Two-Dimensional Image-Based Screening Tool for Infants with Positional Cranial Deformities: A Machine Learning Approach

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
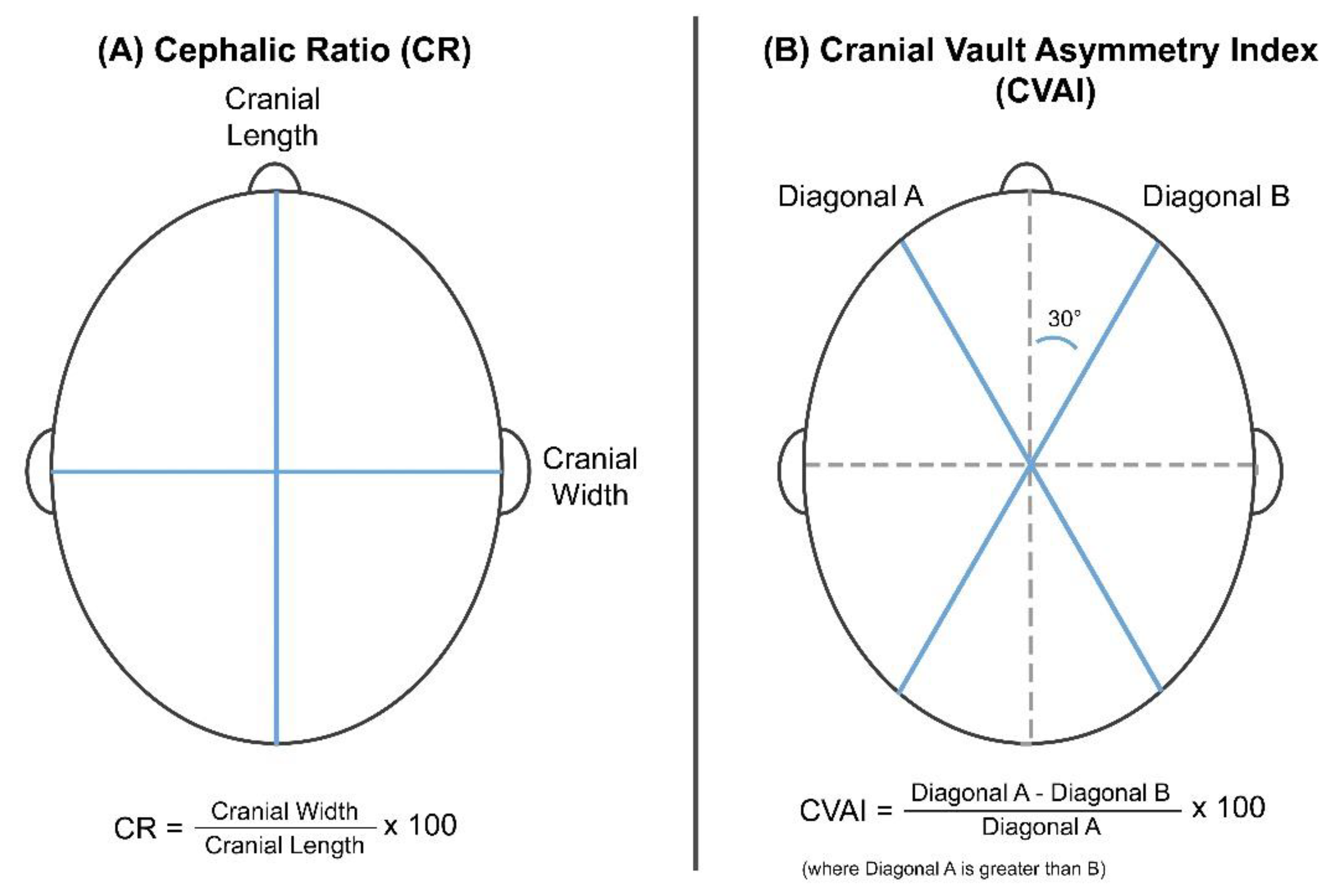
2.2. Diagnostic Indices for Head Deformities
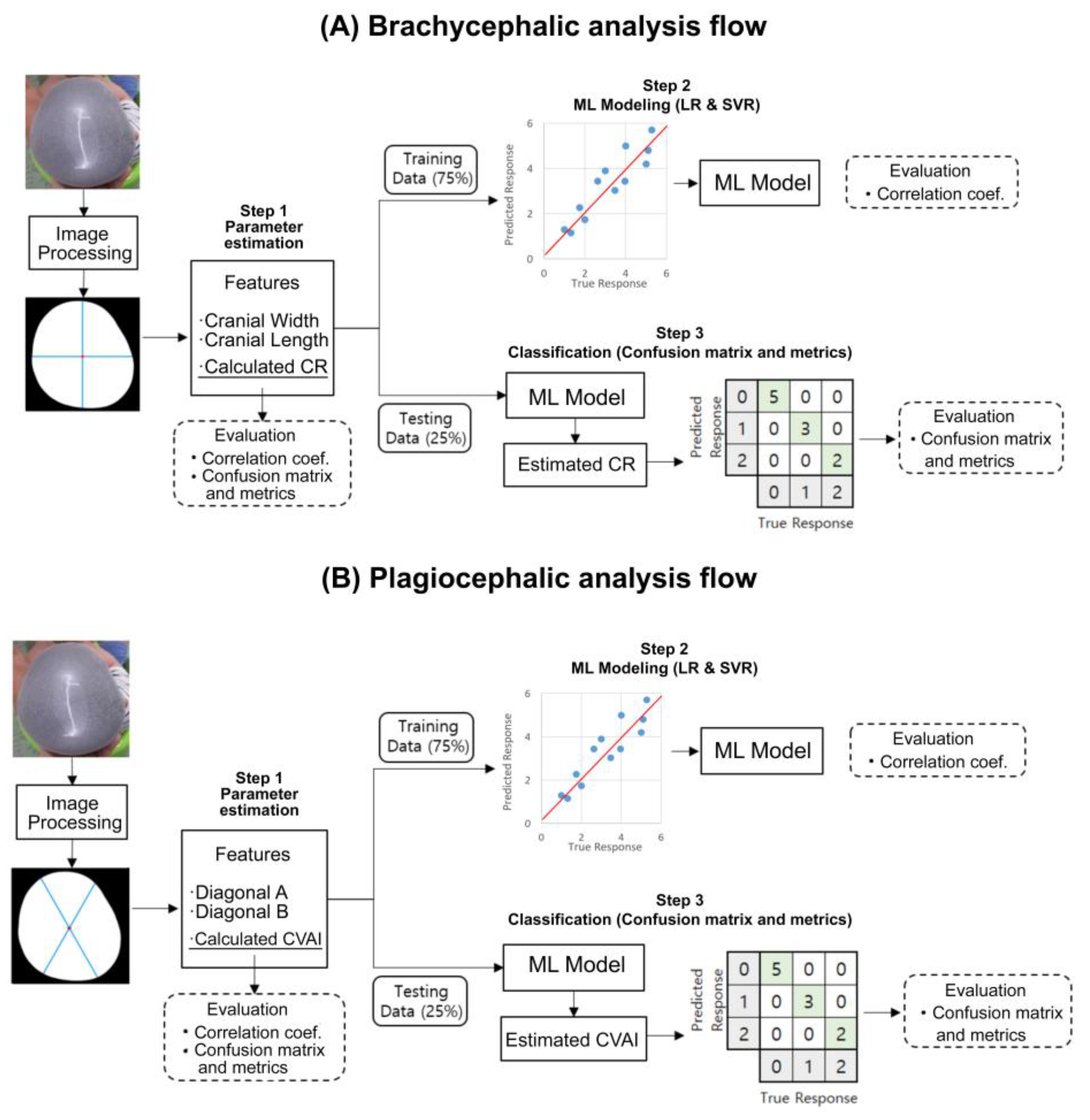
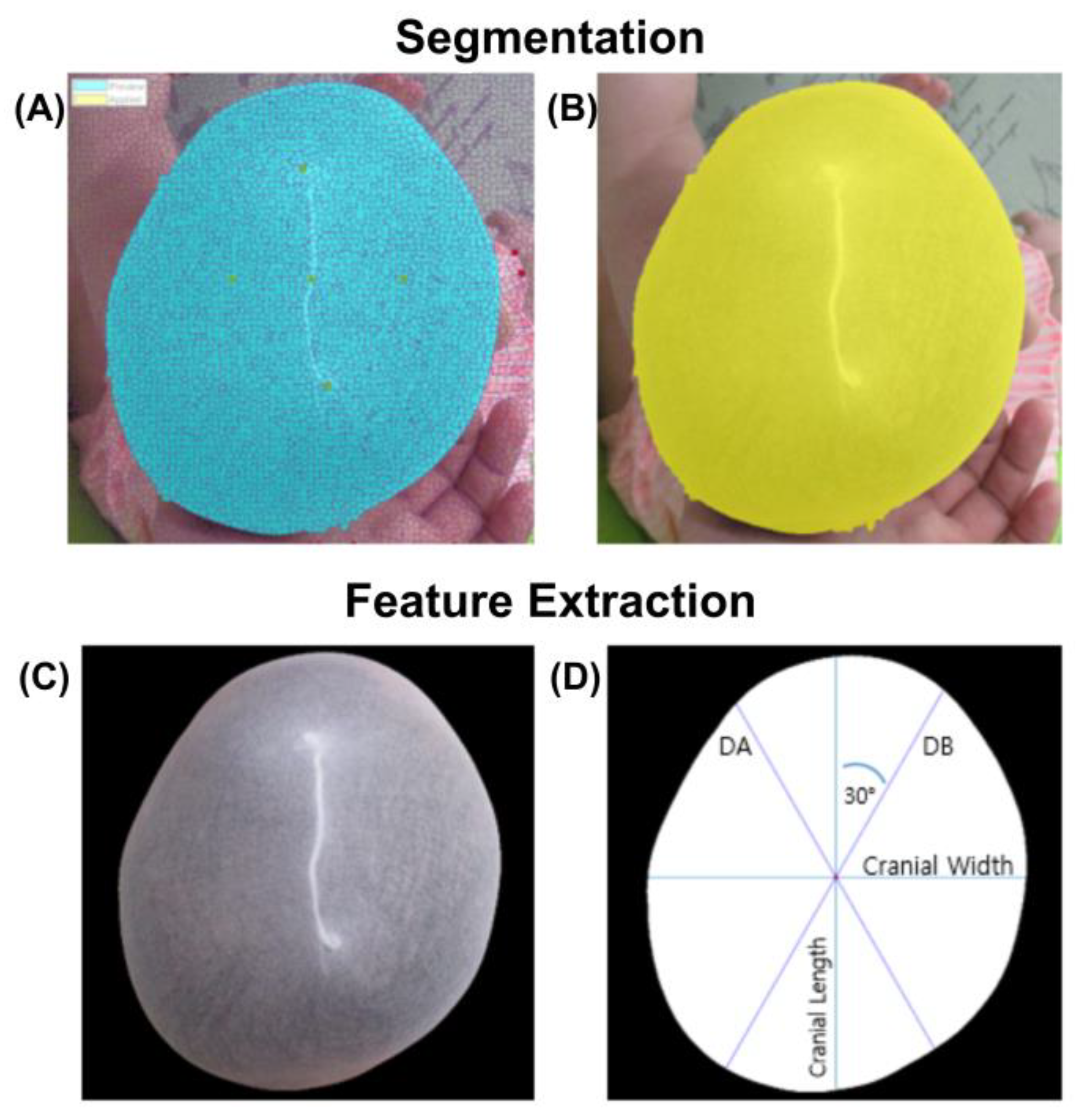
2.3. Image Processing
2.4. Feature Extraction
2.5. Machine Learning Modeling
2.6. Model Evaluation
3. Results
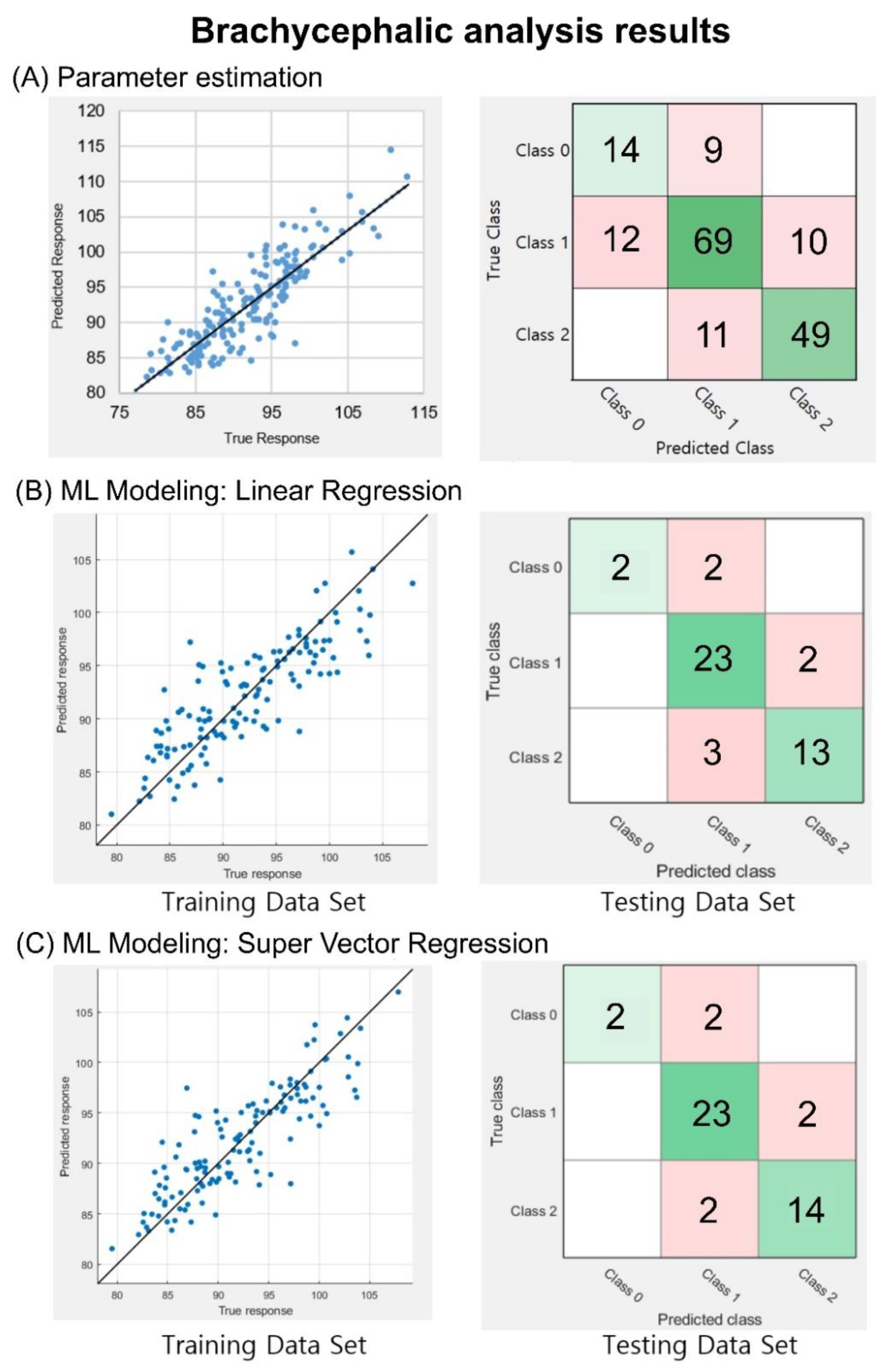
3.1. Brachycephalic Analyses
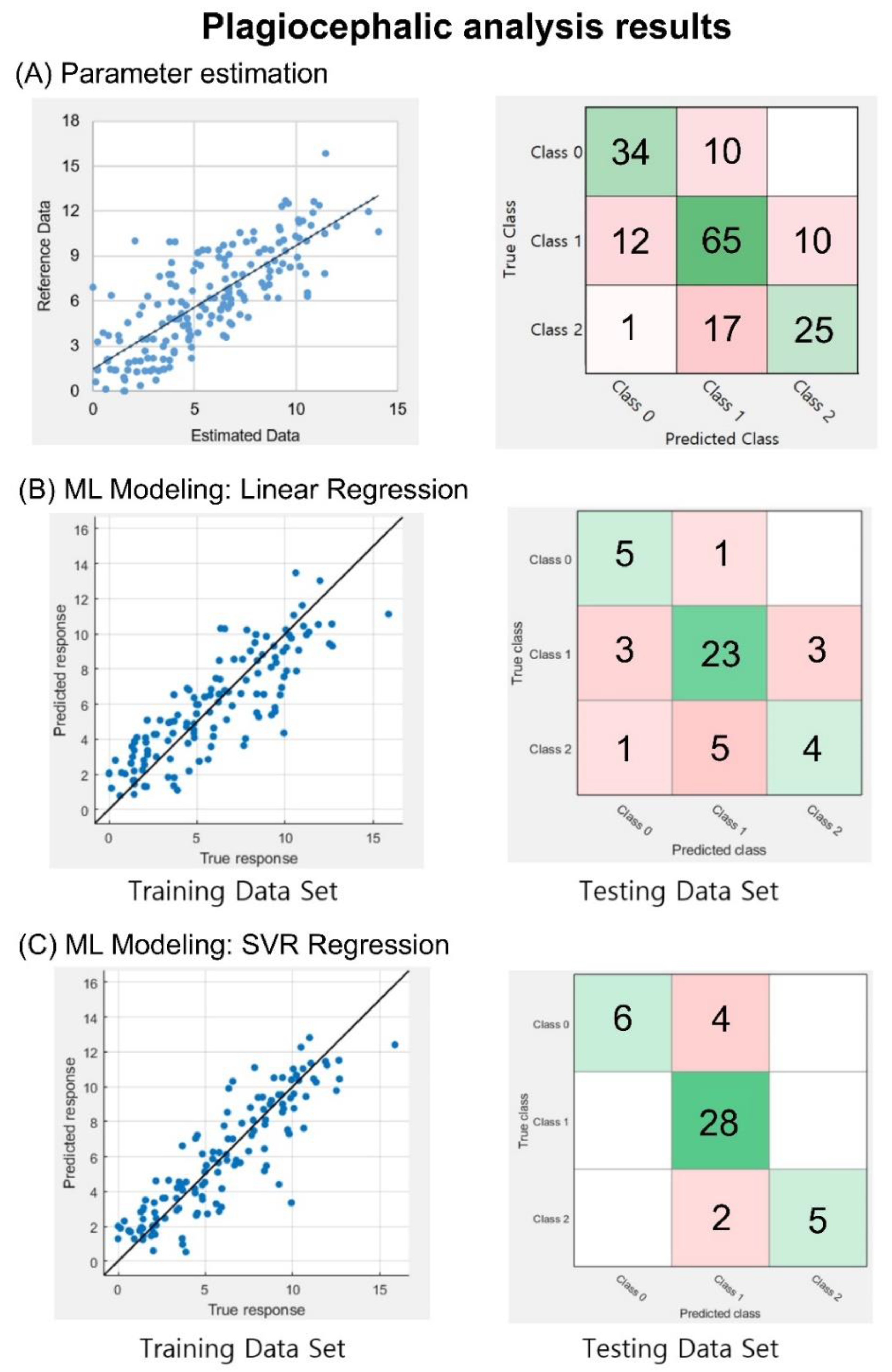
3.2. Plagiocephalic Analyses
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Yang, W.; Chen, J.; Shen, W.; Wang, C.; Wu, Z.; Chang, Q.; Li, W.; Lv, K.; Pan, Q.; Li, H.; et al. Prevalence of positional skull deformities in 530 premature infants with a corrected age of up to 6 months: A multicenter study. BMC Pediatrics 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linz, C.; Kunz, F.; Bohm, H.; Schweitzer, T. Positional Skull Deformities. Dtsch. Arztebl. Int. 2017, 114, 535–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchison, B.L.; Hutchison, L.A.D.; Thompson, J.M.D.; Mitchell, E.A. Plagiocephaly and Brachycephaly in the First Two Years of Life: A Prospective Cohort Study. Pediatrics 2004, 114, 970–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bialocerkowski, A.E.; Vladusic, S.L.; Wei Ng, C. Prevalence, risk factors, and natural history of positional plagiocephaly: A systematic review. Dev. Med. Child. Neurol. 2008, 50, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.F. Deformational plagiocephaly, brachycephaly, and scaphocephaly. Part I: Terminology, diagnosis, and etiopathogenesis. J. Craniofacial Surg. 2011, 22, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Kelly, K.M.; Littlefield, T.R.; Pomatto, J.K.; Ripley, C.E.; Beals, S.P.; Joganic, E.F. Importance of Early Recognition and Treatment of Deformational Plagiocephaly with Orthotic Cranioplasty. Cleft Palate-Craniofacial J. 1999, 36, 127–130. [Google Scholar] [CrossRef]
- van Vlimmeren, L.A.; Engelbert, R.H.; Pelsma, M.; Groenewoud, H.M.; Boere-Boonekamp, M.M.; der Sanden, M.W. The course of skull deformation from birth to 5 years of age: A prospective cohort study. Eur. J. Pediatrics 2017, 176, 11–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lessard, S.; Gagnon, I.; Trottier, N. Exploring the impact of osteopathic treatment on cranial asymmetries associated with nonsynostotic plagiocephaly in infants. Complement. Ther. Clin. Pract. 2011, 17, 193–198. [Google Scholar] [CrossRef]
- Peitsch, W.K.; Keefer, C.H.; LaBrie, R.A.; Mulliken, J.B. Incidence of Cranial Asymmetry in Healthy Newborns. Pediatrics 2002, 110, e72. [Google Scholar] [CrossRef] [Green Version]
- Mortenson, P.; Steinbok, P.; Smith, D. Deformational plagiocephaly and orthotic treatment: Indications and limitations. Childs Nerv. Syst. 2012, 28, 1407–1412. [Google Scholar] [CrossRef]
- Öhman, A. A Craniometer with a Headband Can Be a Reliable Tool to Measure Plagiocephaly and Brachycephaly in Clinical Practice. Health 2016, 8, 1258–1265. [Google Scholar] [CrossRef] [Green Version]
- Martini, M.; Klausing, A.; Luchters, G.; Heim, N.; Messing-Junger, M. Head circumference–a useful single parameter for skull volume development in cranial growth analysis? Head Face Med. 2018, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbero-Garcia, I.; Lerma, J.L.; Marques-Mateu, A.; Miranda, P. Low-Cost Smartphone-Based Photogrammetry for the Analysis of Cranial Deformation in Infants. World Neurosurg. 2017, 102, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Nahles, S.; Klein, M.; Yacoub, A.; Neyer, J. Evaluation of positional plagiocephaly: Conventional anthropometric measurement versus laser scanning method. J. Cranio-Maxillofac. Surg. 2018, 46, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Schaaf, H.; Pons-Kuehnemann, J.; Malik, C.Y.; Streckbein, P.; Preuss, M.; Howaldt, H.P.; Wilbrand, J.F. Accuracy of three-dimensional photogrammetric images in non-synostotic cranial deformities. Neuropediatrics 2010, 41, 24–29. [Google Scholar] [CrossRef]
- Hsung, T.C.; Lo, J.; Li, T.S.; Cheung, L.K. Recording of natural head position using stereophotogrammetry: A new technique and reliability study. J. Oral Maxillofac. Surg. 2014, 72, 2256–2261. [Google Scholar] [CrossRef] [Green Version]
- Wilbrand, J.F.; Schmidtberg, K.; Bierther, U.; Streckbein, P.; Pons-Kuehnemann, J.; Christophis, P.; Hahn, A.; Schaaf, H.; Howaldt, H.P. Clinical classification of infant nonsynostotic cranial deformity. J. Pediatrics 2012, 161, 1120–1125. [Google Scholar] [CrossRef]
- Wilbrand, J.F.; Wilbrand, M.; Pons-Kuehnemann, J.; Blecher, J.C.; Christophis, P.; Howaldt, H.P.; Schaaf, H. Value and reliability of anthropometric measurements of cranial deformity in early childhood. J. Cranio-Maxillofac. Surg. 2011, 39, 24–29. [Google Scholar] [CrossRef]
- Loveday, B.P.T.; de Chalain, T.B. Active Counterpositioning or Orthotic Device to Treat Positional Plagiocephaly? J. Craniofacial Surg. 2001, 12, 308–313. [Google Scholar] [CrossRef]
- D’Souza, P.; Hanson, K.A.; Pillutla, P.; Presto, P.; Nagy, L. Child Abuse and Deformational Plagiocephaly in a West Texas Hospital System. J. Neurosci. Rural Pract. 2020, 11, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Holowka, M.A.; Reisner, A.; Giavedoni, B.; Lombardo, J.R.; Coulter, C. Plagiocephaly Severity Scale to Aid in Clinical Treatment Recommendations. J. Craniofacial Surg. 2017, 28, 717–722. [Google Scholar] [CrossRef]
- Visa, S.; Ramsay, B.; Ralescu, A.L.; Van Der Knaap, E. Confusion Matrix-based Feature Selection. MAICS 2011, 710, 120–127. [Google Scholar]
- Flach, P.A.; Kull, M. Precision-Recall-Gain curves: PR analysis done right. In Proceedings of the 28th International Conference on Neural Information Processing Systems, Montreal, QC, Canada, 7–12 December 2015; pp. 838–846. [Google Scholar]
- Luque, A.; Carrasco, A.; Martín, A.; de las Heras, A. The impact of class imbalance in classification performance metrics based on the binary confusion matrix. Pattern Recognit. 2019, 91, 216–231. [Google Scholar] [CrossRef]
- Mandl, T.; Modha, S.; Majumder, P.; Patel, D.; Dave, M.; Mandlia, C.; Patel, A. Overview of the HASOC track at FIRE 2019: Hate Speech and Offensive Content Identification in Indo-European Languages. In Proceedings of the 11th Forum for Information Retrieval Evaluation, Kolkata, India, 3–5 January 2019; pp. 14–17. [Google Scholar]
- Barbero-García, I.; Lerma, J.L.; Miranda, P.; Marqués-Mateu, Á. Smartphone-based photogrammetric 3D modelling assessment by comparison with radiological medical imaging for cranial deformation analysis. Measurement 2019, 131, 372–379. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) Cranial Ratio | ||
| Brachycephaly Severity | Level | Value |
| Normal | 0 | 75.0–84.9 |
| Mild Brachycephaly | 1 | 85.0–94.9 |
| Moderate Brachycephaly | 2 | 95.0–104.9 |
| Severe Brachycephaly | 3 | ≥105.0 |
| (B) Cranial Vault Asymmetry Index | ||
| Plagiocephaly Severity | Level | Value |
| Normal | 0 | ≤3.49 |
| Mild Plagiocephaly | 1 | 3.50–6.24 |
| Moderate Plagiocephaly I | 2 | 6.25–8.74 |
| Moderate Plagiocephaly II | 3 | 8.75–10.99 |
| Severe Plagiocephaly | 4 | ≥11.00 |
| (A) Cranial Ratio | |||
| Brachycephaly Severity | Class | CR Value | No. Cases |
| Normal | 0 (Level 0)) | 75.0–84.9 | 23 |
| Moderate Brachycephaly | 1 (Level 1) | 85.0–94.9 | 91 |
| Severe Brachycephaly | 2 (Level 2 & 3) | ≥95.0 | 60 |
| Total | 174 | ||
| (B) Cranial Vault Asymmetry Index | |||
| Plagiocephaly Severity | Class | CVAI Value | No. Cases |
| Normal | 0 (Level 0) | ≤3.49 | 43 |
| Moderate Plagiocephaly | 1 (Level 1 & 2) | 3.50–8.74 | 88 |
| Severe Plagiocephaly | 2 (Level 3 & 4) | ≥8.75 | 43 |
| Total | 174 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callejas Pastor, C.A.; Jung, I.-Y.; Seo, S.; Kwon, S.B.; Ku, Y.; Choi, J. Two-Dimensional Image-Based Screening Tool for Infants with Positional Cranial Deformities: A Machine Learning Approach. Diagnostics 2020, 10, 495. https://doi.org/10.3390/diagnostics10070495
Callejas Pastor CA, Jung I-Y, Seo S, Kwon SB, Ku Y, Choi J. Two-Dimensional Image-Based Screening Tool for Infants with Positional Cranial Deformities: A Machine Learning Approach. Diagnostics. 2020; 10(7):495. https://doi.org/10.3390/diagnostics10070495
Chicago/Turabian StyleCallejas Pastor, Cecilia A., Il-Young Jung, Shinhye Seo, Soon Bin Kwon, Yunseo Ku, and Jayoung Choi. 2020. "Two-Dimensional Image-Based Screening Tool for Infants with Positional Cranial Deformities: A Machine Learning Approach" Diagnostics 10, no. 7: 495. https://doi.org/10.3390/diagnostics10070495