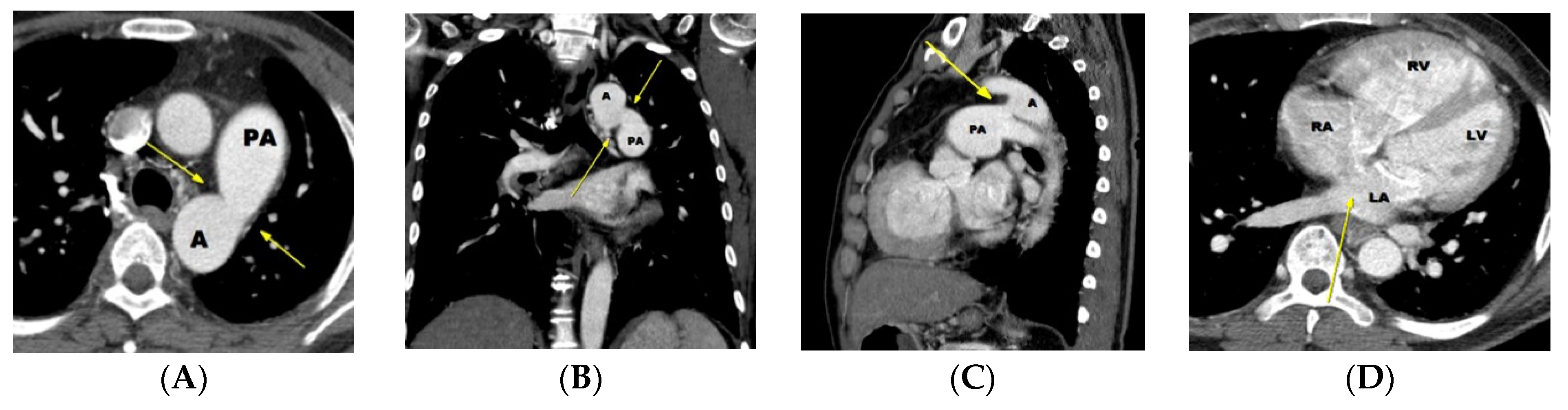
5. CT Anatomy of PDA
6. Potential Role of CT in the Diagnosis of PDA
6.1. Potential Role of CT in Moderate-to Large-Sized PDA
6.2. Potential Role of CT in Small PDAs
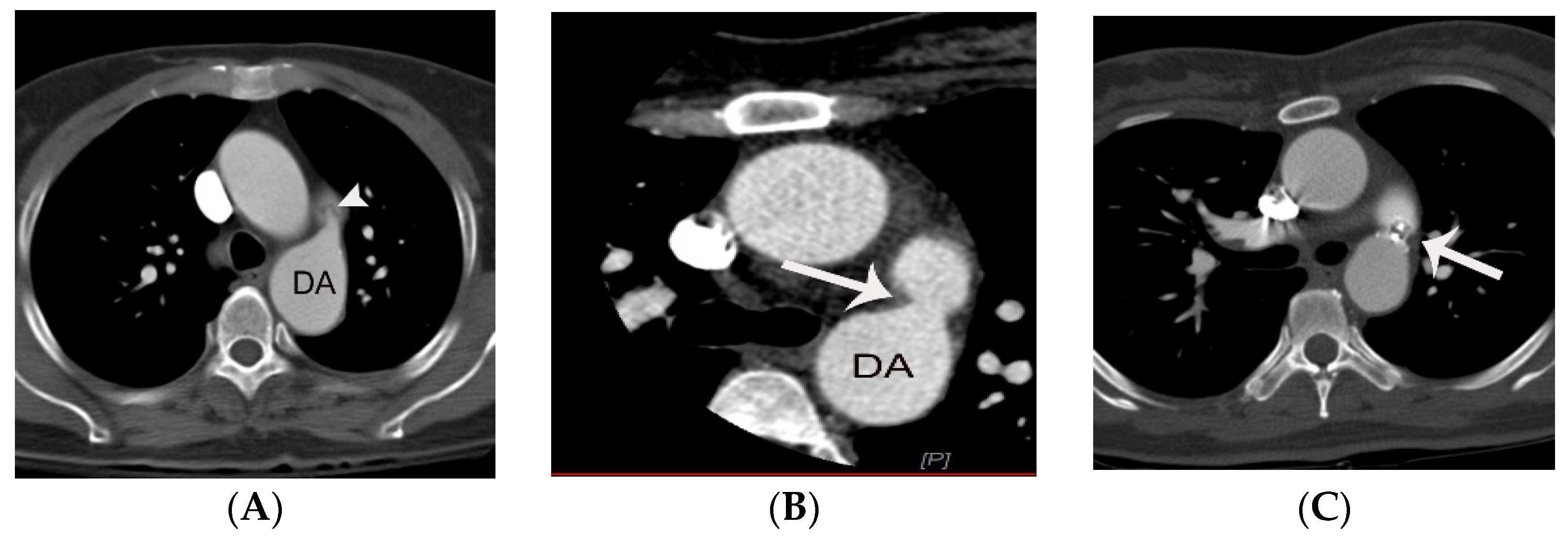
7. Diagnostic Pitfalls of PDA on Chest CT
8. Treatment of PDA; Surgery versus Intervention
8.1. Surgical Treatment
8.2. Transcatheter Closure of PDA
8.2.1. Ideal Device for Transcatheter Closure of PDA
8.2.2. Potential Use of CT Prior to Transcatheter Closure of PDA
8.2.3. Which Is the Best Option for Transcatheter Closure of PDA
8.2.4. Complications of Transcatheter Closure of PDA
8.2.5. Controversy of Transcatheter Closure in Patients with Small Silent PDA
8.2.6. Transcatheter Closure of PDA in Patients with Severe Pulmonary Hypertension
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schneider, D.J. The patent ductus arteriosus in term infants, children, and adults. Semin. Perinatol. 2012, 36, 146–153. [Google Scholar] [CrossRef]
- Krueger, M.; Cronin, P.; Sayyouh, M.; Kelly, A.M. Significant incidental cardiac disease on thoracic CT: What the general radiologist needs to know. Insights Imaging 2019, 10, 10. [Google Scholar] [CrossRef]
- Lloyd, T.R.; Beekman, R.H. Clinically silent patent ductus arteriosus. Am. Heart J. 1994, 127, 1664–1665. [Google Scholar] [CrossRef] [Green Version]
- Schneider, D.J.; Moore, J.W. Patent ductus arteriosus. Circulation 2006, 114, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Reddy, G.P.; Gotway, M.B.; Yeh, B.M.; Higgins, C.B. Cardiovascular shunts: MR imaging evaluation. Radiographics 2003, 23, S181–S194. [Google Scholar] [CrossRef]
- Morgan-Hughes, G.J.; Marshall, A.J.; Roobottom, C. Morphologic assessment of patent ductus arteriosus in adults using retrospectively ECG-gated multidetector CT. Am. J. Roentgenol. 2003, 181, 749–754. [Google Scholar] [CrossRef] [PubMed]
- Gournay, V. The ductus arteriosus: Physiology, regulation, and functional and congenital anomalies. Arch. Cardiovasc. Dis. 2011, 104, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Krichenko, A.; Benson, L.N.; Burrows, P.; Möes, C.A.; McLaughlin, P.; Freedom, R.M. Angiographic classification of the isolated, persistently patent ductus arteriosus and implications for percutaneous catheter occlusion. Am. J. Cardiol. 1989, 63, 877–880. [Google Scholar] [CrossRef]
- Lee, D.; Son, M.; Yoo, S.; Jung, S.; Chun, E.; White, C.S. High Rate of False Negative Diagnosis of Silent Patent Ductus Arteriosus on the Chest CT with 3 mm Slice-Thickness, Suggesting the Need for Analysis with Thinner Slice Thickness. Tomography 2021, 7, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Berko, N.S.; Haramati, L.B. Simple cardiac shunts in adults. Semin. Roentgenol. 2012, 47, 277–288. [Google Scholar] [CrossRef]
- Goitein, O.; Fuhrman, C.R.; Lacomis, J.M. Incidental finding on MDCT of patent ductus arteriosus: Use of CT and MRI to assess clinical importance. Am. J. Roentgenol. 2005, 184, 1924–1931. [Google Scholar] [CrossRef]
- P, S.; Jose, J.; George, O.K. Contemporary outcomes of percutaneous closure of patent ductus arteriosus in adolescents and adults. Indian Heart J. 2018, 70, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Son, M.J.; Chun, E.J.; Yoo, S.M.; Lee, H.Y.; Song, I.S.; White, C.S. High prevalence of a linear valve-like structure on CT at the pulmonary artery terminus of patent ductus arteriosus in adult patients, mimicking endarteritis. Surg. Radiol. Anat. 2021, 43, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Yoo, S.M.; Lee, H.Y.; White, C.S. Computed Tomography Diagnosis of Patent Ductus Arteriosus Endarteritis and Septic Pulmonary Embolism. Korean Circ. J. 2020, 50, 182–183. [Google Scholar] [CrossRef]
- Bilge, M.; Uner, A.; Ozeren, A.; Aydin, M.; Demirel, F.; Ermiş, B.; Ozkökeli, M. Pulmonary endarteritis and subsequent embolization to the lung as a complication of a patent ductus arteriosus--a case report. Angiology 2004, 55, 99–102. [Google Scholar] [CrossRef]
- Callegari, A.; Burkhardt, B.; Relly, C.; Knirsch, W.; Christmann, M. Ductus arteriosus-associated infective endarteritis: Lessons from the past, future perspective. Congenit. Heart Dis. 2019, 14, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Saucedo-Orozco, H.; Vargas-Barrón, J.; Vázquez-Antona, C.A.; Castillo-Castellón, F. Echocardiographic findings in patent ductus arteriosus-associated infective endarteritis. Anatol. J. Cardiol. 2021, 25, 774–780. [Google Scholar] [CrossRef]
- Onji, K.; Matsuura, W. Pulmonary endarteritis and subsequent pulmonary embolism associated with clinically silent patent ductus arteriosus. Intern. Med. 2007, 46, 1663–1667. [Google Scholar] [CrossRef] [Green Version]
- Latson, L.A.; McManus, B.M.; Doer, C.; Kilzer, K.; Cheatham, J.P. Endocarditis risk of the USCI PDA umbrella for transcatheter closure of patent ductus arteriosus. Circulation 1994, 90, 2525–2528. [Google Scholar] [CrossRef] [Green Version]
- Ghani, S.A.; Hashim, R. Surgical management of patent ductus arteriosus. A review of 413 cases. J. R. Coll. Surg. Edinb. 1989, 34, 33–36. [Google Scholar]
- Galal, O.; Nehgme, R.; Al-Fadley, F.; de Moor, M.; Abbag, F.I.; Al-Oufi, S.H.; Williams, E.; Fawzy, M.E.; Al-Halees, Z. The role of surgical ligation of patent ductus arteriosus in the era of the Rashkind device. Ann. Thorac. Surg. 1997, 63, 434–437. [Google Scholar] [CrossRef]
- Narin, N.; Pamukçu, Ö.; Baykan, A.; Argun, M.; Özyurt, A.; Bayram, A.; Üzüm, K. Transcatheter closure of PDA in premature babies less than 2 kg. Anatol. J. Cardiol. 2017, 17, 147–153. [Google Scholar] [PubMed] [Green Version]
- Fraisse, A.; Bautista-Rodriguez, C.; Burmester, M.; Lane, M.; Singh, Y. Transcatheter Closure of Patent Ductus Arteriosus in Infants With Weight Under 1,500 Grams. Front. Pediatr. 2020, 8, 558256. [Google Scholar] [CrossRef] [PubMed]
- Baruteau, A.E.; Hascoët, S.; Baruteau, J.; Boudjemline, Y.; Lambert, V.; Angel, C.Y.; Belli, E.; Petit, J.; Pass, R. Transcatheter closure of patent ductus arteriosus: Past, present and future. Arch. Cardiovasc. Dis. 2014, 107, 122–132. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, A.; Pandya, S.; Reddy, S.V.; Turner, D.R.; Du, W.; Navabi, M.A.; Mirzaaghayan, M.R.; Kiani, A.; Sloan, K.; Forbes, T.J. Trans-catheter closure of patent ductus arteriosus-What is the best device? Catheter. Cardiovasc. Interv. 2010, 76, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Cambier, P.A.; Kirby, W.C.; Wortham, D.C.; Moore, J.W. Percutaneous closure of the small (less than 2.5 mm) patent ductus arteriosus using coil embolization. Am. J. Cardiol. 1992, 69, 815–816. [Google Scholar] [CrossRef]
- Sankar, M.N.; Bhombal, S.; Benitz, W.E. PDA: To treat or not to treat. Congenit. Heart Dis. 2019, 14, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Khajali, Z.; Firouzi, A.; Ghaderian, H.; Aliramezany, M. Trans-catheter closure of large PDA in adult patients with Amplatzer device: Case series. Cardiol. Young 2021, 8, 1–4. [Google Scholar] [CrossRef]
- Lucas, V.S. Percutaneous PDA closure with Amplatzer AVP ll and ADO ll AS devices. Catheter. Cardiovasc. Interv. 2019, 93, E197. [Google Scholar] [CrossRef]
- Lehner, A.; Ulrich, S.; Happel, C.M.; Fischer, M.; Kantzis, M.; Schulze-Neick, I.; Haas, N.A. Closure of very large PDA with pulmonary hypertension: Initial clinical case-series with the new Occlutech PDA occluder. Catheter. Cardiovasc. Interv. 2017, 89, 718–725. [Google Scholar] [CrossRef]
- Glaus, T.M.; Martin, M.; Boller, M.; Johnson, M.S.; Kutter, A.; Flückiger, M.; Tofeig, M. Catheter closure of patent ductus arteriosus in dogs: Variation in ductal size requires different techniques. J. Vet. Cardiol. 2003, 5, 7–12. [Google Scholar] [CrossRef]
- Grifka, R.G. Transcatheter PDA closure: Equipment and technique. J. Interv. Cardiol. 2001, 14, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.C.; Rivera, B.K.; Cooper, J.N.; Smith, C.V.; Berman, D.P.; Slaughter, J.L.; Backes, C.H. Percutaneous closure of the patent uctus arteriosus: Opportunities moving forward. Congenit. Heart Dis. 2019, 14, 95–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masura, J.; Walsh, K.P.; Thanopoulous, B.; Chan, C.; Bass, J.; Goussous, Y.; Gavora, P.; Hijazi, Z.M. Catheter closure of moderate- to large-sized patent ductus arteriosus using the new Amplatzer duct occluder: Immediate and short-term results. J. Am. Coll. Cardiol. 1998, 31, 878–882. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, D.; Salem, M.M.; Forbes, T.J.; Gordon, B.M.; Soriano, B.D.; Dimas, V.; Goldstein, B.H.; Owada, C.; Javois, A.; Bass, J.; et al. Results of the combined U.S. multicenter postapproval study of the Nit-Occlud PDA device for percutaneous closure of patent ductus arteriosus. Catheter. Cardiovasc. Interv. 2019, 93, 645–651. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Echocardiography | CT | MRI | |
|---|---|---|---|
| Functional evaluation | ++ | − | + |
| Diagnosis of PDA with severe pulmonary hypertension | +/− | + | +/− |
| Diagnosis of silent PDA | + | + | − |
| Radiation hazard | − | + | − |
| Iodine hypersensitivity | − | + | − |
| PDA indicates patent ductus arteriosus | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.J.; Yoo, S.M.; Son, M.J.; White, C.S. The Patent Ductus Arteriosus in Adults with Special Focus on Role of CT. Diagnostics 2021, 11, 2394. https://doi.org/10.3390/diagnostics11122394
Lee SJ, Yoo SM, Son MJ, White CS. The Patent Ductus Arteriosus in Adults with Special Focus on Role of CT. Diagnostics. 2021; 11(12):2394. https://doi.org/10.3390/diagnostics11122394
Chicago/Turabian StyleLee, Soo Jeong, Seung Min Yoo, Min Ji Son, and Charles S. White. 2021. "The Patent Ductus Arteriosus in Adults with Special Focus on Role of CT" Diagnostics 11, no. 12: 2394. https://doi.org/10.3390/diagnostics11122394