A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases—Actual Applications and Future Perspectives

 and
and
Abstract
:1. Introduction
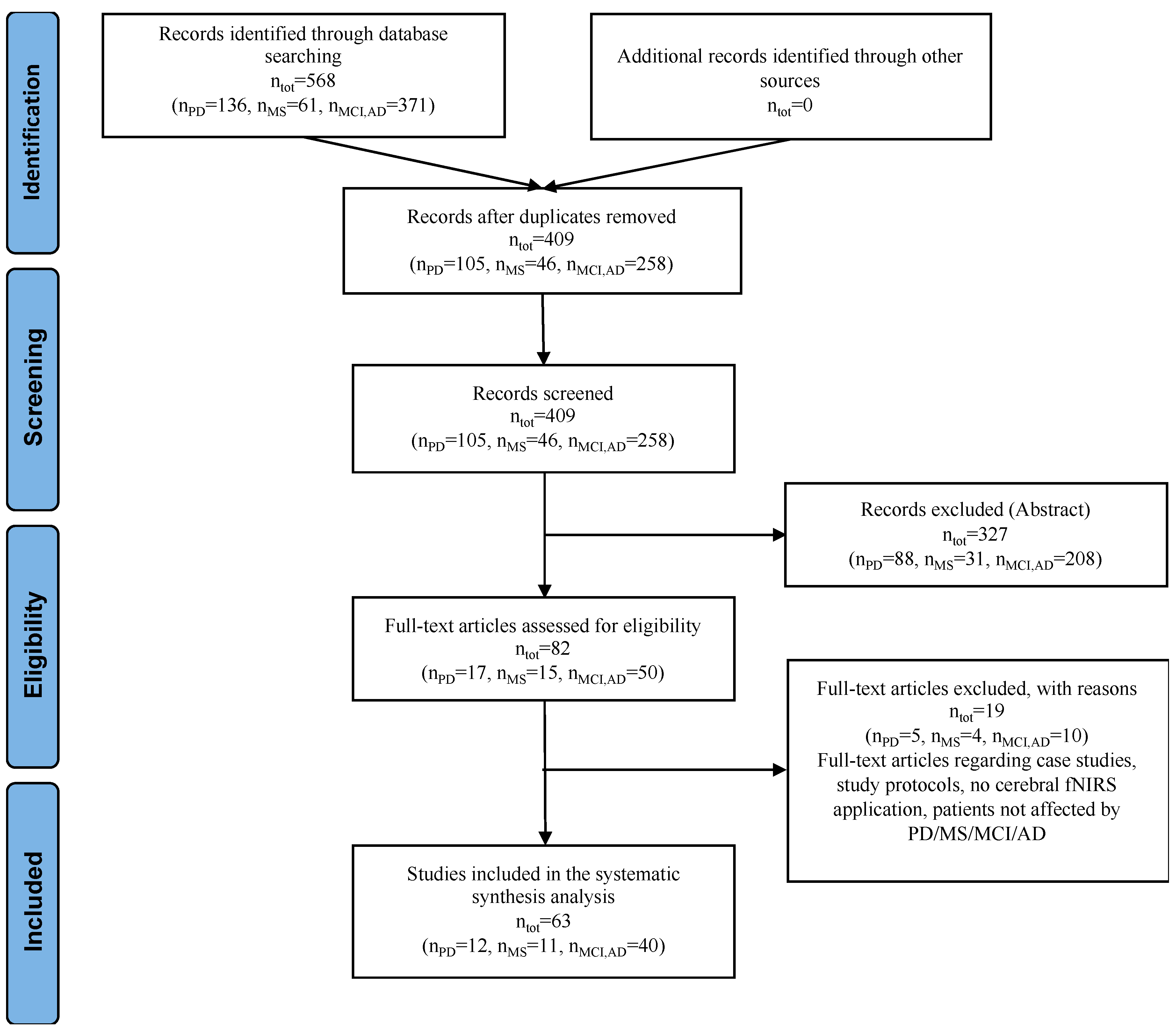
2. Methods
3. fNIRS in Parkinson’s Disease
3.1. Deep Brain Stimulation
3.2. Walking and Dual Walking Task
4. fNIRS in Alzheimer’s Disease and Mild Cognitive Impairment
4.1. Tissue Oxygenation Monitoring
4.2. Functional Resting-State
4.3. Cognitive Tasks–Memory Task
4.4. Cognitive Tasks–Verbal Fluency Task
4.5. Cognitive Tasks–Visuospatial Task
4.6. Ecological Applications
4.7. Longitudinal Monitoring
5. fNIRS in Multiple Sclerosis
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- He, W.; Goodkind, D.; Kowal, P. An Aging World: 2015; International Population Reports; United States Census Bureau: Washington, DC, USA, 2016.
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [Green Version]
- Chang, A.Y.; Skirbekk, V.F.; Tyrovolas, S.; Kassebaum, N.J.; Dieleman, J.L. Measuring population ageing: An analysis of the Global Burden of Disease Study 2017. Lancet Public Health 2019, 4, e159–e167. [Google Scholar] [CrossRef] [Green Version]
- Kehler, D.S. Age-related disease burden as a measure of population ageing. Lancet Public Health 2019, 4, e123–e124. [Google Scholar] [CrossRef] [Green Version]
- Stucki, G.; Bickenbach, J.; Gutenbrunner, C.; Melvin, J. Rehabilitation: The health strategy of the 21st century. J. Rehabil. Med. 2018, 50, 309–316. [Google Scholar] [CrossRef] [Green Version]
- Carmeli, E. Physical Therapy for Neurological Conditions in Geriatric Populations. Front. Public Health 2017, 5, 333. [Google Scholar] [CrossRef] [Green Version]
- Poulos, C.J.; Bayer, A.; Beaupre, L.; Clare, L.; Poulos, R.G.; Wang, R.H.; Zuidema, S.; McGilton, K.S. A comprehensive approach to reablement in dementia. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2017, 3, 450–458. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; Donnell, M.O.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2014, 385, 549–562. [Google Scholar] [CrossRef]
- Chatterji, S.; Byles, J.; Cutler, D.; Seeman, T.; Verdes, E. Health, functioning, and disability in older adults—Present status and future implications. Lancet 2015, 385, 563–575. [Google Scholar] [CrossRef] [Green Version]
- Stucki, G.; Reinhardt, J.D.; Grimby, G. Organizing human functioning and rehabilitation research into distinct scientific fields. Part II: Conceptual descriptions and domains for research. J. Rehabil. Med. 2007, 39, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Straudi, S.; Basaglia, N. Neuroplasticity-Based Technologies and Interventions for Restoring Motor Functions in Multiple Sclerosis; Springer LLC: New York, NY, USA, 2017; pp. 171–185. [Google Scholar]
- Petzinger, G.M.; Fisher, B.E.; McEwen, S.; Beeler, J.A.; Walsh, J.P.; Jakowec, M.W. Exercise-enhanced neuroplasticity targeting motor and cognitive circuitry in Parkinson’s disease. Lancet Neurol. 2013, 12, 716–726. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Amatya, B.; Galea, M.P.; Gonzenbach, R.; Kesselring, J. Neurorehabilitation: Applied neuroplasticity. J. Neurol. 2017, 264, 603–615. [Google Scholar] [CrossRef]
- Uludağ, K.; Roebroeck, A. General overview on the merits of multimodal neuroimaging data fusion. Neuroimage 2014, 102, 3–10. [Google Scholar] [CrossRef]
- Risacher, S.L.; Saykin, A.J. Neuroimaging biomarkers of neurodegenerative diseases and dementia. Semin. Neurol. 2013, 33, 386–416. [Google Scholar] [CrossRef] [Green Version]
- Moon, Y.; Sung, J.H.; An, R.; Hernandez, M.E.; Sosnoff, J.J. Gait variability in people with neurological disorders: A systematic review and meta-analysis. Hum. Mov. Sci. 2016, 47, 197–208. [Google Scholar] [CrossRef]
- Allali, G.; Blumen, H.M.; Devanne, H.; Pirondini, E.; Delval, A.; Van De Ville, D. Brain imaging of locomotion in neurological conditions. Neurophysiol. Clin. 2018, 48, 337–359. [Google Scholar] [CrossRef]
- Küçükdeveci, A.A.; Tennant, A.; Grimby, G.; Franchignoni, F. Strategies for assessment and outcome measurement in physical and rehabilitation medicine: An educational review. J. Rehabil. Med. 2011, 43, 661–672. [Google Scholar] [CrossRef] [Green Version]
- Scarapicchia, V.; Brown, C.; Mayo, C.; Gawryluk, J.R. Functional magnetic resonance imaging and functional near-infrared spectroscopy: Insights from combined recording studies. Front. Hum. Neurosci. 2017, 11, 419. [Google Scholar] [CrossRef]
- Yücel, M.A.; Selb, J.J.; Huppert, T.J.; Franceschini, M.A.; Boas, D.A. Functional Near Infrared Spectroscopy: Enabling routine functional brain imaging. Curr. Opin. Biomed. Eng. 2017, 4, 78–86. [Google Scholar] [CrossRef]
- Delpy, D.T.; Cope, M.; Van Der Zee, P.; Arridge, S.; Wray, S.; Wyatt, J. Estimation of optical pathlength through tissue from direct time of flight measurement. Phys. Med. Biol. 1988, 33, 1433. [Google Scholar] [CrossRef] [Green Version]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85, 6–27. [Google Scholar] [CrossRef]
- Torricelli, A.; Contini, D.; Pifferi, A.; Caffini, M.; Re, R.; Zucchelli, L.; Spinelli, L. Time domain functional NIRS imaging for human brain mapping. Neuroimage 2014, 85, 28–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantini, S.; Sassaroli, A. Frequency-Domain Techniques for Cerebral and Functional Near-Infrared Spectroscopy. Front. Neurosci. 2020, 14, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, M.; Quaresima, V. A brief review on the history of human functional near-infrared spectroscopy (fNIRS) development and fields of application. Neuroimage 2012, 63, 921–935. [Google Scholar] [CrossRef]
- Mihara, M.; Miyai, I. Review of functional near-infrared spectroscopy in neurorehabilitation. Neurophotonics 2016, 3, 031414. [Google Scholar] [CrossRef] [PubMed]
- Cutini, S.; Moro, S.B.; Bisconti, S. Review: Functional near infrared optical imaging in cognitive neuroscience: An introductory review. J. Near Infrared Spectrosc. 2012, 20, 75–92. [Google Scholar] [CrossRef]
- Gramigna, V.; Pellegrino, G.; Cerasa, A.; Cutini, S.; Vasta, R.; Olivadese, G.; Martino, I.; Quattrone, A. Near-Infrared Spectroscopy in Gait Disorders: Is It Time to Begin? Neurorehabil. Neural Repair 2017, 31, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Pinti, P.; Tachtsidis, I.; Hamilton, A.; Hirsch, J.; Aichelburg, C.; Gilbert, S.; Burgess, P.W. The present and future use of functional near-infrared spectroscopy (fNIRS) for cognitive neuroscience. Ann. N. Y. Acad. Sci. 2018, 40, 1–25. [Google Scholar] [CrossRef]
- Hocke, L.M.; Oni, I.K.; Duszynski, C.C.; Corrigan, A.V.; Frederick, B.D.; Dunn, J.F. Automated processing of fNIRS data—A visual guide to the pitfalls and consequences. Algorithms 2018, 11, 67. [Google Scholar] [CrossRef] [Green Version]
- Jacques, S.L. Optical properties of biological tissues: A review. Phys. Med. Biol. 2013, 58, R37. [Google Scholar] [CrossRef]
- Tachtsidis, I.; Scholkmann, F. Publisher’s note: False positives and false negatives in functional near-infrared spectroscopy: Issues, challenges, and the way forward. Neurophotonics 2016, 3, 039801. [Google Scholar] [CrossRef] [Green Version]
- Pfeifer, M.D.; Scholkmann, F.; Labruyère, R. Signal processing in functional near-infrared spectroscopy (fNIRS): Methodological differences lead to different statistical results. Front. Hum. Neurosci. 2018, 11, 641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strangman, G.E.; Li, Z.; Zhang, Q. Depth Sensitivity and Source-Detector Separations for Near Infrared Spectroscopy Based on the Colin27 Brain Template. PLoS ONE 2013, 8, e66319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Yang, Z.; Yuan, T.; Feng, W.; Wang, P. A systemic review of functional near-infrared spectroscopy for stroke: Current application and future directions. Front. Neurol. 2019, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Obrig, H. NIRS in clinical neurology—A ‘promising’ tool? Neuroimage 2014, 85, 535–546. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin. Neurophysiol. 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Fujimoto, H.; Mihara, M.; Hattori, N.; Hatakenaka, M.; Kawano, T.; Yagura, H.; Miyai, I.; Mochizuki, H. Cortical changes underlying balance recovery in patients with hemiplegic stroke. Neuroimage 2014, 85, 547–554. [Google Scholar] [CrossRef]
- Brunetti, M.; Morkisch, N.; Fritzsch, C.; Mehnert, J.; Steinbrink, J.; Niedeggen, M.; Dohle, C. Potential determinants of efficacy of mirror therapy in stroke patients—A pilot study. Restor. Neurol. Neurosci. 2015, 33, 421–434. [Google Scholar] [CrossRef] [Green Version]
- Saita, K.; Morishita, T.; Arima, H.; Hyakutake, K.; Ogata, T.; Yagi, K.; Shiota, E.; Inoue, T. Biofeedback effect of hybrid assistive limb in stroke rehabilitation: A proof of concept study using functional near infrared spectroscopy. PLoS ONE 2018, 13, e0191361. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; Collado-Mateo, D.; et al. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [Green Version]
- Alves, G.; Pedersen, K.F.; Pedersen, K.F. Epidemiology of Parkinson’s disease Epidemiology of Parkinson’s disease. J. Neurol. 2008, 5, 525–535. [Google Scholar]
- Kalia, L.V.; Lang, A.E. Parkinson’s disease. Lancet 2015, 386, 896–912. [Google Scholar] [CrossRef]
- Kalia, L.V.; Lang, A.E. Parkinson disease in 2015: Evolving basic, pathological and clinical concepts in PD. Nat. Rev. Neurol. 2016, 12, 65–66. [Google Scholar] [CrossRef] [PubMed]
- De Pablo-Fernández, E.; Lees, A.J.; Holton, J.L.; Warner, T.T. Prognosis and Neuropathologic Correlation of Clinical Subtypes of Parkinson Disease. JAMA Neurol. 2019, 76, 470–479. [Google Scholar] [CrossRef]
- Sakatani, K.; Katayama, Y.; Yamamoto, T.; Suzuki, S. Changes in cerebral blood oxygenation of the frontal lobe induced by direct electrical stimulation of thalamus and globus pallidus: A near infrared spectroscopy study. J. Neurol. Neurosurg. Psychiatry 1999, 67, 769–773. [Google Scholar] [CrossRef] [Green Version]
- Morishita, T.; Higuchi, M.; Saita, K.; Tsuboi, Y.; Abe, H. Changes in Motor-Related Cortical Activity Following Deep Brain Stimulation for Parkinson’s Disease Detected by Functional Near Infrared Spectroscopy: A Pilot Study. Front. Hum. Neurosci. 2016, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mayer, J.S.; Neimat, J.; Folley, B.S.; Bourne, S.K.; Konrad, P.E.; Charles, D.; Park, S. Deep Brain Stimulation of the Subthalamic Nucleus Alters Frontal Activity during Spatial Working Memory Maintenance of Patients with Parkinson’s Disease. Neurocase 2016, 22, 369–378. [Google Scholar] [CrossRef] [Green Version]
- Eggebrecht, A.T.; Ferradal, S.L.; Robichaux-viehoever, A.; Hassanpour, M.S.; Dehghani, H.; Snyder, A.Z.; Hershey, T.; Culver, J.P. Mapping distributed brain function and networks with diffuse optical tomography. Nat. Photonics 2014, 8, 448–454. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, J.R.; Holtzer, R.; Izzetoglu, M.; Zemon, V.; Verghese, J.; Allali, G. The role of prefrontal cortex during postural control in Parkinsonian syndromes a functional near-infrared spectroscopy study. Brain Res. 2016, 1633, 126–138. [Google Scholar] [CrossRef] [Green Version]
- Nieuwhof, F.; Reelick, M.F.; Maidan, I.; Mirelman, A.; Hausdorff, J.M.; Rikkert, M.G.M.O.; Bloem, B.R.; Muthalib, M.; Claassen, J.A.H.R. Measuring prefrontal cortical activity during dual task walking in patients with Parkinson’s disease: Feasibility of using a new portable fNIRS device. Pilot Feasibility Stud. 2016, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Cornejo, P.; Maidan, I.; Brozgol, M.; Shustak, S.; Gazit, E.; Shema, S.; Bernad-elazari, H.; Beck, Y.; Giladi, N. Treadmill walking reduces pre-frontal activation in patients with Parkinson’s disease. Gait Posture 2018, 62, 384–387. [Google Scholar]
- Stuart, S.; Belluscio, V.; Quinn, J.F.; Mancini, M. Pre-frontal Cortical Activity During Walking and Turning Is Reliable and Differentiates Across Young, Older Adults and People With Parkinson’s Disease. Front. Neurol. 2019, 10, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maidan, I.; Bernad, H.; Nir, E.; Hausdorff, J.M. When is Higher Level Cognitive Control Needed for Locomotor Tasks Among Patients with Parkinson’s Disease? Brain Topogr. 2017, 30, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Maidan, I.; Bernad-Elazari, H.; Gazit, E.; Giladi, N.; Hausdorff, J.M.; Mirelman, A. Changes in oxygenated hemoglobin link freezing of gait to frontal activation in patients with Parkinson disease: An fNIRS study of transient motor-cognitive failures. J. Neurol. 2015, 262, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Maidan, I.; Nieuwhof, F.; Bernad-elazari, H.; Bloem, B.R.; Giladi, N.; Hausdorff, J.M.; Claassen, J.A.H.R.; Mirelman, A. Evidence for Differential Effects of 2 Forms of Exercise on Prefrontal Plasticity During Walking in Parkinson’s Disease. Neurorehabil. Neural Repair 2018, 32, 200–208. [Google Scholar] [CrossRef]
- Maidan, I.; Nieuwhof, F.; Bernad-elazari, H.; Reelick, M.F.; Bloem, B.R.; Giladi, N.; Deutsch, J.E.; Hausdorff, J.M.; Claassen, J.A.H.; Mirelman, A. The Role of the Frontal Lobe in Complex Walking Among Patients With Parkinson’s Disease and Healthy Older Adults: An fNIRS Study. Neurorehabil. Neural Repair 2016, 30, 963–971. [Google Scholar] [CrossRef] [Green Version]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Cummings, J.L.; DeKosky, S.T.; Barberger-Gateau, P.; Delacourte, A.; Frisoni, G.; Fox, N.C.; Galasko, D.; et al. Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 2010, 9, 1118–1127. [Google Scholar] [CrossRef]
- Nichols, E.; Szoeke, C.E.I.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W.; et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [Green Version]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Kirova, A.-M.; Bays, R.B.; Lagalwar, S. Working Memory and Executive Function Decline across Normal Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. BioMed Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Salimi, S.; Irish, M.; Foxe, D.; Hodges, J.R.; Piguet, O.; Burrell, J.R. Visuospatial dysfunction in Alzheimer’s disease and behavioural variant frontotemporal dementia. J. Neurol. Sci. 2019, 402, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Bu, L.; Huo, C.; Qin, Y.; Xu, G.; Wang, Y.; Li, Z. Effective Connectivity in Subjects with Mild Cognitive Impairment as Assessed Using Functional Near-Infrared Spectroscopy. Am. J. Phys. Med. Rehabil. 2019, 98, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Marmarelis, V.Z.; Shin, D.C.; Tarumi, T.; Zhang, R. Comparison of model-based indices of cerebral autoregulation and vasomotor reactivity using transcranial doppler versus near-infrared spectroscopy in patients with amnestic mild cognitive impairment. J. Alzheimer’s Dis. 2017, 56, 89–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viola, S.; Viola, P.; Buongarzone, M.P.; Fiorelli, L.; Litterio, P. Tissue oxygen saturation and pulsatility index as markers for amnestic mild cognitive impairment: NIRS and TCD study. Clin. Neurophysiol. 2013, 124, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Van Beek, A.H.E.A.; Lagro, J.; Olde-Rikkert, M.G.M.; Zhang, R.; Claassen, J.A.H.R. Oscillations in cerebral blood flow and cortical oxygenation in Alzheimer’s disease. Neurobiol. Aging 2012, 33, 428.e21–428.e31. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Zhu, Y.-S.; Khan, M.A.; Brunk, E.; Martin-Cook, K.; Weiner, M.F.; Cullum, C.M.; Lu, H.; Levine, B.D.; Diaz-Arrastia, R.; et al. Global brain hypoperfusion and oxygenation in amnestic mild cognitive impairment. Alzheimer’s Dement. 2014, 10, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Babiloni, C.; Vecchio, F.; Altavilla, R.; Tibuzzi, F.; Lizio, R.; Altamura, C.; Palazzo, P.; Maggio, P.; Ursini, F.; Ercolani, M.; et al. Hypercapnia affects the functional coupling of resting state electroencephalographic rhythms and cerebral haemodynamics in healthy elderly subjects and in patients with amnestic mild cognitive impairment. Clin. Neurophysiol. 2014, 125, 685–693. [Google Scholar] [CrossRef]
- Bär, K.J.; Boettger, M.K.; Seidler, N.; Mentzel, H.J.; Terborg, C.; Sauer, H. Influence of galantamine on vasomotor reactivity in alzheimer’s disease and vascular dementia due to cerebral microangiopathy. Stroke 2007, 38, 3186–3192. [Google Scholar] [CrossRef] [Green Version]
- Niu, H.; Zhu, Z. Abnormal dynamic functional connectivity and brain states in Alzheimer’s diseases: Functional near-infrared spectroscopy study. Neurophotonics 2019, 6, 025010. [Google Scholar] [CrossRef]
- Zeller, J.B.M.; Katzorke, A.; Müller, L.D.; Breunig, J.; Haeussinger, F.B.; Deckert, J.; Warrings, B.; Lauer, M.; Polak, T.; Herrmann, M.J. Reduced spontaneous low frequency oscillations as measured with functional near-infrared spectroscopy in mild cognitive impairment. Brain Imaging Behav. 2019, 13, 283–292. [Google Scholar] [CrossRef]
- Nguyen, T.; Kim, M.; Gwak, J.; Lee, J.J.; Choi, K.Y.; Lee, K.H.; Kim, J.G. Investigation of brain functional connectivity in patients with mild cognitive impairment: A functional near-infrared spectroscopy (fNIRS) study. J. Biophotonics 2019, 12, e201800298. [Google Scholar] [CrossRef] [PubMed]
- Niu, H.J.; Li, X.; Chen, Y.J.; Ma, C.; Zhang, J.Y.; Zhang, Z.J. Reduced Frontal Activation during a Working Memory Task in Mild Cognitive Impairment: A Non-Invasive Near-Infrared Spectroscopy Study. CNS Neurosci. Ther. 2013, 19, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Yeung, M.K.; Sze, S.L.; Woo, J.; Kwok, T.; Shum, D.H.K.; Yu, R.; Chan, A.S. Reduced Frontal Activations at High Working Memory Load in Mild Cognitive Impairment: Near-Infrared Spectroscopy. Dement. Geriatr. Cogn. Disord. 2016, 42, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Hock, C.; Villringer, K.; Müller-Spahn, F.; Hofmann, M.; Schuh-Hofer, S.; Heekeren, H.; Wenzel, R.; Dirnagl, U.; Villringer, A. Near infrared spectroscopy in the diagnosis of Alzheimer’s disease. Ann. N. Y. Acad. Sci. 1996, 777, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Hock, C.; Villringer, K.; Müller-Spahn, F.; Wenzel, R.; Heekeren, H.; Schuh-Hofer, S.; Hofmann, M.; Minoshima, S.; Schwaiger, M.; Dirnagl, U.; et al. Decrease in parietal cerebral hemoglobin oxygenation during performance of a verbal fluency task in patients with Alzheimer’s disease monitored by means of near-infrared spectroscopy (NIRS)—Correlation with simultaneous rCBF-PET measurements. Brain Res. 1997, 755, 293–303. [Google Scholar] [CrossRef]
- Fallgatter, A.J.; Roesler, M.; Sitzmann, L.; Heidrich, A.; Mueller, T.J.; Strik, W.K. Loss of functional hemispheric asymmetry in Alzheimer’s dementia assessed with near-infrared spectroscopy. Cogn. Brain Res. 1997, 6, 67–72. [Google Scholar] [CrossRef]
- Herrmann, M.J.; Langer, J.B.M.; Jacob, C.; Ehlis, A.C.; Fallgatter, A.J. Reduced prefrontal oxygenation in alzheimer disease during verbal fluency tasks. Am. J. Geriatr. Psychiatry 2008, 16, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Takano, M.; Miyakawa, K.; Ota, T.; Takahashi, T.; Asaka, H.; Kawaguchi, T. A quantitative near-infrared spectroscopy study: A decrease in cerebral hemoglobin oxygenation in Alzheimer’s disease and mild cognitive impairment. Brain Cogn. 2006, 61, 189–194. [Google Scholar] [CrossRef]
- Yeung, M.K.; Sze, S.L.; Woo, J.; Kwok, T.; Shum, D.H.K.; Yu, R.; Chan, A.S. Altered frontal lateralization underlies the category fluency deficits in older adults with mild cognitive impairment: A near-infrared spectroscopy study. Front. Aging Neurosci. 2016, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Yap, K.H.; Ung, W.C.; Ebenezer, E.G.M.; Nordin, N.; Chin, P.S.; Sugathan, S.; Chan, S.C.; Yip, H.L.; Kiguchi, M.; Tang, T.B. Visualizing hyperactivation in neurodegeneration based on prefrontal oxygenation: A comparative study of mild Alzheimer’s disease, mild cognitive impairment, and healthy controls. Front. Aging Neurosci. 2017, 9, 287. [Google Scholar] [CrossRef]
- Doi, T.; Makizako, H.; Shimada, H.; Park, H.; Tsutsumimoto, K.; Uemura, K.; Suzuki, T. Brain activation during dual-task walking and executive function among older adults with mild cognitive impairment: A fNIRS study. Aging Clin. Exp. Res. 2013, 25, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Katzorke, A.; Zeller, J.B.M.; Müller, L.D.; Lauer, M.; Polak, T.; Deckert, J.; Herrmann, M.J. Decreased hemodynamic response in inferior frontotemporal regions in elderly with mild cognitive impairment. Psychiatry Res. Neuroimaging 2018, 274, 11–18. [Google Scholar] [CrossRef]
- Metzger, F.G.; Schopp, B.; Haeussinger, F.B.; Dehnen, K.; Synofzik, M.; Fallgatter, A.J.; Ehlis, A.C. Brain activation in frontotemporal and Alzheimer’s dementia: A functional near-infrared spectroscopy study. Alzheimer’s Res. Ther. 2016, 8, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uemura, K.; Shimada, H.; Doi, T.; Makizako, H.; Tsutsumimoto, K.; Park, H.; Suzuki, T. Reduced prefrontal oxygenation in mild cognitive impairment during memory retrieval. Int. J. Geriatr. Psychiatry 2016, 31, 583–591. [Google Scholar] [CrossRef]
- Kato, Y.; Shoji, Y.; Morita, K.; Inoue, M.; Ishii, Y.; Sato, M.; Yamashita, Y.; Okawa, J.; Uchimura, N. Evaluation of changes in oxyhemoglobin during Shiritori task in elderly subjects including those with Alzheimer’s disease. Psychogeriatrics 2017, 17, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Ateş, F.E.; Cangöz, B.; Özel Kızıl, E.T.; Baskak, B.; Baran, Z.; Özgüven, H.D. Frontal activity during a verbal emotional working memory task in patients with Alzheimer’s disease: A functional near-infrared spectroscopy study. Psychiatry Res. Neuroimaging 2017, 261, 29–34. [Google Scholar] [CrossRef]
- Oboshi, Y.; Kikuchi, M.; Terada, T.; Yoshikawa, E.; Bunai, T.; Ouchi, Y. Alterations in Phase-Related Prefrontal Activation during Cognitive Tasks and Nicotinic α 4β2 Receptor Availability in Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 53, 817–830. [Google Scholar] [CrossRef]
- Li, R.; Nguyen, T.; Potter, T.; Zhang, Y. Dynamic cortical connectivity alterations associated with Alzheimer’s disease: An EEG and fNIRS integration study. NeuroImage Clin. 2019, 21, 101622. [Google Scholar] [CrossRef]
- Li, R.; Rui, G.; Chen, W.; Li, S.; Schulz, P.E.; Zhang, Y. Early Detection of Alzheimer’s Disease Using Non-invasive Near-Infrared Spectroscopy. Front. Aging Neurosci. 2018, 10, 366. [Google Scholar] [CrossRef]
- Perpetuini, D.; Chiarelli, A.M.; Cardone, D.; Filippini, C.; Bucco, R.; Zito, M.; Merla, A. Complexity of frontal cortex fNIRS can support Alzheimer disease diagnosis in memory and visuo-spatial tests. Entropy 2019, 21, 26. [Google Scholar] [CrossRef] [Green Version]
- Perpetuini, D.; Bucco, R.; Zito, M.; Merla, A. Study of memory deficit in Alzheimer’s disease by means of complexity analysis of fNIRS signal. Neurophotonics 2017, 5, 011010. [Google Scholar] [CrossRef] [PubMed]
- Kito, H.; Ryokawa, A.; Kinoshita, Y.; Sasayama, D.; Sugiyama, N.; Ogihara, T.; Yasaki, T.; Hagiwara, T.; Inuzuka, S.; Takahashi, T.; et al. Comparison of alterations in cerebral hemoglobin oxygenation in late life depression and Alzheimer’s disease as assessed by near-infrared spectroscopy. Behav. Brain Funct. 2014, 10, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeller, J.B.M.; Herrmann, M.J.; Ehlis, A.C.; Polak, T.; Fallgatter, A.J. Altered parietal brain oxygenation in alzheimer’s disease as assessed with near-infrared spectroscopy. Am. J. Geriatr. Psychiatry 2010, 18, 433–441. [Google Scholar] [CrossRef]
- Tomioka, H.; Yamagata, B.; Takahashi, T.; Yano, M.; Isomura, A.J.; Kobayashi, H.; Mimura, M. Detection of hypofrontality in drivers with Alzheimer’s disease by near-infrared spectroscopy. Neurosci. Lett. 2009, 451, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, N.; Umemura, T.; Matsunaga, M.; Hirai, T. Effects of movement music therapy with a percussion instrument on physical and frontal lobe function in older adults with mild cognitive impairment: A randomized controlled trial. Aging Ment. Health 2018, 22, 1614–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Beek, A.H.E.A.; Sijbesma, J.C.; Jansen, R.W.M.M.; Rikkert, M.G.M.O.; Claassen, J.A.H.R. Cortical oxygen supply during postural hypotension is further decreased in Alzheimer’s disease, but unrelated to cholinesterase-inhibitor use. J. Alzheimer’s Dis. 2010, 21, 519–526. [Google Scholar] [CrossRef]
- Viola, S.; Viola, P.; Buongarzone, M.P.; Fiorelli, L.; Mattucci, F.; Litterio, P. New brain reperfusion rehabilitation therapy improves cognitive impairment in mild alzheimer’s disease: A prospective, controlled, open-label 12-month study with nirs correlates. Aging Clin. Exp. Res. 2014, 26, 417–425. [Google Scholar] [CrossRef]
- Vermeij, A.; Kessels, R.P.C.; Heskamp, L.; Simons, E.M.F.; Dautzenberg, P.L.J.; Claassen, J.A.H.R. Prefrontal activation may predict working-memory training gain in normal aging and mild cognitive impairment. Brain Imaging Behav. 2017, 11, 141–154. [Google Scholar] [CrossRef] [Green Version]
- Araki, T.; Wake, R.; Miyaoka, T.; Kawakami, K.; Nagahama, M.; Furuya, M.; Limoa, E.; Liaury, K.; Hashioka, S.; Murotani, K.; et al. The effects of combine treatment of memantine and donepezil on Alzheimer’s Disease patients and its relationship with cerebral blood flow in the prefrontal area. Int. J. Geriatr. Psychiatry 2014, 29, 881–889. [Google Scholar] [CrossRef]
- Metzger, F.G.; Ehlis, A.C.; Haeussinger, F.B.; Fallgatter, A.J.; Hagen, K. Effects of cholinesterase inhibitor on brain activation in Alzheimer’s patients measured with functional near-infrared spectroscopy. Psychopharmacology 2015, 232, 4383–4391. [Google Scholar] [CrossRef]
- Polak, T.; Herrmann, M.J.; Müller, L.D.; Zeller, J.B.M.; Katzorke, A.; Fischer, M.; Spielmann, F.; Weinmann, E.; Hommers, L.; Lauer, M.; et al. Near-infrared spectroscopy (NIRS) and vagus somatosensory evoked potentials (VSEP) in the early diagnosis of Alzheimer’s disease: Rationale, design, methods, and first baseline data of the Vogel study. J. Neural Transm. 2017, 124, 1473–1488. [Google Scholar] [CrossRef] [PubMed]
- Capitani, E.; Rosci, C.; Saetti, M.C.; Laiacona, M. Mirror asymmetry of Category and Letter fluency in traumatic brain injury and Alzheimer’s patients. Neuropsychologia 2009, 47, 423–429. [Google Scholar] [CrossRef]
- Ontaneda, D.; Thompson, A.J.; Fox, R.J.; Cohen, J.A. Progressive multiple sclerosis: Prospects for disease therapy, repair, and restoration of function. Lancet 2017, 389, 1357–1366. [Google Scholar] [CrossRef]
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef]
- Khan, F.; Amatya, B. Rehabilitation in Multiple Sclerosis: A Systematic Review of Systematic Reviews. Arch. Phys. Med. Rehabil. 2017, 98, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Beer, S.; Khan, F.; Kesselring, J. Rehabilitation interventions in multiple sclerosis: An overview. J. Neurol. 2012, 259, 1994–2008. [Google Scholar] [CrossRef]
- Saleh, S.; Sandroff, B.M.; Vitiello, T.; Owoeye, O.; Hoxha, A.; Hake, P.; Goverover, Y.; Wylie, G.; Yue, G.; Deluca, J. The Role of Premotor Areas in Dual Tasking in Healthy Controls and Persons With Multiple Sclerosis: An fNIRS Imaging Study. Front. Behav. Neurosci. 2018, 12, 296. [Google Scholar] [CrossRef] [Green Version]
- Jimenez, J.J.; Golestani, A.; Goodyear, B.G.; Metz, L.M.; Dunn, J.F. Detection of reduced interhemispheric cortical communication during task execution in multiple sclerosis patients using functional near-infrared spectroscopy Detection of reduced interhemispheric cortical. J. Biomed. Opt. 2019, 19, 076008. [Google Scholar] [CrossRef]
- Borragán, G.; Gilson, M.; Atas, A.; Slama, H. Cognitive Fatigue, Sleep and Cortical Activity in Multiple Sclerosis Disease. A Behavioral, Polysomnographic and Functional Near-Infrared Spectroscopy Investigation. Front. Hum. Neurosci. 2018, 12, 378. [Google Scholar] [CrossRef]
- Wolff, W.; Schüler, J.; Hofstetter, J.; Baumann, L.; Wolf, L.; Dettmers, C. Trait Self-Control Outperforms Trait Fatigue in Predicting MS Patients ’ Cortical and Perceptual Responses to an Exhaustive Task. Neural Plast. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Stojanovic-Radic, J.; Wylie, G.; Voelbel, G. Neuroimaging and cognition using functional near infrared spectroscopy (fNIRS) in multiple sclerosis. Brain Imaging Behav. 2015, 9, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.E.; Holtzer, R.; Chaparro, G.; Jean, K.; Balto, J.M.; Sandroff, B.M.; Izzetoglu, M.; Motl, R.W. Brain activation changes during locomotion in middle-aged to older adults with multiple sclerosis. J. Neurol. Sci. 2016, 370, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, G.; Balto, J.M.; Sandroff, B.M.; Holtzer, R.; Izzetoglu, M.; Motl, R.W.; Hernandez, M.E. Frontal brain activation changes due to dual-tasking under partial body weight support conditions in older adults with multiple sclerosis. J. Neuroeng. Rehabil. 2017, 14, 65. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.E.; O’Donnell, E.; Chaparro, G.; Holtzer, R.; Izzetoglu, M.; Sandroff, B.M.; Motl, R.W. Brain Activation Changes During Balance- and Attention-Demanding Tasks in Middle- and Older-Aged Adults With Multiple Sclerosis. Motor Control 2019, 23, 498–517. [Google Scholar] [CrossRef]
- Molinari, F.; Simonetti, V.; Franzinp, M.; Pandolfp, S.; Vaian, F.; Torino, P. Ozone autohemotherapy induces long-term cerebral metabolic changes in multiple sclerosis patients. Int. J. Immunopathol. Pharmacol. 2014, 27, 379–389. [Google Scholar] [CrossRef] [Green Version]
- Molinari, F.; Rimini, D.; Liboni, W.; Acharya, U.R.; Franzini, M.; Pandolfi, S.; Ricevuti, G.; Vaiano, F.; Valdenassi, L.; Simonetti, V. Cerebrovascular pattern improved by ozone autohemotherapy: An entropy—Based study on multiple sclerosis patients. Med. Biol. Eng. Comput. 2017, 55, 1163–1175. [Google Scholar] [CrossRef]
- Yang, R.; Dunn, J.F. Reduced cortical microvascular oxygenation in multiple sclerosis: A blinded, case-controlled study using a novel quantitative near-infrared spectroscopy method. Nat. Publ. Gr. 2015, 5, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Arenth, P.M.; Ricker, J.H.; Schultheis, M.T. Applications of functional near-infrared spectroscopy (fNIRS) to neurorehabilitation of cognitive disabilities. Clin. Neuropsychol. 2007, 21, 38–57. [Google Scholar] [CrossRef]
- Herold, F.; Wiegel, P.; Scholkmann, F.; Müller, N. Applications of Functional Near-Infrared Spectroscopy (fNIRS) Neuroimaging in Exercise—Cognition Science: A Systematic, Methodology-Focused Review. J. Clin. Med. 2018, 7, 466. [Google Scholar] [CrossRef] [Green Version]
- Naseer, N.; Hong, K.S. fNIRS-based brain-computer interfaces: A review. Front. Hum. Neurosci. 2015, 9, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Sachdev, P.S.; Blacker, D.; Blazer, D.G.; Ganguli, M.; Jeste, D.V.; Paulsen, J.S.; Petersen, R.C. Classifying neurocognitive disorders: The DSM-5 approach. Nat. Rev. Neurol. 2014, 10, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Ismail, F.Y.; Fatemi, A.; Johnston, M.V. Cerebral plasticity: Windows of opportunity in the developing brain. Eur. J. Paediatr. Neurol. 2017, 21, 23–48. [Google Scholar] [CrossRef] [PubMed]
- Irani, F.; Platek, S.M.; Bunce, S.; Ruocco, A.C.; Chute, D. Functional near infrared spectroscopy (fNIRS): An emerging neuroimaging technology with important applications for the study of brain disorders. Clin. Neuropsychol. 2007, 21, 9–37. [Google Scholar] [CrossRef]
- Berlingeri, M.; Danelli, L.; Bottini, G.; Sberna, M.; Paulesu, E. Reassessing the HAROLD model: Is the hemispheric asymmetry reduction in older adults a special case of compensatory-related utilisation of neural circuits? Exp. Brain Res. 2013, 224, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Strangman, G.; Franceschini, M.A.; Boas, D.A. Factors affecting the accuracy of near-infrared spectroscopy concentration calculations for focal changes in oxygenation parameters. Neuroimage 2003, 18, 865–879. [Google Scholar] [CrossRef]
- Wheelock, M.D.; Culver, J.P.; Eggebrecht, A.T. High-density diffuse optical tomography for imaging human brain function. Rev. Sci. Instrum. 2019, 90, 1–24. [Google Scholar] [CrossRef]
- Aasted, C.M.; Yücel, M.A.; Cooper, R.J.; Dubb, J.; Tsuzuki, D.; Becerra, L.; Petkov, M.P.; Borsook, D.; Dan, I.; Boas, D.A. Anatomical guidance for functional near-infrared spectroscopy: AtlasViewer tutorial. Neurophotonics 2015, 2, 020801. [Google Scholar] [CrossRef]
- Cooper, R.J.; Caffini, M.; Dubb, J.; Fang, Q.; Custo, A.; Tsuzuki, D.; Fischl, B.; Wells, W.; Dan, I.; Boas, D.A. Validating atlas-guided DOT: A comparison of diffuse optical tomography informed by atlas and subject-specific anatomies. Neuroimage 2012, 62, 1999–2006. [Google Scholar] [CrossRef] [Green Version]
- Pinti, P.; Scholkmann, F.; Hamilton, A.; Burgess, P.; Tachtsidis, I. Current Status and Issues Regarding Pre-processing of fNIRS Neuroimaging Data: An Investigation of Diverse Signal Filtering Methods Within a General Linear Model Framework. Front. Hum. Neurosci. 2019, 12, 505. [Google Scholar] [CrossRef] [Green Version]
- Cramer, S.C.; Sur, M.; Dobkin, B.H.; O’Brien, C.; Sanger, T.D.; Trojanowski, J.Q.; Rumsey, J.M.; Hicks, R.; Cameron, J.; Chen, D.; et al. Harnessing neuroplasticity for clinical applications. Brain 2011, 134, 1591–1609. [Google Scholar] [CrossRef]
- Gottschalk, S.; Fehm, T.F.; Deán-Ben, X.L.; Tsytsarev, V.; Razansky, D. Correlation between volumetric oxygenation responses and electrophysiology identifies deep thalamocortical activity during epileptic seizures. Neurophotonics 2016, 4, 011007. [Google Scholar] [CrossRef]
- Cao, R.; Li, J.; Ning, B.; Sun, N.; Wang, T.; Zuo, Z.; Hu, S. Functional and oxygen-metabolic photoacoustic microscopy of the awake mouse brain. Neuroimage 2017, 150, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Larney, B.; Hutter, M.A.; Degtyaruk, O.; Deán-Ben, X.L.; Razansky, D. Monitoring of Stimulus Evoked Murine Somatosensory Cortex Hemodynamic Activity With Volumetric Multi-Spectral Optoacoustic Tomography. Front. Neurosci. 2020, 14, 536. [Google Scholar] [CrossRef] [PubMed]
- Ovsepian, S.V.; Jiang, Y.; Sardella, T.C.P.; Malekzadeh-Najafabadi, J.; Burton, N.C.; Yu, X.; Ntziachristos, V. Visualizing cortical response to optogenetic stimulation and sensory inputs using multispectral handheld optoacoustic imaging. Photoacoustics 2020, 17, 100153. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.; Zhang, R.; Li, L.; Shao, J.-Y.; Wang, L.V. Photoacoustic imaging of voltage responses beyond the optical diffusion limit. Sci. Rep. 2017, 7, 2560. [Google Scholar] [CrossRef]
- Gottschalk, S.; Degtyaruk, O.; Mc Larney, B.; Rebling, J.; Hutter, M.A.; Deán-Ben, X.L.; Shoham, S.; Razansky, D. Rapid volumetric optoacoustic imaging of neural dynamics across the mouse brain. Nat. Biomed. Eng. 2019, 3, 392–401. [Google Scholar] [CrossRef] [Green Version]
- Degtyaruk, O.; Mc Larney, B.; Deán-Ben, X.L.; Shoham, S.; Razansky, D. Optoacoustic Calcium Imaging of Deep Brain Activity in an Intracardially Perfused Mouse Brain Model. Photonics 2019, 6, 67. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Parkinson’s Disease (PD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| fNIRS Device | Patient Info | Study Type | Integrated Clinical Outcomes | Cortical Areas | Performed Task | Ch. | Multimodal Integration | ||
| Deep Brain Stimulation | Sakatani et al., 1999 | NIRO-300 (Hamamatsu Photonics K.K., Japan) | 5 PD, 1 essential tremor patient | cross-sectional | UPDRS, tremor rating scale | bilateral PFC | tissue oxygenation monitor | 1 | no |
| Morishita et al., 2016 | FOIRE-3000 (Shimadzu Corporation, Kyoto, Japan) | 6 PD | longitudinal | UPDRS | primary motor cortex | unilateral hand movement | 48 | no | |
| Mayer et al., 2016 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 9 PD, 8 HC | cross-sectional (*) | UPDRS | lateral and medial FC (bilateral hemispheres) | spatial-delayed response task (working memory task) | 22 | no | |
| Eggebrecht et al., 2014 | custom HD-DOT system | (18 HC) 3 PD | cross-sectional | n.d. | almost whole-head (temporal, occipital cortex) | auditory words, resting-state | 1200+ | T1- and T2-MRI, fMRI (not performed on PD patients) | |
| Walking and Dual Walking Task | Mahoney et al., 2016 | fNIR Imager 1000 (fNIR Devices LLC, Protomac, MD, USA) | 26 PD, 117 mild PD, 126 HC | cross-sectional | n.d. | PFC | postural stability control task | 16 | instrumented walkway |
| Nieuwhof et al., 2016 | PortLite (Artinis Medical Systems, Elst, The Netherlands) | 14 PD | cross-sectional | n.d. | bilateral PFC | counting forward, serially subtracting, reciting digit spans | 3 | instrumented walkway with pressure sensors | |
| Cornejo et al., 2018 | PortLite (Artinis Medical Systems, The Netherlands) | 20 PD | cross-sectional | n.d. | dorsolateral PFC and anterior PFC (bilateral BA10) | over-ground and treadmill walking | 3 | instrumented treadmill, 3D-accelerometers | |
| Stuart et al., 2019 | Oxymon (Artinis Medical Systems, The Netherlands) | 24 PD, 19 HOA, 25 HYA | cross-sectional | n.d. | PFC (BA9 and BA10) | turning-in-place task | n.d. | no | |
| Maidan et al., 2015 | Oxymon MKIII (Artinis Medical Systems, The Netherlands) | 11 PD, 11 HC | cross-sectional | n.d. | PFC (bilateral BA10) | walking with anticipated and unanticipated turns (WT) | 6 | no | |
| Maidan et al., 2016 | PortLite (Artinis Medical Systems, Elst, The Netherlands) | 68 PD, 38 HC | cross-sectional | n.d. | dorsolateral PFC and anterior PFC (bilateral BA10) | obstacle negotiation, WT, DWT | 3 | instrumented walkway with pressure sensors | |
| Maidan et al., 2017 | PortLite (Artinis Medical Systems, Elst, The Netherlands) | 49 PD | cross-sectional | n.d. | dorsolateral PFC and anterior PFC (bilateral BA10) | usual walking and turning (WT) | 3 | instrumented walkway with pressure sensors | |
| Maidan et al., 2018 | PortLite (Artinis Medical Systems, Elst, The Netherlands) | 64 PD | longitudinal | UPDRS | dorsolateral PFC and anterior PFC (bilateral BA10) | treadmill training (obstacle negotiation, WT, DWT) | 3 | instrumented walkway with pressure sensors | |
| Mild Cognitive Impairment (MCI) and Alzheimer’s Disease (AD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| fNIRS Device | Patient Info | Study Type | Integrated Clinical Outcomes | Cortical Areas | Performed Task | Ch. | Multimodal Integration | ||
| Tissue Oxygenation Monitoring | Marmarelis et al., 2017 | N.D. (Hamamatsu Photonics K.K., Japan) | (46) 38 aMCI, (22) 14 HC | cross-sectional | n.d. | PFC | tissue oxygenation monitor | n.d. | TCD, finger photo-plethysmography, capnography |
| Viola et al., 2013 | custom NIRS device (T-NIRS EVO II) | 21 aMCI, 10 HC | cross-sectional | MMSE | bilateral frontal and parieto-temporal cortex | tissue oxygenation monitor | 1 | TCD | |
| van Beek et al., 2012 | Oxymon (Artinis Medical Systems, Zetten, The Netherlands) | 21 mild to moderate AD, 20 HC | cross-sectional | n.d. | bilateral FC | tissue oxygenation monitor during repeated sit-stand manoeuvres | n.d. | TCD, finger photo-plethysmography, ECG | |
| Liu et al., 2014 | NIRO-200NX (Hamamatsu Photonics K.K., Japan) | 32 aMCI, 21 HC | cross-sectional (**) | n.d. | n.d. | tissue oxygenation monitor | 2 | color-coded duplex ultrasonography, MRI, sphygmomanometer, pulse oximeter, ECG, capnography | |
| Babiloni et al., 2014 | ISS oximeter, Model 96,208 (ISS Inc., Champaign, IL, USA) | 10 aMCI, 10 HC | cross-sectional | MMSE | bilateral PFC | tissue oxygenation monitor under resting-state and hypercapnia conditions | 2 | concurrent NIRS-EEG | |
| Bär et al., 2007 | NIRO-500 (Hamamatsu Photonics K.K., Japan) | 17 AD, 17 vascular dementia patients, 20 HOA, 20 HYA | cross-sectional | MMSE | left FC | tissue oxygenation monitor under normocapnia and hypercapnia conditions | 2 | TCD, finger blood pressure monitor | |
| Functional Resting-State | Niu et al., 2019 | CW6 (TechEn Inc., Milford, MA, USA) | 23 AD, 25 aMCI, 30 HC | cross-sectional | MMSE, AVLT, MoCA | whole-head | resting-state | 46 | no |
| Zeller et al., 2019 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 54 MCI, 61 HOA, 25 HYA | cross-sectional | DemTect, RCFT, RWT, VLMT, TAP, WMS-R | frontal and parietal cortex | resting-state | 96 | no | |
| Bu et al., 2019 | NirSmart (Danyang Huichuang Medical Equipment Co., PR China) | 26 MCI, 28 HC | cross-sectional | MMSE, MoCA | bilateral PFC, motor and occipital cortex | resting-state | 14 | no | |
| Nguyen et al., 2019 | Custom fNIRS device | 42 MCI, 42 HC | cross-sectional | MMSE | PFC | resting-state, oddball task, 1-back task, letter and category fluency task | 4 | no | |
| Cognitive Task - Memory Task | Niu et al., 2013 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 8 aMCI, 16 HC | cross-sectional | MMSE, AVLT, BNT, Stroop Test | bilateral frontal, parietal and temporal cortex | n-back task (WMT) | 54 | no |
| Yeung et al., 2016 | OEG-SpO2 system (Spectratech Inc., Tokyo, Japan) | 10 aMCI, 16 MCI, 26 HC | cross-sectional | n.d. | bilateral PFC | n-back task | 16 | no | |
| Uemura et al., 2016 | FOIRE-3000 (Shimadzu Corporation, Kyoto, Japan) | 64 aMCI, 66 HC | cross-sectional | n.d. | bilateral prefrontal and frontopolar cortex (BA9, 46, 10) | memory encoding and delayed retrieval task | 22 | no | |
| Kato et al., 2017 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 42 AD, 98 intermediate group (65 high score HDS-R/MMSE, 33 low score HDS-R/MMSE), 91 HC | cross-sectional | MMSE, HDS-R, Z-score of VSRAD | FC, dorsolateral PFC, bilateral parietal cortex | single-word presentation task | 44 | MRI | |
| Ateş et al., 2017 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 20 AD, 20 HC | cross-sectional | n.d. | dorsolateral and ventral PFC | emotional working memory (n-back task) | 24 | no | |
| Oboshi et al., 2016 | OEG-16 system (Spectratech Inc., Yokohama, Japan) | 11 early-to-moderate AD, 11 HC (*) | cross-sectional | alfa4beta2 nicotinic receptor tracer [18F]2FA | PFC | visual WMT | 16 | PET | |
| Li et al., 2018 | NIRScout (NIRx Medizintechnik GmbH, Germany) | 9 MCI, 13 AD (6 mild AD, 7 moderate to severe AD), 8 HC | cross-sectional | MMSE | FC, bilateral parietal cortex | digit verbal span task | 46 | no | |
| Li et al., 2019 | NIRScout (NIRx Medizintechnik GmbH, Germany) | 14 mild AD, 8 HC | cross-sectional | n.d. | FC, bilateral parietal cortex | digit verbal span task | 46 | concurrent fNIRS-EEG | |
| Perpetuini et al., 2017 | Imagent (ISS Inc., Champaign, IL, USA) | 11 mild AD, 11 HC | cross-sectional | free and cued selective reminding test | bilateral PFC | free and cued selective reminding test | 17 | no | |
| Perpetuini et al., 2019 | Imagent (ISS Inc., Champaign, IL, USA) | 11 mild AD, 11 HC | cross-sectional | CDT | bilateral FC and PFC | CDT, digit span test, Corsi block tapping test | 21 | no | |
| Cognitive Task - Verbal Fluency Task (VFT) | Hock et al., 1996 | NIRO-500 (Hamamatsu Photonics K.K., Japan) | (17 HOA, 12 HYA) 19 AD, 19 HC | cross-sectional | n.d. | bilateral PFC and parietal cortex | calculation task | 2 | no |
| Hock et al., 1997 | NIRO-500 (Hamamatsu Photonics K.K., Japan) | 29 mild AD, 27 HC | cross-sectional | n.d. | frontal, prefrontal and parietal cortex | letter fluency, modified Stroop colour word interference test | 2 | concurrent NIRS-PET | |
| Fallgatter et al., 1997 | Critikon 2020 Cerebral Redox Monitor (Johnson and Johnson Medical) | 10 AD, 10HC | cross-sectional | n.d. | bilateral PFC | letter and category fluency tasks | 4 | no | |
| Herrmann et al., 2008 | ETG-100 (Hitachi Medical Co., Tokyo, Japan) | 16 AD, 16 HC | cross-sectional | n.d. | bilateral PFC | letter and category fluency tasks | 24 | no | |
| Arai et al., 2006 | ETG-7000 (Hitachi Medical Co., Tokyo, Japan) | 15 AD, 15 MCI, 32 HC | cross-sectional | MMSE | FC, occipital cortex, bilateral parietal cortex | letter fluency task | 84 | no | |
| Yeung et al., 2016 | OEG-SpO2 system (Spectratech Inc., Tokyo, Japan) | 10 aMCI, 16 MCI, 26 HC | cross-sectional | BNT, HKLLT, RCFT, STT | bilateral PFC | category fluency task | 16 | no | |
| Yap et al., 2017 | OT-R40 fNIRS topography system (Hitachi Medical Co., Tokyo, Japan) | 18 mild AD, 12 MCI, 31 HC | cross-sectional | MMSE | PFC, partial temporal cortex | semantic fluency task | 52 | no | |
| Doi et al., 2013 | OEG-16 system (Spectratech Inc., Yokohama, Japan) | 16 MCI | cross-sectional | modified Stroop colour and word test | bilateral PFC | normal and dual-task walking (letter fluency task) | 16 | no | |
| Katzorke et al., 2018 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 55 MCI, 55 HC | cross-sectional | n.d. | FC, PFC and temporal cortex | letter and category fluency task, control condition | 52 | no | |
| Metzger et al., 2016 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 8 bvFTD, 8 AD, 8 HC | cross-sectional | n.d. | bilateral PFC and temporal cortex | letter and category fluency task, control condition | 22 | no | |
| Visuospatial Task | Kito et al., 2014 | FOIRE-3000 (Shimadzu Corporation, Kyoto, Japan) | 30 patients with depression, 28 AD, 33 HC | cross-sectional | MMSE, CDR, FAB, HAMD | FC and parietal cortex | letter fluency task, Benton Judgment of Line Orientation | 44 | no |
| Zeller et al., 2010 | ETG-100 (Hitachi Medical Co., Tokyo, Japan) | 13 mild to moderate AD, 13 HC | cross-sectional | n.d. | parietal cortex | modified version of the Benton Line Orientation Task | 24 | no | |
| Ecological Applications | Tomioka et al., 2009 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 12 AD, 14 HC | cross-sectional | n.d. | bilateral PFC and temporal cortex | collision avoidance (driving task) | 52 | driving simulator |
| Shimizu et al., 2018 | LABNIRS (Shimadzu Corporation, Kyoto, Japan) | 45 MCI (35 intervention group, 10 control group) | longitudinal | FAB, CS-30 test, one-leg standing test, sit-and-reach test, timed Up & Go test | bilateral PFC | movement music therapy (physical-cognitive task) | 45 | digital sit-and-reach instrument box, digital handgrip dynamometer, walking measurement instrument | |
| Longitudinal Applications | van Beek et al., 2010 | Oxymon (Artinis Medical Systems, The Netherlands) | 21 AD, 20 HC | longitudinal | n.d. | bilateral FC | tissue oxygenation monitor during postural change task | n.d. | TCD, pulse-oximeter, capnography, finger photo-plethysmography |
| Araki et al., 2014 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 37 moderate-to-severe AD (19 experimental group, 18 control group) | longitudinal | MMSE, CDT, CGI-I scale, NPI, J-ZBI | FC | letter fluency task | 22 | no | |
| Metzger et. al, 2015 | ETG-4000 (Hitachi Medical Co., Tokyo, Japan) | 24 AD | longitudinal | MMSE, immediate and delayed word list recall trials | bilateral PFC and temporal cortex | letter and category fluency task | 44 | no | |
| Viola et al., 2014 | custom NIRS instrument (T-NIRS EVO II) | 25 mild AD | longitudinal | MMSE, AVLT | bilateral frontal and parieto-temporal cortex | tissue oxygenation monitor | 1 | no | |
| Vermeij et al., 2017 | Oxymon MKIII (Artinis Medical Systems, The Netherlands,) | 14 MCI, 21 HC | longitudinal | n.d. | bilateral PFC | verbal n-back task | n.d. | finger photoplethysmography, ECG | |
| Polak et al., 2017s | ETG-4000 and ETG-100 (Hitachi Medical Co., Tokyo, Japan) | 530 AD, 74 MCI | longitudinal | MMSE, Anxiety Status Inventory, Bayer Activities of Daily Living Scale, BDI-II, DemTect, Edinburgh test of handedness, GDS, HAMD, RCFT, RWT, VLMT, TAP, WMS-R | prefrontal and parietal cortex | resting-state, letter and category fluency task, trail making test, angle discrimination test | 52 and 24 | blood test, vagus somatosensory evoked potentials (EEG), intima media thickness, left ventricular ejection fraction, MRI, PET, CSF analysis | |
| Multiple Sclerosis (MS) | ||||||||
|---|---|---|---|---|---|---|---|---|
| fNIRS Device | Patient Info | Study Type | Integrated Clinical Outcomes | Investigated Cortical Areas | Performed Task | Ch. | Multimodal Integration | |
| Chaparro et al., 2017 | fNIR Imager 1000 (fNIR Devices LLC, Protomac, MD, USA) | 10 MS, 12 HC | cross-sectional | RBANS, SPPB | PFC | walking while talking with/without partial body weight support (WT, DWT) | 16 | instrumented treadmill |
| Saleh et al., 2018 | NIRSport (NIRx Medizintechnik GmbH, Germany) | 14 RRMS, 14 HC | cross-sectional | BVMT-R, CVLT-II, SDMT, T25FW | bilateral premotor and supplementary motor areas | serial 7′s subtraction cognitive task, walking and DWT | 12 | no |
| Hernandez et al., 2016 | fNIR Imager 1000 (fNIR Devices LLC, Protomac, MD, USA) | 8 MS, 8 HC | cross-sectional | EDSS | PFC | walking without/while talking (WT, DWT) | 16 | instrumented walkway |
| Hernandez et al., 2019 | fNIR Imager 1000 (fNIR Devices LLC, Protomac, MD, USA) | 10 MS, 12 HC (*) | cross-sectional | n.d. | PFC | reciting alternate letters, virtual beam walking without/while talking | 16 | instrumented treadmill |
| Borragán et al., 2018 | BrainSight NIRS V2.3b16 (Rogue Research Inc., Canada) | 10 RRMS, 11 HC (*) | cross-sectional | VASf | dorsolateral and ventrolateral PFC, inferior parietal cortex | TloadDback (dual working memory task) | 24 | polysomnography (including EEG, EOG, EMG, ECG, abdominal and thoracic belts, oronasal airflow and thermocouple, finger pulse oximeter) |
| Jimenez et al., 2014 | CW5 (TechEn Inc., Milford, MA, USA) | 4 RRMS, 2 SPMS, 2 MS, 1 CIS, 1 MS (unspecified), 8 HC | cross-sectional | n.d. | motor cortex | unilateral finger tapping, resting-state | n.d. | no |
| Wolff et al., 2019 | NIRSport (NIRx Medical Technologies LLC, NY, USA) | 26 RRMS, 18 SPMS, 6 PPMS | cross-sectional | BDI, CR10 scale, FSMC, SCS-K-D | PFC (BA10) | isometric contraction task | 22 | Hand dynamometer |
| Stojanovic-Radic et al., 2015 | DYNOT Imaging System, Model 264 (NIRx Medical Technologies LLC, Glen Head, NY, USA) | 13 MS, 12 HC (*) | cross-sectional | n.d. | bilateral superior frontal and middle frontal gyri (BA10) | n-back task (working memory task) | 900 | no |
| Molinari et al., 2014 | NIRO-200 (Hamamatsu Photonics K.K., Japan) | 22 RRMS, 10 other neurological disease, 22 HC (*) | cross-sectional | n.d. | FC | monitoring during ozone autohemotherapy | 2 | transcranial doppler, ozone autohemotherapy |
| Molinari et al., 2017 | NIRO-200 (Hamamatsu Photonics K.K., Japan) | 10 RRMS, 10 HC (*) | cross-sectional | n.d. | bilateral FC | monitoring during ozone autohemotherapy | 2 | ozone autohemotherapy |
| Yang and Dunn, 2015 | ISS OxiplexTS (ISS Inc., Champaign, IL, USA) | 51 RRMS, 16 SPMS, 15 PPMS, 3 CIS, 19 HC | cross-sectional | EDSS, SDMT, T25FT, 9 hole peg test | bilateral FC | tissue oxygenation monitor | 4 | concurrent NIRS-MRI |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonilauri, A.; Sangiuliano Intra, F.; Pugnetti, L.; Baselli, G.; Baglio, F. A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases—Actual Applications and Future Perspectives. Diagnostics 2020, 10, 581. https://doi.org/10.3390/diagnostics10080581
Bonilauri A, Sangiuliano Intra F, Pugnetti L, Baselli G, Baglio F. A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases—Actual Applications and Future Perspectives. Diagnostics. 2020; 10(8):581. https://doi.org/10.3390/diagnostics10080581
Chicago/Turabian StyleBonilauri, Augusto, Francesca Sangiuliano Intra, Luigi Pugnetti, Giuseppe Baselli, and Francesca Baglio. 2020. "A Systematic Review of Cerebral Functional Near-Infrared Spectroscopy in Chronic Neurological Diseases—Actual Applications and Future Perspectives" Diagnostics 10, no. 8: 581. https://doi.org/10.3390/diagnostics10080581