
Cumulative Effective Dose from Medical Imaging in Inflammatory Bowel Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
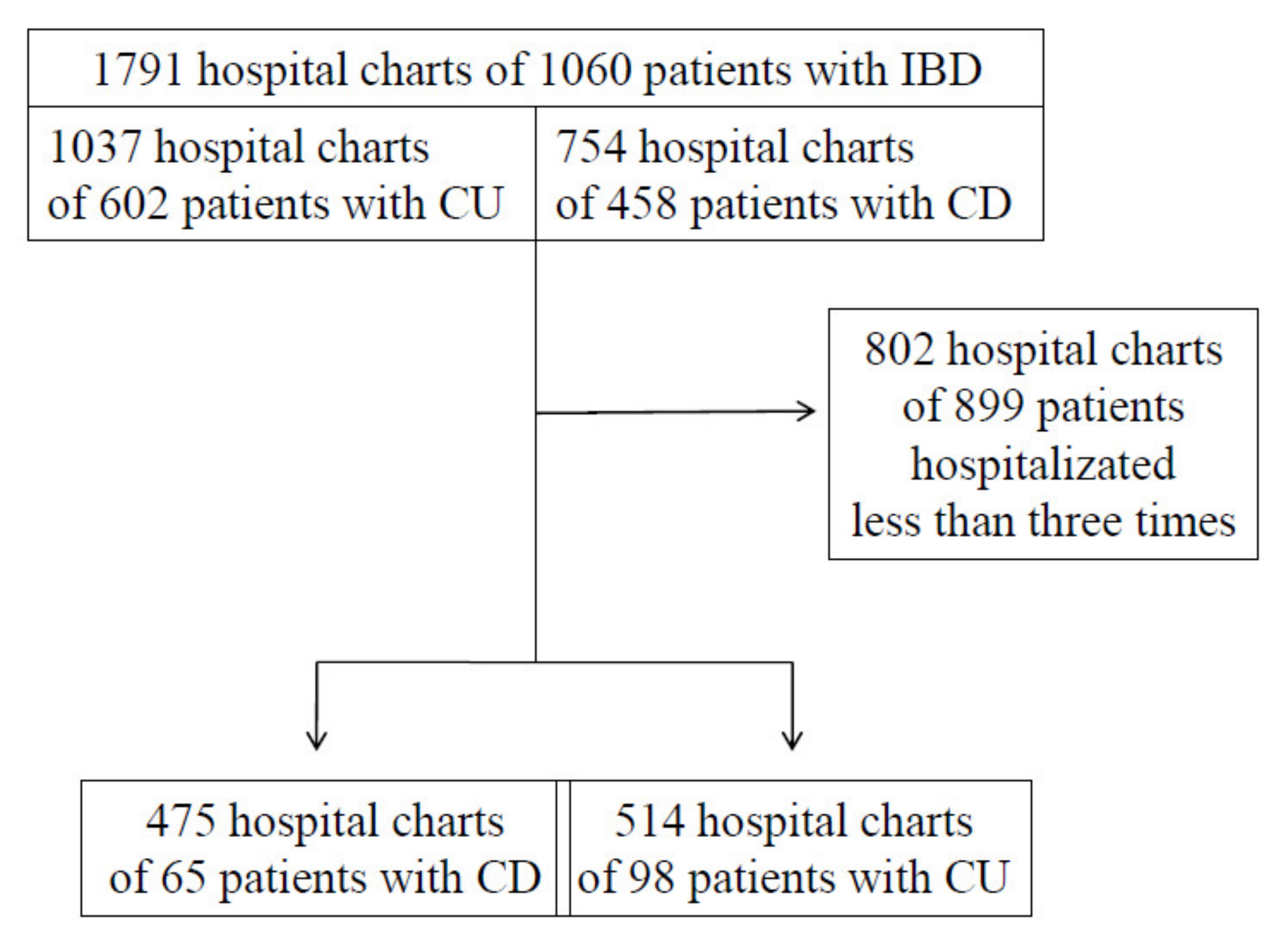
2.1. Study Design and Population
2.2. Measured Radiation Exposure
2.3. Statistical Analysis
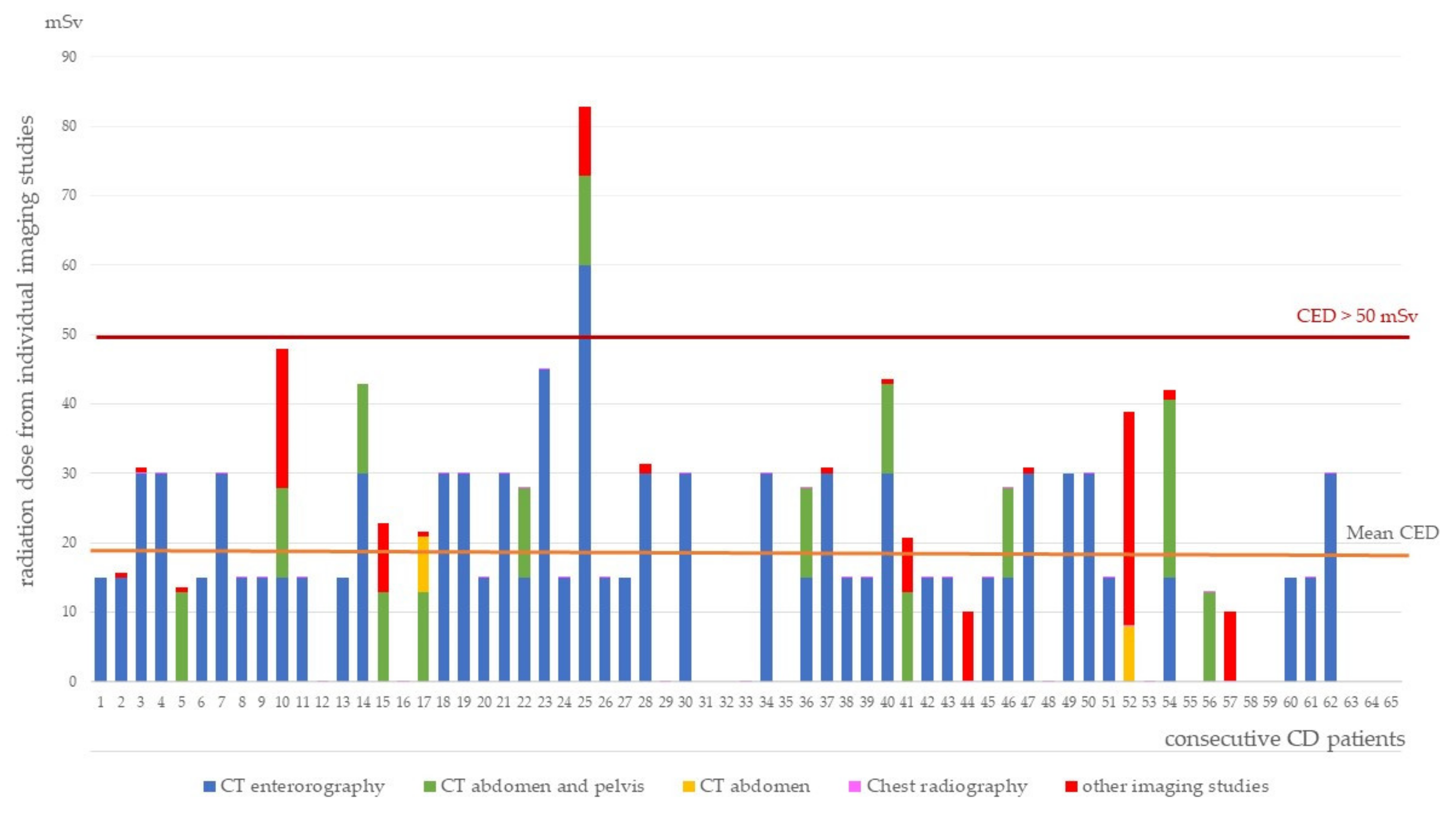
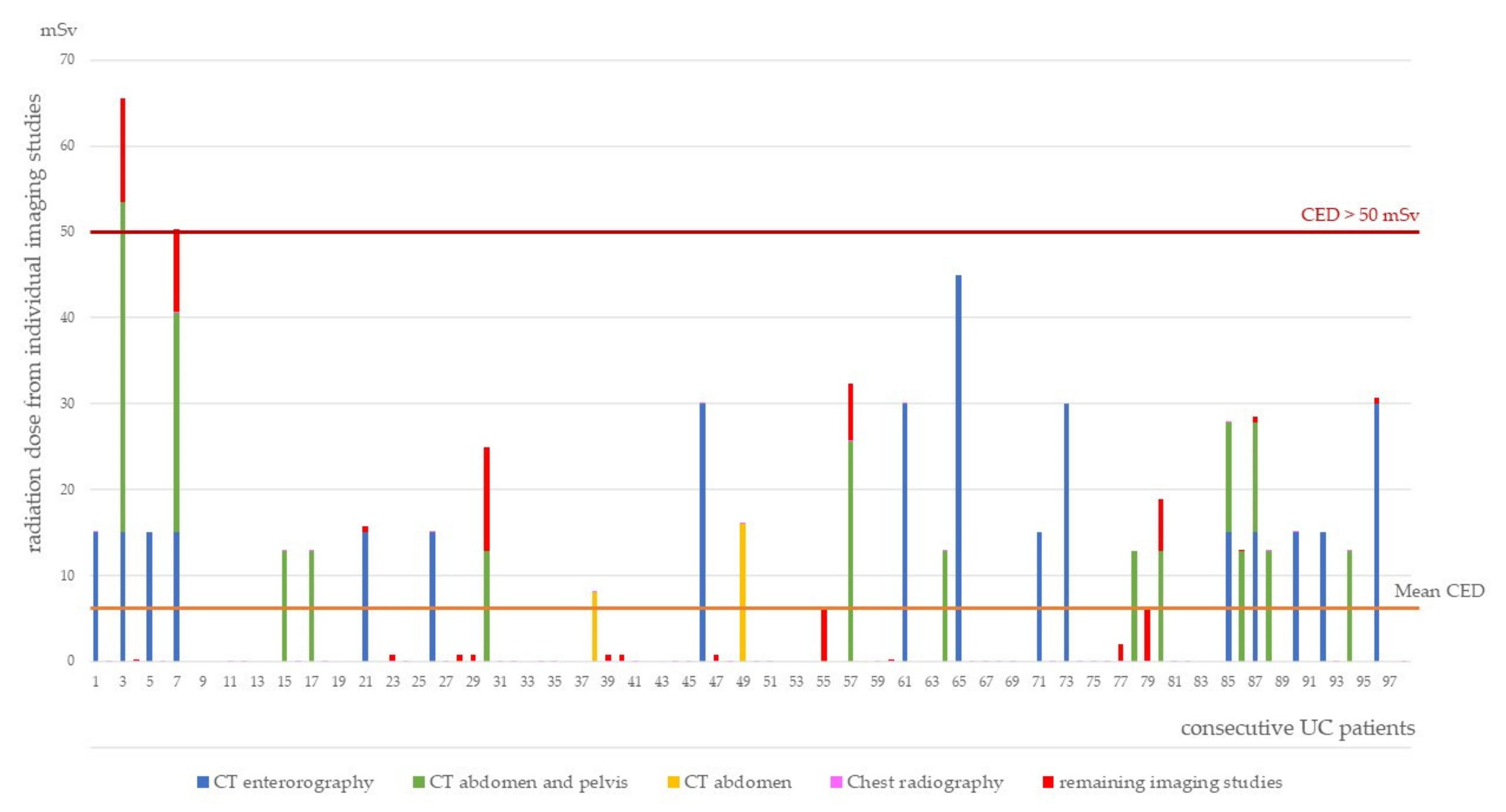
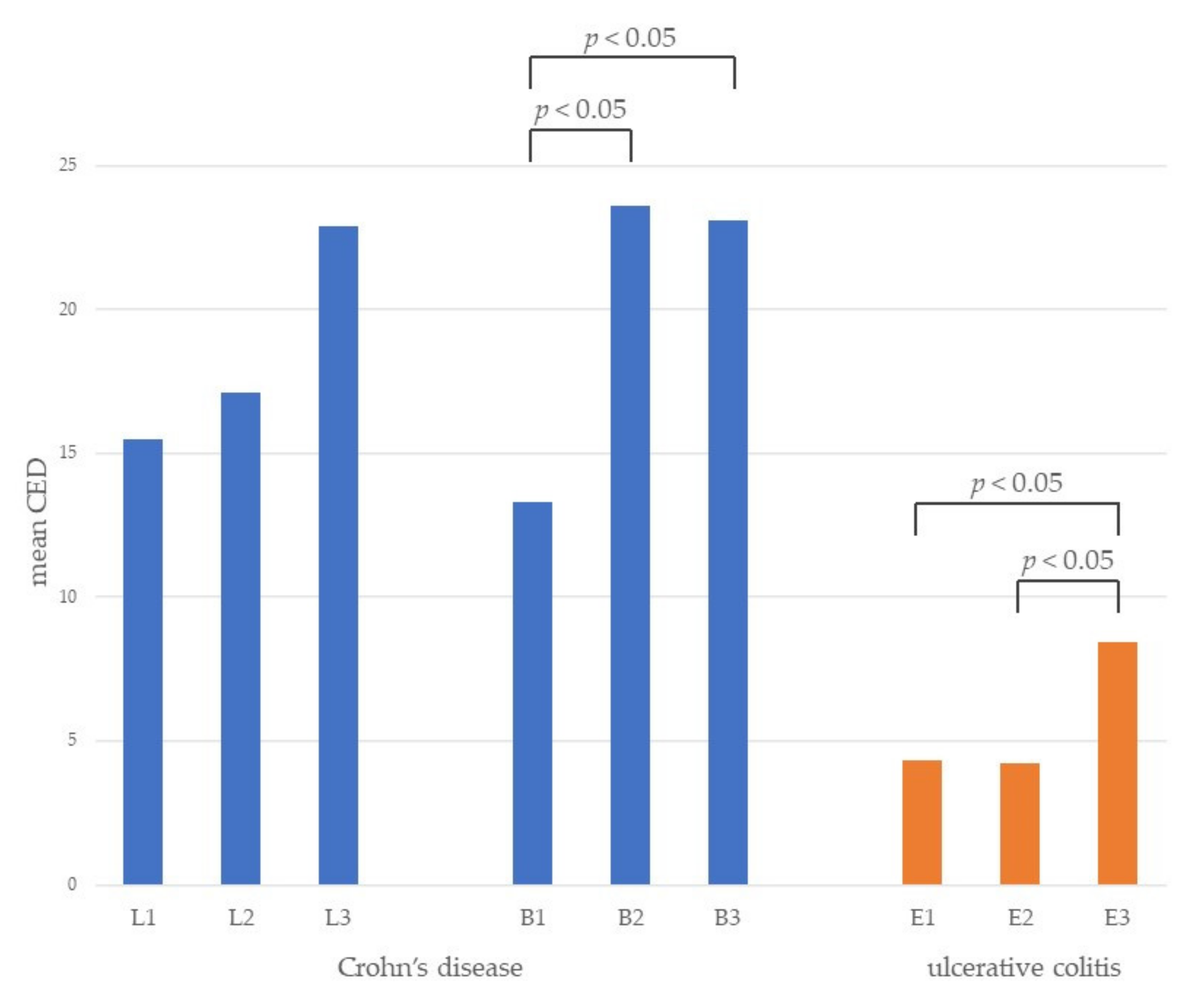
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ungaro, R.; Mehandru, S.; Allen, P.B.; Peyrin-Biroulet, L. Ulcerative colitis. Lancet 2017, 389, 1756–1770. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2016, 6736, 1741–1755. [Google Scholar] [CrossRef]
- Estay, C.; Simian, D.; Lubascher, J.; Figueroa, C.; O’Brien, A.; Quera, R. Ionizing radiation exposure in patients with inflammatory bowel disease: Are we overexposing our patients? J. Dig. Dis. 2015, 16, 83–89. [Google Scholar] [CrossRef]
- Zakeri, N.; Pollok, R.C.G. Diagnostic imaging and radiation exposure in inflammatory bowel disease. World J. Gastroenterol. 2016, 22, 2165–2178. [Google Scholar] [CrossRef] [Green Version]
- Mettler, F.A.; Huda, W.; Yoshizumi, T.T.; Mahesh, M. Effective doses in radiology and diagnostic nuclear medicine: A catalog. Radiology 2008, 248, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, M.; Vassileva, J.; Kuchcinska, A.; Rehani, M.M. Multinational data on cumulative radiation exposure of patients from recurrent radiological procedures: Call for action. Eur. Radiol. 2020, 30, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Long, M.D.; Martin, C.F.; Pipkin, C.A.; Herfarth, H.H.; Sandler, R.S.; Kappelman, M.D. Risk of melanoma and nonmelanoma skin cancer among patients with inflammatory bowel disease. Gastroenterology 2012, 143, 390–399.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.R.; Chang, D.K. Colorectal cancer in inflammatory bowel disease: The risk, pathogenesis, prevention and diagnosis. World J. Gastroenterol. 2014, 20, 9872–9881. [Google Scholar] [CrossRef]
- Ilangovan, R.; Burling, D.; George, A.; Gupta, A.; Marshall, M.; Taylor, S.A. CT enterography: Review of technique and practical tips. Br. J. Radiol. 2012, 85, 876–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, E.C. Radiation Risk From Medical Imaging. Mayo Clin. Proc. 2010, 85, 1142–1146. [Google Scholar] [CrossRef] [Green Version]
- Kroeker, K.I.; Lam, S.; Birchall, I.; Fedorak, R.N. Patients with IBD are exposed to high levels of ionizing radiation through CT scan diagnostic imaging: A five-year study. J. Clin. Gastroenterol. 2011, 45, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Naidu, J.; Wong, Z.; Palaniappan, S.; Ngiu, C.S.; Yaacob, N.Y. Radiation exposure in patients with inflammatory bowel disease: A fourteen-year review at a tertiary care centre in Malaysia. Asian Pac. J. Cancer Prev. 2017, 18, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Langevin, C.; Normandeau, L.; Bouin, M. Diagnostic radiation exposure in patients with inflammatory bowel disease. Can. J. Gastroenterol. Hepatol. 2019, 2019, 2030735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, G.C.; Low, D.; Chong, R.Y.; Diong, C.; Chawla, T. Utilization of diagnostic imaging and ionization radiation exposure among an inflammatory bowel disease inception cohort. Inflamm. Bowel Dis. 2020, 26, 898–906. [Google Scholar] [CrossRef]
- Fuchs, Y.; Markowitz, J.; Weinstein, T.; Kohn, N.; Choi-Rosen, J.; Levine, J. Pediatric inflammatory bowel disease and imaging-related radiation: Are we increasing the likelihood of malignancy? J. Pediatr. Gastroenterol. Nutr. 2011, 52, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Desmond, A.N.; O’Regan, K.; Curran, C.; McWilliams, S.; Fitzgerald, T.; Maher, M.M.; Shanahan, F. Crohn’s disease: Factors associated with exposure to high levels of diagnostic radiation. Gut 2008, 57, 1524–1529. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.K.; Malaty, H.M.; Thirumurthi, S. Radiation exposure from diagnostic imaging studies among patients with inflammatory bowel disease in a safety-net health-care system. Dig. Dis. Sci. 2014, 59, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.A.; Rustgi, A.; Quezada, S.M.; Flasar, M.H.; Vandermeer, F.; Cross, R.K. Anti-TNF therapy is associated with decreased imaging and radiation exposure in patients with Crohn’s disease. Inflamm. Bowel Dis. 2013, 19, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Park, D.I.; Kim, E.R.; Kim, Y.H.; Lee, C.K.; Lee, S.H.; Kim, J.H.; Huh, K.C.; Jung, S.A.; Yoon, S.M.; et al. Quantifying exposure to diagnostic radiation and factors associated with exposure to high levels of radiation in Korean patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 1852–1857. [Google Scholar] [CrossRef] [PubMed]
- Levi, Z.; Fraser, A.; Krongrad, R.; Hazazi, R.; Benjaminov, O.; Meyerovitch, J.; Tal, O.B.; Choen, A.; Niv, Y.; Fraser, G. Factors associated with radiation exposure in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2009, 30, 1128–1136. [Google Scholar] [CrossRef]
- Newnham, E.; Hawkes, E.; Surender, A.; James, S.L.; Gearry, R.; Gibson, P.R. Quantifying exposure to diagnostic medical radiation in patients with inflammatory bowel disease: Are we contributing to malignancy? Aliment. Pharmacol. Ther. 2007, 26, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Palmer, L.; Herfarth, H.; Porter, C.Q.; Fordham, L.A.; Sandler, R.S.; Kappelman, M.D. Diagnostic ionizing radiation exposure in a population-based sample of children with inflammatory bowel diseases. Am. J. Gastroenterol. 2009, 104, 2816–2823. [Google Scholar] [CrossRef] [Green Version]
- Chatu, S.; Subramanian, V.; Pollok, R.C.G. Meta-analysis: Diagnostic medical radiation exposure in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2012, 35, 529–539. [Google Scholar] [CrossRef]
- Patil, S.A.; Flasar, M.H.; Lin, J.; Lingohr-Smith, M.; Skup, M.; Wang, S.; Chao, J.; Cross, R.K. Reduced imaging radiation exposure and costs associated with anti-tumor necrosis factor therapy in Crohn’s disease. Dig. Dis. Sci. 2019, 64, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Englund, H.; Lidén, K.K.; Lind, T.; Sundström, T.; Karling, P. Radiation exposure in patients with inflammatory bowel disease and irritable bowel syndrome in the years 2001–2011. Scand. J. Gastroenterol. 2017, 52, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Davari, M.; Keshtkar, A.; Sajadian, E.S.; Delavari, A.; Iman, R. Safety and effectiveness of MRE in comparison with CTE in diagnosis of adult Crohn’s disease. Med. J. Islam. Repub. Iran 2019, 33, 132. [Google Scholar] [CrossRef] [PubMed]
- Sturm, A.; Maaser, C.; Calabrese, E.; Annese, V.; Fiorino, G.; Kucharzik, T.; Vavricka, S.R.; Verstockt, B.; Van Rheenen, P.; Tolan, D.; et al. ECCO-ESGGAR guideline for diagnostic assessment in IBD part 2: IBD scores and general principles and technical aspects. J. Crohn’s Colitis 2019, 13, 284. [Google Scholar] [CrossRef] [PubMed]
- Horsthuis, K.; Bipat, S.; Bennink, R.J.; Stoker, J. Inflammatory bowel disease diagnosed with US, MR, scintigraphy, and CT: Meta-analysis of prospective studies. Radiology 2008, 247, 64–79. [Google Scholar] [CrossRef]
- Fiorino, G.; Bonifacio, C.; Peyrin-Biroulet, L.; Minuti, F.; Repici, A.; Spinelli, A.; Fries, W.; Balzarini, L.; Montorsi, M.; Malesci, A.; et al. Prospective comparison of computed tomography enterography and magnetic resonance enterography for assessment of disease activity and complications in ileocolonic Crohn’s disease. Inflamm. Bowel Dis. 2011, 17, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Haas, K.; Rubesova, E.; Bass, D. Role of imaging in the evaluation of inflammatory bowel disease: How much is too much? World J. Radiol. 2016, 8, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Kunze, G.; Seitz, K.; Mauch, M.; Petersen, F. Clinical ultrasound in inflammatory bowel disease. Ultraschall Med. 2019, 40, 132–162. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Procedure | Effective Dose, mSv | Reference |
|---|---|---|
| CT enterorography | 15 | [9] |
| CT abdomen and pelvis | 12.8 | [10] |
| CT abdomen | 8 | [5] |
| Abdomen radiography | 0.7 | [5] |
| Chest radiography | 0.02 | [5] |
| Endoscopic retrograde cholangiopancreatography | 4 | [5] |
| Features | CD | UC | p-Value |
|---|---|---|---|
| Females/males, n | 33/32 | 47/51 | 0.85 |
| Mean age (SD) | 40.8 (14.55) | 42.65 (15.66) | 0.45 |
| Mean duration of the disease, years (SD) | 10.72 (8.74) | 12.84 (9.769) | 0.16 |
| Mean age of the onset of the disease, years (SD) | 30.18 (14.49) | 29.91 (13.18) | 0.91 |
| Number of hospitalizations of all patients, n | 475 | 514 | 0.02 |
| Hospitalization days of all patients | 1879 | 2572 | 0.37 |
| Mean length of single hospitalization, days (SD) | 5.63 (4.069) | 5.35 (3.00) | 0.31 |
| Number of patients after surgical procedures in course of disease, n (%) | 40 (61.54%) | 10 (10.20%) | <0.001 |
| Location of CD L1/L2/L3 (n) | 7/21/34 | ||
| Behavior of CD B1/B2/B3 (n) | 27/21/17 | ||
| Extension of UC E1/E2/E3 (n) | 7/32/55 |
| Number of Imaging Studies | CD | UC | p-Value |
|---|---|---|---|
| Number of all imaging studies performed, n | 250 | 233 | <0.001 |
| Number of imaging studies with ionization radiation performed, n | 181 | 170 | 0.002 |
| CT abdomen, n | 2 | 3 | |
| CT abdomen and pelvis, n | 14 | 18 | 0.99 |
| CT enterography, n | 63 | 22 | 0.68 |
| Chest X-rays, n | 75 | 92 | <0.001 |
| Abdomen X-rays, n | 11 | 11 | 0.14 |
| Parameters | All Patients | CD | UC | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Age | 0.15 | 0,07 | 0.34 | <0.01 | 0.07 | 0.51 |
| Duration of the disease | 0.14 | 0.07 | 0.01 | 0.92 | 0.07 | 0.48 |
| Number of hospitalizations | 0.19 | 0.02 | 0.11 | 0.40 | 0.18 | 0.09 |
| Hospitalization days | 0.49 | <0.00001 | 0.55 | <0.00001 | 0.48 | <0.00001 |
| Number of surgical procedures | 0.40 | <0.00001 | 0.27 | 0.03 | 0.29 | <0.01 |
| Steroid treatment | −0.05 | 0.56 | 0.04 | 0.77 | −0.11 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łukawska, A.; Ślósarz, D.; Zimoch, A.; Serafin, K.; Poniewierka, E.; Kempiński, R. Cumulative Effective Dose from Medical Imaging in Inflammatory Bowel Disease. Diagnostics 2021, 11, 2387. https://doi.org/10.3390/diagnostics11122387
Łukawska A, Ślósarz D, Zimoch A, Serafin K, Poniewierka E, Kempiński R. Cumulative Effective Dose from Medical Imaging in Inflammatory Bowel Disease. Diagnostics. 2021; 11(12):2387. https://doi.org/10.3390/diagnostics11122387
Chicago/Turabian StyleŁukawska, Agata, Dominika Ślósarz, Aneta Zimoch, Karol Serafin, Elżbieta Poniewierka, and Radosław Kempiński. 2021. "Cumulative Effective Dose from Medical Imaging in Inflammatory Bowel Disease" Diagnostics 11, no. 12: 2387. https://doi.org/10.3390/diagnostics11122387