Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Examinations
2.2. Tear Function Test and Ocular Surface Vital Staining
2.3. In Vivo Laser-Scanning Confocal Microscopy
2.4. Corneal Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Tear Functions and Ocular Surface Staining Scores
3.2. In Vivo Laser-Scanning Confocal Microscopy
3.2.1. Corneal Cell Density and Area
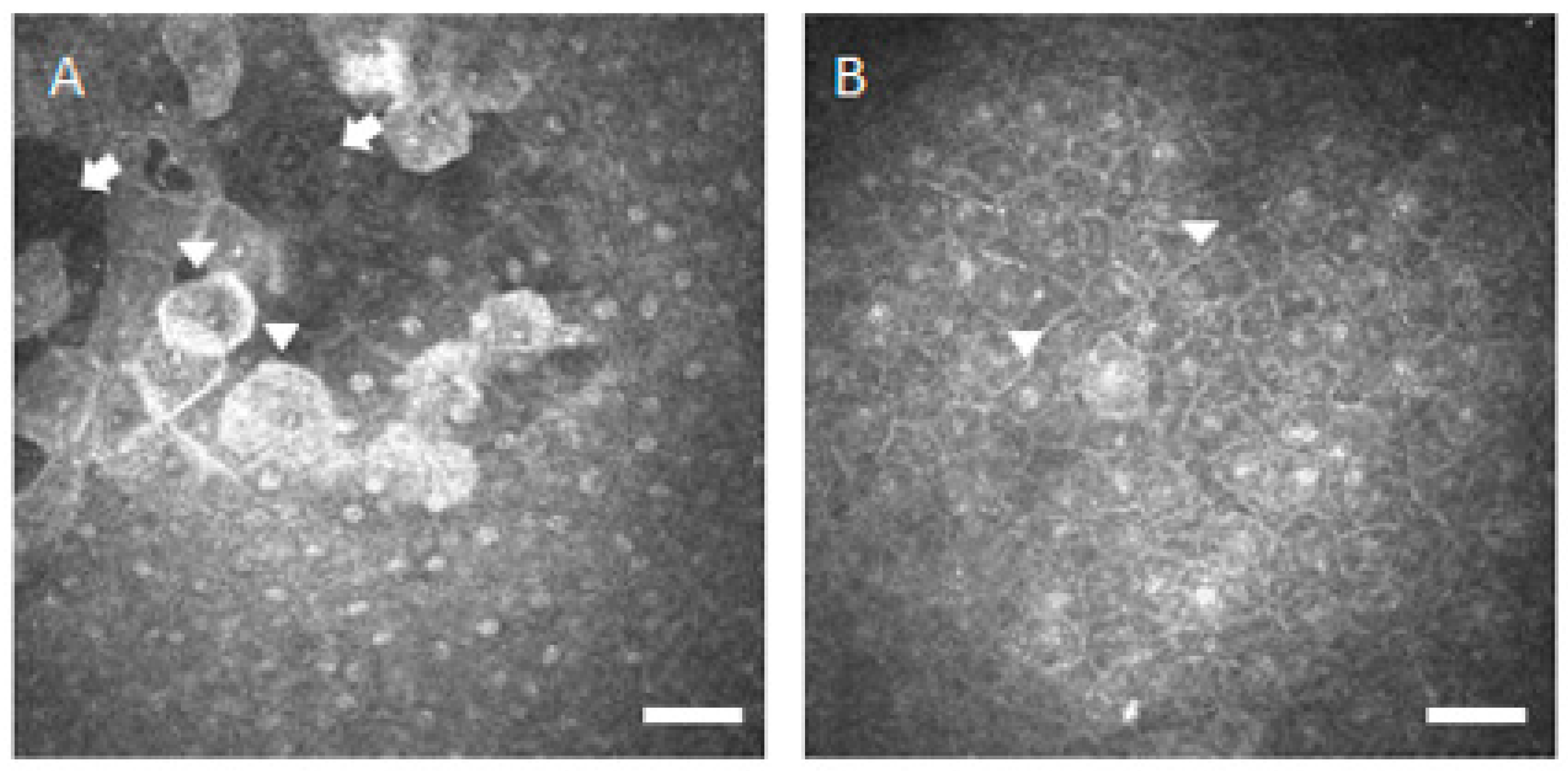
3.2.2. Corneal Inflammatory Cell Density
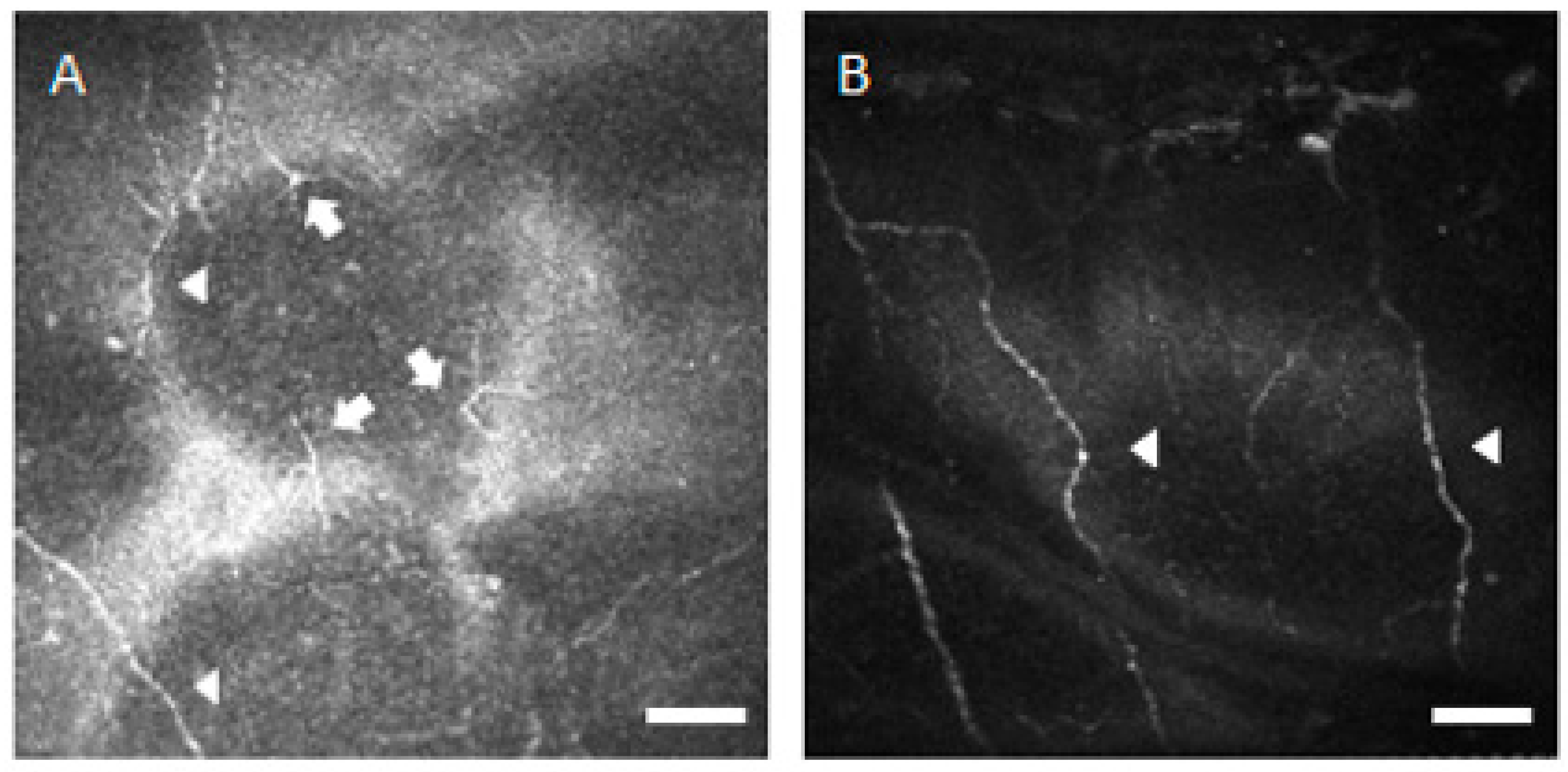
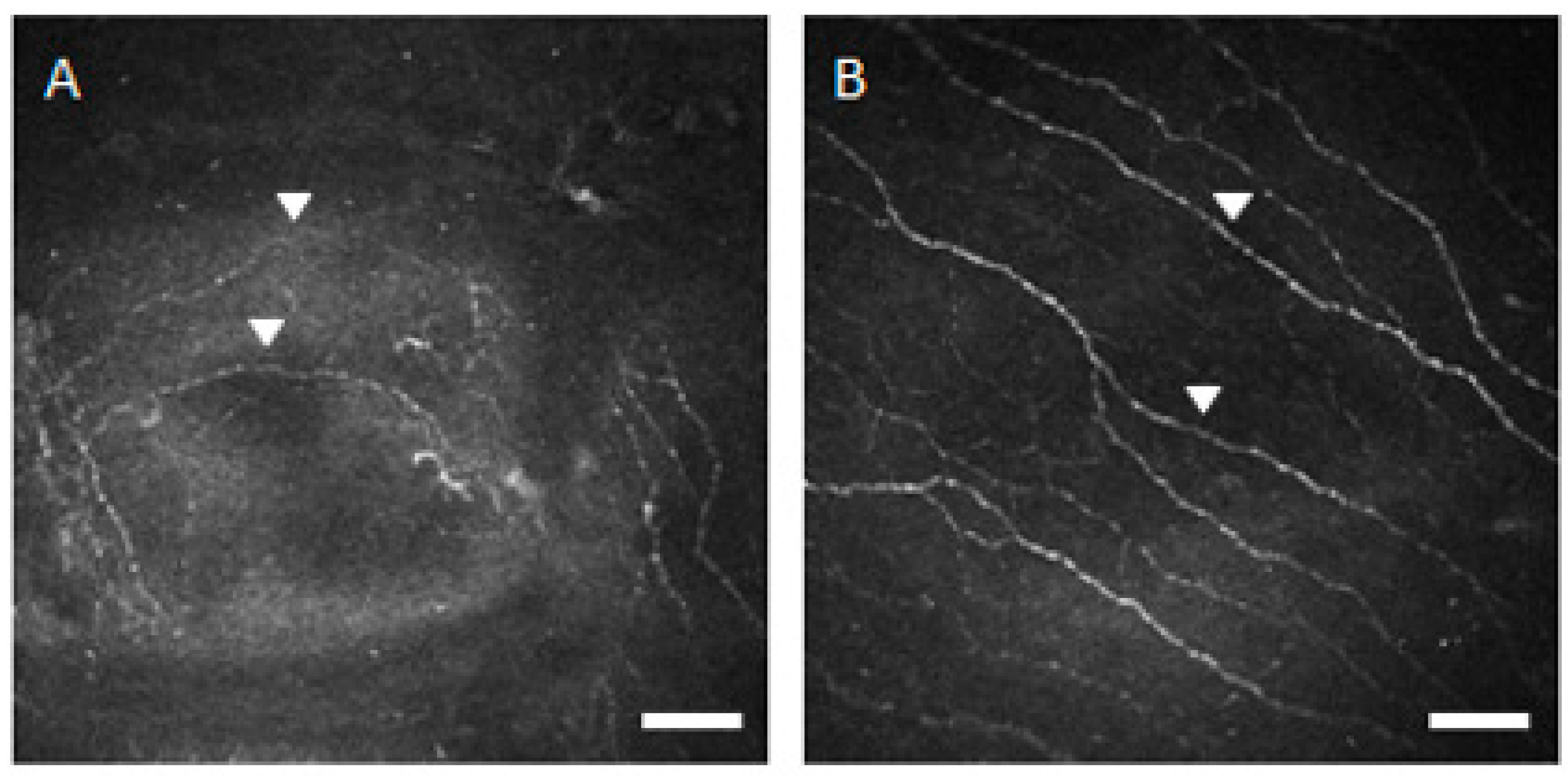
3.2.3. Corneal Nerve Density and Morphology
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wakamatsu, T.H.; Sato, E.A.; Matsumoto, Y.; Ibrahim, O.M.A.; Dogru, M.; Kaido, M.; Ishida, R.; Tsubota, K. Conjunctival in vivo confocal scanning laser microscopy in patients with Sjögren’s syndrome. Investig. Ophthalmol. Vis. Sci. 2010, 51, 144–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonsson, R.; Moen, K.; Vestrheim, D.; Szodoray, P. Current issues in Sjögren’s syndrome. Oral. Dis. 2002, 8, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.S.; Azar, D.T.; Dohlman, C.H. Sjögren’s syndrome. In The Cornea: Scientific Foundation and Clinical Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004; p. 629. [Google Scholar]
- Solomon, A.; Dursun, D.; Liu, Z.; Xie, Y.; Macri, A.; Pflugfelder, S.C. Pro- and anti-inflammatory forms of interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2283–2292. [Google Scholar]
- Tishler, M.; Yaron, I.; Geyer, O.; Shirazi, I.; Naftaliev, E.; Yaron, M. Elevated tear interleukin-6 levels in patients with Sjögren’s syndrome. Ophthalmology 1998, 105, 2327–2329. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Jones, D.; Ji, Z.; Afonso, A.; Monroy, D. Altered cytokine balance in the tear fluid and conjunctiva of patients with Sjögren’s syndrome keratocunjunctivitis sicca. Curr. Eye Res. 1999, 19, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Benitez del Castillo, J.M.; Wasfy, M.A.S.; Fernandez, C.; Garcia-Sanchez, J. An in vivo confocal masked study on corneal epithelium and subbasal nerves in patients with dry eye. Investig. Ophthalmol. Vis. Sci. 2004, 45, 3030–3035. [Google Scholar] [CrossRef] [Green Version]
- Benitez del Castillo, J.M.; Acosta, M.C.; Wassfi, M.A.; Diaz-Valle, D.; Gegundez, J.A.; Fernandez, C.; Garcia-Sanchez, J. Relation between corneal innervation with confocal microscopy and corneal sensitivity with noncontact esthesiometry in patients with dry eye. Investig. Ophthalmol. Vis. Sci. 2007, 48, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Villani, E.; Galimberti, D.; Viola, F.; Mapelli, C.; Ratiglia, R. The cornea in Sjögren’s syndrome: An in vivo confocal study. Investig. Ophthalmol. Vis. Sci. 2007, 48, 2017–2022. [Google Scholar] [CrossRef]
- Villani, E.; Galimberti, D.; Viola, F.; Mapelli, C.; Del Papa, N.; Ratiglia, R. Corneal involvement in rheumatoid arthritis: An in vivo confocal study. Investig. Ophthalmol. Vis. Sci. 2008, 49, 560–564. [Google Scholar] [CrossRef]
- Pflugfelder, S.C.; Huang, A.J.; Feuer, W.; Chuchovski, P.T.; Pereira, I.C.; Tseng, S.C. Conjunctival cytologic features of primary Sjögren’s syndrome. Ophthalmology 1990, 97, 985–991. [Google Scholar] [CrossRef]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II definition and classification report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Zhivov, A.; Stachs, O.; Kraak, R.; Stave, J.; Guthoff, R.F. In vivo confocal microscopy of the ocular surface. Ocul. Surf. 2006, 4, 81–93. [Google Scholar] [CrossRef]
- Efron, N.; Perez-Gomez, I.; Mutalib, H.A.; Hollingsworth, J. Confocal microscopy of the normal human cornea. Contact Lens Anterior Eye 2001, 24, 16–24. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Dogru, M.; Sato, E.A.; Katono, Y.; Uchino, Y.; Shimmura, S.; Tsubota, K. The application of in vivo confocal scanning laser microscopy in the management of Acanthamoeba keratitis. Mol. Vis. 2007, 13, 1319–1326. [Google Scholar] [PubMed]
- Brasnu, E.; Bourcier, T.; Dupas, B.; Degorge, S.; Rodallec, T.; Laroche, L.; Borderie, V.; Baudouin, C. In vivo confocal microscopy in fungal keratitis. Br. J. Ophthalmol. 2007, 91, 588–591. [Google Scholar] [CrossRef] [Green Version]
- Messmer, E.M.; Mackert, M.J.; Zapp, D.M.; Kampik, A. In vivo confocal microscopy of normal conjunctiva and conjunctivitis. Cornea 2006, 25, 781–788. [Google Scholar] [CrossRef]
- Hu, Y.; Adan, E.S.; Matsumoto, Y.; Dogru, M.; Fukagawa, K.; Takano, Y.; Tsubota, K.; Fujishima, H. Conjunctival in vivo confocal scanning laser microscopy in patients with atopic keratoconjunctivitis. Mol. Vis. 2007, 13, 1379–1389. [Google Scholar]
- Kojima, T.; Matsumoto, Y.; Ibrahim, O.M.; Sato, E.A.; Dogru, M.; Tsubota, K. In vivo evaluation of superior limbic keratoconjunctivitis using laser scanning confocal microscopy and conjunctival impression cytology. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3986–3992. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, Y.; Sato, E.A.; Ibrahim, O.M.A.; Dogru, M.; Tsubota, K. The application of in vivo laser confocal microscopy to the diagnosis and evaluation of meibomian gland dysfunction. Mol. Vis. 2008, 14, 1263–1271. [Google Scholar]
- Sato, E.A.; Matsumoto, Y.; Dogru, M.; Kaido, M.; Wakamatsu, T.; Ibrahim, O.M.A.; Obata, H.; Tsubota, K. Lacrimal gland in Sjögren’s syndrome. Ophthalmology 2010, 117, 1055. [Google Scholar] [CrossRef]
- Fujibayashi, T.; Sugai, S.; Miyasaka, N.; Hayashi, Y.; Tsubota, K. Revised Japanese criteria for Sjögren’s syndrome (1999): Availability and validity. Mod. Rheumatol. 2004, 14, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, J. (Dry Eye Society). Definition and diagnosis of dry eye 2006. Atarashii Ganka 2007, 24, 181–184. (In Japanese) [Google Scholar]
- Toda, I.; Tsubota, K. Practical double vital staining for ocular surface evaluation. Cornea 1993, 12, 366–367. [Google Scholar] [CrossRef]
- Oliveira-Soto, L.; Efron, N. Morphology of corneal nerves using confocal microscopy. Cornea 2001, 20, 374–384. [Google Scholar] [CrossRef]
- Tsubota, K.; Toda, I.; Fujishima, H.; Yamada, M.; Sugawara, T.; Shimazaki, J. Extended wear soft contact lenses induce corneal epithelial changes. Br. J. Ophthalmol. 1994, 78, 907–911. [Google Scholar] [CrossRef] [Green Version]
- Tsubota, K.; Hata, S.; Toda, I.; Yagi, Y.; Sakata, M.; Shimazaki, J. Increase in corneal epithelial cell size with extended wear soft contact lenses depends on continuous wearing time. Br. J. Ophthalmol. 1996, 80, 144–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Pflugfelder, S.C. Corneal thickness is reduced in dry eye. Cornea 1999, 18, 403–407. [Google Scholar] [CrossRef] [PubMed]
- Funderburgh, J.L.; Mann, M.M.; Funderburgh, M.L. Keratocyte phenotype mediates proteoglycan structure: A role for fibroblasts in corneal fibrosis. J. Biol. Chem. 2003, 278, 45629–45637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, S.E.; Mohan, R.R.; Mohan, R.R.; Ambrosio, R., Jr.; Hong, J.; Lee, J. The corneal wound healing response: Cytokine-mediated interaction of the epithelium, stroma, and inflammatory cells. Prog. Retin. Eye Res. 2001, 20, 625–637. [Google Scholar] [CrossRef]
- Lambiase, A.; Manni, L.; Bonini, S.; Rama, P.; Micera, A.; Aloe, L. Nerve growth factor promotes corneal healing: Structural, biochemical, and molecular analyses of rat and human corneas. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1063–1069. [Google Scholar]
- Lambiase, A.; Rama, P.; Bonini, S.; Caprioglio, G.; Aloe, L. Topical treatment with nerve growth factor for corneal neurotrophic ulcers. N. Engl. J. Med. 1998, 338, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Bonini, S.; Lambiase, A.; Rama, P.; Caprioglio, G.; Aloe, L. Topical treatment with nerve growth factor for neurotrophic keratitis. Ophthalmology 2000, 107, 1347–1351. [Google Scholar] [CrossRef]
- De Paiva, C.S.; Corrales, R.M.; Villarreal, A.L.; Farley, W.J.; Li, D.Q.; Stern, M.E.; Pflugfelder, S.C. Corticosteroid and doxycycline suppress MMP-9 and inflammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. Exp. Eye Res. 2006, 83, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Li, W.; Dong, N.; Chen, W.; Liu, J.; Chen, L.; Yuan, H.; Geng, Z.; Liu, Z. Changes in corneal epithelial layer inflammatory cells in aqueous tear-deficient dry eye. Investig. Ophthalmol. Vis. Sci. 2010, 51, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Matsumoto, M.; Kotani, M.; Makino, T. Possible involvement of matrix metalloproteinase-9 in Langerhans cell migration and maturation. J. Immunol. 1999, 163, 5989–5993. [Google Scholar] [PubMed]
- Dekaris, I.; Zhu, S.N.; Dana, M.R. TNF-alpha regulates corneal Langerhans cell migration. J. Immunol. 1999, 162, 4235–4239. [Google Scholar]
- Tuominen, I.S.J.; Konttinen, Y.T.; Vesaluoma, M.H.; Moilanen, J.A.O.; Helinto, M.; Tervo, T.M.T. Corneal innervation and morphology in primary Sjögren’s syndrome. Investig. Ophthalmol. Vis. Sci. 2003, 44, 2545–2549. [Google Scholar] [CrossRef] [Green Version]
- Tuisku, I.S.; Konttinen, Y.T.; Konttinen, L.M.; Tervo, T.M. Alterations in corneal sensitivity and nerve morphology in patients with primary Sjögren’s syndrome. Exp. Eye Res. 2008, 86, 879–885. [Google Scholar] [CrossRef]
- Cruzat, A.; Witkin, D.; Baniasadi, N.; Zheng, L.; Ciolino, J.B.; Jurkunas, U.V.; Chodosh, J.; Pavan-Langston, D.; Dana, R.; Hamrah, P. Inflammation and the nervous system: The connection in the cornea in patients with infectious keratitis. Investig. Ophthalmol. Vis. Sci. 2011, 52, 5136–5143. [Google Scholar] [CrossRef]
- Parlanti, P.; Pal-Ghosh, S.; Williams, A.; Tadvalkar, G.; Popratiloff, A.; Stepp, M.A. Axonal debris accumulates in corneal epithelial cells after intraepithelial corneal nerves are damaged: A focused Ion Beam Scanning Electron Microscopy (FIB-SEM) study. Exp. Eye Res. 2020, 194. in press. [Google Scholar] [CrossRef]
- Stepp, M.A.; Pal-Ghosh, S.; Downie, L.E.; Zhang, A.C.; Chinnery, H.R.; Machet, J.; Girolamo, N.D. Corneal epithelial “Neuromas”: A case of mistaken identity? Cornea 2020, 39, 930–934. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.P.; Yagi, Y.; Tsubota, K. Decrease in corneal sensitivity and change in tear function in dry eye. Cornea 1996, 15, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Allan, S.M.; Tyrrell, P.J.; Rothwell, N.J. Interleukin-1 and neuronal injury. Nat. Rev. Immunol. 2005, 5, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Park, K.M.; Bowers, W.J. Tumor necrosis factor-alpha mediated signaling in neuronal homeostasis and dysfunction. Cell Signal. 2010, 22, 977–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, P.Y.; Carrel, H.; Huang, J.S.; Wang, I.J.; Hou, Y.C.; Chen, W.L.; Wang, J.Y.; Hu, F.R. Decreased density of corneal basal epithelium and subbasal nerve bundle changes in patients with diabetic retinopathy. Am. J. Ophthalmol. 2006, 142, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, K.; Ueda, H.; Kim, K.J.; Lee, V.H. Nucleotide stimulation of Cl- secretion in the pigmented rabbit conjunctiva. J. Pharmacol. Exp. Ther. 1999, 291, 53–59. [Google Scholar] [PubMed]
- Li, Y.; Kuang, K.; Yerxa, B.; Wen, Q.; Rosskothen, H.; Fischbarg, J. Rabbit conjunctival epithelium transports fluid, and P2Y22 receptor agonists stimulate Cl− and fluid secretion. Am. J. Physiol. Cell Physiol. 2001, 281, C595–C602. [Google Scholar] [CrossRef] [Green Version]
- Jumblatt, J.E.; Jumblatt, M.M. Regulation of ocular mucin secretion by P2Y2 nucleotide receptors in rabbit and human conjunctiva. Exp. Eye Res. 1998, 67, 341–346. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ohashi, Y.; Watanabe, H.; Tsubota, K. For the Diquafosol Ophthalmic Solution Phase 2 Study Group. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: A Japanese phase 2 clinical trial. Ophthalmology 2012, 119, 1954–1960. [Google Scholar] [CrossRef]
- Takamura, E.; Tsubota, K.; Watanabe, H.; Ohashi, Y. For the Diquafosol Ophthalmic Solution Phase 3 Study Group. A randomized, double-masked comparison study of diquafosol versus sodium hyaluronate ophthalmic solutions in dry eye patients. Br. J. Ophthalmol. 2012, 96, 1310–1315. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ibrahim, O.M.A. Application of in vivo confocal microscopy in dry eye disease. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES41–DES47. [Google Scholar] [CrossRef]
- Kheirkhah, A.; Dohlman, T.H.; Amparo, F.; Arnoldner, M.A.; Jamari, A.; Hamrah, P.; Dana, R. Effects of corneal nerve density on the response to treatment in dry eye disease. Ophthalmology 2015, 122, 662–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villani, E.; Garoli, E.; Termine, V.; Pichi, F.; Ratiglia, R.; Nucci, P. Corneal confocal microscopy in dry eye treated with corticosteroids. Optom. Vis. Sci. 2015, 92, e290–e295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iaccheri, B.; Torroni, G.; Cagini, C.; Fiore, T.; Cerquaglia, A.; Lupidi, M.; Cillino, S.; Dua, H.S. Corneal confocal scanning laser microscopy in patients with dry eye disease treated with topical cyclosporine. Eye 2017, 31, 788–794. [Google Scholar] [CrossRef] [Green Version]
- Levy, O.; Labbé, A.; Borderie, V.; Hamiche, T.; Dupas, B.; Laroche, L.; Baudouin, C.; Bouheraoua, N. Increased corneal sub-basal nerve density in patients with Sjögren syndrome treated with topical cyclosporine A. Clin. Exp. Ophthalmol. 2017, 45, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Sjögren’s Syndrome | Healthy Control | Probability | |
|---|---|---|---|
| Schirmer test (mm) | 2.3 ± 1.4 | 9.0 ± 4.7 | <0.0001 |
| Fluorescein staining score (points) | 3.8 ± 1.8 | 0.2 ± 0.6 | <0.0001 |
| Rose Bengal staining score (points) | 5.0 ± 1.9 | 0.1 ± 0.3 | <0.0001 |
| Break-up time (seconds) | 3.3 ± 1.0 | 11.1 ± 6.1 | <0.0001 |
| Superficial epithelial cell density (cells/mm2) | 829.7 ± 188.5 | 1215.9 ± 265.8 | <0.0001 |
| Superficial epithelial cell area (μm2) | 898.5 ± 167.0 | 717.9 ± 150.5 | =0.002 |
| Intermediate epithelial cell density (cells/mm2) | 3770.0 ± 521.1 | 3850.5 ± 360.7 | =0.62 |
| Intermediate epithelial cell area (μm2) | 193.7 ± 30.1 | 168.4 ± 29.1 | =0.10 |
| Basal epithelial cell density (cells/mm2) | 6087.9 ± 399.8 | 6301.1 ± 596.2 | =0.20 |
| Basal epithelial cell area (μm2) | 116.8 ± 22.5 | 109.8 ± 19.6 | =0.28 |
| Anterior stromal cell density (cells/mm2) | 477.0 ± 47.7 | 529.1 ± 93.9 | =0.04 |
| Intermediate stromal cell density (cells/mm2) | 393.3 ± 45.1 | 429.8 ± 58.7 | =0.06 |
| Posterior stromal cell density (cells/mm2) | 333.6 ± 33.6 | 338.0 ± 53.3 | =0.77 |
| Endothelial cell density (cells/mm2) | 3126.3 ± 237.0 | 3294.2 ± 330.0 | =0.27 |
| Endothelial cell area (μm2) | 319.1 ± 25.1 | 289.4 ± 47.9 | =0.17 |
| Sub-basal inflammatory cell density (cells/mm2) | 87.0 ± 52.5 | 17.3 ± 18.8 | <0.0001 |
| Sub-basal nerve number (nerves/frame) | 3.57 ± 0.62 | 5.12 ± 0.85 | <0.0001 |
| Sub-basal nerve density (μm/mm2) | 1145.6 ± 385.0 | 1799.9 ± 427.4 | <0.0001 |
| Sub-basal nerve beadings number (beadings/100 μm) | 10.2 ± 2.5 | 6.6 ± 2.3 | <0.0002 |
| Sub-basal nerve tortuosity (grade) | 2.91 ± 0.75 | 1.63 ± 0.57 | <0.0001 |
| Sub-basal nerve reflectively (grade) | 2.13 ± 0.55 | 1.73 ± 0.41 | =0.04 |
| Before Treatment | After Treatment | Probability | |
|---|---|---|---|
| Fluorescein staining score (points) | 3.1 ± 1.6 | 2.3 ± 2.1 | =0.13 |
| Rose Bengal staining score (points) | 4.9 ± 3.7 | 3.7 ± 1.9 | =0.14 |
| Break-up time (seconds) | 2.1 ± 1.1 | 3.6 ± 1.5 | =0.27 |
| Superficial epithelial cell density (cells/mm2) | 1001.1 ± 170.6 | 1396.4 ± 207.7 | =0.001 |
| Superficial epithelial cell area (μm2) | 790.0 ± 121.4 | 599.1 ± 76.4 | =0.01 |
| Intermediate epithelial cell density (cells/mm2) | 4043.8 ± 410.6 | 4503.4 ± 392.5 | =0.10 |
| Intermediate epithelial cell area (μm2) | 152.5 ± 21.8 | 138.9 ± 18.3 | =0.28 |
| Basal epithelial cell density (cells/mm2) | 6697.9 ± 483.7 | 6628.9 ± 655.7 | =0.87 |
| Basal epithelial cell area (μm2) | 94.6 ± 16.3 | 91.1 ± 16.2 | =0.94 |
| Anterior stromal cell density (cells/mm2) | 446.1 ± 60.3 | 456.8 ± 86.8 | =0.94 |
| Intermediate stromal cell density (cells/mm2) | 352.6 ± 34.4 | 349.2 ± 13.0 | =0.96 |
| Posterior stromal cell density (cells/mm2) | 306.9 ± 22.5 | 323.2 ± 21.9 | =0.54 |
| Endothelial cell density (cells/mm2) | 3245.1 ± 243.2 | 3434.0 ± 331.4 | =0.63 |
| Endothelial cell area (μm2) | 289.1 ± 23.4 | 267.2 ± 15.8 | =0.36 |
| Sub-basal inflammatory cell density (cells/mm2) | 117.3 ± 53.7 | 68.0 ± 35.2 | =0.03 |
| Sub-basal nerve number (nerves/frame) | 2.63 ± 0.96 | 3.96 ± 1.07 | =0.04 |
| Sub-basal nerve density (μm/mm2) | 829.6 ± 348.0 | 1238.6 ± 410.1 | =0.02 |
| Sub-basal nerve beadings number (beadings/100 μm) | 10.7 ± 2.3 | 7.9 ± 1.8 | =0.0008 |
| Sub-basal nerve tortuosity (grade) | 1.78 ± 0.38 | 1.19 ± 0.38 | =0.04 |
| Sub-basal nerve reflectively (grade) | 2.14 ± 0.30 | 1.89 ± 0.38 | =0.18 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, Y.; Ibrahim, O.M.A.; Kojima, T.; Dogru, M.; Shimazaki, J.; Tsubota, K. Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome. Diagnostics 2020, 10, 497. https://doi.org/10.3390/diagnostics10070497
Matsumoto Y, Ibrahim OMA, Kojima T, Dogru M, Shimazaki J, Tsubota K. Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome. Diagnostics. 2020; 10(7):497. https://doi.org/10.3390/diagnostics10070497
Chicago/Turabian StyleMatsumoto, Yukihiro, Osama M. A. Ibrahim, Takashi Kojima, Murat Dogru, Jun Shimazaki, and Kazuo Tsubota. 2020. "Corneal In Vivo Laser-Scanning Confocal Microscopy Findings in Dry Eye Patients with Sjögren’s Syndrome" Diagnostics 10, no. 7: 497. https://doi.org/10.3390/diagnostics10070497