Measuring Spinal Mobility Using an Inertial Measurement Unit System: A Validation Study in Axial Spondyloarthritis

 ,
,  , , , ,
, , , ,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
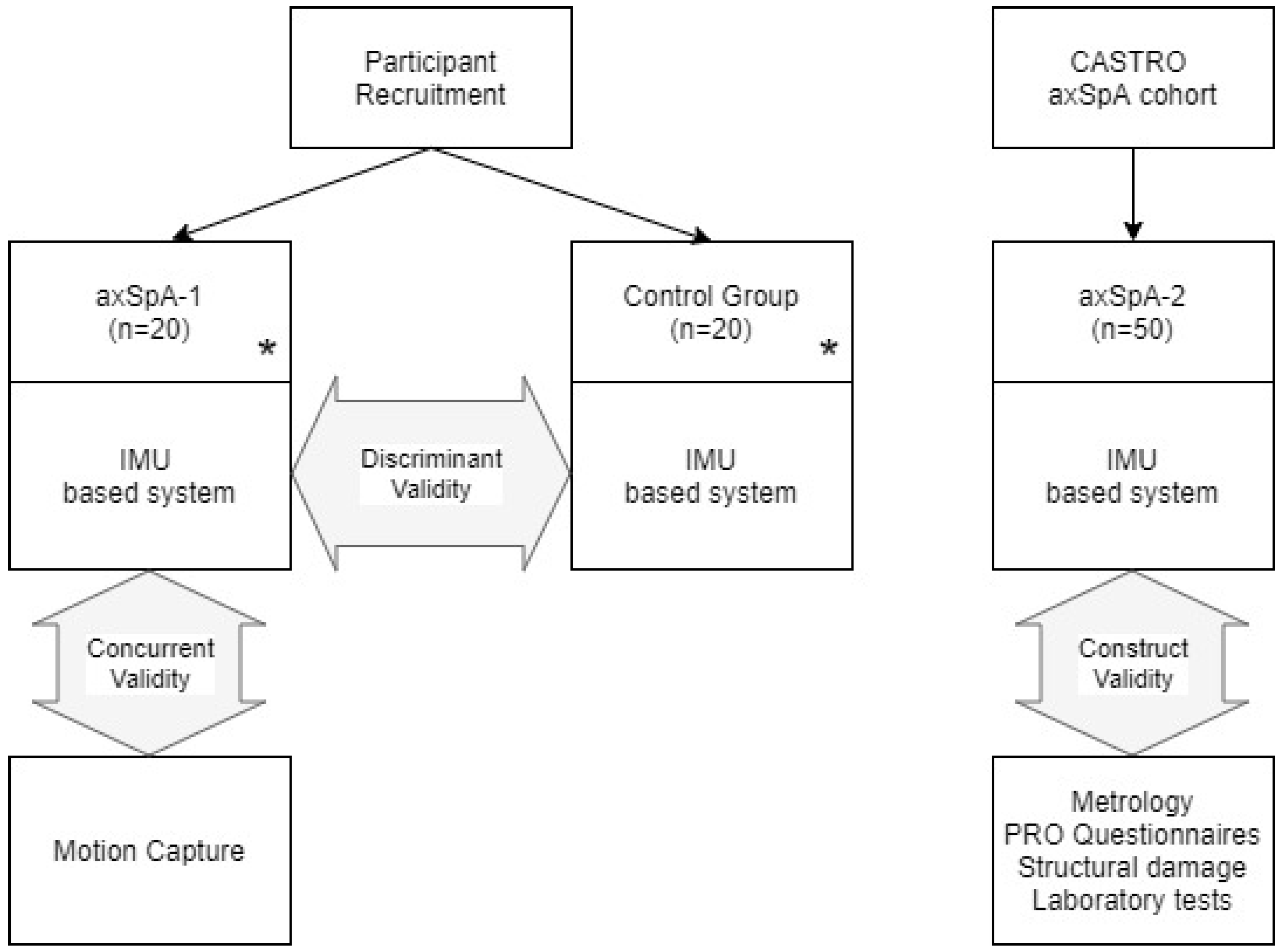
2.1. Study Population
2.2. Data Collection and Assessment
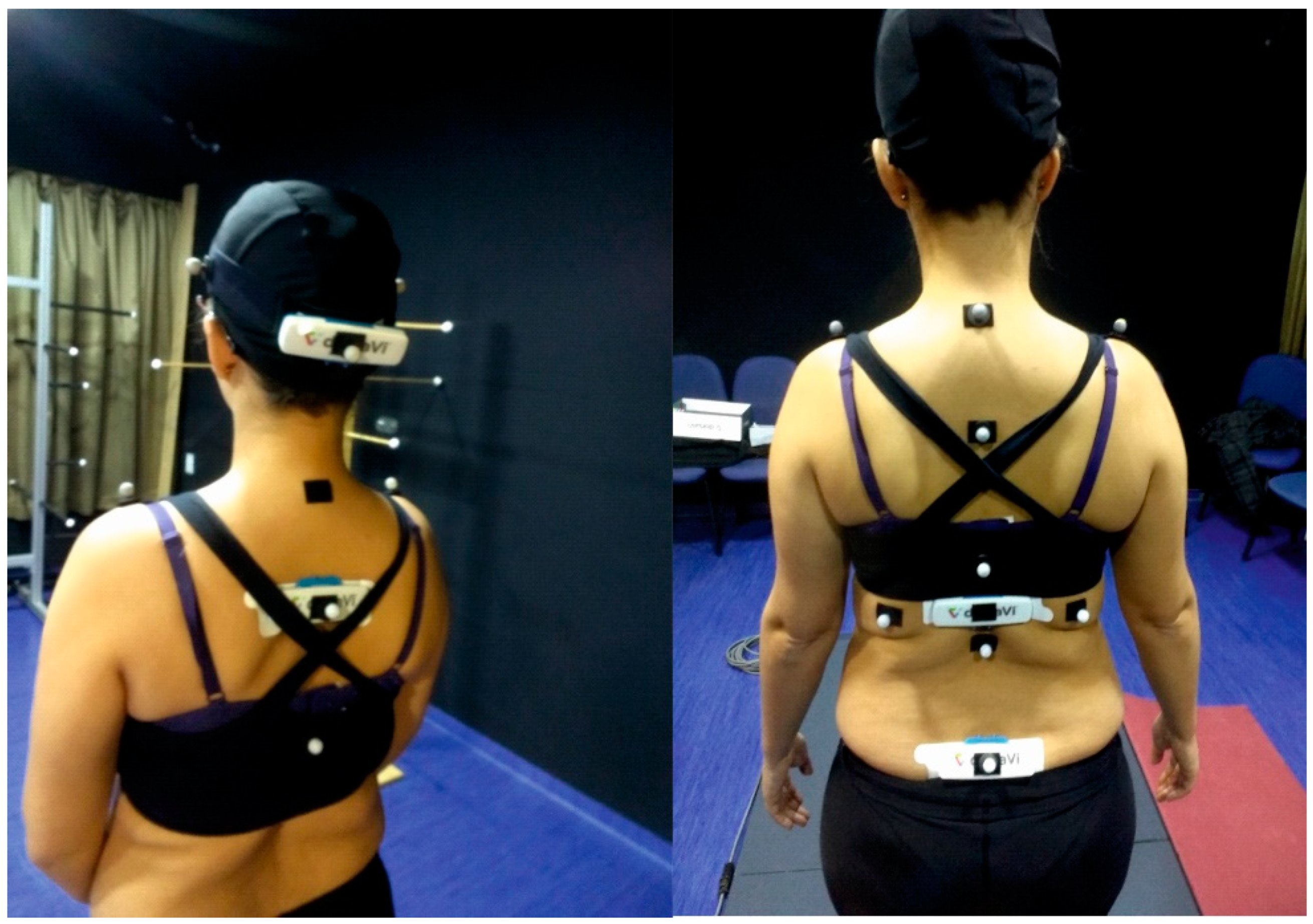
2.3. Instrumentation
2.4. Sample Size and Statistical Analysis
3. Results
3.1. Subjects
3.2. Discriminant Validity
3.3. Concurrent Validity
3.4. Construct Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dougados, M.; Baeten, D. Spondyloarthritis. Lancet 2011, 377, 2127–2137. [Google Scholar] [CrossRef]
- López-Medina, C.; Schiotis, R.E.; Font-Ugalde, P.; Castro-Villegas, M.C.; Calvo-Gutiérrez, J.; Ortega-Castro, R.; Jiménez-Gasco, R.; Escudero-Contreras, A.; Collantes-Estévez, E.; REGISPONSER Working Group. Assessment of Fatigue in Spondyloarthritis and Its Association with Disease Activity. J. Rheumatol. 2016, 43, 751–757. [Google Scholar]
- Calvo-Gutierrez, J.; Garrido-Castro, J.L.; Gil-Cabezas, J.; Gonzalez-Navas, C.; Ugalde, P.F.; Carmona, L.; Collantes-Estevez, E. Is spinal mobility in patients with spondylitis determined by age, structural damage, and inflammation? Arthritis Care Res. 2015, 67, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.; Landewé, R.; Braun, J.; Hermann, K.G.A.; Baker, D.; Van Der Heijde, D. Both structural damage and inflammation of the spine contribute to impairment of spinal mobility in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2010, 69, 1465–1470. [Google Scholar] [CrossRef]
- Van Der Heijde, D.; Calin, A.; Dougados, M.; Khan, M.A.; Van Der Linden, S.; Bellamy, N. Selection of instruments in the core set for DC-ART, SMARD, physical therapy, and clinical record keeping in ankylosing spondylitis. Progress report of the ASAS Working Group. J. Rheumatol. 1999, 26, 951–954. [Google Scholar] [PubMed]
- Kennedy, L.G.; Jenkinson, T.R.; Mallorie, P.A.; Whitelock, H.C.; Garrett, S.L.; Calin, A. Ankylosing spondylitis: The correlation between a new metrology score and radiology. Rheumatology 1995, 34, 767–770. [Google Scholar] [CrossRef]
- Wanders, A.; Landewé, R.; Dougados, M.; Mielants, H.; Van Der Linden, S.; Van Der Heijde, D. Association between radiographic damage of the spine and spinal mobility for individual patients with ankylosing spondylitis: Can assessment of spinal mobility be a proxy for radiographic evaluation? Ann. Rheum. Dis. 2005, 64, 988–994. [Google Scholar] [CrossRef] [Green Version]
- Ramiro, S.; Van Tubergen, A.; Stolwijk, C.; Van Der Heijde, D.; Royston, P.; Landewé, R.; Kvien, T.K. Reference intervals of spinal mobility measures in normal individuals: The mobility study. Ann. Rheum. Dis. 2015, 74, 1218–1224. [Google Scholar] [CrossRef]
- Sieper, J.; Rudwaleit, M.; Baraliakos, X.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Dougados, M.; Hermann, K.G.; Landewe, R.; Maksymowych, W.; et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: A guide to assess spondyloarthritis. Ann. Rheum. Dis. 2009, 68 (Suppl. 2), ii1–ii44. [Google Scholar] [CrossRef]
- Jenkinson, T.R.; Mallorie, P.A.; Whitelock, H.C.; Kennedy, L.G.; Garrett, S.L.; Calin, A. Defining spinal mobility in ankylosing spondylitis (AS): The Bath AS metrology index. J. Rheumatol. 1994, 21, 1694–1698. [Google Scholar]
- Calvo-Gutiérrez, J.; Garrido-Castro, J.L.; González-Navas, C.; Castro-Villegas, M.C.; Ortega-Castro, R.; López-Medina, C.; Font-Ugalde, P.; Escudero-Contreras, A.; Collantes-Estévez, E. Inter-rater reliability of clinical mobility measures in ankylosing spondylitis. BMC Musculoskelet. Disord. 2016, 17, 382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in ankylosing spondylitis: The bath ankylosing spondylitis disease activity index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar] [PubMed]
- Garrido-Castro, J.L.; Medina-Carnicer, R.; Schiottis, R.; Galisteo, A.M.; Collantes-Estevez, E.; Gonzalez-Navas, C. Assessment of spinal mobility in ankylosing spondylitis using a video-based motion capture system. Man. Ther. 2012, 17, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Castro, J.L.; Escudero, A.; Medina-Carnicer, R.; Galisteo, A.M.; Gonzalez-Navas, C.; Carmona, L.; Collantes-Estevez, E. Validation of a new objective index to measure spinal mobility: The University of Cordoba Ankylosing Spondylitis Metrology Index (UCOASMI). Rheumatol. Int. 2014, 34, 401–406. [Google Scholar] [CrossRef]
- Garrido-Castro, J.L.; Curbelo, R.; Mazzucchelli, R.; Domínguez-González, M.E.; Gonzalez-Navas, C.; Flores Robles, B.J.; Zarco, P.; Mulero, J.; Cea-Calvo, L.; Arteaga, M.J.; et al. High Reproducibility of an Automated Measurement of Mobility for Patients with Axial Spondyloarthritis. J. Rheumatol. 2018, 45, 1383–1388. [Google Scholar] [CrossRef]
- Tunca, C.; Pehlivan, N.; Ak, N.; Arnrich, B.; Salur, G.; Ersoy, C. Inertial sensor-based robust gait analysis in non-hospital settings for neurological disorders. Sensors 2017, 17, 825. [Google Scholar] [CrossRef] [Green Version]
- Cardarelli, S.; Verdini, F.; Mengarelli, A.; Strazza, A.; Di Nardo, F.; Burattini, L.; Fioretti, S. Position estimation of an IMU placed on Pelvis through meta-heuristically optimised WFLC. In World Congress on Medical Physics and Biomedical Engineering 2018; Springer: Singapore, 2019. [Google Scholar]
- Odonkor, C.; Kuwabara, A.; Tomkins-Lane, C.; Zhang, W.; Muaremi, A.; Leutheuser, H.; Sun, R.; Smuck, M. Gait features for discriminating between mobility-limiting musculoskeletal disorders: Lumbar spinal stenosis and knee osteoarthritis. Gait Posture 2020, 80, 96–100. [Google Scholar] [CrossRef]
- Wong, W.Y.; Wong, M.S. Trunk posture monitoring with inertial sensors. Eur. Spine J. 2008, 17, 743–753. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.M.; Haq, I.; Lee, R.Y. A novel approach to the clinical evaluation of differential kinematics of the lumbar spine. Man. Ther. 2013, 18, 130–135. [Google Scholar] [CrossRef]
- Williams, J.M.; Haq, I.; Lee, R.Y. An experimental study investigating the effect of pain relief from oral analgesia on lumbar range of motion, velocity, acceleration and movement irregularity. BMC Musculoskelet. Disord. 2014, 15, 304. [Google Scholar] [CrossRef] [Green Version]
- Schall, M.C.; Fethke, N.B.; Chen, H.; Gerr, F. A comparison of instrumentation methods to estimate thoracolumbar motion in field-based occupational studies. Appl. Ergon. 2015, 48, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Carmona-Pérez, C.; Garrido-Castro, J.L.; Vidal, F.T.; Alcaraz-Clariana, S.; García-Luque, L.; Alburquerque-Sendín, F.; Rodrigues-De-Souza, D.P. Concurrent validity and reliability of an inertial measurement unit for the assessment of craniocervical range of motion in subjects with cerebral palsy. Diagnostics 2020, 10, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta-Vargas, A.I.; Galán-Mercant, A.; Williams, J.M. The use of inertial sensors system for human motion analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swinnen, T.W.; Scheers, T.; Lefevre, J.; Dankaerts, W.; Westhovens, R.; De Vlam, K. Physical activity assessment in patients with axial spondyloarthritis compared to healthy controls: A technology-based approach. PLoS ONE 2014, 9, e85309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolink, S.A.A.N.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.C.; Meijer, K.; Grimm, B. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit-stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med. Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef]
- Cardarelli, S.; Mengarelli, A.; Tigrini, A.; Strazza, A.; Di Nardo, F.; Fioretti, S.; Verdini, F. Single IMU Displacement and Orientation Estimation of Human Center of Mass: A Magnetometer-Free Approach. IEEE Trans. Instrum. Meas. 2019, 99, 1. [Google Scholar] [CrossRef]
- Goodvin, C.; Park, E.J.; Huang, K.; Sakaki, K. Development of a real-time three-dimensional spinal motion measurement system for clinical practice. Med. Biol. Eng. Comput. 2006, 44, 1061–1075. [Google Scholar] [CrossRef]
- Samadani, A.; Lee, A.; Kulic, D. A Spinal Motion Measurement Protocol Utilizing Inertial Sensors Without Magnetometers. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society 2018, Honolulu, HI, USA, 17–21 July 2018; Volume 2018, pp. 1–4. [Google Scholar]
- Leroy, E. Analysis of the spine through a multibody model and IMU technology. Ph.D. Thesis, Université catholique de Louvain, Ottignies-Louvain-la-Neuve, Belgium, 2019. [Google Scholar]
- Charry, E.; Umer, M.; Taylor, S. Design and validation of an ambulatory inertial system for 3-D measurements of low back movements. In Proceedings of the 7th International Conference on Intelligent Sensors, Sensor Networks and Information Processing. (ISSNIP 2011), Adelaide, Australia, 6–9 December 2011; pp. 58–63. [Google Scholar]
- Mjøsund, H.L.; Boyle, E.; Kjaer, P.; Mieritz, R.M.; Skallgård, T.; Kent, P. Clinically acceptable agreement between the ViMove wireless motion sensor system and the Vicon motion capture system when measuring lumbar region inclination motion in the sagittal and coronal planes. BMC Musculoskelet. Disord. 2017, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Laird, R.A.; Kent, P.; Keating, J.L. Modifying patterns of movement in people with low back pain -does it help? A systematic review. BMC Musculoskelet. Disord. 2012, 13, 169. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, P.V.; Small, D.; Muñoz-Esquivel, K.; Condell, J.; Cuesta-Vargas, A.; Williams, J.; Machado, P.M.; Garrido-Castro, J.L. Validity and reliability of a sensor-based electronic spinal mobility index for axial spondyloarthritis. Rheumatology 2020. [Google Scholar] [CrossRef]
- Boers, M.; Kirwan, J.R.; Wells, G.; Beaton, D.; Gossec, L.; d’Agostino, M.-A.; Conaghan, P.G.; Bingham, C.O.; Brooks, P.; Landewé, R.; et al. Developing Core Outcome Measurement Sets for Clinical Trials: OMERACT Filter 2.0. J. Clin. Epidemiol. 2014, 67, 745–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudwaleit, M.; Van Der Heijde, D.; Landewé, R.; Listing, J.; Akkoc, N.; Brandt, J.; Braun, J.; Chou, C.T.; Collantes-Estevez, E.; Dougados, M.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): Validation and final selection. Ann. Rheum. Dis. 2009, 68, 777–783. [Google Scholar] [CrossRef] [Green Version]
- Calin, A.; Garrett, S.; Whitelock, H.; O’Hea, J.; Mallorie, P.; Jenkinson, T. A new approach to defining functional ability in ankylosing spondylitis: The development of the bath ankylosing spondylitis functional index. J. Rheumatol. 1994, 21, 2281–2285. [Google Scholar] [PubMed]
- Jones, S.D.; Steiner, A.; Garrett, S.L.; Calin, A. The bath ankylosing spondylitis patient global score (BAS-G). Br. J. Rheumatol. 1996, 35, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Kiltz, U.; Van Der Heijde, D.; Boonen, A.; Cieza, A.; Stucki, G.; Khan, M.A.; Maksymowych, W.P.; Marzo-Ortega, H.; Reveille, J.; Stebbings, S.; et al. Development of a health index in patients with ankylosing spondylitis (ASAS HI): Final result of a global initiative based on the ICF guided by ASAS. Ann. Rheum. Dis. 2015, 74, 830–835. [Google Scholar] [CrossRef]
- Creemers, M.C.W.; Franssen, M.J.A.M.; Van’t Hof, M.A.; Gribnau, F.W.J.; Van De Putte, L.B.A.; Van Riel, P.L.C.M. Assessment of outcome in ankylosing spondylitis: An extended radiographic scoring system. Ann. Rheum. Dis. 2005, 64, 127–129. [Google Scholar] [CrossRef] [Green Version]
- Van Der Heijde, D.; Lie, E.; Kvien, T.K.; Sieper, J.; Van Den Bosch, F.; Listing, J.; Braun, J.; Landewe, R. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2009, 68, 1811–1818. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Haley, S.M.; Fragala-Pinkham, M.A. Interpreting Change Scores of Tests and Measures Used in Physical Therapy. Phys. Ther. 2006, 86, 735–743. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| axSpA-1 (n = 20) | Control (n = 20) | axSpA-2 (n = 50) | |||||
|---|---|---|---|---|---|---|---|
| Mean (s.d.) | Range | Mean (s.d.) | Range | p-Value | Mean (s.d.) | Range | |
| Age, years | 46 (12.0) | 25–69 | 44 (8.5) | 29–61 | 0.537 | 43 (12.3) | 25–64 |
| Sex (women/men) | 5/15 | 5/15 | 18/32 | ||||
| Disease dur., years | 24 (13.7) | 3–48 | - | - | - | 17 (13.7) | 1–50 |
| Height (m) | 1.7 (0.1) | 1.6–1.8 | 1.7 (0.1) | 1.5–2.0 | 0.963 | 1.7 (0.1) | 1.5–1.8 |
| Weight (Kg) | 75.1 (11.4) | 51.7–100.0 | 75.7 (19.8) | 45.3–103.6 | 0.915 | 70.6 (14.6) | 48.0–125.5 |
| BMI, kg/m2 | 25.1 (3.7) | 18.9–33.8 | 25.0 (4.3) | 17.7–32.1 | 0.847 | 26.1 (4.0) | 20.1–42.4 |
| BAS-G (0–10) | 4.0 (2.9) | 0.5–10 | - | - | - | 4.2 (2.6) | 0–8 |
| BASDAI (0–10) | 3.9 (2.7) | 0.4–9.4 | - | - | - | 3.7 (2.1) | 0–8.2 |
| BASFI (0–10) | 3.2 (2.7) | 0–8.8 | - | - | - | 2.7 (2.4) | 0–9.5 |
| ASDAS | 2.4 (0.9) | 0.7–4.57 | |||||
| mSASSS | 11.8 (13.7) | 0–61 | |||||
| ASAS-HI | 4.1 (3.7) | 0–12 | |||||
| axSpA-1 (n = 20) | Control (n = 20) | axSpA-2 (n = 50) | |||||
|---|---|---|---|---|---|---|---|
| Mean (s.d.) | Range | Mean (s.d.) | Range | p-Value | Mean (s.d.) | Range | |
| Cervical region IMU | |||||||
| Flexion + extension (deg) | 82.1 (24.8) | 22–116 | 99.3 (15.6) | 72–132 | 0.013 * | 95.3 (23.1) | 4–155 |
| Lateral flexion L + R (deg) | 56.2 (26.2) | 3–104 | 67.7 (12.7) | 45–97 | 0.088 | 64.5 (22.7) | 0–111 |
| Rotation L + R (deg) | 111.9 (39.1) | 36–175 | 138.6 (17.2) | 107–163 | 0.010 * | 129.7 (29.3) | 7–180 |
| L1 region IMU | |||||||
| Flexion + extension (deg) | 119.5 (23.6) | 73–166 | 139.6 (19.9) | 104–175 | 0.006 * | 124.7 (23.7) | 71–167 |
| Lateral flexion L + R (deg) | 50.5 (20.2) | 5–77 | 69.5 (12.8) | 45–99 | 0.001 * | 54.8 (16.4) | 10–82 |
| Rotation L + R (deg) | 126.3 (29.6) | 77–204 | 128.2 (24.5) | 70–191 | 0.820 | 138.1 (29.5) | 65–185 |
| Lumbar region IMU | |||||||
| Flexion + extension (deg) | 49.7 (21.4) | 8–87 | 61.4 (12.5) | 35–79 | 0.042 * | 62.2 (23.4) | 6–108 |
| Lateral flexion L + R (deg) | 41.8 (17.8) | 3–67 | 53.6 (11.6) | 33–74 | 0.018 * | 44.4 (15.1) | 1–68 |
| Rotation L + R (deg) | 21.2 (8.7) | 6–39 | 26.6 (7.1) | 14–39 | 0.038 * | 25.4 (8.7) | 11–43 |
| IUCOASMI (0–10) | 4.8 (1.9) | 1.7–8.7 | 3.1 (1.0) | 1.2–5.2 | <0.001 * | 3.9 (1.6) | 0.8–9.1 |
| Conventional metrology | |||||||
| Side flexion L + R (cm) | 11.7 (5.7) | 3–21.75 | 21.6 (16.7) | 7.25–91 | 0.019 * | 13.9 (8.1) | 2.5–52.5 |
| Tragus-to-wall distance (cm) | 13.5 (4.7) | 9.5–27 | 11.1 (1.2) | 9.25–14 | 0.037 * | 11.4 (3.9) | 1.25–28 |
| Modified Schober (cm) | 4.8 (1.9) | 0.8–6.5 | 5.3 (1.0) | 3.5–7 | 0.291 | 5.3 (1.8) | 0.5–10.25 |
| Intermalleolar distance (cm) | 95.5 (16.3) | 66–125 | 117.0 (15.4) | 86–148 | <0.001 * | 100.0 (19.6) | 50.5–138 |
| Cervical rotation L + R (deg) | 56.1 (18.1) | 21–90 | 75.0 (7.2) | 63–91 | <0.001 * | 65.5 (17.3) | 2–91.5 |
| BASMILIN (0–10) | 3.4 (1.9) | 0.8–7 | 1.7 (0.5) | 0.9–2.6 | <0.001 * | 2.8 (1.7) | 0.8–8.2 |
| 95% LoA | ||||||||
|---|---|---|---|---|---|---|---|---|
| ICC2,1 (95% CI) | R | RMSE | Bias | Lower | Upper | SEM | MDC | |
| Cervical region | ||||||||
| Flexion + extension(deg) | 0.982 (0.954, 0.993) | 0.98 | 8.01 | −4.2 | −14.2 | 5.8 | 3.6 | 10.0 |
| Lateral flexion L + R(deg) | 0.874 (0.704, 0.950) | 0.87 | 8.12 | −2.1 | −30.5 | 26.2 | 10.2 | 28.4 |
| Rotation L + R(deg) | 0.909 (0.779, 0.964) | 0.91 | 9.99 | 1.2 | −31.5 | 33.8 | 11.8 | 32.6 |
| L1 region | ||||||||
| Flexion + extension(deg) | 0.959 (0.897, 0.984) | 0.96 | 5.59 | −7.2 | −20.7 | 6.3 | 4.9 | 13.5 |
| Lateral flexion L + R(deg) | 0.988 (0.968, 0.995) | 0.99 | 3.74 | −1.9 | −8.3 | 4.5 | 2.3 | 6.4 |
| Rotation L + R(deg) | 0.913 (0.790, 0.966) | 0.92 | 3.74 | −0.4 | −25.4 | 24.5 | 9.0 | 24.9 |
| Lumbar region | ||||||||
| Flexion + extension(deg) | 0.790 (0.532, 0.913) | 0.81 | 14.11 | 5.5 | −19.7 | 30.7 | 9.0 | 25.0 |
| Lateral flexion L + R(deg) | 0.939 (0.849, 0.976) | 0.94 | 3.90 | −3.0 | −15.6 | 9.5 | 4.5 | 12.5 |
| Rotation L + R(deg) | 0.631 (0.261, 0.840) | 0.69 | 10.36 | −14.7 | −32.9 | 3.5 | 6.4 | 17.8 |
| IUCOASMI (0–10) | 0.953 (0.882, 0.982) | 0.96 | 0.58 | −0.1 | −1.2 | 1.1 | 0.4 | 1.1 |
| Lateral Flexion | TTW | mSchober | IMD | Cervical Rotation | BASMI | |
|---|---|---|---|---|---|---|
| Cervical region IMU | ||||||
| Flexion + extension | 0.56 *** | –0.69 *** | 0.51 *** | 0.70 *** | 0.85 *** | –0.82 *** |
| Lateral flexion L + R | 0.44 ** | –0.65 *** | 0.58 *** | 0.78 *** | 0.71 *** | –0.77 *** |
| Rotation L + R | 0.41 ** | –0.76 *** | 0.58 *** | 0.64 *** | 0.94 *** | –0.85 *** |
| L1 region IMU | ||||||
| Flexion + extension | 0.45 ** | –0.44 ** | 0.59 *** | 0.72 *** | 0.58 *** | –0.72 *** |
| Lateral flexion L + R | 0.51 *** | –0.72 *** | 0.56 *** | 0.64 *** | 0.71 *** | –0.81 *** |
| Rotation L + R | 0.38 * | –0.44 ** | 0.38 * | 0.42 ** | 0.59 *** | –0.54 *** |
| Lumbar region IMU | ||||||
| Flexion + extension | 0.66 *** | –0.59 *** | 0.66*** | 0.59 *** | 0.48 ** | –0.75 *** |
| Lateral flexion L + R | 0.52 *** | –0.78 *** | 0.62 *** | 0.58 *** | 0.67 *** | –0.81 *** |
| Rotation L + R | 0.54 *** | –0.37 * | 0.54 *** | 0.43 ** | 0.40 ** | –0.53 *** |
| IUCOASMI | –0.60 *** | 0.71 *** | –0.68 *** | –0.77 *** | –0.83 *** | 0.91 *** |
| mSASSS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Dis.Dur. | BASDAI | ASDAS | BASFI | ASAS-HI | Total | Lumbar | Cervical | |
| Cervical region IMU | |||||||||
| Flexion + extension | 0.33 * | 0.29 | –0.41 ** | –0.31 * | –0.66 *** | –0.58 *** | –0.71 *** | –0.62 *** | –0.70 *** |
| Lateral flexion L + R | –0.69 *** | –0.63 *** | –0.2 | –0.16 | –0.43 ** | –0.46 ** | –0.63 *** | –0.52 *** | –0.66 *** |
| Rotation L + R | –0.70 *** | –0.62 *** | –0.28 | –0.27 | –0.60 *** | –0.49 *** | –0.71 *** | –0.60 *** | –0.74 *** |
| L1 region IMU | |||||||||
| Flexion + extension | –0.61 *** | –0.61 *** | –0.36 * | –0.26 | –0.55 *** | –0.52 *** | –0.66 *** | –0.60 *** | –0.62 *** |
| Lateral flexion L + R | –0.56 *** | –0.47 ** | –0.25 | –0.3 | –0.46 ** | –0.43 ** | –0.67 *** | –0.66 *** | –0.57 *** |
| Rotation L + R | –0.45 ** | –0.42 ** | –0.39 * | –0.37 * | –0.45 ** | –0.44 ** | –0.47 ** | –0.49 ** | –0.37 * |
| LU region IMU | |||||||||
| Flexion+extension | –0.21 | –0.15 | –0.37 * | –0.43 ** | –0.46 ** | –0.47 ** | –0.70 *** | –0.64 *** | –0.66 *** |
| Lateral flexion L+R | –0.58 *** | –0.44 ** | –0.17 | –0.25 | –0.39 * | –0.36 * | –0.71 *** | –0.70 *** | –0.61 *** |
| Rotation L + R | –0.49 *** | –0.44 ** | –0.33 * | –0.33 * | –0.33 * | –0.26 | –0.45 ** | –0.45 ** | –0.38 * |
| IUCOASMI | 0.62 *** | 0.54 *** | 0.40 ** | 0.36 * | 0.62 *** | 0.55 *** | 0.76 *** | 0.71 *** | 0.71 *** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aranda-Valera, I.C.; Cuesta-Vargas, A.; Garrido-Castro, J.L.; Gardiner, P.V.; López-Medina, C.; Machado, P.M.; Condell, J.; Connolly, J.; Williams, J.M.; Muñoz-Esquivel, K.; et al. Measuring Spinal Mobility Using an Inertial Measurement Unit System: A Validation Study in Axial Spondyloarthritis. Diagnostics 2020, 10, 426. https://doi.org/10.3390/diagnostics10060426
Aranda-Valera IC, Cuesta-Vargas A, Garrido-Castro JL, Gardiner PV, López-Medina C, Machado PM, Condell J, Connolly J, Williams JM, Muñoz-Esquivel K, et al. Measuring Spinal Mobility Using an Inertial Measurement Unit System: A Validation Study in Axial Spondyloarthritis. Diagnostics. 2020; 10(6):426. https://doi.org/10.3390/diagnostics10060426
Chicago/Turabian StyleAranda-Valera, I. Concepción, Antonio Cuesta-Vargas, Juan L. Garrido-Castro, Philip V. Gardiner, Clementina López-Medina, Pedro M. Machado, Joan Condell, James Connolly, Jonathan M. Williams, Karla Muñoz-Esquivel, and et al. 2020. "Measuring Spinal Mobility Using an Inertial Measurement Unit System: A Validation Study in Axial Spondyloarthritis" Diagnostics 10, no. 6: 426. https://doi.org/10.3390/diagnostics10060426