A Rare Case of Sigmoid Colon Carcinoma in Incarcerated Inguinal Hernia

 , ,
, , {kind=link}
{kind=link}
Abstract
:1. Introduction
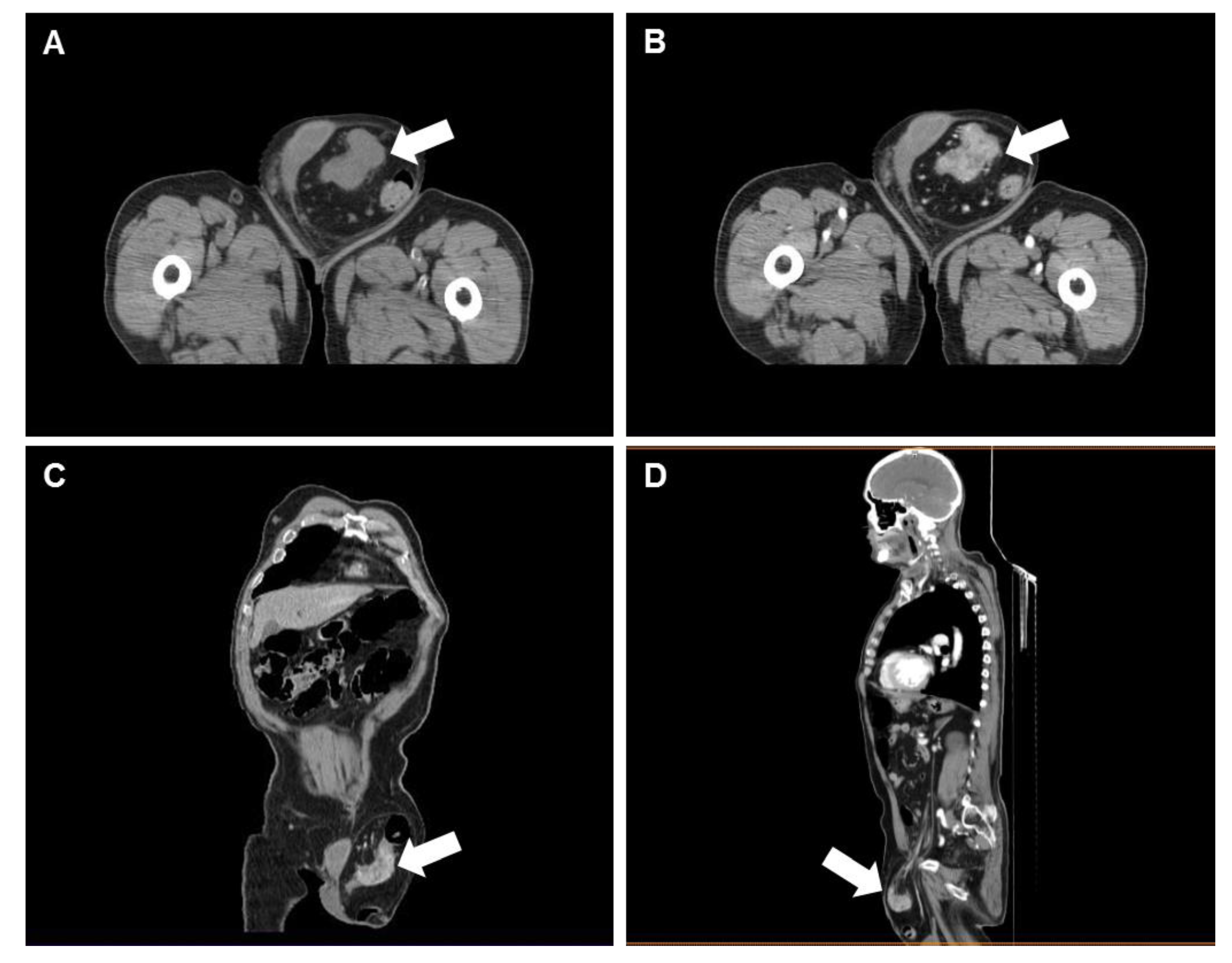
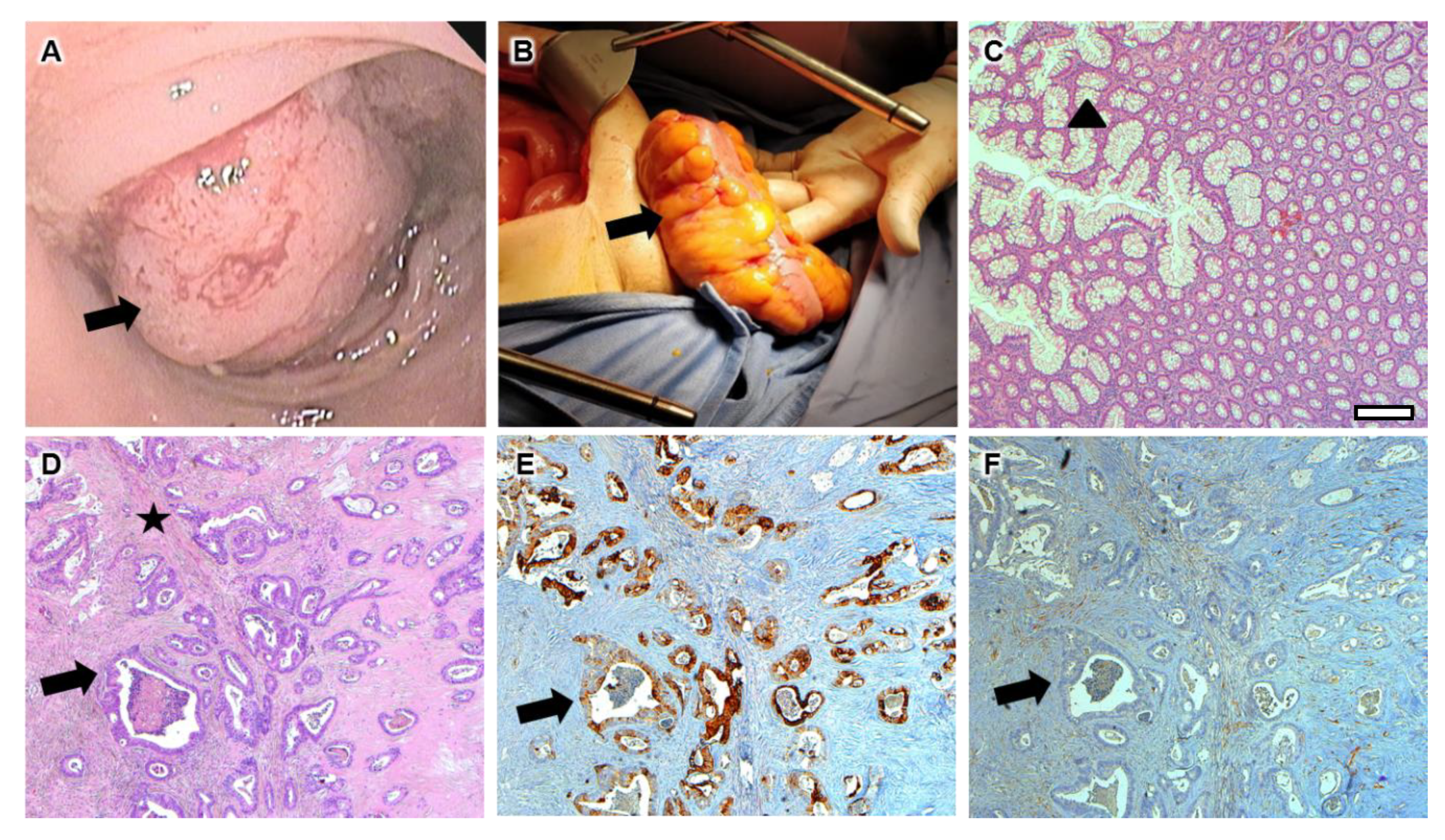
2. Case Report
3. Discussion
Funding
Conflicts of Interest
Informed Consent
References
- Jenkins, J.T.; O’dwyer, P.J. Inguinal hernias. BMJ 2008, 336, 269–272. [Google Scholar] [CrossRef] [PubMed]
- MacFadyen, B.V., Jr.; Charles, R.M. Inguinal herniorrhaphy: Complications and recurrences. In Seminars in Laparoscopic Surgery; Sage CA: Thousand Oaks, CA, USA, 1994; Volume 1. [Google Scholar]
- Chern, T.Y.; Tay, Y.K.; Perera, D.S. A rare case of ascending colon adenocarcinoma incarcerated in an inguinoscrotal hernia: Case report and literature review. Surg. Case Rep. 2018, 4, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lejars, J. Neoplasmes herniaires et periherniaires. Gaz De Hop Par 1889, 62, 801–811. [Google Scholar]
- Meniconi, R.L.; Vennarecci, G.; Lepiane, P.; Laurenzi, A.; Santoro, R.; Colasanti, M.; Ettorre, G.M. Locally advanced carcinoma of the cecum presenting as a right inguinal hernia: a case report and review of the literature. J. Med Case Rep. 2013, 7, 206. [Google Scholar] [CrossRef]
- Slater, R.; Amatya, U.; Shorthouse, A.J. Colonic carcinoma presenting as strangulated inguinal hernia: Report of two cases and review of the literature. Tech. Coloproctol. 2008, 12, 255. [Google Scholar] [CrossRef]
- Yoell, J.H. Surprises in hernial sacs—Diagnosis of tumors by microscopic examination. Calif. Med. 1959, 91, 146. [Google Scholar]
- Matsumoto, G.; Ise, H.; Inoue, H.; Ogawa, H.; Suzuki, N.; Matsuno, S. Metastatic colon carcinoma found within an inguinal hernia sac: Report of a case. Surg. Today 2000, 30, 74–77. [Google Scholar] [CrossRef]
- Korn, O.; Moyano, L.; Cabello, R.; Csendes, A. Hallazgo incidental de cáncer en saco herniario inguinal. Rev. Médica De Chile 2002, 130, 91–93. [Google Scholar] [CrossRef]
- Tan, G.Y.; Guy, R.J.; Eu, K.W. Obstructing sigmoid cancer with local invasion in an incarcerated inguinal hernia. Anz J. Surg. 2003, 73, 80–82. [Google Scholar] [CrossRef]
- Roslyn, J.J.; Stabile, B.E.; Rangenath, C. Cancer in inguinal and femoral hernias. Am. Surg. 1980, 46, 358–362. [Google Scholar]
- Pernazza, G.; Monsellato, I.; Alfano, G.; Bascone, B.; Felicioni, F.; Ferrari, R.; D’Annibale, A. Laparoscopic treatment of a carcinoma of the cecum incarcerated in a right groin hernia: Report of a case. Surg. Today 2011, 41, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Avidan, B.; Sonnenberg, A.; Bhatia, H.; Aranha, G.; Schnell, T.G.; Sontag, S.J. Inguinal hernia is not a sign of colon cancer: Results of a prospective screening trial. Aliment. Pharmacol. Ther. 2002, 16, 1197–1201. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, M.D.; Merchea, A.; Heller, S.F.; You, Y.N. Emergency management of perforated colon cancers: How aggressive should we be? J. Gastrointest. Surg. 2011, 15, 2232–2238. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, R.; Haltas, H.; Yenidunya, S. The value of CDX2 and cytokeratins 7 and 20 expression in differentiating colorectal adenocarcinomas from extraintestinal gastrointestinal adenocarcinomas: Cytokeratin 7-/20+ phenotype is more specific than CDX2 antibody. Diagn. Pathol. 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, B.P.; Skarin, A.T.; Pisick, E.; Rizk, M.; Salgia, R. Use of cytokeratins 7 and 20 in determining the origin of metastatic carcinoma of unknown primary, with special emphasis on lung cancer. Eur. J. Cancer Prev. 2001, 10, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Jessup, J.M.; Stewart, A.; Greene, F.L.; Minsky, B.D. Adjuvant chemotherapy for stage III colon cancer: Implications of race/ethnicity, age, and differentiation. J. Am. Med Assoc. 2005, 294, 2703–2711. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.; Platell, C.; McCaul, K.; Millward, M.; van Hazel, G.; Bayliss, E.; Trotter, J.; Ransom, D.; Iacopetta, B. Survival rates for stage II colon cancer patients treated with or without chemotherapy in a population-based setting. Int. J. Colorectal Dis. 2007, 22, 887–895. [Google Scholar] [CrossRef]
- Fata, F.; Mirza, A.; Craig Wood, G.; Nair, S.; Law, A.; Gallagher, J.; Ellison, N.; Bernath, A. Efficacy and toxicity of adjuvant chemotherapy in elderly patients with colon carcinoma: A 10-year experience of the Geisinger Medical Center. Cancer 2002, 94, 1931–1938. [Google Scholar] [CrossRef]
- Kouraklis, G.; Kouskos, E.; Glinavou, A.; Raftopoulos, J.; Karatzas, G. Perforated carcinoma of the sigmoid colon in an incarcerated inguinal hernia: Report of a case. Surg. Today 2003, 33, 707–708. [Google Scholar] [CrossRef]
- Boormans, J.L.; Hesp, W.L.; Teune, T.M.; Plaisier, P.W. Carcinoma of the sigmoid presenting as a right inguinal hernia. Hernia 2006, 10, 93–96. [Google Scholar] [CrossRef]
- Ruiz-Tovar, J.; Ripalda, E.; Beni, R.; Nistal, J.; Monroy, C.; Carda, P. Carcinoma of the sigmoid colon in an incarcerated inguinal hernia. Can. J. Surg. 2009, 52, E31–E32. [Google Scholar] [PubMed]
- Ko, K.H.; Yu, C.Y.; Kao, C.C.; Tsai, S.H.; Huang, G.S.; Chang, W.C. Perforated sigmoid colon cancer within an irreducible inguinal hernia: A case report. Korean J. Radiol. 2010, 11, 231–233. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldi, D.; Alfano, V.; Punzo, B.; Tramontano, L.; Baselice, S.; Spidalieri, G.; Micera, O.; Cavaliere, C. A Rare Case of Sigmoid Colon Carcinoma in Incarcerated Inguinal Hernia. Diagnostics 2020, 10, 99. https://doi.org/10.3390/diagnostics10020099
Baldi D, Alfano V, Punzo B, Tramontano L, Baselice S, Spidalieri G, Micera O, Cavaliere C. A Rare Case of Sigmoid Colon Carcinoma in Incarcerated Inguinal Hernia. Diagnostics. 2020; 10(2):99. https://doi.org/10.3390/diagnostics10020099
Chicago/Turabian StyleBaldi, Dario, Vincenzo Alfano, Bruna Punzo, Liberatore Tramontano, Simona Baselice, Gianluca Spidalieri, Osvaldo Micera, and Carlo Cavaliere. 2020. "A Rare Case of Sigmoid Colon Carcinoma in Incarcerated Inguinal Hernia" Diagnostics 10, no. 2: 99. https://doi.org/10.3390/diagnostics10020099