Similarities and Differences between Clear Cell Tubulo-Papillary and Conventional Clear Cell Renal Cell Carcinoma: A Comparative Phenotypical and Mutational Analysis




{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Immunohistochemistry
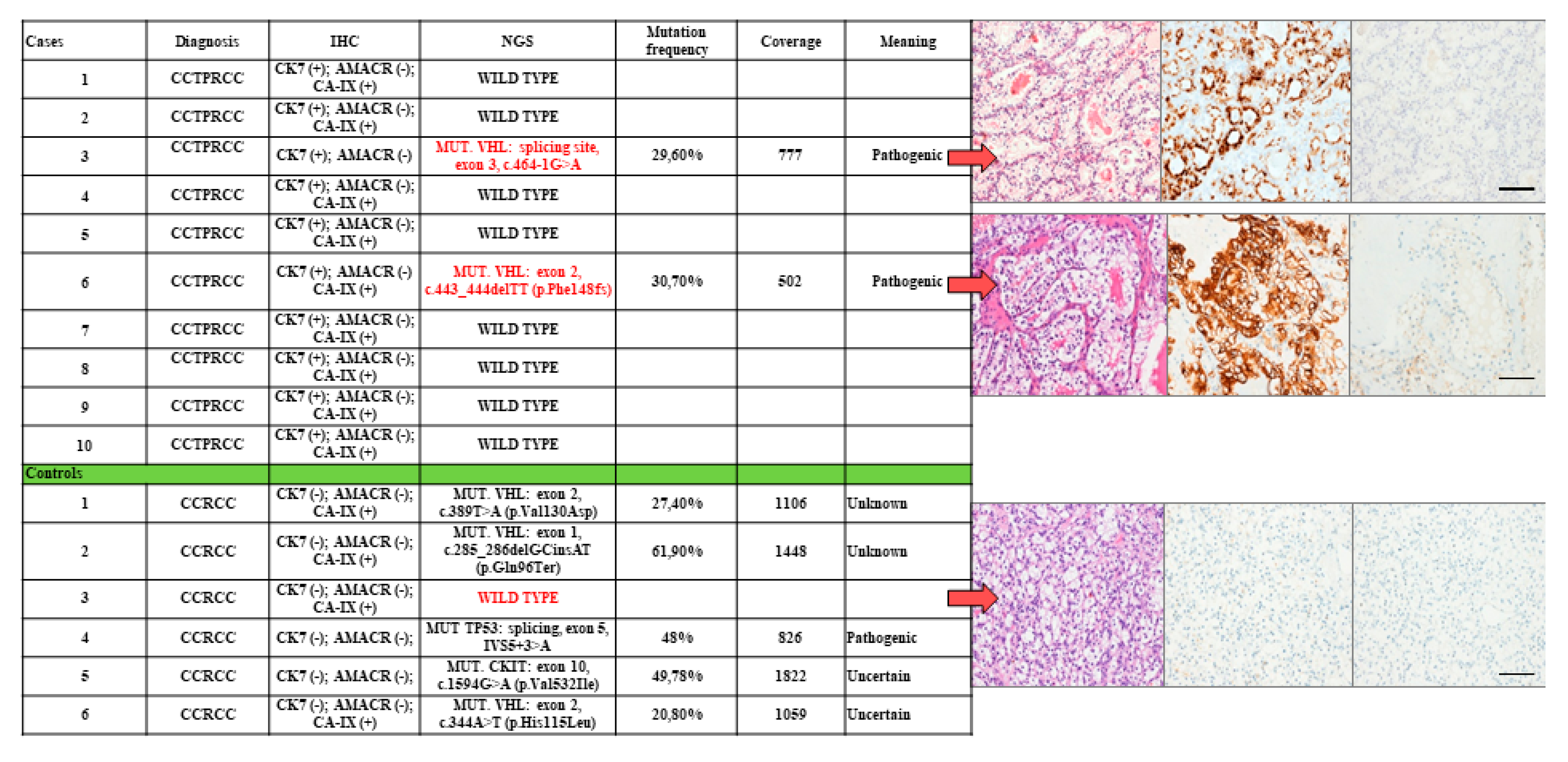
2.2. NGS Analysis
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V.E. WHO Classification of Tumours of the Urinary System and Male Genital Organs; International Agency for Research on Cancer (IARC): Lyon, France, 2016; pp. 11–43. [Google Scholar]
- Kuroda, N.; Ohe, C.; Kawakami, F.; Mikami, S.; Furuya, M.; Matsuura, K.; Moriyama, M.; Nagashima, Y.; Zhou, M.; Petersson, F.; et al. Clear cell papillary renal cell carcinoma: A review. Int. J. Clin. Exp. Pathol. 2014, 7, 7312–7318. [Google Scholar] [PubMed]
- Tickoo, S.K.; dePeralta-Venturina, M.N.; Harik, L.R.; Worcester, H.D.; Salama, M.E.; Young, A.N.; Moch, H.; Amin, M.B. Spectrum of epithelial neoplasms in endstage renal disease: An experience from 66 tumor-bearing kidneys with emphasis on histologic patterns distinct from those in sporadic adult renal neoplasia. Am. J. Surg. Pathol. 2006, 30, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Williamson, S.R.; Zhang, S.; Eble, J.N.; Grignon, D.J.; Martignoni, G.; Brunelli, M.; Wang, M.; Gobbo, S.; Baldridge, L.A.; Cheng, L. Clear cell papillary renal cell carcinoma-like tumors in patients with von Hippel-Lindau disease are unrelated to sporadic clear cell papillary renal cell carcinoma. Am. J. Surg. Pathol. 2013, 37, 1131–1139. [Google Scholar] [CrossRef]
- Alexiev, B.A.; Drachenberg, C.B. Clear cell papillary renal cell carcinoma: Incidence, morphological features, immunohistochemical profile, and biologic behavior: A single institution study. Pathol. Res. Pr. 2014, 210, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Gobbo, S.; Eble, J.N.; Grignon, D.J.; Martignoni, G.; MacLennan, G.T.; Shah, R.B.; Zhang, S.; Brunelli, M.; Cheng, L. Clear cell papillary renal cell carcinoma: A distinct histopathologic and molecular genetic entity. Am. J. Surg. Pathol. 2008, 32, 1239–1245. [Google Scholar] [CrossRef]
- Diolombi, M.L.; Cheng, L.; Argani, P.; Epstein, J.I. Do clear cell papillary renal cell carcinomas have malignant potential? Am. J. Surg. Pathol. 2015, 39, 1621–1634. [Google Scholar] [CrossRef]
- Chen, W.J.; Pan, C.C.; Shen, S.H.; Chung, H.J.; Lin, C.C.; Lin, A.T.; Chang, Y.H. Clear cell papillary renal cell carcinoma—An indolent subtype of renal tumor. J. Chin. Med. Assoc. 2018, 81, 878–883. [Google Scholar] [CrossRef]
- Aydin, H.; Chen, L.; Cheng, L.; Vaziri, S.; He, H.; Ganapathi, R.; Delahunt, B.; Magi-Galluzzi, C.; Zhou, M. Clear cell tubulopapillary renal cell carcinoma: A study of 36 distinctive low-grade epithelialtumors of the kidney. Am. J. Surg. Pathol. 2010, 34, 1608–1621. [Google Scholar] [CrossRef]
- Adam, J.; Couturier, J.; Molinie, V.; Vieillefond, A.; Sibony, M. Clear-cell papillary renal cell carcinoma: 24 cases of a distinct low-grade renal tumour and a comparative genomic hybridization array study of seven cases. Histopathology 2011, 58, 1064–1071. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Zheng, S.; Truong, L.D.; Ro, J.Y.; Ayala, A.G.; Shen, S.S. Clear cell papillary renal cell carcinoma is the fourth most common histologic type of renal cell carcinoma in 290 consecutive nephrectomies for renal cell carcinoma. Hum. Pathol. 2014, 45, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Lawrie, C.H.; Larrea, E.; Larrinaga, G.; Goicoechea, I.; Arestin, M.; Fernandez-Mercado, M.; Hes, O.; Cáceres, F.; Manterola, L.; López, J.I. Targeted next-generation sequencing and non-coding RNA expression analysis of clear cell papillary renal cell carcinoma suggests distinct pathological mechanisms from other renal tumour subtypes. J. Pathol. 2014, 232, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Leroy, X.; Camparo, P.; Gnemmi, V.; Aubert, S.; Flamand, V.; Roupret, M.; Fantoni, J.C.; Comperat, E. Clear cell papillary renal cell carcinoma is an indolent and low-grade neoplasm with overexpression of cyclin-D1. Histopathology 2014, 64, 1032–1036. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.S.; Shen, Q.; Xia, Q.Y.; Tu, P.; Shi, Q.L.; Zhou, X.J.; Rao, Q. Clear cell papillary renal cell carcinoma: A clinicopathological study emphasizing ultrastructural features and cytogenetic heterogeneity. Int. J. Clin. Exp. Pathol. 2013, 6, 2936–2942. [Google Scholar] [PubMed]
- Kuroda, N.; Shiotsu, T.; Kawada, C.; Shuin, T.; Hes, O.; Michal, M.; Ohe, C.; Mikami, S.; Pan, C.C. Clear cell papillary renal cell carcinoma and clear cell renal cell carcinoma arising in acquired cystic disease of the kidney: An immunohistochemical and genetic study. Ann. Diagn. Pathol. 2011, 15, 282–285. [Google Scholar] [CrossRef]
- Bing, Z.; Tomaszewski, J.E. Clear cell papillary renal cell carcinoma in the bilateral native kidneys after 2 years of renal transplantation: Report of a case and review of the literature. Case Rep. Transplant. 2011, 2011, 387645. [Google Scholar] [CrossRef]
- Rohan, S.M.; Xiao, Y.; Liang, Y.; Dudas, M.E.; Al-Ahmadie, H.A.; Fine, S.W.; Gopalan, A.; Reuter, V.E.; Rosenblum, M.K.; Russo, P.; et al. Clear cell papillary renal cell carcinoma: Molecular and immunohistochemical analysis with emphasis on the von Hippel Lindau gene and hypoxia inducible factor pathway related proteins. Mod. Pathol. 2011, 24, 1207–1220. [Google Scholar] [CrossRef] [Green Version]
- Favazza, L.; Chitale, D.A.; Barod, R.; Rogers, C.G.; Kalyana-Sundaram, S.; Palanisamy, N.; Gupta, N.S.; Williamson, S.R. Renal cell tumors with clear cell histology and intact VHL and chromosome 3p: A histological review of tumors from the Cancer Genome Atlas database. Mod. Pathol. 2017, 30, 1603–1612. [Google Scholar] [CrossRef]
- Fiorentino, M.; Gruppioni, E.; Massari, F.; Giunchi, F.; Altimari, A.; Ciccarese, C.; Bimbatti, D.; Scarpa, A.; Iacovelli, R.; Porta, C.; et al. Wide spetcrum mutational analysis of metastatic renal cell cancer: A retrospective next generation sequencing approach. Oncotarget 2017, 8, 7328–7335. [Google Scholar] [CrossRef] [Green Version]
- Batavia, A.A.; Schraml, P.; Moch, H. Clear cell renal cell carcinoma with wild-type von Hippel-Lindau gene: A non-existent or new tumour entity? Histopathology 2019, 74, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Skinnider, B.F.; Folpe, A.L.; Hennigar, R.A.; Lim, S.D.; Cohen, C.; Tamboli, P.; Young, A.; de Peralta-Venturina, M.; Amin, M.B. Distribution of cytokeratins and vimentin in adult renal neoplasms and normal renal tissue: Potential utility of a cytokeratin antibody panel in the differential diagnosis of renal tumors. Am. J. Surg. Pathol. 2005, 29, 747–754. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giunchi, F.; Franceschini, T.; Gruppioni, E.; Altimari, A.; Capizzi, E.; Massari, F.; Schiavina, R.; Brunelli, M.; Martignoni, G.; Fiorentino, M. Similarities and Differences between Clear Cell Tubulo-Papillary and Conventional Clear Cell Renal Cell Carcinoma: A Comparative Phenotypical and Mutational Analysis. Diagnostics 2020, 10, 123. https://doi.org/10.3390/diagnostics10020123
Giunchi F, Franceschini T, Gruppioni E, Altimari A, Capizzi E, Massari F, Schiavina R, Brunelli M, Martignoni G, Fiorentino M. Similarities and Differences between Clear Cell Tubulo-Papillary and Conventional Clear Cell Renal Cell Carcinoma: A Comparative Phenotypical and Mutational Analysis. Diagnostics. 2020; 10(2):123. https://doi.org/10.3390/diagnostics10020123
Chicago/Turabian StyleGiunchi, Francesca, Tania Franceschini, Elisa Gruppioni, Annalisa Altimari, Elisa Capizzi, Francesco Massari, Riccardo Schiavina, Matteo Brunelli, Guido Martignoni, and Michelangelo Fiorentino. 2020. "Similarities and Differences between Clear Cell Tubulo-Papillary and Conventional Clear Cell Renal Cell Carcinoma: A Comparative Phenotypical and Mutational Analysis" Diagnostics 10, no. 2: 123. https://doi.org/10.3390/diagnostics10020123