Somatostatin Receptor PET/CT Imaging for the Detection and Staging of Pancreatic NET: A Systematic Review and Meta-Analysis

 , , , , , , , and
, , , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Quality Evaluation and Statistical Analysis
3. Results
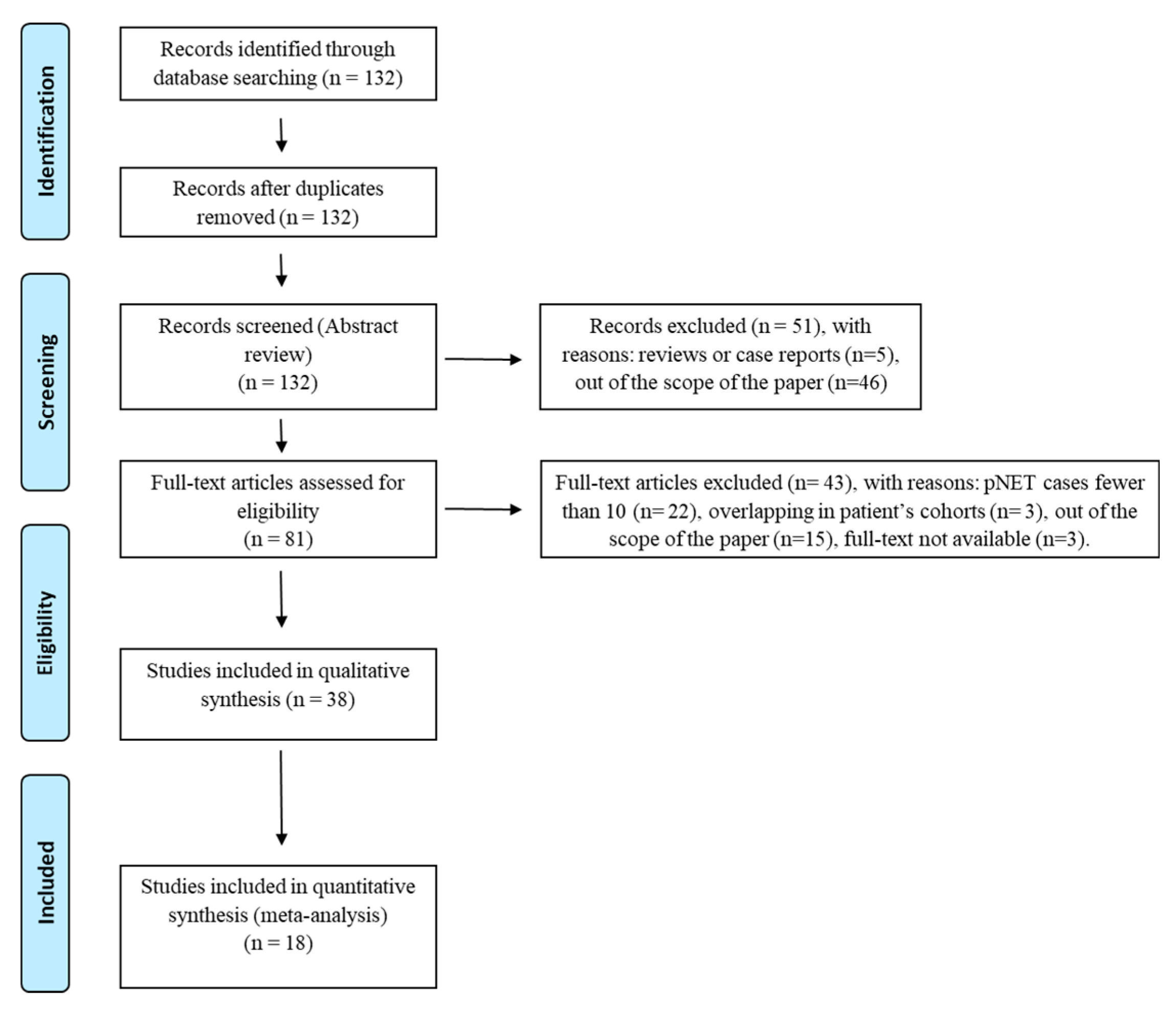
3.1. Search Results
3.2. Study Characteristics
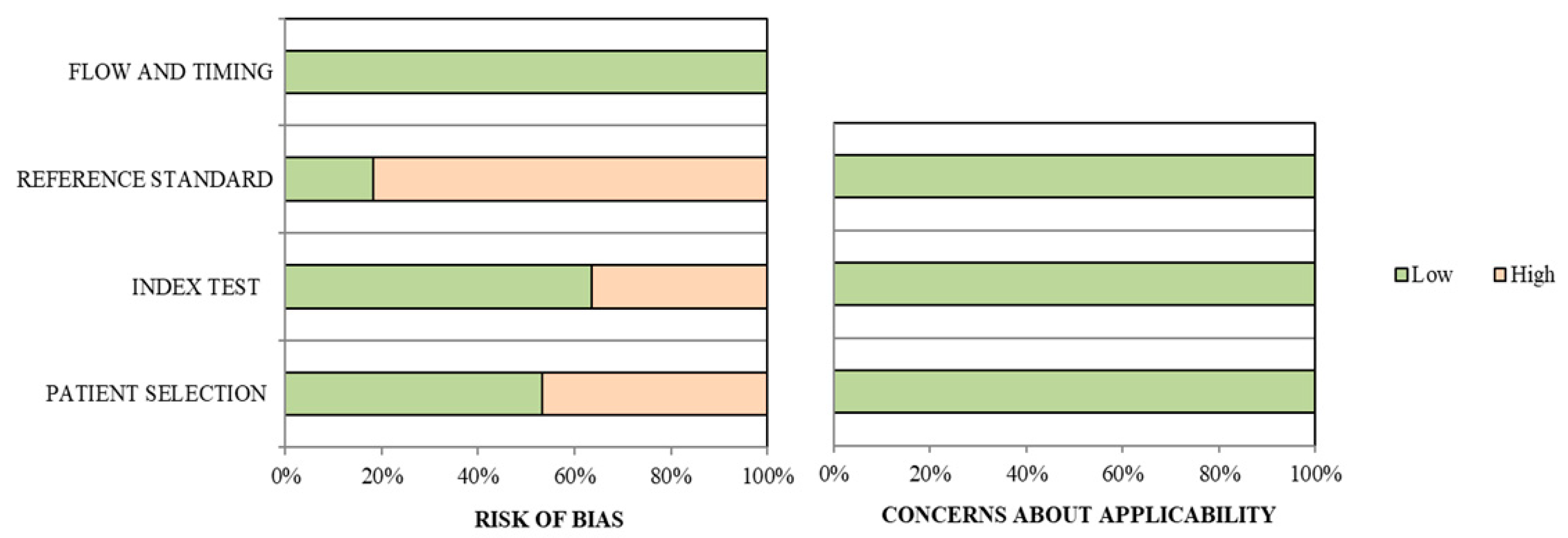
3.3. Qualitative Analysis
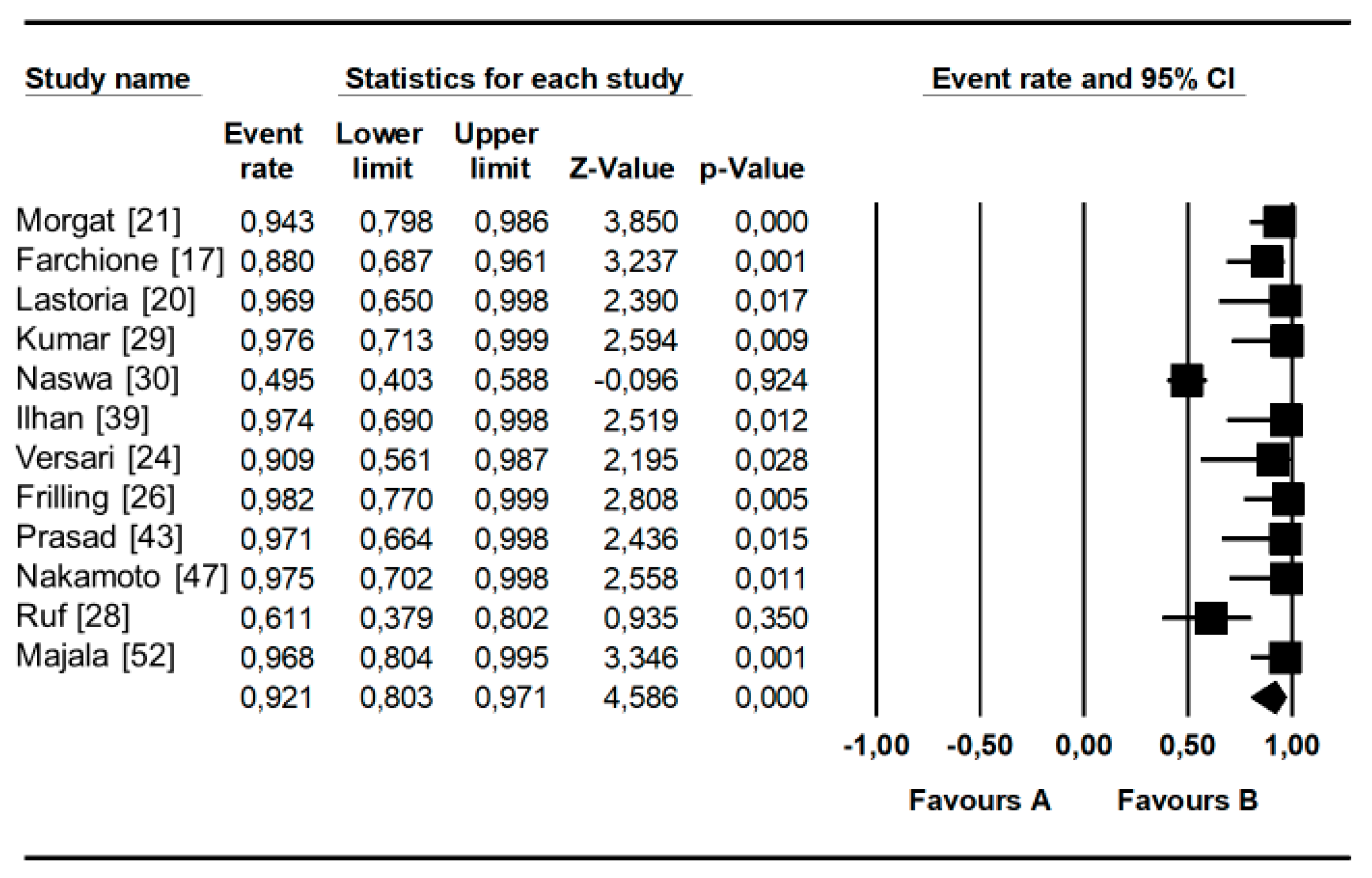
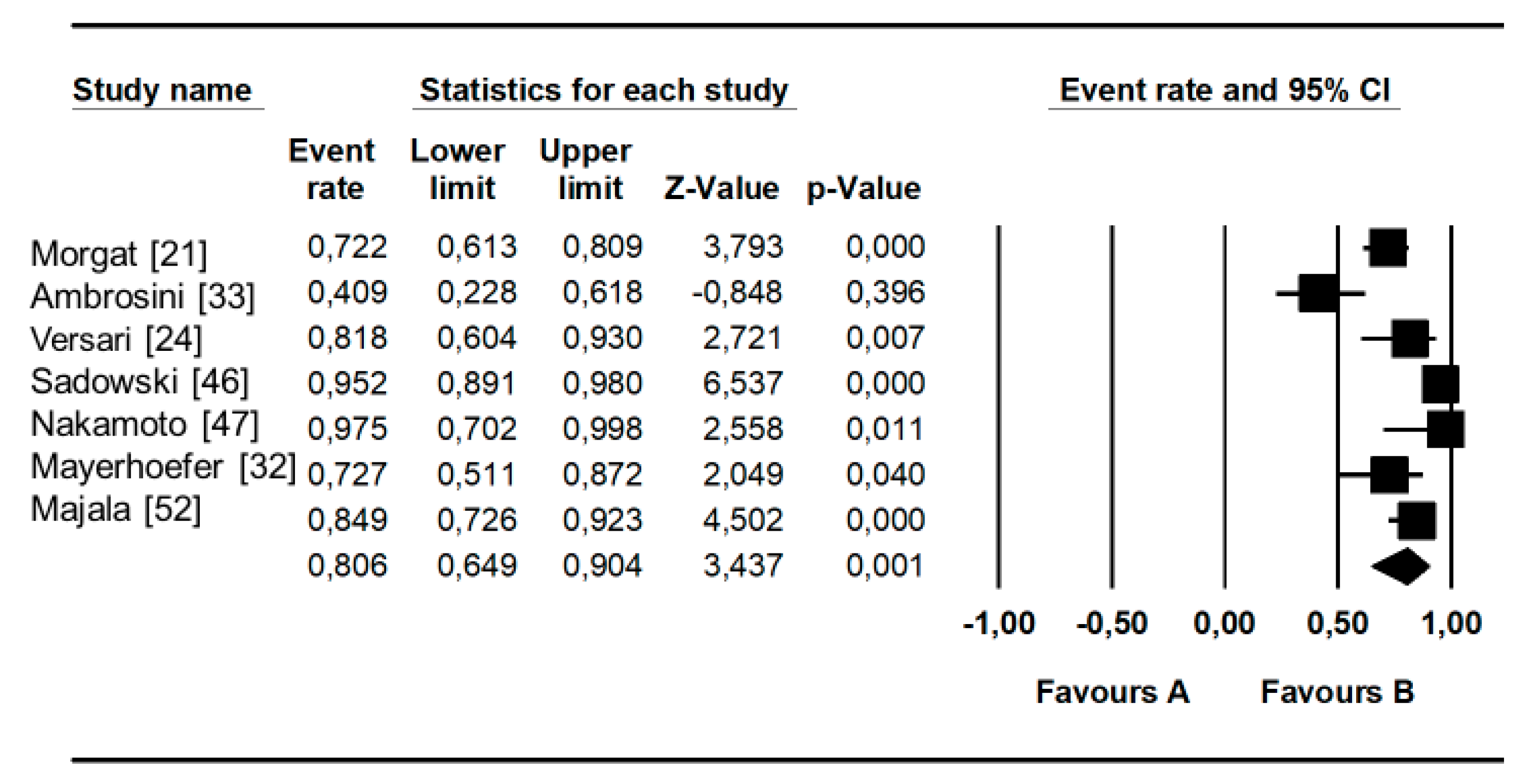
3.4. Quantitative Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Abdalla, E.K.; Fleming, J.B.; Vauthey, J.N.; Rashid, A.; et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraenkel, M.; Kim, M.K.; Faggiano, A.; Valk, G.D. Epidemiology of gastroenteropancreatic neuroendocrine tumours. Best Pract. Res. Clin. Gastroenterol. 2012, 26, 691–703. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G. Classification and pathology of gastroenteropancreatic neuroendocrine neoplasms. Endocr. Relat. Cancer 2011, 18, S1–S16. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.T.; Berna, M.J.; Bingham, D.B.; Norton, J.A. Inherited pancreatic endocrine tumor syndromes: Advances in molecular pathogenesis, diagnosis, management, and controversies. Cancer 2008, 113, 1807–1843. [Google Scholar] [CrossRef] [Green Version]
- Dromain, C.; Déandréis, D.; Scoazec, J.Y.; Goere, D.; Ducreux, M.; Baudin, E.; Tselikas, L. Imaging of neuroendocrine tumors of the pancreas. Diagn. Interv. Imaging 2016, 97, 1241–1257. [Google Scholar] [CrossRef]
- Papotti, M.; Bongiovanni, M.; Volante, M.; Allìa, E.; Landolfi, S.; Helboe, L.; Schindler, M.; Cole, S.L.; Bussolati, G. Expression of somatostatin receptor types 1-5 in 81 cases of gastrointestinal and pancreatic endocrine tumors. A correlative immunohistochemical and reverse-transcriptase polymerase chain reaction analysis. Virchows Arch. 2002, 440, 461–475. [Google Scholar] [CrossRef]
- Reubi, J.C.; Waser, B. Concomitant expression of several peptide receptors in neuroendocrine tumours: Molecular basis for in vivo multireceptor tumour targeting. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 781–793. [Google Scholar] [CrossRef]
- Modlin, I.M.; Oberg, K.; Chung, D.C.; Jensen, R.T.; de Herder, W.W.; Thakker, R.V.; Caplin, M.; Delle Fave, G.; Kaltsas, G.A.; Krenning, E.P.; et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008, 9, 61–72. [Google Scholar] [CrossRef]
- Öksüz, M.Ö.; Winter, L.; Pfannenberg, C.; Reischl, G.; Müssig, K.; Bares, R.; Dittmann, H. Peptide receptor radionuclide therapy of neuroendocrine tumors with (90)Y-DOTATOC: Is treatment response predictable by pre-therapeutic uptake of (68)Ga-DOTATOC? Diagn. Interv. Imaging 2014, 95, 289–300. [Google Scholar] [CrossRef] [Green Version]
- Poeppel, T.D.; Binse, I.; Petersenn, S.; Lahner, H.; Schott, M.; Antoch, G.; Brandau, W.; Bockisch, A.; Boy, C. 68Ga-DOTATOC versus 68Ga-DOTATATE PET/CT in functional imaging of neuroendocrine tumors. J. Nucl. Med. 2011, 52, 1864–1870. [Google Scholar] [CrossRef] [Green Version]
- Wild, D.; Bomanji, J.B.; Benkert, P.; Maecke, H.; Ell, P.J.; Reubi, J.C.; Caplin, M.E. Comparison of 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT within patients with gastroenteropancreatic neuroendocrine tumors. J. Nucl. Med. 2013, 54, 364–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 3, e123–e130. [Google Scholar] [PubMed]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Wallace, B.C.; Schmid, C.H.; Lau, J.; Trikalinos, T.A. Meta-Analyst: Software for meta-analysis of binary, continuous and diagnostic data. BMC Med. Res. Methodol. 2009, 9, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nockel, P.; Babic, B.; Millo, C.; Herscovitch, P.; Patel, D.; Nilubol, N.; Sadowski, S.M.; Cochran, C.; Gorden, P.; Kebebew, E. Localization of Insulinoma Using 68Ga-DOTATATE PET/CT Scan. J. Clin. Endocrinol. Metab. 2017, 102, 195–199. [Google Scholar] [CrossRef] [Green Version]
- Farchione, A.; Rufini, V.; Brizi, M.G.; Iacovazzo, D.; Larghi, A.; Massara, R.M.; Petrone, G.; Poscia, A.; Treglia, G.; De Marinis, L.; et al. Evaluation of the Added Value of Diffusion-Weighted Imaging to Conventional Magnetic Resonance Imaging in Pancreatic Neuroendocrine Tumors and Comparison with 68Ga-DOTANOC Positron Emission Tomography/Computed Tomography. Pancreas 2016, 45, 345–354. [Google Scholar] [CrossRef]
- Shell, J.; Tirosh, A.; Millo, C.; Sadowski, S.M.; Assadipour, Y.; Green, P.; Patel, D.; Nilubol, N.; Kebebew, E. The utility of 68Gallium-DOTATATE PET/CT in the detection of von Hippel-Lindau disease associated tumors. Eur. J. Radiol. 2019, 112, 130–135. [Google Scholar] [CrossRef]
- Sadowski, S.M.; Millo, C.; Cottle-Delisle, C.; Merkel, R.; Yang, L.A.; Herscovitch, P.; Pacak, K.; Simonds, W.F.; Marx, S.J.; Kebebew, E. Results of (68)Gallium-DOTATATE PET/CT Scanning in Patients with Multiple Endocrine Neoplasia Type 1. J. Am. Coll. Surg. 2015, 221, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Lastoria, S.; Marciello, F.; Faggiano, A.; Aloj, L.; Caracò, C.; Aurilio, M.; D’Ambrosio, L.; Di Gennaro, F.; Ramundo, V.; Camera, L.; et al. Role of (68)Ga-DOTATATE PET/CT in patients with multiple endocrine neoplasia type 1 (MEN1). Endocrine 2016, 52, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Morgat, C.; Vélayoudom-Céphise, F.L.; Schwartz, P.; Guyot, M.; Gaye, D.; Vimont, D.; Schulz, J.; Mazère, J.; Nunes, M.L.; Smith, D.; et al. Evaluation of (68)Ga-DOTA-TOC PET/CT for the detection of duodenopancreatic neuroendocrine tumors in patients with MEN1. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1258–1266. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, M.; Oberauer, A.; Dobrozemsky, G.; Decristoforo, C.; Putzer, D.; Kendler, D.; Uprimny, C.; Kovacs, P.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: Comparison with somatostatin receptor scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Putzer, D.; Gabriel, M.; Henninger, B.; Kendler, D.; Uprimny, C.; Dobrozemsky, G.; Decristoforo, C.; Bale, R.J.; Jaschke, W.; Virgolini, I.J. Bone metastases in patients with neuroendocrine tumor: 68Ga-DOTA-Tyr3-octreotide PET in comparison to CT and bone scintigraphy. J. Nucl. Med. 2009, 50, 1214–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versari, A.; Camellini, L.; Carlinfante, G.; Frasoldati, A.; Nicoli, F.; Grassi, E.; Gallo, C.; Giunta, F.P.; Fraternali, A.; Salvo, D.; et al. Ga-68 DOTATOC PET, endoscopic ultrasonography, and multidetector CT in the diagnosis of duodenopancreatic neuroendocrine tumors: A single-centre retrospective study. Clin. Nucl. Med. 2010, 35, 321–328. [Google Scholar] [CrossRef]
- Srirajaskanthan, R.; Kayani, I.; Quigley, A.M.; Soh, J.; Caplin, M.E.; Bomanji, J. The role of 68Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111In-DTPA-octreotide scintigraphy. J. Nucl. Med. 2010, 51, 875–882. [Google Scholar] [CrossRef] [Green Version]
- Frilling, A.; Sotiropoulos, G.C.; Radtke, A.; Malago, M.; Bockisch, A.; Kuehl, H.; Li, J.; Broelsch, C.E. The impact of 68Ga-DOTATOC positron emission tomography/computed tomography on the multimodal management of patients with neuroendocrine tumors. Ann. Surg. 2010, 252, 850–856. [Google Scholar] [CrossRef]
- Prasad, V.; Ambrosini, V.; Hommann, M.; Hoersch, D.; Fanti, S.; Baum, R.P. Detection of unknown primary neuroendocrine tumours (CUP-NET) using (68)Ga-DOTA-NOC receptor PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 67–77. [Google Scholar] [CrossRef]
- Ruf, J.; Heuck, F.; Schiefer, J.; Denecke, T.; Elgeti, F.; Pascher, A.; Pavel, M.; Stelter, L.; Kropf, S.; Wiedenmann, B.; et al. Impact of Multiphase 68Ga-DOTATOC-PET/CT on therapy management in patients with neuroendocrine tumors. Neuroendocrinology 2010, 91, 101–109. [Google Scholar] [CrossRef]
- Kumar, R.; Sharma, P.; Garg, P.; Karunanithi, S.; Naswa, N.; Sharma, R.; Thulkar, S.; Lata, S.; Malhotra, A. Role of (68)Ga-DOTATOC PET-CT in the diagnosis and staging of pancreatic neuroendocrine tumours. Eur. Radiol. 2011, 21, 2408–2416. [Google Scholar] [CrossRef]
- Naswa, N.; Sharma, P.; Kumar, A.; Nazar, A.H.; Kumar, R.; Chumber, S.; Bal, C. Gallium-68-DOTA-NOC PET/CT of patients with gastroenteropancreatic neuroendocrine tumors: A prospective single-center study. AJR. Am. J. Roentgenol. 2011, 197, 1221–1228. [Google Scholar] [CrossRef]
- Krausz, Y.; Rubinstein, R.; Appelbaum, L.; Mishani, E.; Orevi, M.; Fraenkel, M.; Tshori, S.; Glaser, B.; Bocher, M.; Salmon, A.; et al. Ga-68 DOTA-NOC uptake in the pancreas: Pathological and physiological patterns. Clin. Nucl. Med. 2012, 37, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Schuetz, M.; Magnaldi, S.; Weber, M.; Trattnig, S.; Karanikas, G. Are contrast media required for (68)Ga-DOTATOC PET/CT in patients with neuroendocrine tumours of the abdomen? Eur. Radiol. 2012, 22, 938–946. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, V.; Campana, D.; Nanni, C.; Cambioli, S.; Tomassetti, P.; Rubello, D.; Fanti, S. Is 68Ga-DOTA-NOC PET/CT indicated in patients with clinical, biochemical or radiological suspicion of neuroendocrine tumour? Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1278–1283. [Google Scholar] [CrossRef]
- Kroiss, A.; Putzer, D.; Decristoforo, C.; Uprimny, C.; Warwitz, B.; Nilica, B.; Gabriel, M.; Kendler, D.; Waitz, D.; Widmann, G.; et al. 68Ga-DOTA-TOC uptake in neuroendocrine tumour and healthy tissue: Differentiation of physiological uptake and pathological processes in PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Schmid-Tannwald, C.; Schmid-Tannwald, C.M.; Morelli, J.N.; Neumann, R.; Haug, A.R.; Jansen, N.; Nikolaou, K.; Schramm, N.; Reiser, M.F.; Rist, C. Comparison of abdominal MRI with diffusion-weighted imaging to 68Ga-DOTATATE PET/CT in detection of neuroendocrine tumors of the pancreas. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Kunikowska, J.; Pawlak, D.; Kolasa, A.; Mikołajczak, R.; Królicki, L. A frequency and semiquantitative analysis of pathological 68Ga DOTATATE PET/CT uptake by primary site-dependent neuroendocrine tumor metastasis. Clin. Nucl. Med. 2014, 39, 855–861. [Google Scholar] [CrossRef]
- Mapelli, P.; Tam, H.H.; Sharma, R.; Aboagye, E.O.; Al-Nahhas, A. Frequency and significance of physiological versus pathological uptake of 68Ga-DOTATATE in the pancreas: Validation with morphological imaging. Nucl. Med. Commun. 2014, 35, 613–619. [Google Scholar] [CrossRef]
- Kaemmerer, D.; Wirtz, R.M.; Fischer, E.K.; Hommann, M.; Sänger, J.; Prasad, V.; Specht, E.; Baum, R.P.; Schulz, S.; Lupp, A. Analysis of somatostatin receptor 2A immunohistochemistry, RT-qPCR, and in vivo PET/CT data in patients with pancreatic neuroendocrine neoplasm. Pancreas 2015, 44, 648–654. [Google Scholar] [CrossRef]
- Ilhan, H.; Fendler, W.P.; Cyran, C.C.; Spitzweg, C.; Auernhammer, C.J.; Gildehaus, F.J.; Bartenstein, P.; Angele, M.K.; Haug, A.R. Impact of (68)Ga-DOTATATE PET/CT on the surgical management of primary neuroendocrine tumors of the pancreas or ileum. Ann. Surg. Oncol. 2015, 22, 164–171. [Google Scholar] [CrossRef]
- Malmberg, C.; Ripa, R.S.; Johnbeck, C.B.; Knigge, U.; Langer, S.W.; Mortensen, J.; Oturai, P.; Loft, A.; Hag, A.M.; Kjær, A. 64Cu-DOTATATE for Noninvasive Assessment of Atherosclerosis in Large Arteries and Its Correlation with Risk Factors: Head-to-Head Comparison with 68Ga-DOTATOC in 60 Patients. J. Nucl. Med. 2015, 56, 1895–1900. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Arora, S.; Dhull, V.S.; Naswa, N.; Kumar, R.; Ammini, A.C.; Bal, C. Evaluation of (68)Ga-DOTANOC PET/CT imaging in a large exclusive population of pancreatic neuroendocrine tumors. Abdom. Imaging 2015, 40, 299–309. [Google Scholar] [CrossRef]
- Skoura, E.; Michopoulou, S.; Mohmaduvesh, M.; Panagiotidis, E.; Al Harbi, M.; Toumpanakis, C.; Almukhailed, O.; Kayani, I.; Syed, R.; Navalkissoor, S.; et al. The Impact of 68Ga-DOTATATE PET/CT Imaging on Management of Patients with Neuroendocrine Tumors: Experience from a National Referral Center in the United Kingdom. J. Nucl. Med. 2016, 57, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, V.; Tiling, N.; Denecke, T.; Brenner, W.; Plöckinger, U. Potential role of (68)Ga-DOTATOC PET/CT in screening for pancreatic neuroendocrine tumour in patients with von Hippel-Lindau disease. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 2014–2020. [Google Scholar] [CrossRef] [PubMed]
- Deppen, S.A.; Liu, E.; Blume, J.D.; Clanton, J.; Shi, C.; Jones-Jackson, L.B.; Lakhani, V.; Baum, R.P.; Berlin, J.; Smith, G.T.; et al. Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging, and Treatment Management of Neuroendocrine Tumors. J. Nucl. Med. 2016, 57, 708–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazmierczak, P.M.; Rominger, A.; Wenter, V.; Spitzweg, C.; Auernhammer, C.; Angele, M.K.; Rist, C.; Cyran, C.C. The added value of 68Ga-DOTA-TATE-PET to contrast-enhanced CT for primary site detection in CUP of neuroendocrine origin. Eur. Radiol. 2017, 27, 1676–1684. [Google Scholar] [CrossRef]
- Sadowski, S.M.; Neychev, V.; Millo, C.; Shih, J.; Nilubol, N.; Herscovitch, P.; Pacak, K.; Marx, S.J.; Kebebew, E. Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites. J. Clin. Oncol. 2016, 34, 588–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamoto, Y.; Ishimori, T.; Sano, K.; Temma, T.; Ueda, M.; Saji, H.; Togashi, K. Clinical efficacy of dual-phase scanning using (68)Ga-DOTATOC-PET/CT in the detection of neuroendocrine tumours. Clin. Radiol. 2016, 71, e1–e1069. [Google Scholar] [CrossRef]
- Cingarlini, S.; Ortolani, S.; Salgarello, M.; Butturini, G.; Malpaga, A.; Malfatti, V.; DʼOnofrio, M.; Davì, M.V.; Vallerio, P.; Ruzzenente, A.; et al. Role of Combined 68Ga-DOTATOC and 18F-FDG Positron Emission Tomography/Computed Tomography in the Diagnostic Workup of Pancreas Neuroendocrine Tumors: Implications for Managing Surgical Decisions. Pancreas 2017, 46, 42–47. [Google Scholar] [CrossRef]
- Bertani, E.; Fazio, N.; Radice, D.; Zardini, C.; Spinoglio, G.; Chiappa, A.; Ribero, D.; Biffi, R.; Partelli, S.; Falconi, M. Assessing the role of primary tumour resection in patients with synchronous unresectable liver metastases from pancreatic neuroendocrine tumour of the body and tail. A propensity score survival evaluation. Eur. J. Surg. Oncol. 2017, 43, 372–379. [Google Scholar] [CrossRef]
- Chen, S.H.; Chang, Y.C.; Hwang, T.L.; Chen, J.S.; Chou, W.C.; Hsieh, C.H.; Yeh, T.S.; Hsu, J.T.; Yeh, C.N.; Tseng, J.H.; et al. 68Ga-DOTATOC and 18F-FDG PET/CT for identifying the primary lesions of suspected and metastatic neuroendocrine tumors: A prospective study in Taiwan. J. Formos. Med. Assoc. 2018, 117, 480–487. [Google Scholar] [CrossRef]
- Komek, H.; Ansal Balci, T.; Can, C. Efficacy of Galium-68 DOTATATE PET/CT in the Detection of Metastasis Rate of Well-Differentiated Gastroenteropancreatic Neuroendocrine Tumors. Asia Ocean. J. Nucl. Med. Biol. 2019, 7, 141–148. [Google Scholar] [PubMed]
- Majala, S.; Seppänen, H.; Kemppainen, J.; Sundström, J.; Schalin-Jäntti, C.; Gullichsen, R.; Schildt, J.; Mustonen, H.; Vesterinen, T.; Arola, J.; et al. Prediction of the aggressiveness of non-functional pancreatic neuroendocrine tumors based on the dual-tracer PET/CT. EJNMMI Res. 2019, 9, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geijer, H.; Breimer, L.H. Somatostatin receptor PET/CT in neuroendocrine tumours: Update on systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, T.; Stölzel, U.; Bäder, M.; Koppenhagen, K.; Hamm, B.; Buhr, H.; Riecken, E.O.; Wiedenmann, B. Endoscopic ultrasonography and somatostatin receptor scintigraphy in the preoperative localisation of insulinomas and gastrinomas. Gut 1996, 39, 562–568. [Google Scholar] [CrossRef]
- Ambrosini, V.; Tomassetti, P.; Castellucci, P.; Campana, D.; Montini, G.; Rubello, D.; Nanni, C.; Rizzello, A.; Franchi, R.; Fanti, S. Comparison between 68Ga-DOTA-NOC and 18F-DOPA PET for the detection of gastro-entero-pancreatic and lung neuro-endocrine tumours. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1431–1438. [Google Scholar] [CrossRef]
- Prasad, V.; Baum, R.P. Biodistribution of the Ga-68 labeled somatostatin analogue DOTA-NOC in patients with neuroendocrine tumors: Characterization of uptake in normal organs and tumor lesions. Q. J. Nucl. Med. Mol. Imaging 2010, 54, 61–67. [Google Scholar]
- Ambrosini, V.; Campana, D.; Bodei, L.; Nanni, C.; Castellucci, P.; Allegri, V.; Montini, G.C.; Tomassetti, P.; Paganelli, G.; Fanti, S. 68Ga-DOTANOC PET/CT clinical impact in patients with neuroendocrine tumors. J. Nucl. Med. 2010, 51, 669–673. [Google Scholar] [CrossRef] [Green Version]
- Hofland, L.J.; Lamberts, S.W. The pathophysiological consequences of somatostatin receptor internalization and resistance. Endocr. Rev. 2003, 24, 28–47. [Google Scholar] [CrossRef] [Green Version]
- Muffatti, F.; Partelli, S.; Cirocchi, R.; Andreasi, V.; Mapelli, P.; Picchio, M.; Gianolli, L.; Falconi, M. Combined 68Ga-DOTA-peptides and 18F-FDG PET in the diagnostic work-up of neuroendocrine neoplasms (NEN). Clin. Transl. Imaging 2019, 7, 181–188. [Google Scholar] [CrossRef]
- Panzuto, F.; Nasoni, S.; Falconi, M.; Corleto, V.D.; Capurso, G.; Cassetta, S.; Di Fonzo, M.; Tornatore, V.; Milione, M.; Angeletti, S.; et al. Prognostic factors and survival in endocrine tumor patients: Comparison between gastrointestinal and pancreatic localization. Endocr. Relat. Cancer 2005, 12, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.A.; Pampaloni, M.H.; Nakakura, E.; VanBrocklin, H.; Slater, J.; Jivan, S.; Aparici, C.M.; Yee, J.; Bergsland, E. Simultaneous (68)Ga-DOTA-TOC PET/MRI with gadoxetate disodium in patients with neuroendocrine tumor. Abdom. Imaging 2015, 40, 1432–1440. [Google Scholar] [CrossRef] [PubMed]
- Seith, F.; Schraml, C.; Reischl, G.; Nikolaou, K.; Pfannenberg, C.; la Fougère, C.; Schwenzer, N. Fast non-enhanced abdominal examination protocols in PET/MRI for patients with neuroendocrine tumors (NET): Comparison to multiphase contrast-enhanced PET/CT. Radiol. Med. 2018, 123, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, L.M.; Deuschl, C.; Beiderwellen, K.; Ruhlmann, V.; Poeppel, T.D.; Heusch, P.; Lahner, H.; Führer, D.; Bockisch, A.; Herrmann, K.; et al. Evaluation of 68Ga-DOTATOC PET/MRI for whole-body staging of neuroendocrine tumours in comparison with 68Ga-DOTATOC PET/CT. Eur. Radiol. 2017, 27, 4091–4099. [Google Scholar] [CrossRef]
- Mapelli, P.; Ironi, G.; Fallanca, F.; Partelli, S.; Muffatti, F.; Andreasi, V.; Gianolli, L.; Falconi, M.; De Cobelli, F.; Picchio, M. 68Ga-DOTA-peptides PET/MRI in pancreatico-duodenal neuroendocrine tumours: A flash pictorial essay on assets and lacks. Clin. Transl. Imaging 2019, 7, 363–371. [Google Scholar] [CrossRef]
- Berzaczy, D.; Giraudo, C.; Haug, A.R.; Raderer, M.; Senn, D.; Karanikas, G.; Weber, M.; Mayerhoefer, M.E. Whole-Body 68Ga-DOTANOC PET/MRI Versus 68Ga-DOTANOC PET/CT in Patients with Neuroendocrine Tumors: A Prospective Study in 28 Patients. Clin. Nucl. Med. 2017, 42, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Adams, L.C.; Bressem, K.K.; Brangsch, J.; Reimann, C.; Nowak, K.; Brenner, W.; Makowski, M.R. Quantitative 3D assessment of 68Ga-DOTATOC PET/MRI with diffusion-weighted imaging to assess imaging markers for gastroendopancreatic neuroendocrine tumors: Preliminary results. J. Nucl. Med. 2020, 61, 1021–1027. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Characteristics | Patients Characteristics | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Year | Journal | Country | Study Design | Setting | N Pancreas/N Patients | Mean Age (Range) | Grading | Type of Treatment (n) | Detection of Suspected pNET-Diagnosis n | Staging n |
| [22] | 2007 | J Nucl Med | Austria | prospective | diagnosis, staging, restaging | 18/84 | 58 (28–79) | nr | 6 surgery 7 surgery + chemotherapy 16 surgery + long-acting somatostatin analogs | 13 | 36 |
| [23] | 2009 | J Nucl Med | Austria | retrospective | staging and restaging | 11/51 | Nr (32–87) | nr | nr | 0 | 11 |
| [24] | 2010 | Clin Nucl Med | Italy | retrospective | diagnosis | 11/19 | 56 (21–80) | 9 WDET 4 WDEC | none | 11 | 0 |
| [25] | 2010 | J Nucl Med | UK | retrospective | staging, restaging | 13/51 | 55.5 | 28 G1 19 G2 4 G3 | 9 surgery 10 Chemotherapy 27 long-acting somatostatin analogs 5 none | 0 | 13 |
| [26] | 2010 | Ann Surg | Germany | prospective | diagnosis, staging | 27/52 | 52 (24–76) | 51 G1-G2 1 G3 | none | 1 | 26 |
| [27] | 2010 | EJNMMI | Germany-Italy | retrospective | diagnosis | 16/59 | 65 | 16 G1 2 G2 4 G3 13 nr | none | 16 | 0 |
| [28] | 2010 | Neuro endocrinology | Germany | retrospective | diagnosis, staging, restaging | 18/66 | 56 (29–79) | nr | 33 surgery 5 surgery + chemotherapy 4 surgery + long-acting somatostatin analogs 2 long-acting somatostatin analogs 2 long-acting somatostatin analogs + chemotherapy 2 surgery + long-acting somatostatin analogs + chemotherapy 1 chemotherapy 17 none | nr | nr |
| [29] | 2011 | Eur Radiol | India | retrospective | diagnosis and staging | 20/20 | 42.5* | nr | none | 17 | 3 |
| [30] | 2011 | AJR | India | prospective | staging, restaging | 26/109 | 50* (21–76) | nr | 60 none 30 surgery 11 surgery + long-acting somatostatin analogs 5 long-acting somatostatin analogs 2 surgery + chemotherapy or radiotherapy 1 long-acting somatostatin analogs + chemotherapy | 0 | 26 |
| [31] | 2012 | Clin Nucl Med | Israel | retrospective | diagnosis, treatment response evaluation, detection of SSTR expression | 40/96 | 59 (16–89) | nr | Nr | 0 | 40 |
| [32] | 2012 | Eur Radiol | Austria | retrospective | diagnosis, staging, restaging | 19/55 | 62 (37–80) | 34 G1 10 G2 4 G3 | nr | 19 | 0 |
| [33] | 2012 | EJNMMI | Italy | retrospective | staging, restaging | 10/131 | nr | nr | nr | 10 | 0 |
| [34] | 2013 | EJNMMI | Austria | retrospective | staging and restaging | 22/249 | 59.5 (15–90) | nr | nr | nr | nr |
| [35] | 2013 | EJNMMI | Germany | retrospective | diagnosis | 18/18 | 56 (26–80) | nr | 6 surgery other nr | 18 | 0 |
| [10] | 2013 | Recent Results Cancer Res | Germany | prospective | before PRRT | 9/27 | 62 (46–81) | 7 surgery 7 surgery + chemotherapy + PRRT 5 surgery + long-acting somatostatin analogs 2 none 6 other | 9 | 0 | |
| [36] | 2014 | Clin Nucl Med | Poland | retrospective | staging or restaging after surgery | 56/245 | 56 (18–78) | G1: 103 G2: 142 | 35 surgery 12 PRRT 6 chemotherapy 16 long-acting somatostatin analogs | 0 | 56 |
| [37] | 2014 | Nucl Med Comm | United Kingdom | retrospective | diagnosis, restaging after surgery, treatment response evaluation, detection of SSTR expression | 38/138 | 56 (20–84) | nr | nr | 0 | 38 |
| [38] | 2015 | Pancreas | Germany | retrospective | staging | 19/19 | 58 (33–72) | G1: 3 G2: 15 G3: 1 | Pre-operative | 0 | 19 |
| [19] | 2015 | J Am Coll Surg | USA | prospective | staging, restaging | 26/26 | 42 (19–82) | nr | 10 surgery 16 none | 12 | 14 |
| [39] | 2015 | Ann Surg Oncol | Germany | prospective | staging | 18/44 | 56* (32–77) | nr (but all G1-G2) | Pre surgery | 0 | 18 |
| [40] | 2015 | J Nucl Med | Denmark | prospective | staging, restaging | 11/59 | 61 (32–81) | G1: 12 G2: 40 7 nr | 32 surgery ** 32 long-acting ** somatostatin analogs 27 interferon ** 19 PRRT ** 16 chemotherapy ** | 0 | 11 |
| [41] | 2015 | Abdom Imaging | India | retrospective | staging, restaging | 141/141 | 46 (6–81) | nr | nr | 88 | 0 |
| [42] | 2015 | J Nucl Med | UK | retrospective | all | 142/728 | 54 (15–86) | 260 G1 89 G2 63 G3 | nr | nr | nr |
| [43] | 2016 | EJNMMI | Germany | prospective | diagnosis | 20/20 | 45 (22–64) | nr | nr | 20 | 0 |
| [20] | 2016 | Endocrine | Italy | prospective | diagnosis | 11/18 | 40 (16–61) | nr | nr | 11 | 0 |
| [17] | 2016 | Pancreas | Italy | retrospective | staging, treatment response evaluation | 25/25 | 58 (27–84) | G1: 7 G2: 7 G3: 2 nr: 9 | 16 naive 6 SST analogs 1 PRRT1 PRRT + Chemotherapy 1 PRRT+SST analogs | 0 | 25 |
| [21] | 2016 | EJNMMI | France | prospective | diagnosis and restaging | 19/19 | 47 (26–70) | nr | surgery | 4 | 15 |
| [44] | 2016 | J Nucl Med | USA | prospective | diagnosis, staging, treatment response | 22/97 (gastro-entero-pancreatic) | 54 | 24 G1 37 G2 6 G3 30 nr | 51 long-acting somatostatin analogs other nr | 0 | 22 |
| [45] | 2016 | Eur Radiol | Germany | retrospective | diagnosis, staging | 12/38 | 63 (34–76) | 16 G1 8 G2 | none | 12 | 0 |
| [46] | 2016 | JCO | USA | prospective | diagnosis | 31/131 | 51 (19–82) | nr | none | 31 | 0 |
| [47] | 2016 | Clin Radiol | Japan | retrospective | diagnosis, staging, restaging | 19/54 | 55 (27–81) | nr | nr | 8 | 20 |
| [16] | 2017 | J Clin Endocrinol Metab | Switzerland | retrospective | diagnosis | 10/31 | 57.5* (21.75) | G1: 8 G2: 1 | surgery | 10 | 0 |
| [48] | 2017 | Pancreas | Italy | retrospective | diagnosis | 35/35 | 59 (41–84) | G1: 10 G2: 25 | surgery | 35 | 0 |
| [49] | 2017 | EJSO | Italy | prospective | diagnosis, prognostication | 124/124 | 55 | 6 G1 69 G2 5 G3 | 63 surgery 61 none | 0 | 124 |
| [50] | 2018 | J Formos Med Assoc | Taiwan | prospective | diagnosis | 10/17 | 56 (24–84) | G1: 6 G2: 7 G3: 1 3 nr | None | 10 | 0 |
| [51] | 2019 | AOJNMB | Turkey | retrospective | staging metastases detection | 19/38 | 50* (27–80) | 18 G1 20 G2 | nr | 0 | 19 |
| [18] | 2019 | Eur J Radiol | USA | prospective | diagnosis | 36/36 | 46 | nr | nr | 36 | 0 |
| [52] | 2019 | EJNMMI Research | Finland | prospective | diagnosis, prognostication | 31/31 | 60 (20–83) | 13 G1 8 G2 1 G3 | nr | 0 | 31 |
| Reference | Device | Radiotracer (Peptide) | Activity Injected MBq Mean (Range) | Uptake Time Min Mean (Range) | PET Analysis | Semiquantitative Parameters | SUVmax Mean (Range) |
|---|---|---|---|---|---|---|---|
| [22] | PET | DOTATOC | 150 | 20, 60, 100 | visual and semiquantitative | SUVmax | nr |
| [23] | PET/CT | DOTATOC | 150 | 60–90 | visual | / | / |
| [24] | PET/CT | DOTATOC | 1.5–2 MBq/Kg | 60 | visual | / | / |
| [25] | PET/CT | DOTATATE | 120–200 | 60 | visual | / | / |
| [26] | PET/CT | DOTATOC | 120–250 | 60 | visual and semiquantitative | SUVmax | nr |
| [27] | PET/CT | DOTANOC | 100 (46–260) | 60 | visual and semiquantitative | SUVmax | 18.6 (7.8–34.8) |
| [28] | PET & PET/CT | DOTATOC | 100–120 | 60 | visual | / | / |
| [29] | PET/CT | DOTATOC | 132–222 | 30–45 | visual and semiquantitative | SUVmax | 12.6 (8.8–27.6) only in pancreas |
| [30] | PET/CT | DOTANOC | 132–222 | 45–60 | visual and semiquantitative | SUVmax | 13 * (1–125) |
| [31] | PET/CT | DOTANOC | 132 (77–196) | 73 (50–120) | visual and semiquantitative | SUVmax | 26 (5.5–165) |
| [32] | PET/CT | DOTATOC | 150 | 90 | visual | / | / |
| [33] | PET/CT | DOTANOC | 120–185 | 60 | visual | / | / |
| [34] | PET/CT | DOTATOC | 119 (68–220) | 87 (51–148) | visual and semiquantitative | SUVmax | 34.6 only in pancreas |
| [35] | PET/CT | DOTATATE | 200 | 60 | visual and semiquantitative | SUVmax | 36.5 |
| [10] | PET and PET/CT | DOTATOC and DOTATATE | 88 (52–111) 102 (60–123) | 68 (29–162) 56 (24–161) | visual and semiquantitative | SUVmax | 37.4 19.6 |
| [36] | PET/CT | DOTATATE | 156 (120–200) | 60–70 | visual and semiquantitative | SUVmax | 24.9 only in pancreas |
| [37] | PET/CT | DOTATATE | 117 (51–212) | 24–44 | visual and semiquantitative | SUVmax | 32 (10–151) |
| [38] | PET/CT | DOTATOC or DOTANOC or DOTATATE | 122 (86–149) | 60 | visual and semiquantitative | SUVmax; SUVmean | 22.5 (5.7–100.4) |
| [19] | PET/CT | DOTATATE | 185 | 60 | visual and semiquantitative | SUVmax | 72.8 (19,2–191) |
| [39] | PET/CT | DOTATATE | 200 | 60 | visual | / | / |
| [40] | PET/CT | DOTATOC and DOTATATE° | 150 200 | 45 60 | visual and semiquantitative | SUVmax; TBR | 44.5 61.2 |
| [41] | PET/CT | DOTANOC | 132–222 | 45–60 | visual and semiquantitative | SUVmax | 14.7 (5–32.5) only in pancreas |
| [42] | PET/CT | DOTATATE | 250 | 45–60 | visual | / | / |
| [43] | PET/CT | DOTATOC | 1.7 MBq/Kg | 45–60 | visual and semiquantitative | SUVmax | 18.9 (5–65.6) |
| [20] | PET/CT | DOTATATE | 120–220 | 45–60 | visual and semiquantitative | SUVmax | 28 (3.9–85.8) only in pancreas |
| [17] | PET/CT | DOTANOC | 2.5 MBq/Kg | 60 | visual and semiquantitative | SUVmax | 14.6 (4.2–82.9) |
| [21] | PET/CT | DOTATOC | 97 (74–124) | 60 | visual | / | / |
| [44] | PET/CT | DOTATATE | 196 | 55–93 | visual | / | / |
| [45] | PET/CT | DOTATATE | 206 (127–302) | 60 | visual and semiquantitative | SUVmax; tumor to spleen ratio | 26.5 (5.7–77.9) |
| [46] | PET/CT | DOTATATE | 185 | 60 | visual and semiquantitative | SUVmax | 65.4 (6.9–244) |
| [47] | PET/CT | DOTATOC | 11–185 | 64 (55–75) | visual and semiquantitative | SUVmax; tumor to pancreas ratio | 31.7 |
| [16] | PET/CT | DOTATATE | 185 | 60 | visual and semiquantitative | SUVmax | nr |
| [48] | PET/CT | DOTATOC | 1.5 MBq/Kg | 60 | visual and semiquantitative | SUVmax | 45.6 (2–178) |
| [49] | PET/CT | DOTANOC | nr | nr | visual | / | / |
| [50] | PET/CT | DOTATOC | 74–185 | 60 | visual and semiquantitative | SUVmax; SUVmean, MTV; TLG | 53.8 (23,8–96) G1 11.5 (4.1–61.8) G2–3 |
| [51] | PET/CT | DOTATATE | 2 MBq/Kg | 60 | visual and semiquantitative | SUVmax | 18.5 Only in pancreas |
| [18] | PET/CT | DOTATATE | 185 | 60 | visual and semiquantitative | SUVmax | nr |
| [52] | PET/CT | DOTANOC | 143 | 64 | visual and semiquantitative | SUVmax | (8.7–104.7) |
| Sensitivity (95%CI) | Pooled Specificity (95%CI) | LR+ (95%CI) | LR– (95%CI) | DOR (95%CI) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pooled | I2 (%) | X2 (p) | Pooled | I2 (%) | X2 (p) | Pooled | I2 (%) | X2 (p) | Pooled | I2 (%) | X2 (p) | Pooled | I2 (%) | X2 (p) | |
| Patients-based analysis | 79.6% (71–87) | 59.6% | 4.95 (0.08) | 95% (75–100) | 51.5% | 4.12 (0.13) | 5.76 (1.4–24.3) | 21% | 2.53 (0.28) | 0.201 (0.06–0.70) | 64% | 5.56 (0.06) | 35.6 (4.67–270.9) | 21% | 2.52 (0.28) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauckneht, M.; Albano, D.; Annunziata, S.; Santo, G.; Guglielmo, P.; Frantellizzi, V.; Branca, A.; Ferrari, C.; Vento, A.; Mirabile, A.; et al. Somatostatin Receptor PET/CT Imaging for the Detection and Staging of Pancreatic NET: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 598. https://doi.org/10.3390/diagnostics10080598
Bauckneht M, Albano D, Annunziata S, Santo G, Guglielmo P, Frantellizzi V, Branca A, Ferrari C, Vento A, Mirabile A, et al. Somatostatin Receptor PET/CT Imaging for the Detection and Staging of Pancreatic NET: A Systematic Review and Meta-Analysis. Diagnostics. 2020; 10(8):598. https://doi.org/10.3390/diagnostics10080598
Chicago/Turabian StyleBauckneht, Matteo, Domenico Albano, Salvatore Annunziata, Giulia Santo, Priscilla Guglielmo, Viviana Frantellizzi, Alessia Branca, Cristina Ferrari, Antonio Vento, Alessia Mirabile, and et al. 2020. "Somatostatin Receptor PET/CT Imaging for the Detection and Staging of Pancreatic NET: A Systematic Review and Meta-Analysis" Diagnostics 10, no. 8: 598. https://doi.org/10.3390/diagnostics10080598