Technical Assessment of Ultrasonic Cerebral Tomosphygmography and New Scientific Evaluation of Its Clinical Interest for the Diagnosis of Electrohypersensitivity and Multiple Chemical Sensitivity

Abstract
:1. Introduction
2. Scientific Background
3. What Is UCTS?
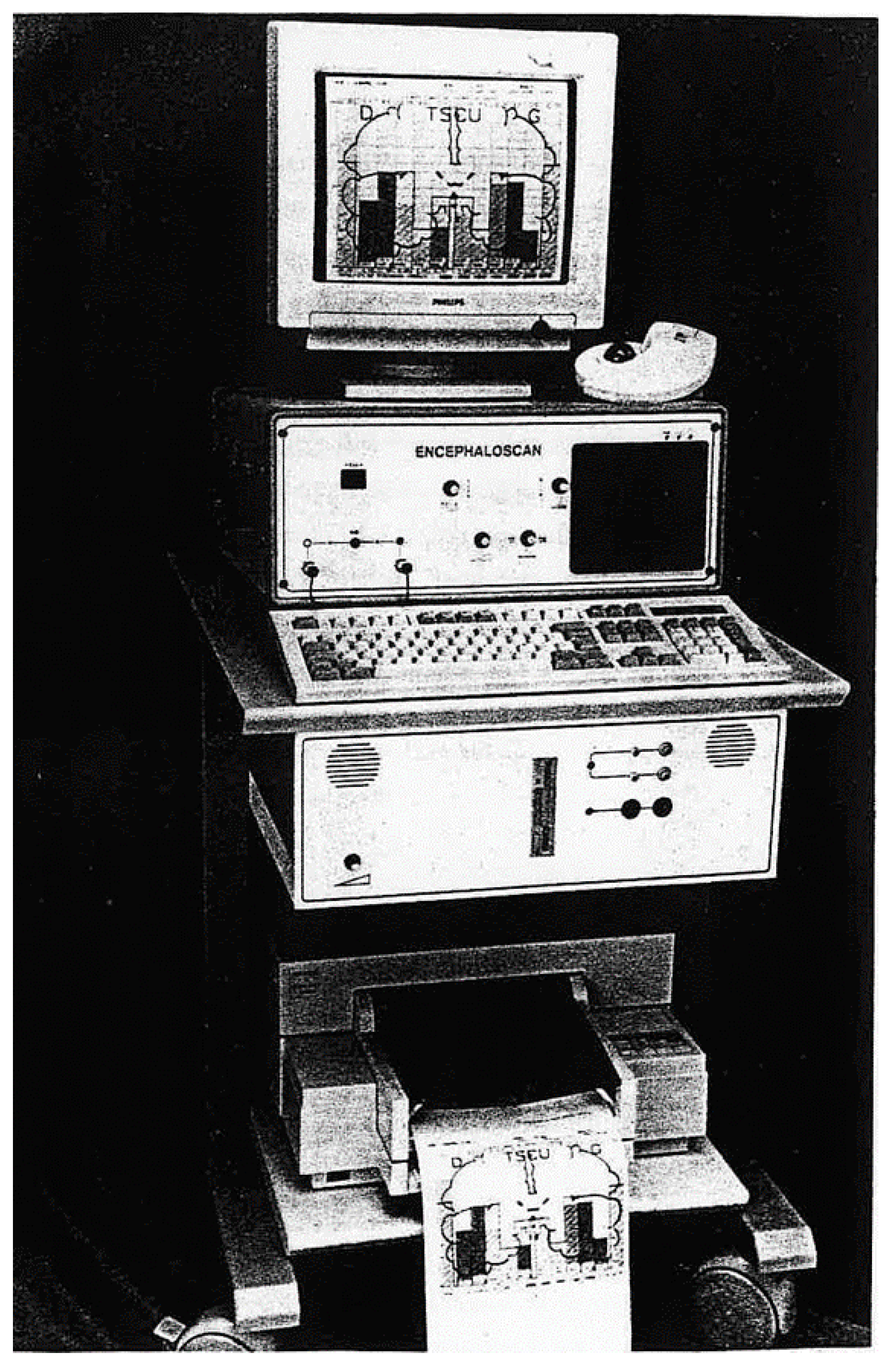
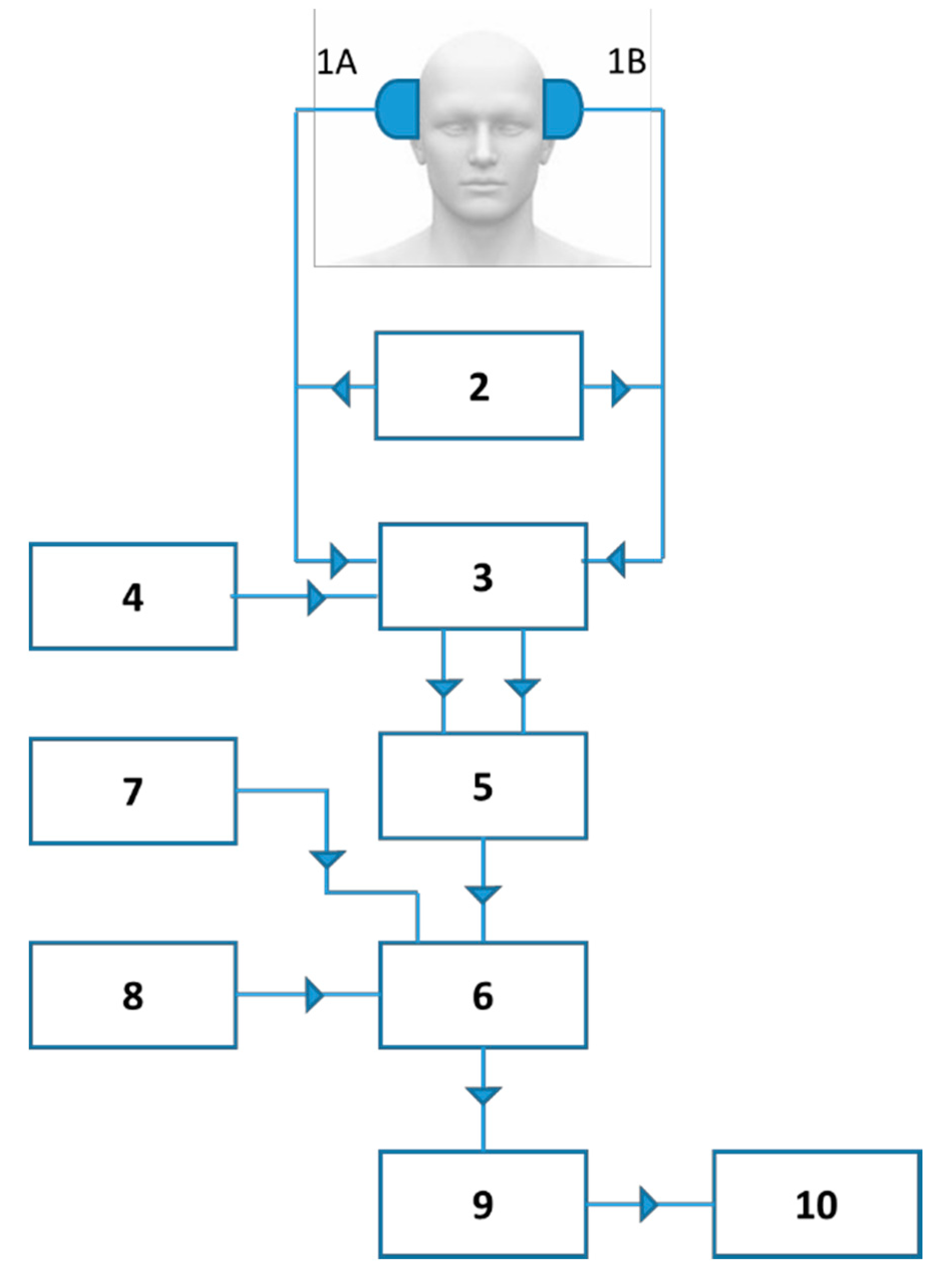
4. UCTS Engineering and Technical Equipment to Measure and Record Spontaneous Cerebral Pulsations
5. Modalities of Use
5.1. Type of Probe and Positioning
5.2. Calibration—Definition of the Pulsometric Index
5.3. The Different Temporal Regions Explored
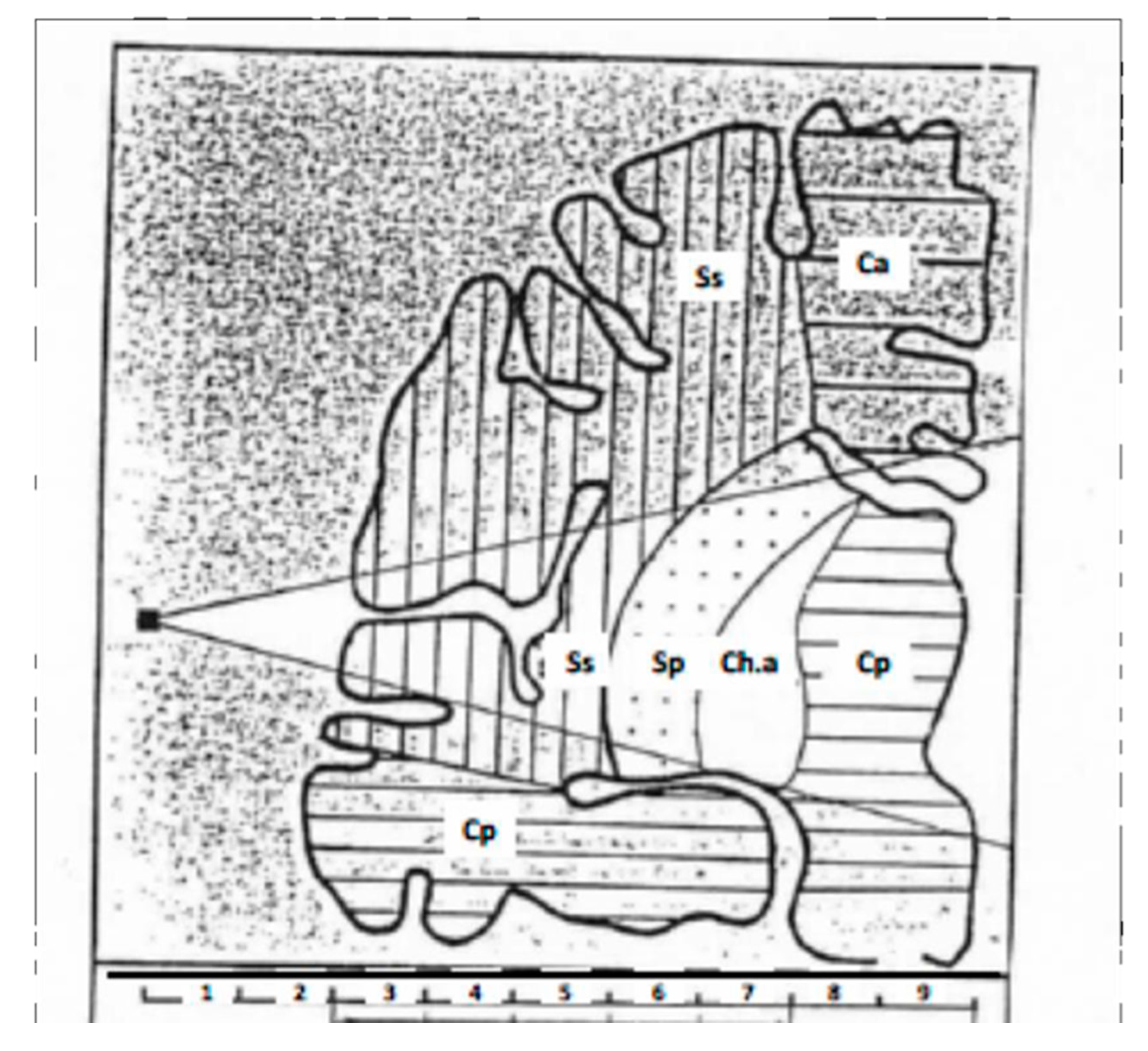
6. Search for Correspondence between the Anatomical Regions So Far Individualized in Temporal Lobes and the Different Neurovascular Structures They Are Associated with
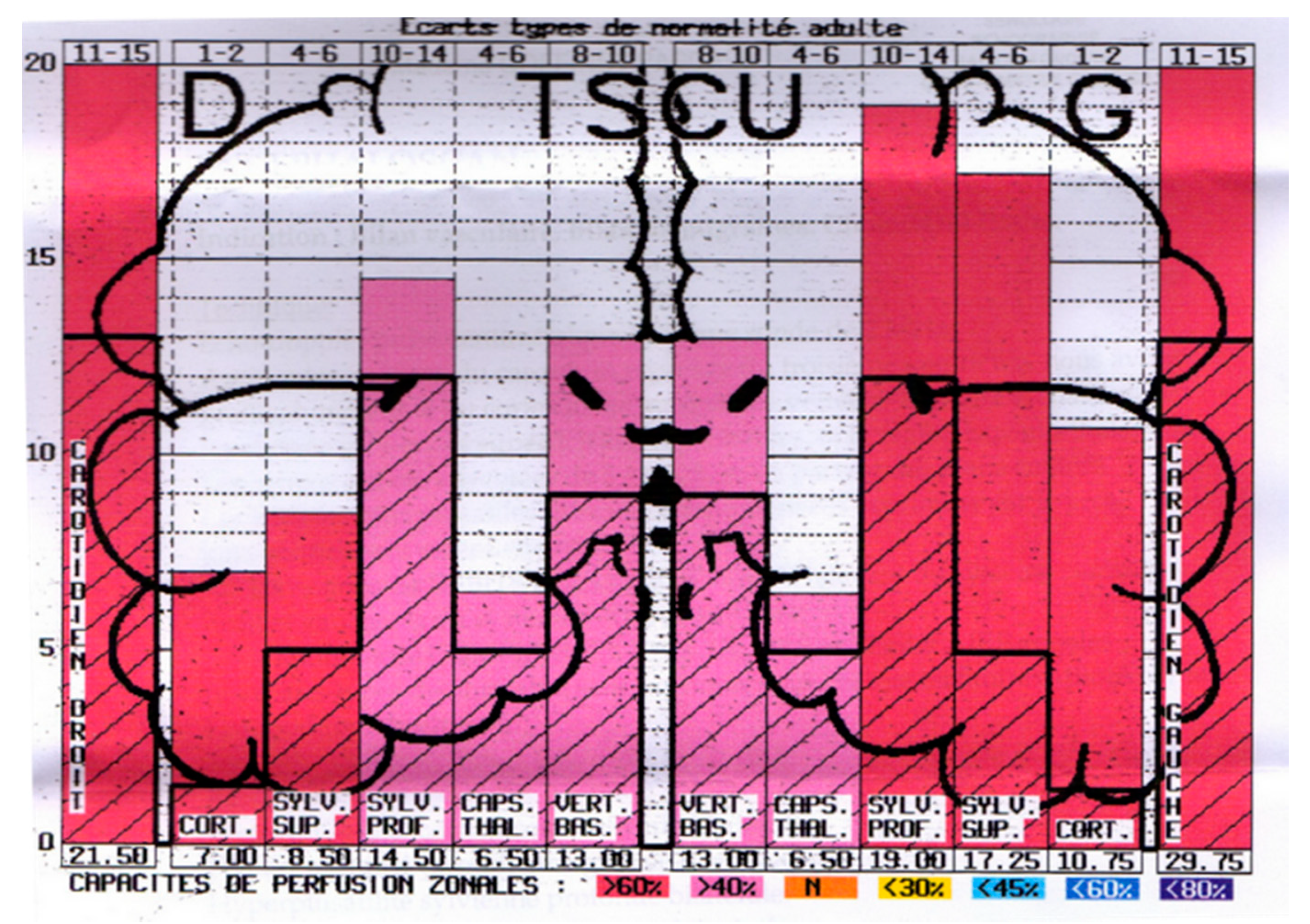
7. Presentation of Results as Pictograms
8. Physio-Pathological Relevance
9. The UCTS Compared to Transcranial Doppler
10. Clinical Assessment of UCTS Use for the Diagnosis of EHS and MCS
Funding
Acknowledgments
Conflicts of Interest
References
- WHO (World Health Organization). Electromagnetic Fields and Public Health, Electromagnetic Hypersensitivity. WHO Fact Sheet No. 296. 2005. Available online: http://www.who.int/peh-emf/publications/facts/fs296/en/ (accessed on 15 November 2019).
- Hansson Mild, K.; Repacholi, M.; van Deventer, E.; Ravazzani, P. Working Group Report. In Proceedings of the International Workshop on EMF hypersensitivity, Prague, Czech Republic, 25–27 October 2004; WHO Press: Milan, Italy, 2006; pp. 15–26. [Google Scholar]
- Belpomme, D.; Campagnac, C.; Irigaray, P. Reliable disease biomarkers characterizing and identifying electrohypersensitivity and multiple chemical sensitivity as two etiopathogenic aspects of a unique pathological disorder. Rev. Environ. Health 2015, 30, 251–271. [Google Scholar] [CrossRef] [PubMed]
- Irigaray, P.; Catherine, G.; Carine, H.; Pierre, M.; Dominique, B. Beneficial effects of a Fermented Papaya Preparation for the treatment of electrohypersensitivity self-reporting patients: Results of a phase I-II clinical trial with special reference to cerebral pulsation measurement and oxidative stress analysis. Funct. Foods Health Dis. 2018, 8, 122–144. [Google Scholar] [CrossRef]
- Irigaray, P.; Lebar, P.; Belpomme, D. How Ultrasonic Cerebral Tomosphygmography can Contribute to the Diagnosis of Electrohypersensitivity. J. Clin. Diagn. Res. 2018, 6, 143. [Google Scholar]
- Belpomme, D.; Irigaray, P. Electrohypersensitivity as a Newly Identified and Characterized Neurologic Pathological Disorder: How to Diagnose, Treat, and Prevent It. Int. J. Mol. Sci. 2020, 21, 1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ANSES (French Agency for Food, Environmental and Occupational Health & Safely). Hypersensibilite Electromagnetique Ou Intolerance Environmentale Idiopathique Attribuee Aux Champs Electromagnetiques. Rapport du groupe de travail “Radiofrequence et Sante”). 2018. Available online: https://www.anses.fr/fr/system/files/AP2011SA0150Ra.pdf (accessed on 12 December 2018).
- Milbled, G.; Agneray, H.; Parquet, P.J.; Wyremblewski, F. Ultrasonic sphygmoencephalography. Lille Med. 1966, 11, 959–960. [Google Scholar] [PubMed]
- Leksell, L. Echo-encephalography. I. Detection of intracranial complications following head injury. Acta Chir. Scand. 1956, 110, 301–315. [Google Scholar] [PubMed]
- Vlieger, M.D.; Ridder, H.J. Use of Echoencephalography. Neurology 1959, 9, 216. [Google Scholar] [CrossRef]
- Ter Braak, J.W.G.; Crezée, P.; Grandia, W.A.M.; De Vlieger, M. The significance of some reflections in “Echo-encephalography”. Acta Neurochir. 1961, 9, 382–397. [Google Scholar] [CrossRef]
- Jeppsson, S. A method for recording the intracranial pressure with the aid of the echoencephaiographic technique. A preliminary report. Acta Chir. Scand. 1964, 128, 218–224. [Google Scholar]
- Planiol, T.; Fischgoid, H. Etude des pulsations cerebrales a I’aide de I’echographie ultrasonore. C. R. Soc. Biol. 1965, 159, 1294–1299. [Google Scholar]
- Planiol, T.; Pottier, J.M. Registration of cerebral echo-pulsations and comparison with rheo-encephalographic oscillations. In Proceedings in Echo-Encephalography; Kazner, E., Schiefer, W., Zulch, K., Eds.; Springer: Berlin, Germany, 1968; pp. 189–192. [Google Scholar]
- Wallace, W.K.; Avant, W.S.; McKinney, W.M.; Thurstone, F.L. Ultrasonic techniques for measuring intracranial pulsations. Research and clinical studies. Neurology 1966, 16, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Hiromoto, H.; Uchihashi, H.; Tachibana, U.; Takeo, K.; Shirahata, M.; Matsuno, T. Study on intracranial echo pulsations. Proc. Jpn. Soc. Ultrason. Med. 1968, 14, 16. [Google Scholar]
- Planiol, T.; Pourcelot, L.; Pottier, J.M.; Fleyrac, R. Study of various factors influencing the cerebral circulation with the aid of ultrasound and rheography. In Ultrasonographia Medica; Bock, J., Ossoinig, K., Eds.; Verlag Wiener Med. Akad: Vienna, Austria, 1971; pp. 267–281. [Google Scholar]
- Lepetit, J.M. Les critères circulatoires, et biologiques de la mort du cerveau. Echoencephalographie. Neuro. Chirurg. 1972, 18, 9–48. [Google Scholar]
- Lepetit, J.M.; Pefferkorn, J.P.; Dany, A. Pulsatile echography and irreversible loss of cerebral functions. Ann. Anesthesiol. Fr. 1974, 15, 101–108. [Google Scholar] [PubMed]
- Lepetit, J.M.; Chanchole, S.; Dany, A.; Ravon, R.; Bokor, J.; Pefferkorn, J.P. New technic of cerebral function examination: Centimetric ultrasound recording of cerebral pulsativity. Application to the diagnosis of intracranial tumors. Rev. Electroencéphalogr. Neurophysiol. Clin. 1976, 6, 400–407. [Google Scholar] [PubMed]
- Parini, M.; Lepetit, J.M.; Dumas, M.; Tapie, P.; Lemoine, J. Ultrasonic cerebral tomosphygmography. Application in 143 healthy subjects. Agressologie 1984, 25, 585–589. [Google Scholar]
- Barnes, R.W.; Binkley, R.P.; Havard, G. Detection of vascular disease using R-wave to echo activity delay time. In Proceedings of the 23rd Annual Meeting of AIUM, San Diego, CA, USA, 19–23 October 1978; Volume 1, p. 101. [Google Scholar]
- Wagshul, M.E.; Eide, P.K.; Madsen, J.R. The pulsating brain: A review of experimental and clinical studies of intracranial pulsatility. Fluids Barriers CNS 2011, 8, 5. [Google Scholar] [CrossRef] [Green Version]
- White, D. Pulsatile echoencephalography. Ultrasound Med. Biol. 1981, 7, 335–364. [Google Scholar] [CrossRef]
- White, D. The early development of neurosonology: III. Pulsatile echoencephalography and Doppler techniques. Ultrasound Med. Biol. 1992, 18, 323–376. [Google Scholar] [CrossRef]
- Chovin, C. Echotomopulsographe Cérébrale ou Tomosphygmographie Cérébrale Ultra- Sonore: A Propos de L’exploration Pulsographique de 50 Hématomes Intra-Cérébraux Spontanés. Ph.D. Thesis, Faculty of Medicine and Pharmacy, Limoges, France, 1985. [Google Scholar]
- Lassen, N.A.; Christensen, M.S. Physiology of cerebral blood flow. Br. J. Anaesth. 1976, 48, 719–734. [Google Scholar] [CrossRef] [Green Version]
- Dardaillon, I. Etude de Faisabilité et Intérêt de la Mesure de la Pulsatilité Cérébrale par la Tomosphygmographie Cérébrale Ultrasonore au Cours de la Chirurgie Carotidienne. Ph.D. Thesis, Faculty of medicine, Limoges, France, 1994. [Google Scholar]
- Aaslid, R.; Markwalder, T.-M.; Nornes, H. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. J. Neurosurg. 1982, 57, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Parini-Betz, G. La Tomosphygmographie Cérébrale Ultrasonore: Aspects Tomosphygmographiques de 69 Accidents Vasculaires Cérébraux. Ph.D. Thesis, Faculty of Medicine and Pharmacy, Limoges, France, 1983. [Google Scholar]
- Clement, J.P. Contribution de la Tomosphygmographie Cérébrale Ultrasonore au Diagnostic des Démences. Ph.D. Thesis, Faculty of Medicine and Pharmacy, Limoges, France, 1988. [Google Scholar]
- Dany, F.; Lepetit, J.M.; Kim, M.; Tapie, P.; Christides, C.; Gros, J.P.; Rohee, M. Pulsatile echography (ultrasonic cerebral tomosphygmography) in carotid and vertebral pathology. Surgical applications. J. Mal. Vasc. 1985, 10, 189–196. [Google Scholar] [PubMed]
- Cazes-Garnaud, C. Apport de la Tomosphygmographie Cérébrale Ultrasonore Dans le Bilan Pré-Opératoire et la Surveillance des Endartériectomies Carotidiennes. Ph.D. Thesis, Faculty of Medicine and Pharmacy, Limoges, France, 1987. [Google Scholar]
- Garnaud, V. Apport de la Tomosphygmographie Cérébrale Ultrasonore Dans le Bilan Bilan Fonctionnel des Anastomoses Temporo-Sylviennes. Ph.D. Thesis, Faculty of Medicine and Pharmacy, Limoges, France, 1985. [Google Scholar]
- Belpomme, D.; Hardell, L.; Belyaev, I.; Burgio, E.; Carpenter, D.O. Thermal and non-thermal health effects of low intensity non-ionizing radiation: An international perspective. Environ. Pollut. 2018, 242, 643–658. [Google Scholar] [CrossRef]
- Irigaray, P.; Caccamo, D.; Belpomme, D. Oxidative stress in electrohypersensitivity self-reporting patients: Results of a prospective in vivo investigation with comprehensive molecular analysis. Int. J. Mol. Med. 2018, 42, 1885–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heuser, G.; Heuser, S.A. Functional brain MRI in patients complaining of electrohypersensitivity after long term exposure to electromagnetic fields. Rev. Environ. Health 2017, 32, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Greco, F. New Independent Analysis Confirming the Interest of Ultrasonic Cerebral Tomosphygmography for the Diagnosis of Electrohypersensitivity and/or Chemical Sensitivity; Anesthesia and Intensive Care Unit, University Hospital of Montpellier: Montpellier, France, 2020. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Centimeters 3 and 4 | Cortico-subcortical region |
| Centimeters 3–5 | Superficial Sylvian region |
| Centimeters 5–7 | Deep Sylvian region |
| Centimeter 7 | Intermediate region (capsulo-thalamic) |
| Centimeters 3–7 | Carotid region |
| Pulsometric Index | Very High | High | Normal | Slightly Low | Low | Very Low | Extremely Low |
|---|---|---|---|---|---|---|---|
| Cortico-Subcortical | 4–6 | 2–4 | 1–2 | 0.5–1 | 0.25–0.50 | 0–0.25 | 0 |
| Superficial Sylvian | 8–12 | 6–8 | 4–6 | 3–4 | 2–3 | 0.50–2 | 0–0.50 |
| Deep Sylvian | 18–22 | 14–18 | 10–14 | 6–10 | 4–6 | 2–4 | 0–2 |
| Global Carotid | 20–25 | 15–20 | 11–15 | 8–11 | 5–8 | 3–5 | 0–3 |
| Intermediate | 7.5–8.5 | 6–7.5 | 4–6 | 3–4 | 2–3 | 1–2 | 0 |
| Vertebro-Basilar | 13–16 | 10–13 | 8–10 | 6–8 | 4–6 | 2–4 | 0–2 |
| Temporal Lobe | Tissue Areas Analyzed | Apparently Healthy Subjects ± SD n = 84 | EHS Patients ± SD n = 65 | p ** | EHS-MCS Patients ± SD n = 29 | p *** | MCS Patients ± SD n = 6 | p **** |
|---|---|---|---|---|---|---|---|---|
| Right | carotidian | 20.39 ± 4.33 | 12.74 ± 4.25 | <0.00001 | 12.38 ± 3.58 | <0.00001 | 12.75 ± 2.12 | 0.0004 |
| cortical-subcortical | 6.02 ± 2.90 | 5.26 ± 3.01 | 0.19 | 4.91 ± 3.04 | 0.12 | 4.25 ± 1.68 | 0.19 | |
| superficial MCA | 10.38 ± 3.99 | 7.79 ± 3.55 | 0.00055 | 7.97 ± 3.89 | 0.013 | 8.55 ± 1.97 | 0.32 | |
| deep MCA | 14.40 ± 2.44 | 7.47 ± 2.78 | <0.00001 | 7.82 ± 2.34 | <0.00001 | 8.50 ± 1.57 | <0.00001 | |
| capsulo-thalamic | 5.81 ± 0.96 | 2.14 ± 1.56 | <0.00001 | 2.22±1.57 | <0.00001 | 3.00 ± 0.59 | <0.00001 | |
| vertebro-basilar | 11.04 ± 1.65 | 8.02 ± 2.12 | <0.00001 | 8.45 ± 1.61 | <0.00001 | 7.55 ± 0.94 | <0.00001 | |
| Left | vertebro-basilar | 10.95 ± 1.81 | 5.22 ± 2.71 | <0.00001 | 5.55 ± 3.04 | <0.00001 | 5.40 ± 3.34 | <0.00001 |
| capsulo-thalamic | 5.32 ± 1.38 | 3.24 ± 2.19 | <0.00001 | 3.19 ± 2.28 | <0.00001 | 3.00 ± 2.21 | 0.0016 | |
| deep MCA | 13.89 ± 2.54 | 9.77 ± 3.36 | <0.00001 | 9.33 ± 3.19 | <0.00001 | 6.95 ± 3.92 | <0.00001 | |
| superficial MCA | 11.29 ± 4.25 | 8.63 ± 3.51 | 0.0005 | 8.81 ± 3.61 | 0.012 | 7.15 ± 2.99 | 0.039 | |
| cortical-subcortical | 6.88 ± 3.50 | 5.06 ± 2.93 | 0.004 | 5.34 ± 3.25 | 0.063 | 4.95 ± 3.00 | 0.24 | |
| carotidian | 20.58 ± 5.09 | 14.85 ± 4.55 | <0.00001 | 17.27 ± 13.58 | 0.15 | 11.90 ± 2.95 | 0.0005 |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, F. Technical Assessment of Ultrasonic Cerebral Tomosphygmography and New Scientific Evaluation of Its Clinical Interest for the Diagnosis of Electrohypersensitivity and Multiple Chemical Sensitivity. Diagnostics 2020, 10, 427. https://doi.org/10.3390/diagnostics10060427
Greco F. Technical Assessment of Ultrasonic Cerebral Tomosphygmography and New Scientific Evaluation of Its Clinical Interest for the Diagnosis of Electrohypersensitivity and Multiple Chemical Sensitivity. Diagnostics. 2020; 10(6):427. https://doi.org/10.3390/diagnostics10060427
Chicago/Turabian StyleGreco, Frédéric. 2020. "Technical Assessment of Ultrasonic Cerebral Tomosphygmography and New Scientific Evaluation of Its Clinical Interest for the Diagnosis of Electrohypersensitivity and Multiple Chemical Sensitivity" Diagnostics 10, no. 6: 427. https://doi.org/10.3390/diagnostics10060427