Sonographic Pearls for Imaging the Brachial Plexus and Its Pathologies

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
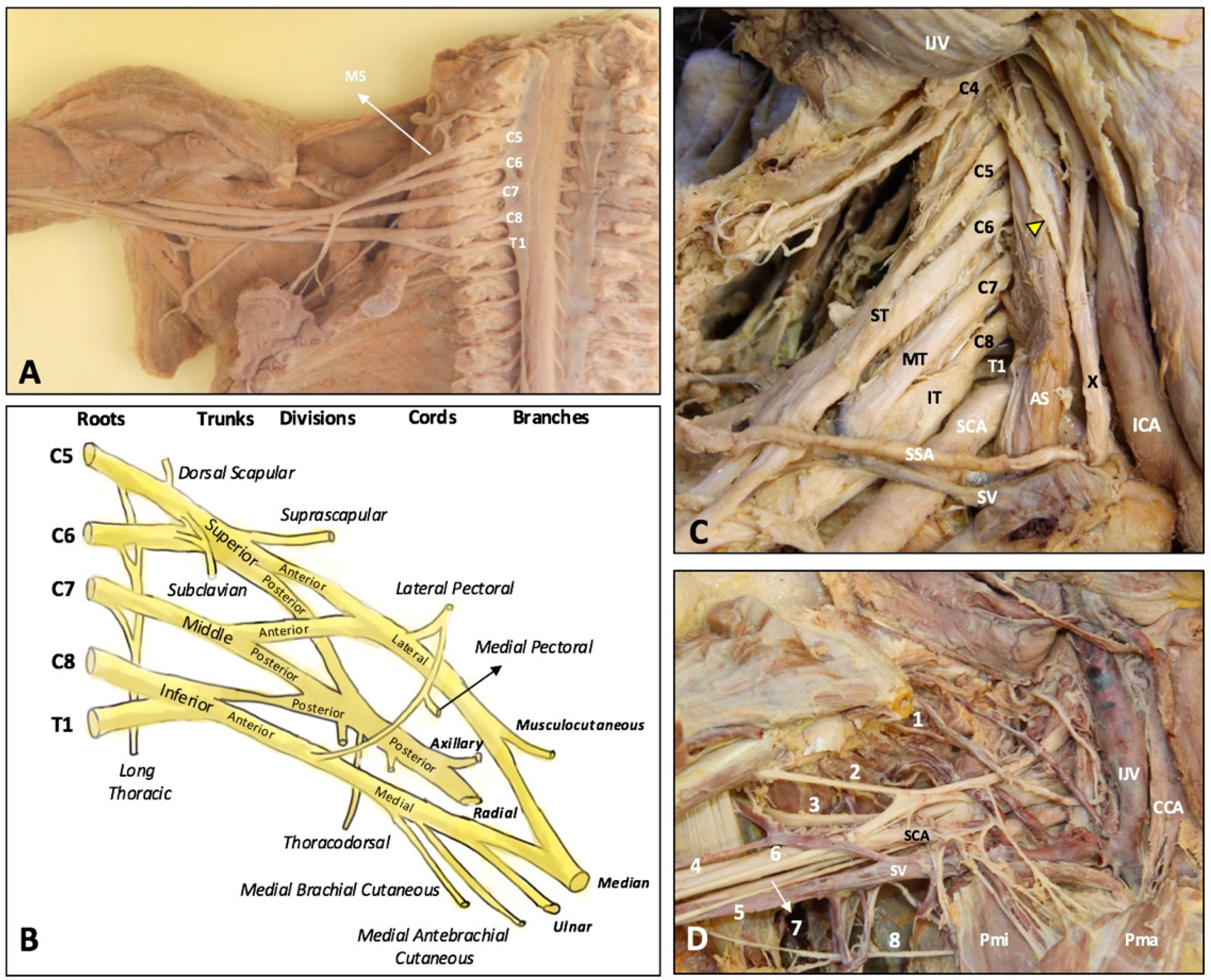
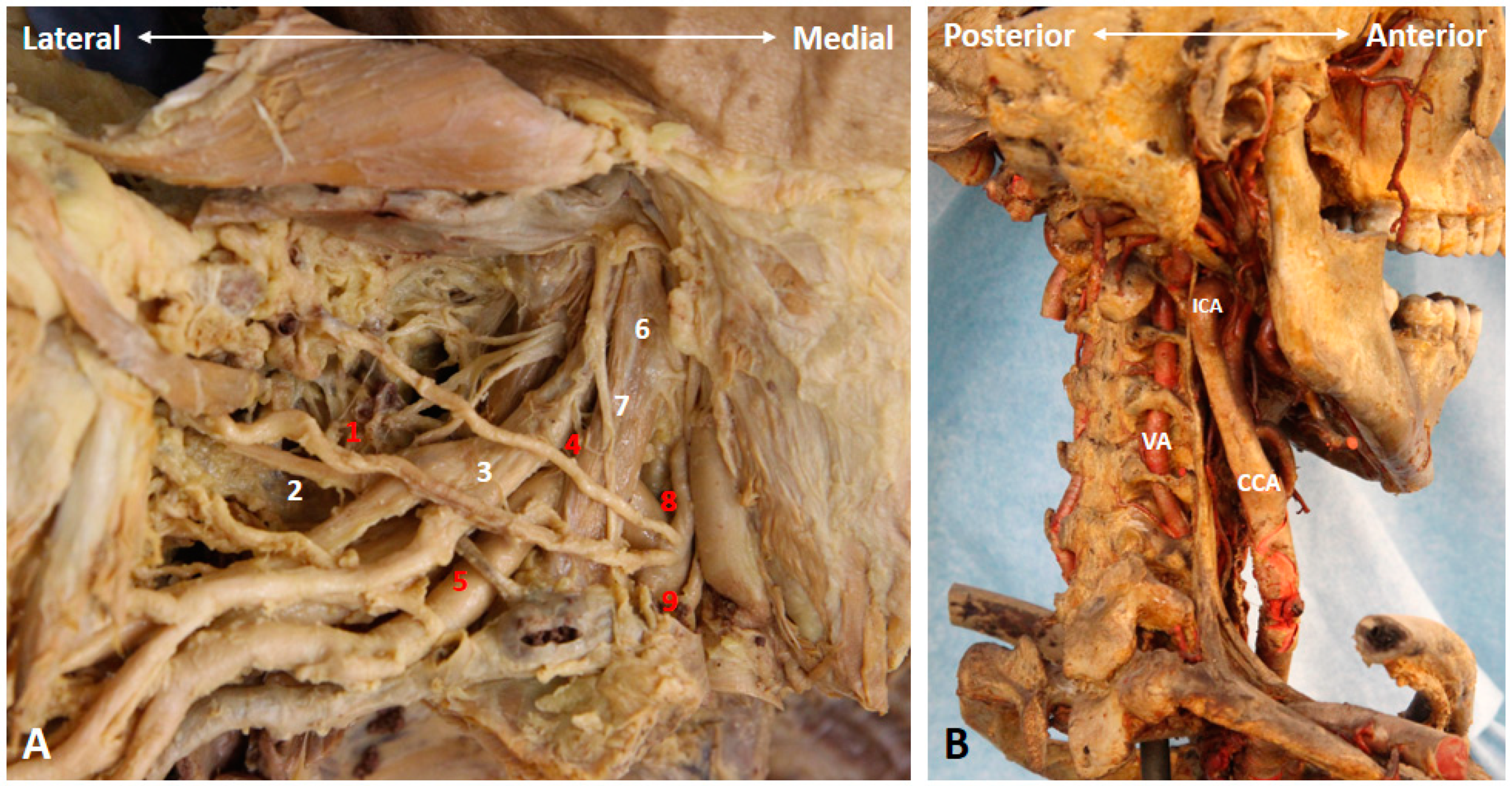
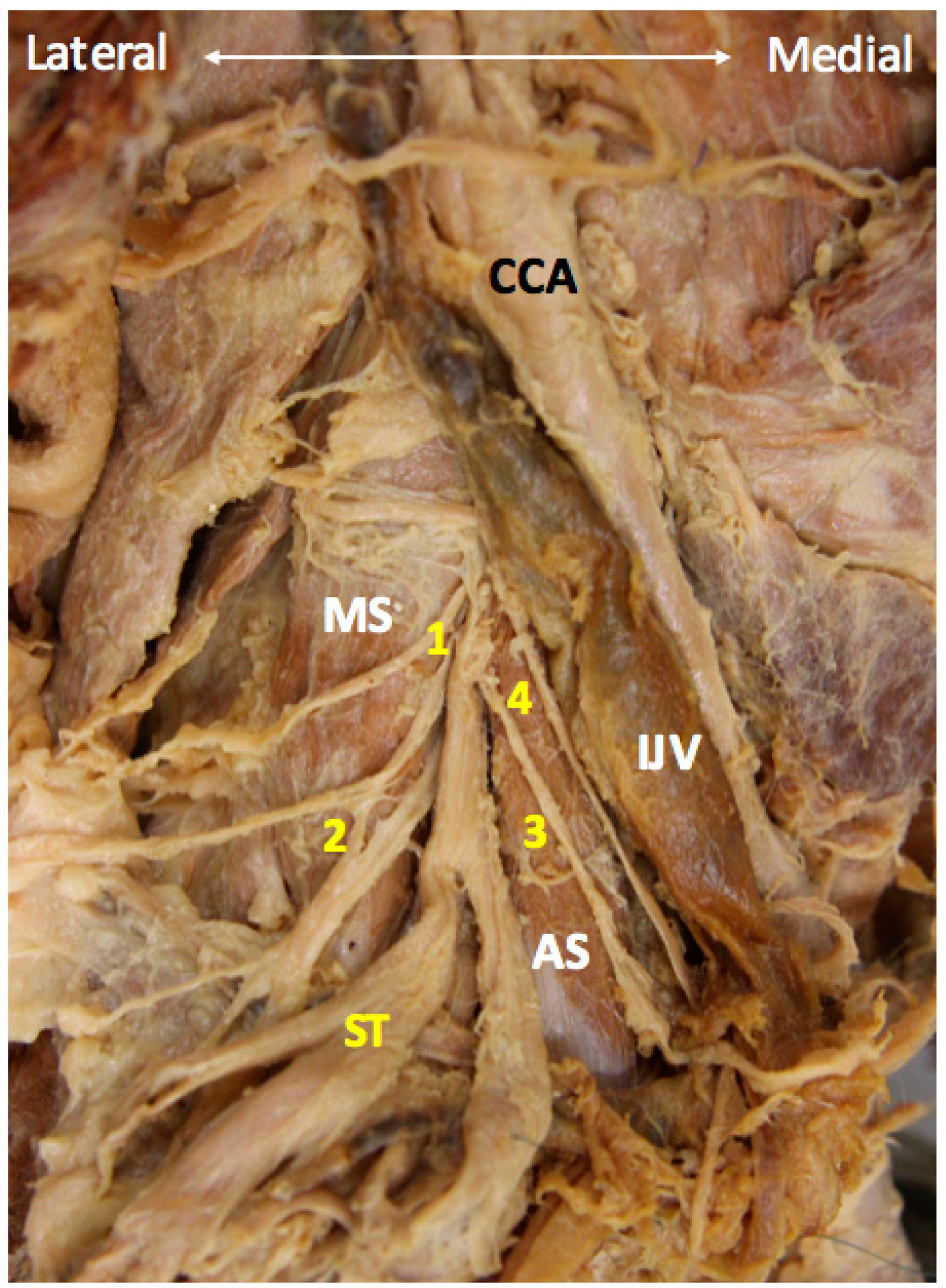
2. Anatomy
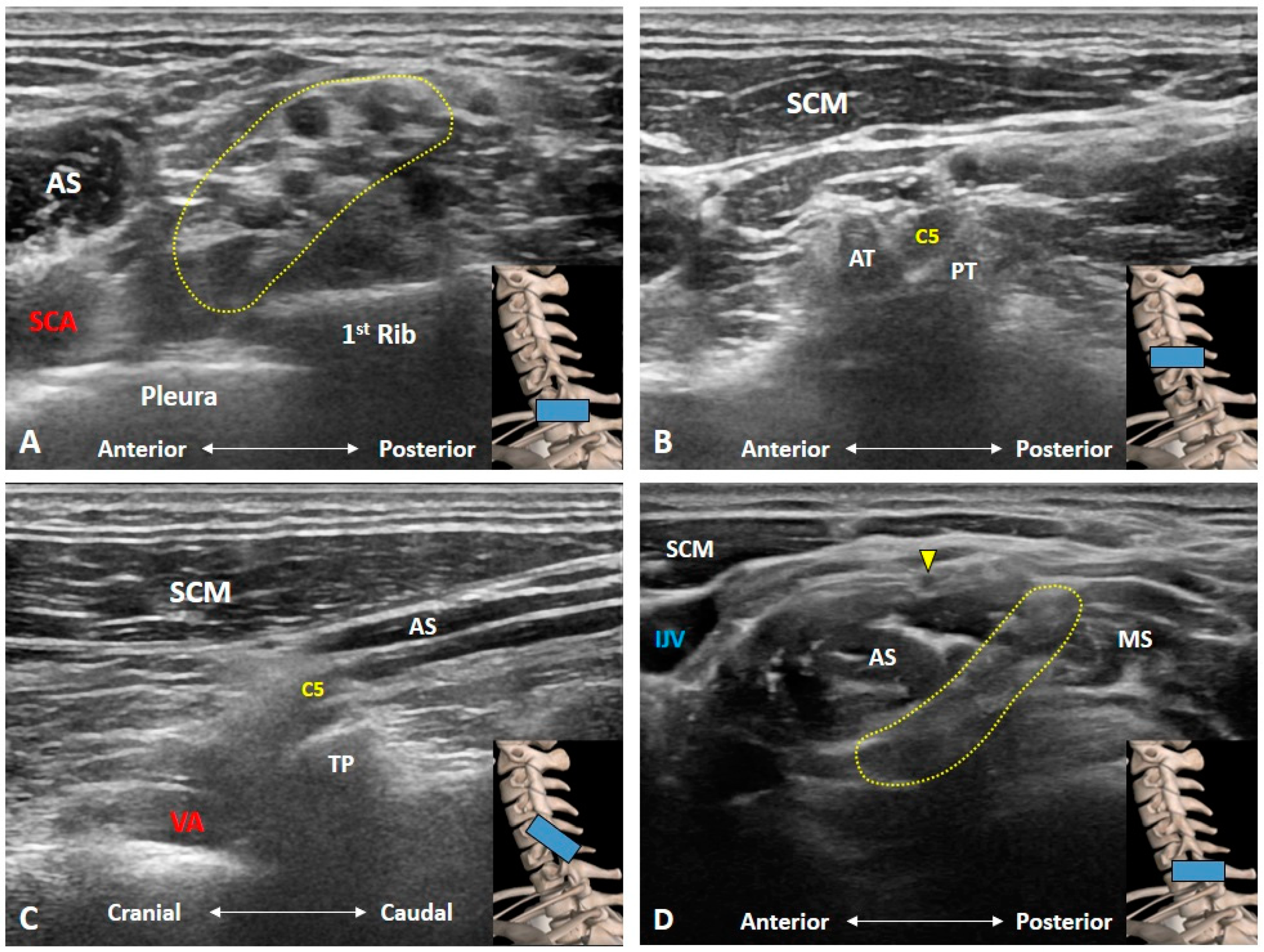
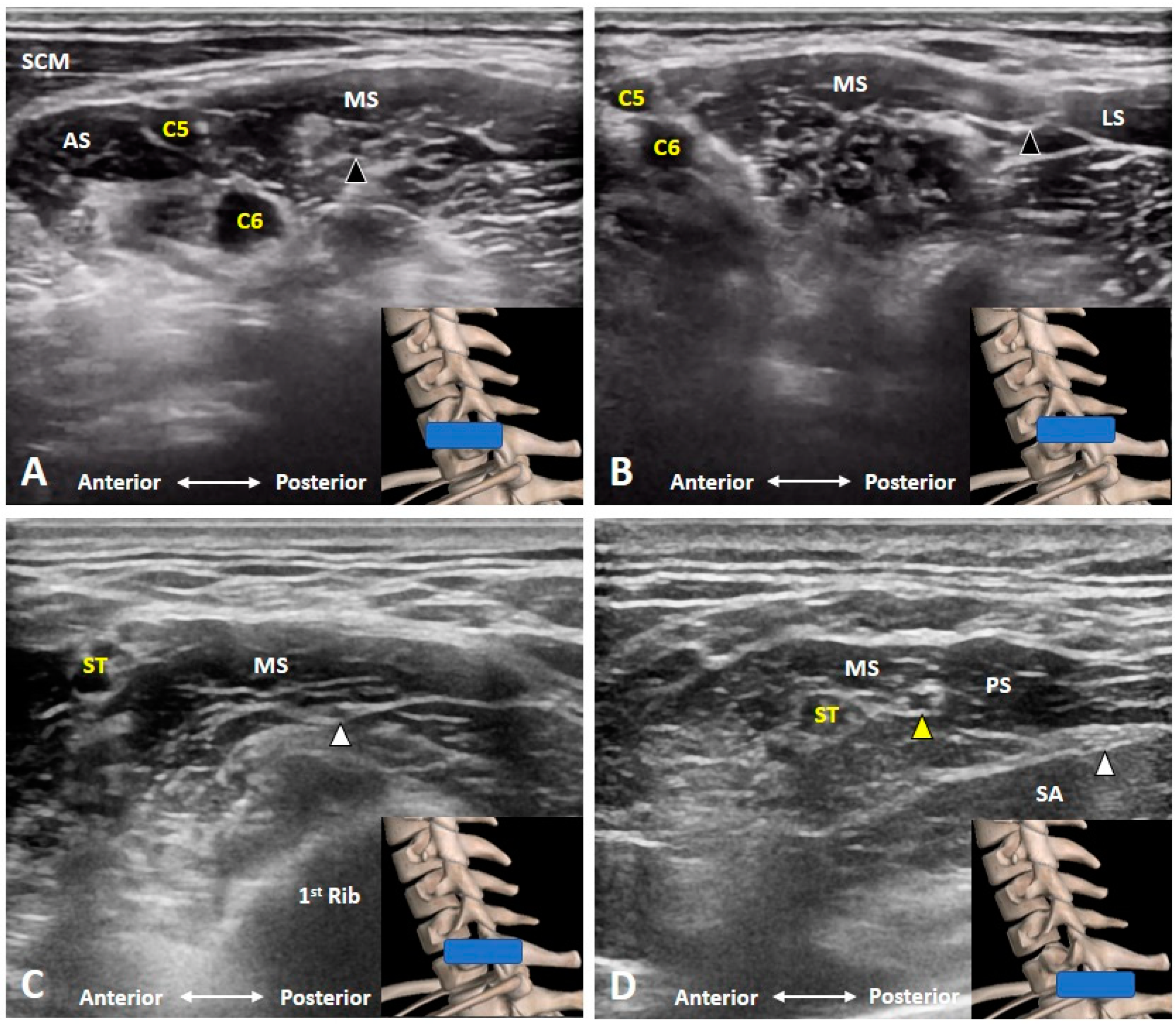
3. Imaging for Normal BP
3.1. Should We Start the Scanning Cranially?
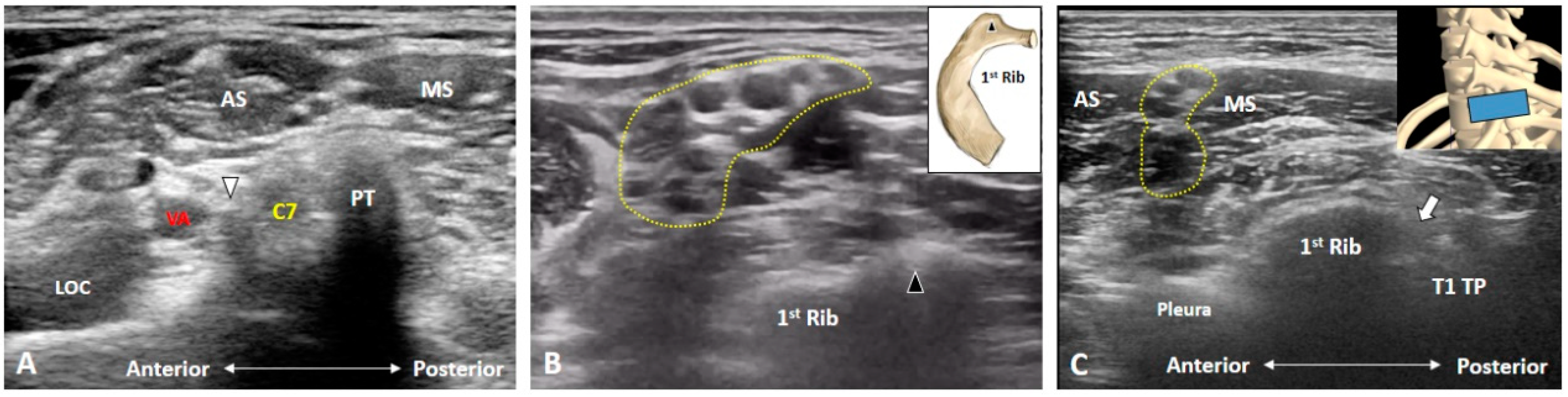
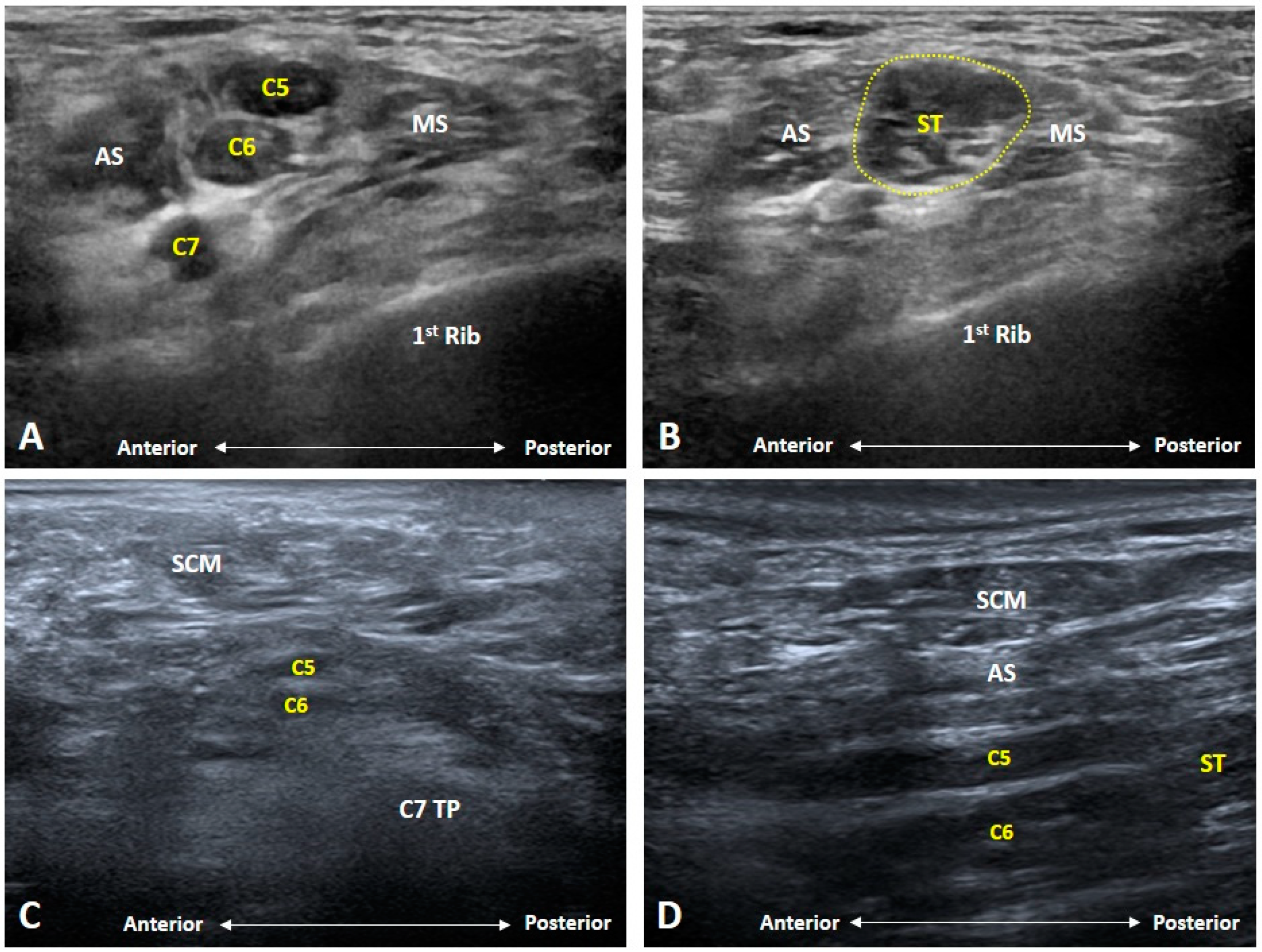
3.2. Is the C7 Transverse Process Easily Recognized?
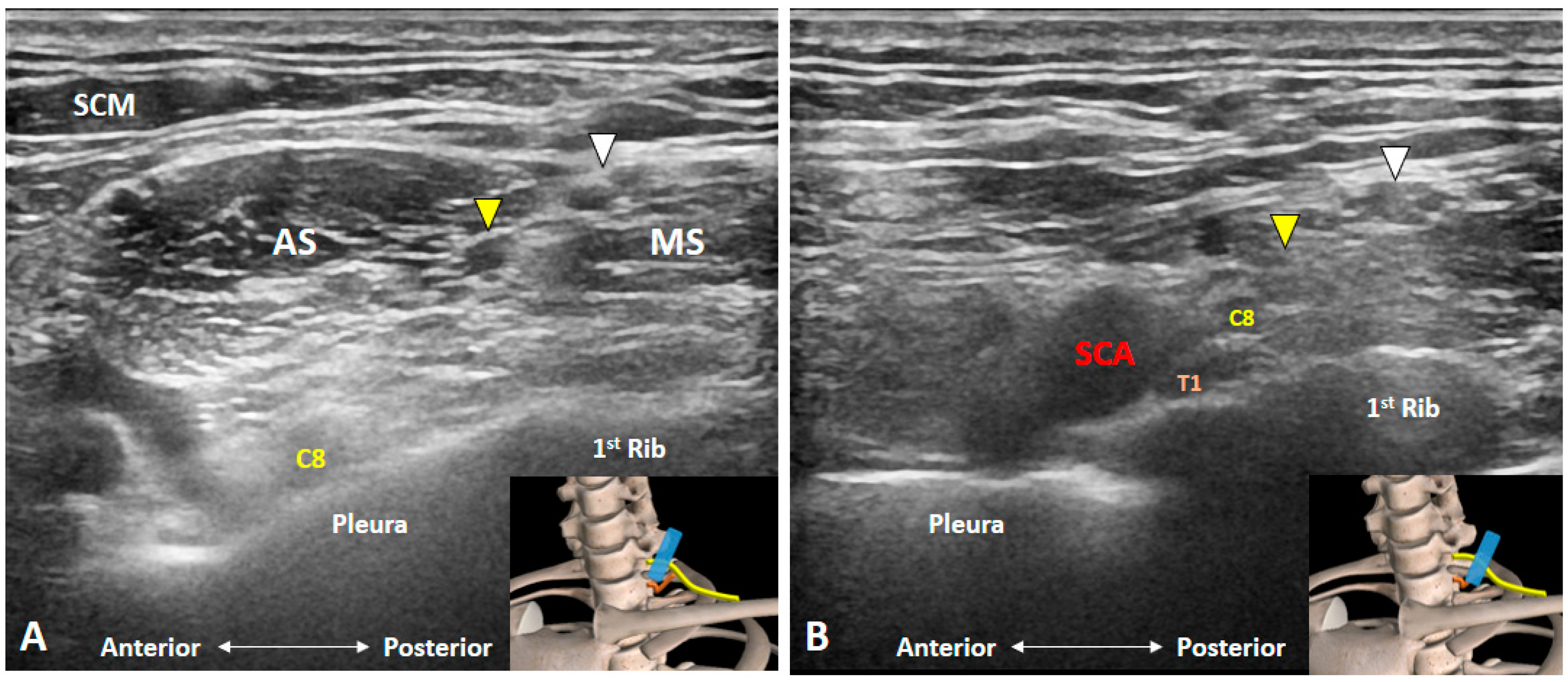
3.3. How Can We Locate the C8 and T1 Roots?
3.4. How Can We Better Visualize Cervical Anterior Rami during the Scanning Process?
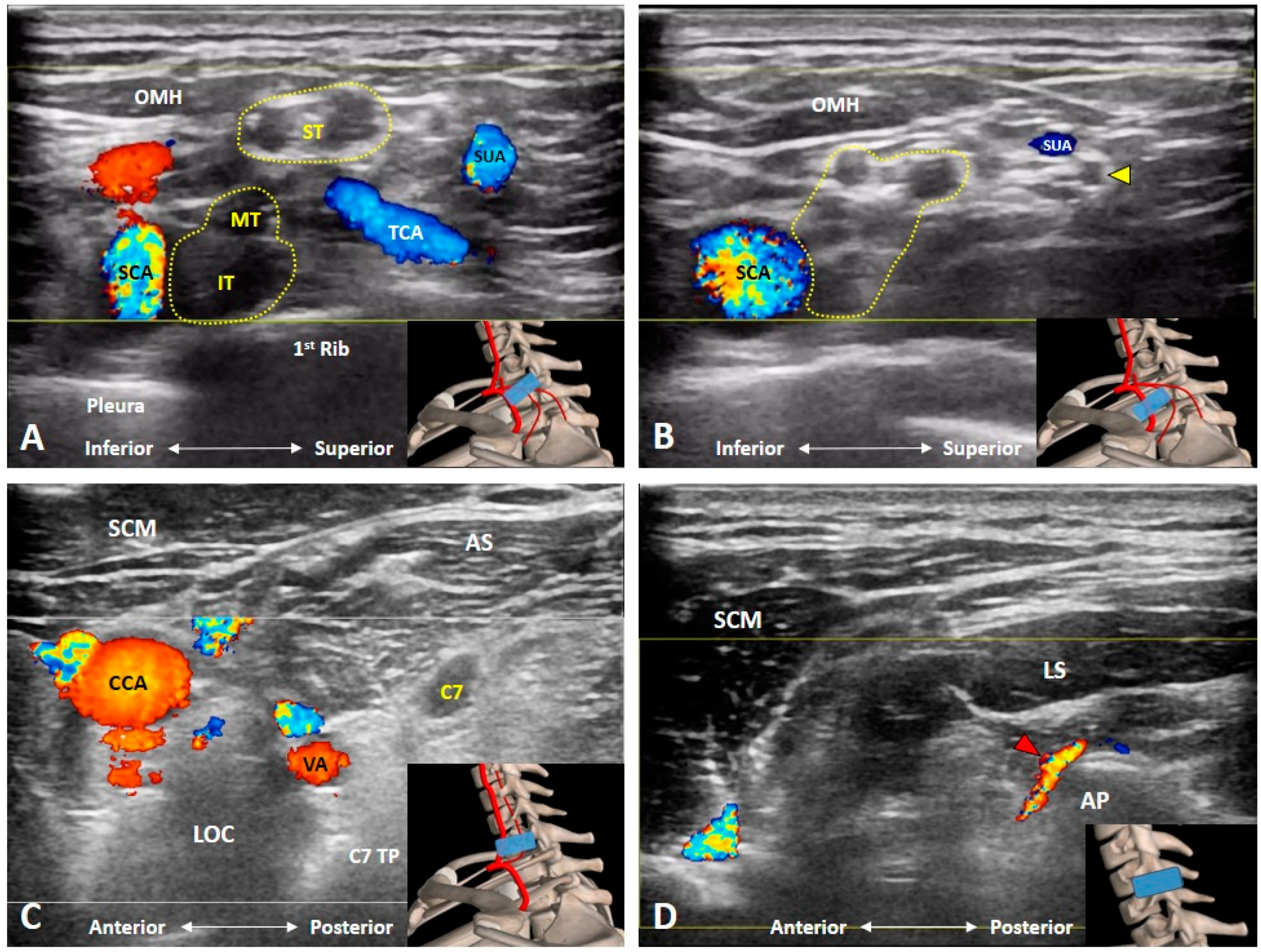
3.5. Which Vascular Structure(s) Should We Be Aware Of?
3.6. Which Branches of the BP Can Be Seen in the Cervical Region?
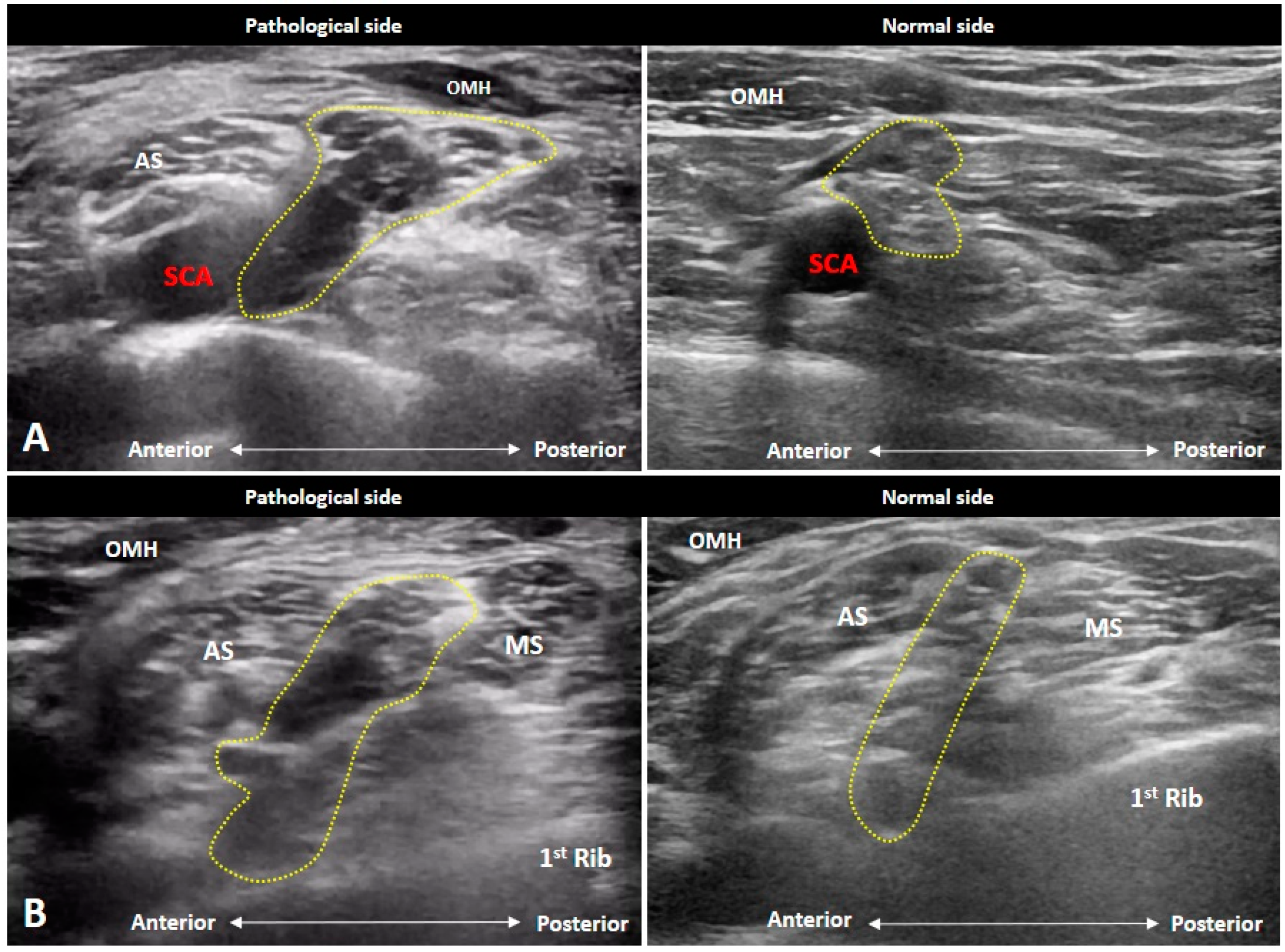
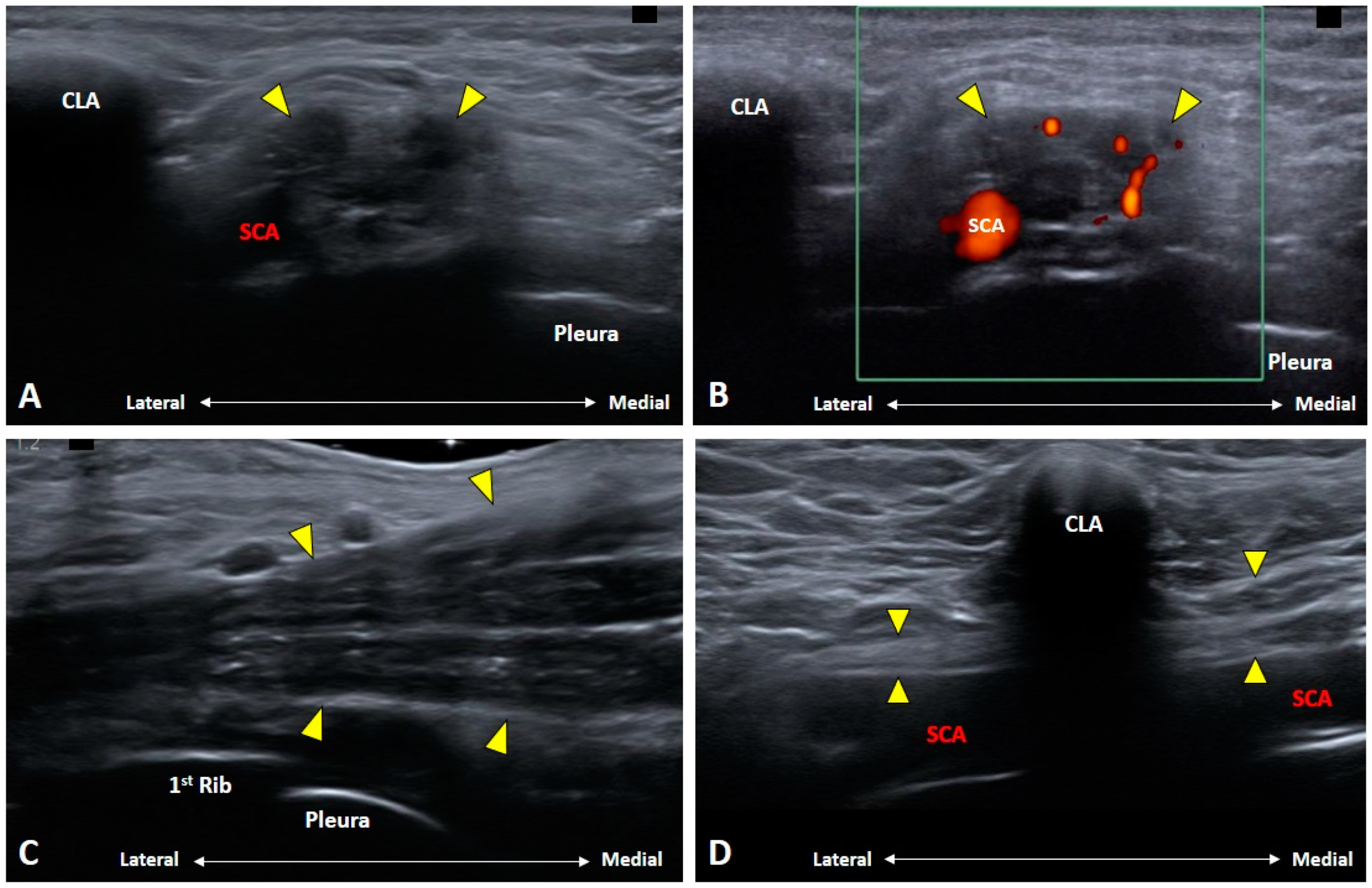
4. Imaging for BP Pathologies
4.1. Radiation-Induced Brachial Plexopathy
4.2. Neoplastic/Metastatic Brachial Plexopathy
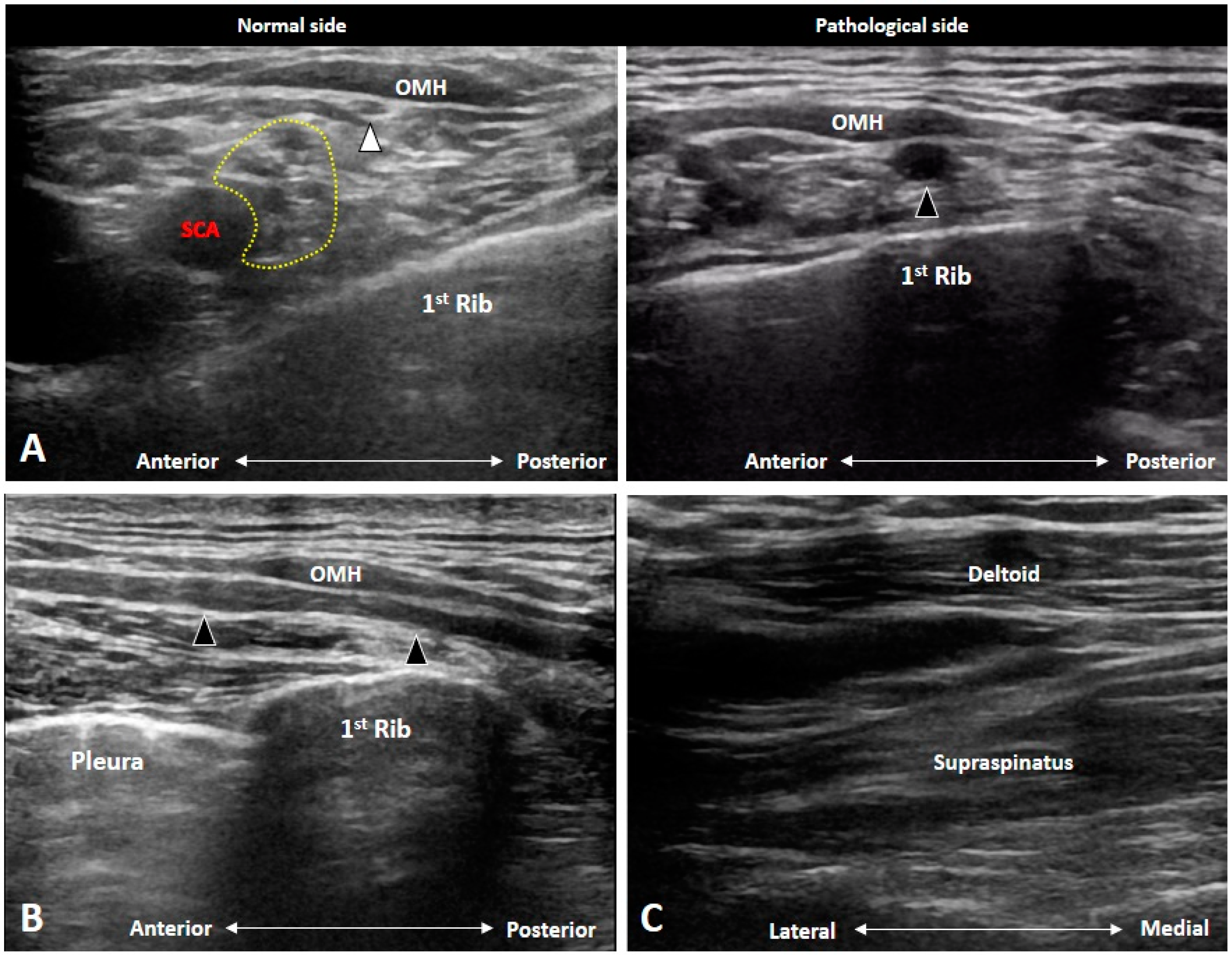
4.3. Parsonage-Turner Syndrome (Neuralgic Amyotrophy)
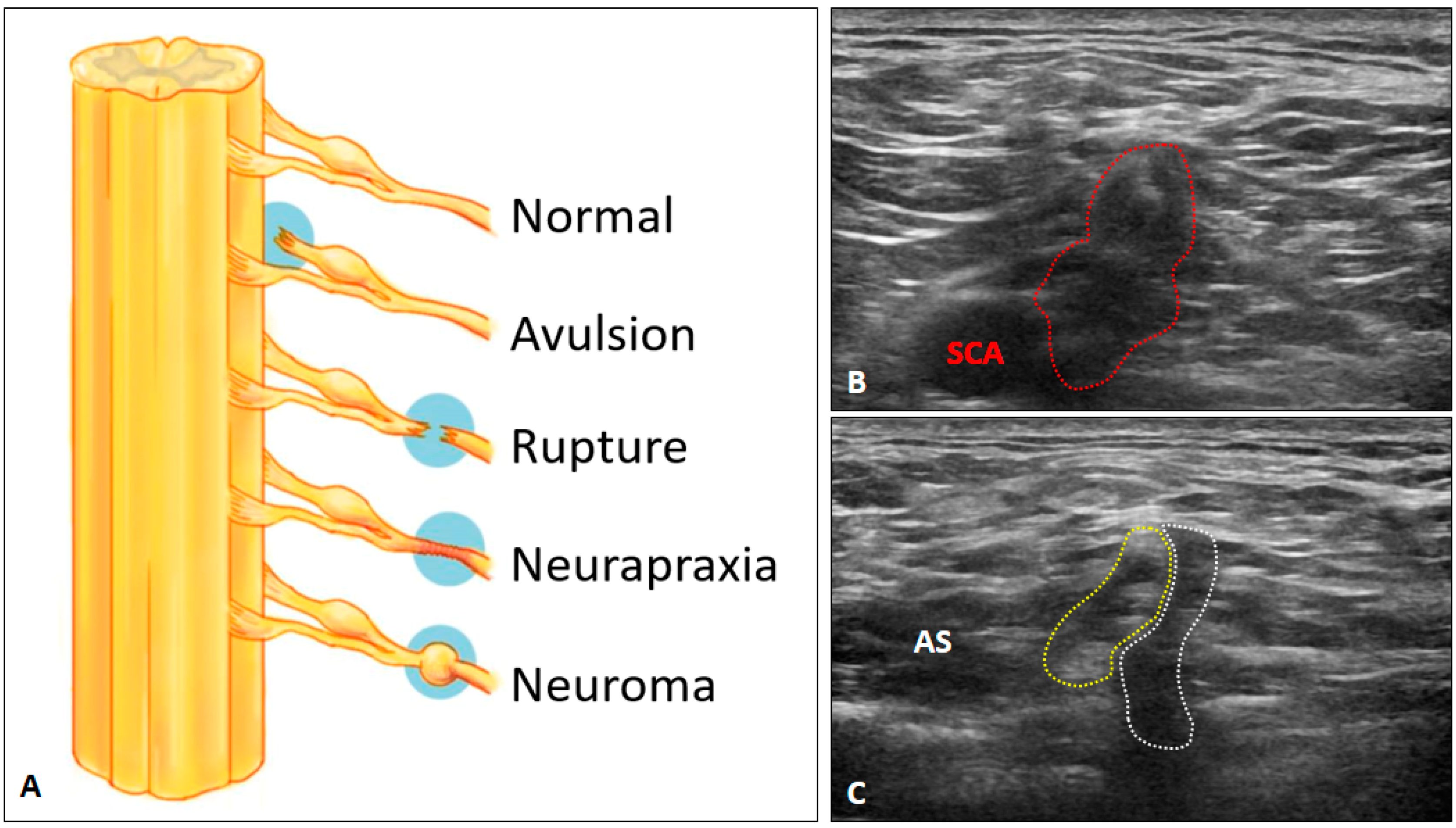
4.4. Brachial Plexus Trauma
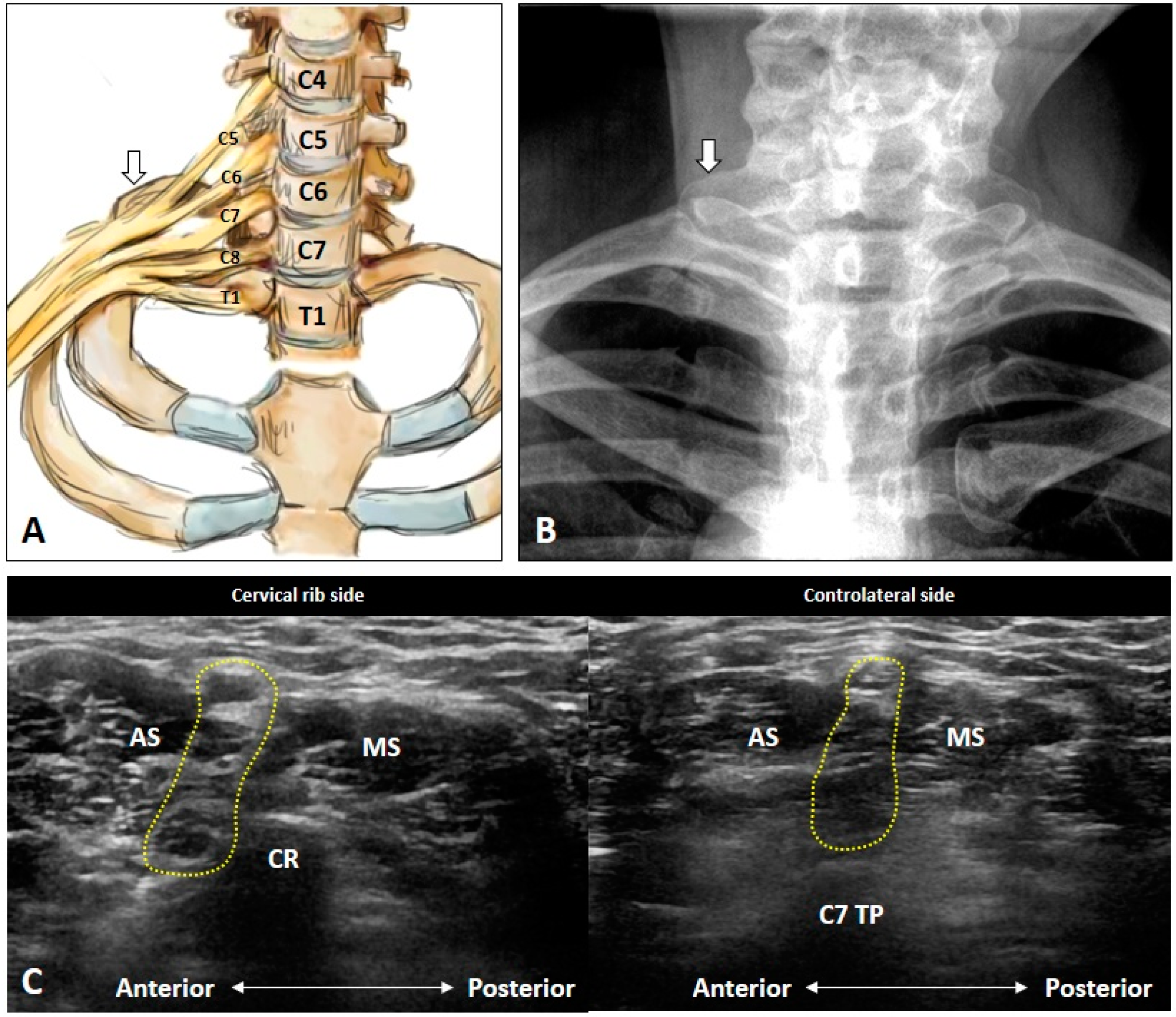
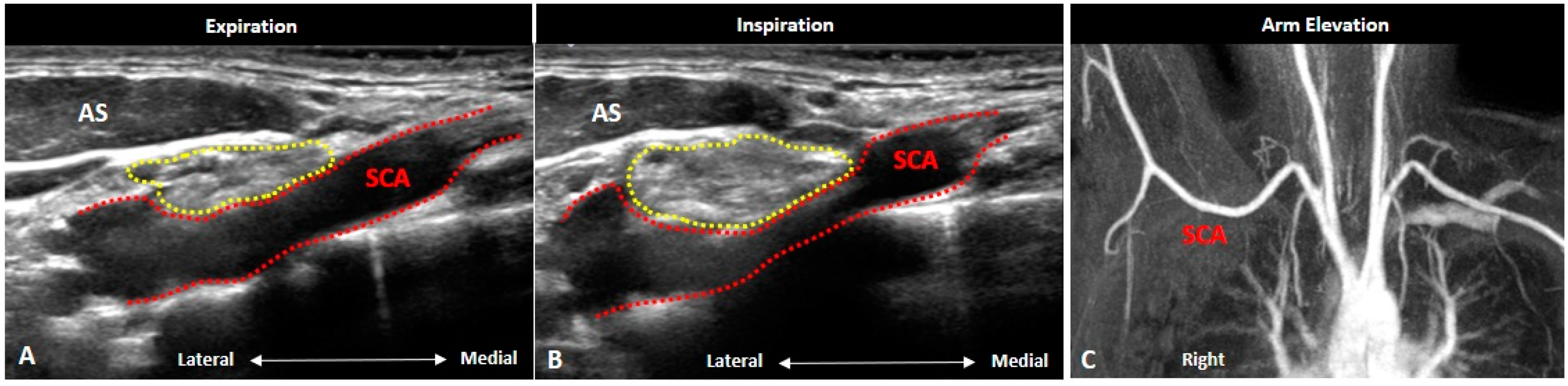
4.5. Thoracic Outlet Syndrome
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Griffith, J.F. Ultrasound of the brachial plexus. In Seminars in Musculoskeletal Radiology; Thieme Medical Publishers: New York, NY, USA, 2018; Volume 22, pp. 323–333. [Google Scholar] [CrossRef]
- Lapegue, F.; Faruch-Bilfeld, M.; Demondion, X.; Apredoaei, C.; Bayol, M.A.; Artico, H.; Chiavassa-Gandois, H.; Railhac, J.J.; Sans, N. Ultrasonography of the brachial plexus, normal appearance and practical applications. Diagn. Interv. Imaging 2014, 95, 259–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.V.; Mezian, K.; Nanka, O.; Wu, W.T.; Lou, Y.M.; Wang, J.C.; Martinoli, C.; Ozcakar, L. Ultrasound imaging for the cutaneous nerves of the extremities and relevant entrapment syndromes: From anatomy to clinical implications. J. Clin. Med. 2018, 7, 457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.T.; Chang, K.V.; Mezian, K.; Nanka, O.; Lin, C.P.; Ozcakar, L. Basis of shoulder nerve entrapment syndrome: An ultrasonographic study exploring factors influencing cross-sectional area of the suprascapular nerve. Front. Neurol. 2018, 9, 902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.V.; Kara, M.; Su, D.C.; Gurcay, E.; Kaymak, B.; Wu, W.T.; Ozcakar, L. Sonoanatomy of the spine: A comprehensive scanning protocol from cervical to sacral region. Med. Ultrason. 2019, 21, 474–482. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T.; Ozcakar, L. Ultrasound-guided interventions of the cervical spine and nerves. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 93–103. [Google Scholar] [CrossRef]
- Chang, K.V.; Lin, C.P.; Hung, C.Y.; Ozcakar, L.; Wang, T.G.; Chen, W.S. Sonographic nerve tracking in the cervical region: A pictorial essay and video demonstration. Am. J. Phys. Med. Rehabil. 2016, 95, 862–870. [Google Scholar] [CrossRef]
- Chang, K.V.; Lin, C.P.; Lin, C.S.; Wu, W.T.; Karmakar, M.K.; Ozcakar, L. Sonographic tracking of trunk nerves: Essential for ultrasound-guided pain management and research. J. Pain Res. 2017, 10, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.H.; Chang, K.V.; Ozcakar, L.; Hsiao, M.Y.; Hung, C.Y.; Shyu, S.G.; Wang, T.G.; Chen, W.S. Sonographic tracking of the upper limb peripheral nerves: A pictorial essay and video demonstration. Am. J. Phys. Med. Rehabil. 2015, 94, 740–747. [Google Scholar] [CrossRef]
- Leonhard, V.; Smith, R.; Caldwell, G.; Smith, H.F. Anatomical variations in the brachial plexus roots: Implications for diagnosis of neurogenic thoracic outlet syndrome. Ann. Anat. 2016, 206, 21–26. [Google Scholar] [CrossRef]
- Finlayson, R.J.; Etheridge, J.P.; Chalermkitpanit, P.; Tiyaprasertkul, W.; Nelems, B.; Tran, D.Q.; Huntoon, M.A. Real-time detection of periforaminal vessels in the cervical spine: An ultrasound survey. Reg. Anesth. Pain Med. 2016, 41, 130–134. [Google Scholar] [CrossRef]
- Williams, A.A.; Smith, H.F. Anatomical entrapment of the dorsal scapular and long thoracic nerves, secondary to brachial plexus piercing variation. Anat. Sci. Int. 2020, 95, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Wu, W.T.; Mezian, K.; Nanka, O.; Ozcakar, L. Sonoanatomy revisited: The long thoracic nerve. Med. Ultrason. 2019, 21, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Mezian, K.; Nanka, O.; Wu, W.T.; Lin, C.P.; Ozcakar, L. Ultrasound-guided interventions for painful shoulder: From anatomy to evidence. J. Pain Res. 2018, 11, 2311–2322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Purkayastha, A.; Sharma, N.; Sarin, A.; Bhatnagar, S.; Chakravarty, N.; Mukundan, H.; Suhag, V.; Singh, S. Radiation fibrosis syndrome: The evergreen menace of radiation therapy. Asia Pac. J. Oncol. Nurs. 2019, 6, 238–245. [Google Scholar] [CrossRef]
- Warade, A.C.; Jha, A.K.; Pattankar, S.; Desai, K. Radiation-induced brachial plexus neuropathy: A review. Neurol. India 2019, 67, S47–S52. [Google Scholar] [CrossRef]
- Chang, K.V.; Wu, W.T. Ultrasound imaging for an uncommon cause of shoulder pain: Metastatic brachial plexopathy in a woman with breast cancer. J. Med. Ultrasound 2019, 27, 160–161. [Google Scholar] [CrossRef]
- Jia, X.; Yang, J.; Chen, L.; Yu, C.; Kondo, T. Primary brachial plexus tumors: Clinical experiences of 143 cases. Clin. Neurol. Neurosurg. 2016, 148, 91–95. [Google Scholar] [CrossRef]
- Van Eijk, J.J.; Groothuis, J.T.; Van Alfen, N. Neuralgic amyotrophy: An update on diagnosis, pathophysiology, and treatment. Muscle Nerve 2016, 53, 337–350. [Google Scholar] [CrossRef]
- Gruber, L.; Loizides, A.; Loscher, W.; Glodny, B.; Gruber, H. Focused high-resolution sonography of the suprascapular nerve: A simple surrogate marker for neuralgic amyotrophy? Clin. Neurophysiol. 2017, 128, 1438–1444. [Google Scholar] [CrossRef]
- Haber, H.P.; Sinis, N.; Haerle, M.; Schaller, H.E. Sonography of brachial plexus traction injuries. Am. J. Roentgenol. 2006, 186, 1787–1791. [Google Scholar] [CrossRef]
- Wade, R.G.; Takwoingi, Y.; Wormald, J.C.R.; Ridgway, J.P.; Tanner, S.; Rankine, J.J.; Bourke, G. Magnetic resonance imaging for detecting root avulsions in traumatic adult brachial plexus injuries: Protocol for a systematic review of diagnostic accuracy. Syst. Rev. 2018, 7, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaya, Y.; Sarikcioglu, L. Sir Herbert Seddon (1903–1977) and his classification scheme for peripheral nerve injury. Childs Nerv. Syst. 2015, 31, 177–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Povlsen, S.; Povlsen, B. Diagnosing thoracic outlet syndrome: Current approaches and future directions. Diagnostics (Basel) 2018, 8, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Archie, M.; Rigberg, D. Vascular TOS—Creating a protocol and sticking to it. Diagnostics (Basel) 2017, 7, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonhard, V.; Caldwell, G.; Goh, M.; Reeder, S.; Smith, H.F. Ultrasonographic diagnosis of thoracic outlet syndrome secondary to brachial plexus piercing variation. Diagnostics (Basel) 2017, 7, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranyi, Z.; Csillik, A.; Bohm, J.; Schelle, T. Ultrasonographic identification of fibromuscular bands associated with neurogenic thoracic outlet syndrome: The “wedge-sickle” sign. Ultrasound Med. Biol. 2016, 42, 2357–2366. [Google Scholar] [CrossRef] [Green Version]















© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Chang, K.-V.; Mezian, K.; Naňka, O.; Wu, W.-T.; Yang, Y.-C.; Meng, S.; Ricci, V.; Özçakar, L. Sonographic Pearls for Imaging the Brachial Plexus and Its Pathologies. Diagnostics 2020, 10, 324. https://doi.org/10.3390/diagnostics10050324
Hsu P-C, Chang K-V, Mezian K, Naňka O, Wu W-T, Yang Y-C, Meng S, Ricci V, Özçakar L. Sonographic Pearls for Imaging the Brachial Plexus and Its Pathologies. Diagnostics. 2020; 10(5):324. https://doi.org/10.3390/diagnostics10050324
Chicago/Turabian StyleHsu, Po-Cheng, Ke-Vin Chang, Kamal Mezian, Ondřej Naňka, Wei-Ting Wu, Yi-Chiang Yang, Stefan Meng, Vincenzo Ricci, and Levent Özçakar. 2020. "Sonographic Pearls for Imaging the Brachial Plexus and Its Pathologies" Diagnostics 10, no. 5: 324. https://doi.org/10.3390/diagnostics10050324