Prognostic Value of Circulating IGFBP2 and Related Autoantibodies in Children with Metastatic Rhabdomyosarcomas

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Blood Specimens
2.2. Quantitative RT-PCR
2.3. Direct ELISA Assay for Plasmatic IGFBP2 Assessment
2.4. Indirect ELISA Assay for Plasmatic Anti-IGFBP2 Autoantibodies Detection
2.5. Total IgG Measurement
2.6. Statistical Analysis
3. Results
3.1. Patients Characteristics
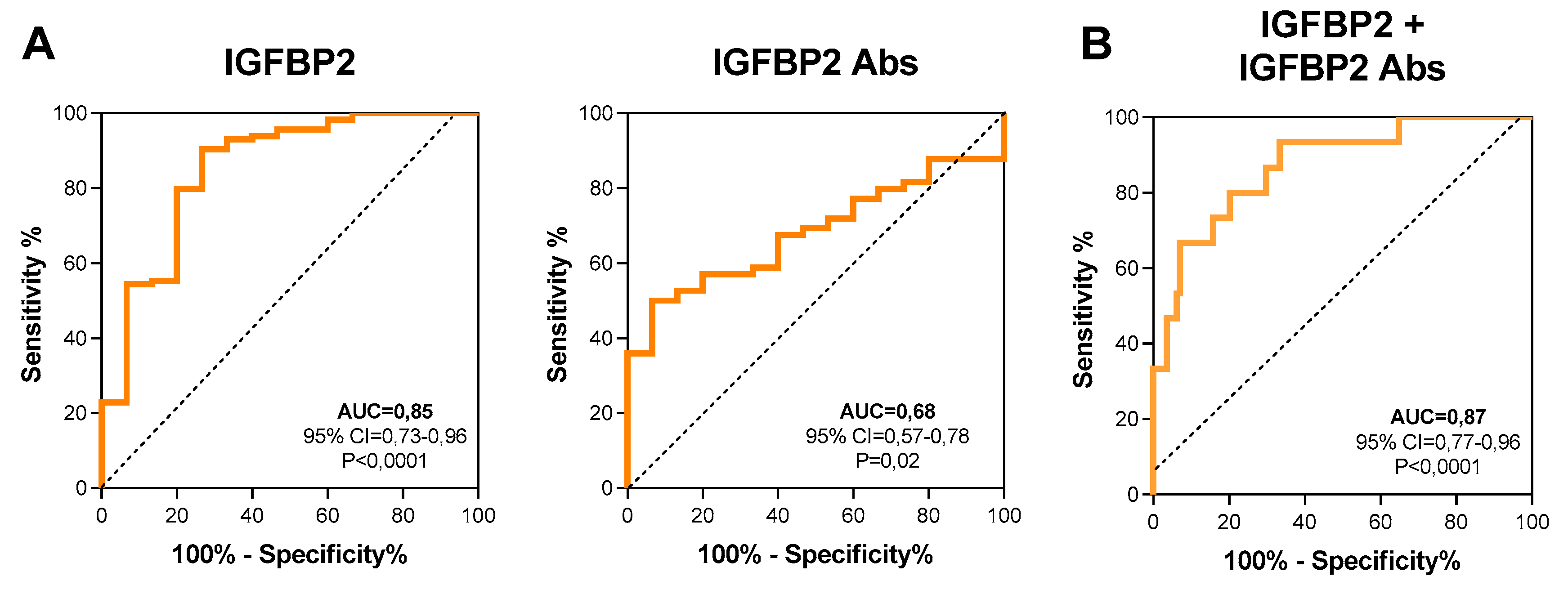
3.2. Plasmatic IGFBP2 Protein and Anti-IGFBP2 Autoantibodies as Diagnostic Biomarkers in RMS Patients
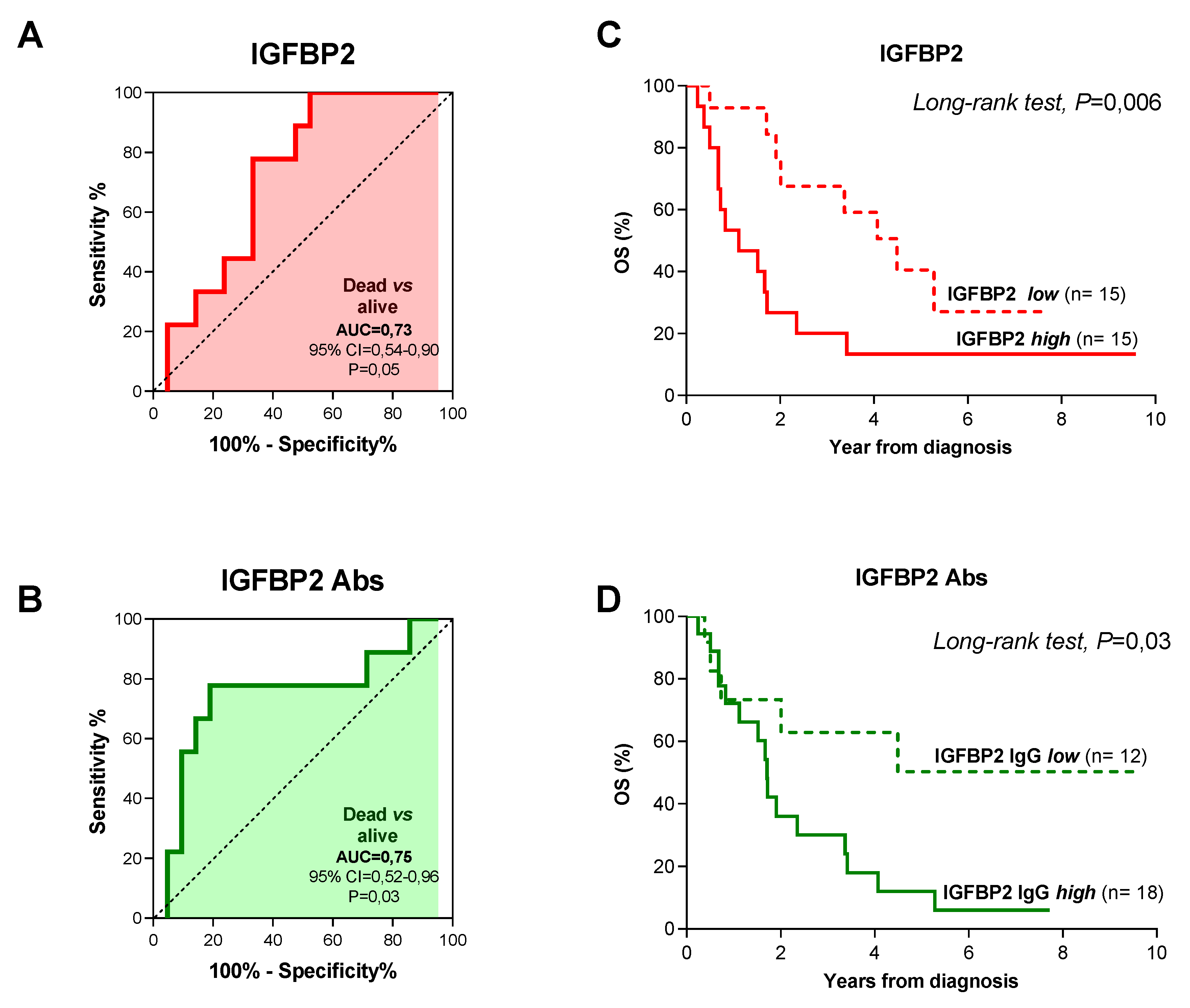
3.3. IGFBP2 and Anti-IGFBP2 Antibodies Prognostic Significance
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| IGFBP2 | Insulin-like growth factor-binding protein 2 |
| IGF | Insulin growth factor |
| RMS | Rhabdomyosarcoma |
| ARMS | Alveolar Rhabdomyosarcoma |
| ERMS | Embryonal Rhabdomyosarcoma |
| SRMS | Spindle cell/Sclerosing Rhabdomyosarcoma |
| PRMS | Pleomorphic Rhabdomyosarcoma |
| HS | Healthy subjects |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| TAA | Tumor-Associated Antigens |
| TAAB | Tumor-Associated Autoantibodies |
| CI | Confidence Interval |
| Yrs | Years |
| Abs | Antibodies |
| ROC | Receiver-Operator Characteristic curve |
| AUC | Area Under the Curve |
| IRS | International Rhabdomyosarcoma Study Group |
| EFS | Event-Free Survival |
| OS | Overall Survival |
References
- Linet, M.S.; Ries, L.A.; Smith, M.A.; Tarone, R.E.; Devesa, S.S. Cancer surveillance series: recent trends in childhood cancer incidence and mortality in the United States. J. Natl. Cancer. Inst. 1999, 91, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Rudzinski, E.R.; Anderson, J.R.; Hawkins, D.S.; Skapek, S.X.; Parham, D.M.; Teot, L.A. The World Health Organization Classification of Skeletal Muscle Tumors in Pediatric Rhabdomyosarcoma: A Report From the Children’s Oncology Group. Arch. Pathol. Lab. Med. 2015, 139, 1281–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, S.J.; Pressey, J.G.; Barr, F.G. Molecular pathogenesis of rhabdomyosarcoma. Cancer Biol. Ther. 2002, 1, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, P.H.; Lynch, J.C.; Qualman, S.J.; Tirabosco, R.; Lim, J.F.; Maurer, H.M.; Bridge, J.A.; Crist, W.M.; Triche, T.J.; Barr, F.G. PAX3-FKHR and PAX7-FKHR gene fusions are prognostic indicators in alveolar rhabdomyosarcoma: a report from the children’s oncology group. J. Clin. Oncol. 2002, 20, 2672–2679. [Google Scholar] [CrossRef]
- Davis, R.J.; D’Cruz, C.M.; Lovell, M.A.; Biegel, J.A.; Barr, F.G. Fusion of PAX7 to FKHR by the variant t(1;13)(p36;q14) translocation in alveolar rhabdomyosarcoma. Cancer Res. 1994, 54, 2869–2872. [Google Scholar]
- Weber-Hall, S.; Anderson, J.; McManus, A.; Abe, S.; Nojima, T.; Pinkerton, R.; Pritchard-Jones, K.; Shipley, J. Gains, losses, and amplification of genomic material in rhabdomyosarcoma analyzed by comparative genomic hybridization. Cancer Res. 1996, 56, 3220–3224. [Google Scholar]
- Oberlin, O.; Rey, A.; Lyden, E.; Bisogno, G.; Stevens, M.C.; Meyer, W.H.; Carli, M.; Anderson, J.R. Prognostic factors in metastatic rhabdomyosarcomas: results of a pooled analysis from United States and European cooperative groups. J. Clin. Oncol. 2008, 26, 2384–2389. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, I.; Nagata, M.; Takiguchi, N.; Nabeya, Y.; Ikeda, A.; Yokoi, S.; Kuwajima, A.; Tagawa, M.; Matsushita, K.; Sstoshi, Y.; et al. Panel of autoanti-bodies against multiple tumor-associated antigens for detecting gastric cancer. Cancer Sci. 2017, 108, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Xian, Z.; Fu, D.; Liu, S.; Yao, Y.; Gao, C. Association between B Cell Growth Factors and Primary Sjögren’s Syndrome-Related Autoantibodies in Patients with Non-Hodgkin’s Lymphoma. J. Immunol. Res. 2019, 2019, 7627384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Qin, J.; Ye, H.; Li, L.; Wang, X.; Zhang, J. Using a panel of multiple tumor-associated antigens to enhance the autoantibody detection in the immunodiagnosis of ovarian cancer. J. Cell Biochem. 2019, 120, 3091–3100. [Google Scholar] [CrossRef] [PubMed]
- Nagayoshi, Y.; Nakamura, M.; Matsuoka, K.; Ohtsuka, T.; Mori, Y.; Kono, H.; Aso, T.; Ideno, N.; Takahata, S.; Ryo, A.; et al. Profiling of autoantibodies in sera of pancreatic cancer patients. Ann. Surg. Oncol. 2014, 21, S459–S465. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.F.; Qin, J.J.; Ren, P.F.; Shi, J.X.; Xia, J.F.; Ye, H.; Wang, P.; Song, C.H.; Wang, K.J.; Zhang, J.Y. A panel of autoantibodies against multiple tumor-associated antigens in the immunodiagnosis of esophageal squamous cell cancer. Cancer Immunol. Immunother 2016, 65, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Babel, I.; Barderas, R.; Díaz-Uriarte, R.; Martínez-Torrecuadrada, J.L.; Sánchez-Carbayo, M.; Casal, J.I. Identification of tumor-associated autoantigens for the diagnosis of colorectal cancer in serum using high density protein microarrays. Mol. Cell Proteomics 2009, 8, 2382–2395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babel, I.; Barderas, R.; Diaz-Uriarte, R.; Moreno, V.; Suarez, A.; Fernandez-Aceñero, M.J.; Ramón, S.; Capellá, G.; Casal, I. Identification of MST1/STK4 and SULF1 proteins as autoantibody targets for the diagnosis of colorectal cancer by using phage microarrays. Mol. Cell Proteomics 2011, 10, M110. [Google Scholar] [CrossRef] [Green Version]
- Le Roith, D.; Blakesley, V.A. The yin and the yang of the IGF system: immunological manifestations of GH resistance. Eur. J. Endocrinol 1997, 136, 33–34. [Google Scholar] [CrossRef]
- Chua, C.Y.; Liu, Y.; Granberg, K.J.; Hu, L.; Haapasalo, H.; Annala, M.J.; Cogdell, D.E.; Verploegen, M.; Moore, L.M.; Fuller, G.N.; et al. IGFBP2 potentiates nuclear EGFR-STAT3 signaling. Oncogene 2016, 35, 738–747. [Google Scholar] [CrossRef] [Green Version]
- Rajaram, S.; Baylink, D.J.; Mohan, S. Insulin-like growth factor-binding proteins in serum and other biological fluids: regulation and functions. Endocr. Rev. 1997, 18, 801–831. [Google Scholar]
- Kalli, K.R.; Krco, C.J.; Hartmann, L.C.; Goodman, K.; Maurer, M.J.; Yu, C.; Johnson, E.M.; Erskine, C.L.; Disis, M.L.; Wettstein, P.J.; et al. An HLA-DR-degenerate epitope pool detects insulin-like growth factor binding protein2-specific immunity in patients with cancer. Cancer Res. 2008, 68, 4893–4901. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Zhang, Y.; Ramanujan, K.; Ma, Y.; Kirsch, D.G.; Glass, D.J. Oncogenic NRAS, required for pathogenesis of embryonic rhabdomyosarcoma, relies upon the HMGA2-IGF2BP2 pathway. Cancer Res. 2013, 73, 3041–3050. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Ying, X.; Han, S.; Wang, J.; Zhou, X.; Bai, E.; Zhang, J.Y.; Zhu, Q. Autoantibodies against insulin-like growth factor binding protein-2 as a serological biomarker in the diagnosis of lung cancer. Int. J. Oncol. 2013, 42, 93–100. [Google Scholar] [CrossRef] [Green Version]
- De Pittà, C.; Tombolan, L.; Albiero, G.; Sartori, F.; Romualdi, C.; Jurman, G.; Carli, M.; Furlamo, C.; Lanfranchi, G.; Rosolen, A. Gene expression profiling identifies potential relevant genes in alveolar rhabdomyosarcoma pathogenesis and discriminates PAX3-FKHR positive and negative tumors. Int. J. Cancer 2006, 118, 2772–2781. [Google Scholar] [CrossRef] [PubMed]
- Tombolan, L.; Orso, F.; Guzzardo, V.; Casara, S.; Zin, A.; Bonora, M.; Romualdi, C.; Giorgi, C.; Bisogno, G.; Alaggio, R.; et al. High IGFBP2 expres-sion correlates with tumor severity in pediatric rhabdomyosarcoma. Am. J. Pathol. 2011, 179, 2611–2624. [Google Scholar] [CrossRef] [PubMed]
- Jalal, H.; Pechlivanoglou, P.; Krijkamp, E.; Alarid-Escudero, F.; Enns, E.; Hunink, M.G.M. An Overview of R in Health Decision Sciences. Med. Decis. Making 2017, 37, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.R.; Lyden, E.R.; Anderson, J.R.; Hawkins, D.S.; Spunt, S.L.; Walterhouse, D.O.; Wolden, S.L.; Parham, D.M.; Rodeberg, D.A.; Kao, S.C.; et al. Histo-logic and clinical characteristics can guide staging evaluations for children and adolescents with rhabdomyosarcoma: a report from the Children’s Oncology Group Soft Tissue Sarcoma Committee. J. Clin. Oncol. 2013, 31, 3226–3232. [Google Scholar] [CrossRef]
- Arnold, M.A.; Anderson, J.R.; Gastier-Foster, J.M.; Barr, F.G.; Skapek, S.X.; Hawkins, D.S.; Jr Raney, R.B.; Parham, D.M.; Teot, L.A.; Rudzinski, E.R.; et al. Histology, Fusion Status, and Outcome in Alveolar Rhabdomyosarcoma With Low-Risk Clinical Features: A Report From the Children’s Oncology Group. Pediatr Blood Cancer 2016, 63, 634–639. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Guo, W.; Shen, J.K.; Mankin, H.J.; Hornicek, F.J.; Duan, Z. Rhabdomyosarcoma: Advances in Molecular and Cellular Biology. Sarcoma 2015, 2015, 232010. [Google Scholar] [CrossRef] [Green Version]
- Rudzinski, E.R.; Anderson, J.R.; Chi, Y.Y.; Gastier-Foster, J.M.; Astbury, C.; Barr, F.G.; Skapek, S.X.; Hawkins, D.S.; Weigel, B.J.; Pappo, A.; et al. Histology, fusion status, and outcome in metastatic rhabdomyosarcoma: A report from the Children’s Oncology Group. Pediatr Blood Cancer 2017, 64, e26645. [Google Scholar] [CrossRef]
- Kim, J.R.; Yoon, H.M.; Koh, K.N.; Jung, A.Y.; Cho, Y.A.; Lee, J.S. Rhabdomyosarcoma in Children and Adolescents: Patterns and Risk Factors of Distant Metastasis. AJR Am. J. Roentgenol 2017, 209, 409–416. [Google Scholar] [CrossRef]
- Mohan, A.C.; Venkatramani, R.; Okcu, M.F.; Nuchtern, J.G.; Vasudevan, S.A.; Mahajan, A.; Rainusso, N.C.; Allen-Rhoades, W.; Chintagumpala, M.; Paulino, A. Local therapy to distant metastatic sites in stage IV rhabdomyosarcoma. Pediatr Blood Cancer 2018, 65, e26859. [Google Scholar] [CrossRef]
- Borinstein, S.C.; Steppan, D.; Hayashi, M.; Loeb, D.M.; Isakoff, M.S.; Binitie, O.; Brohl, A.S.; Bridge, J.A.; Stavas, M.; Shinohara, E.T.; et al. Consensus and controversies regarding the treatment of rhabdomyosarcoma. Pediatr Blood Cancer 2018, 65, e26809. [Google Scholar] [CrossRef] [Green Version]
- Gallego, S.; Zanetti, I.; Orbach, D.; Ranchère, D.; Shipley, J.; Zin, A.; Bergeron, C.; de Salvo, G.L.; Chisholm, J.; Ferrari, A.; et al. Fusion status in patients with lymph node-positive (N1) alveolar rhabdomyosarcoma is a powerful predictor of prog-nosis: Experience of the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG). Cancer 2018, 124, 3201–3209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaenker, P.; Gray, E.S.; Ziman, M.R. Autoantibody Production in Cancer-The Humoral Immune Response toward Autologous Antigens in Cancer Patients. Autoimmun. Rev. 2016, 15, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yadav, S.; Kashaninejad, N.; Masud, M.K.; Yamauchi, Y.; Nguyen, N.T.; Shiddiky, M.J.A. Autoantibodies as diagnostic and prognostic cancer biomarker: Detection techniques and approaches. Biosens Bioelectron 2019, 139, 111315. [Google Scholar] [CrossRef] [PubMed]
- Bassaro, L.; Russell, S.J.; Pastwa, E.; Somiari, S.A.; Somiari, R.I. Screening for Multiple Autoanti-bodies in Plasma of Patients with Breast Cancer. Cancer Genomics Proteomics 2017, 14, 427–435. [Google Scholar]
- Wu, J.; Li, X.; Song, W.; Fang, Y.; Yu, L.; Liu, S.; Churilov, L.P.; Zhang, F. The roles and applications of autoantibodies in progression, diagnosis, treatment and prognosisof human malignant tumours. Autoimmun Rev 2017, 16, 1270–1281. [Google Scholar] [CrossRef]
- Tang, Z.M.; Ling, Z.G.; Wang, C.M.; Wu, Y.B.; Kong, J.L. Serum tumor-associated autoantibodies as diagnostic biomarkers for lung cancer: A systematic review and meta-analysis. Plos ONE 2017, 12, e0182117. [Google Scholar] [CrossRef] [Green Version]
- Meeusen, E.; Lim, E.; Mathivanan, S. Secreted Tumor Antigens - Immune Biomarkers for Diagnosis and Therapy. Proteomics 2017, 17, 23–24. [Google Scholar] [CrossRef]
- Li, Y.; Jiang, T.; Zhang, J.; Zhang, B.; Yang, W.; You, G.; Xu, K.; Wu, J.; Luo, C.; Song, S.W. Elevated serum antibodies against insulin-like growth factor-binding protein-2 allow detecting early-stage cancers: evidences from glioma and colorectal carcinoma studies. Ann. Oncol. 2012, 23, 2415–2422. [Google Scholar] [CrossRef]
- Pickard, A.; McCance, D.J. IGF-Binding Protein 2 - Oncogene or Tumor Suppressor? Front Endocrinol. (Lausanne) 2015, 6, 25. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.; Sun, S.; Zhou, X.; Guo, W.; Zhang, L. IGF-binding protein 2 is a candidate target of therapeutic otential in cancer. Tumour Biol. 2016, 37, 1451–1459. [Google Scholar] [CrossRef]
- Russo, V.C.; Azar, W.J.; Yau, S.W.; Sabin, M.A.; Werther, G.A. IGFBP-2: The dark horse in metabolism and cancer. Cytokine Growth Factor Rev. 2015, 26, 329–346. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.C. IGF binding proteins in cancer: mechanistic and clinical insights. Nat. Rev. Cancer 2014, 14, 329–341. [Google Scholar] [CrossRef] [PubMed]
- Kang, Z.; Yu, Y.; Zhu, Y.J.; Davis, S.; Walker, R.; Meltzer, P.S.; Helman, L.J.; Cao, L. Downregulation of IGFBP2 is associated with resistance to IGF1R therapy in rhabdomyosarcoma. Oncogene 2014, 33, 5697–5705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Fu, L.; Wang, S.; Jin, Y.; Han, S.; Chu, P.; Lu, J.; Guo, Y.; He, L.; Ni, X. Investigation of IGF2, IGFBP2 and p63 proteins in rhabdomyosarcoma tumors. Growth Horm IGF Res 2017, 33, 17–22. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # of Cases (%) | ||
|---|---|---|
| Gender | Male | 58 (51%) |
| Female | 56 (49%) | |
| Age | <10 years | 72 (63%) |
| ≥10 years | 42 (37%) | |
| Site | Favorable * | 27 (24%) |
| Unfavorable * | 81 (71%) | |
| Unknown | 6 (5%) | |
| Size | ≤5 cm | 36 (32%) |
| >5 cm | 67 (59%) | |
| Not evaluable | 3 (3%) | |
| Unknown | 8 (6%) | |
| IRS Group† | I | 3 (3%) |
| II | 9 (8%) | |
| III | 63 (55%) | |
| IV | 35 (30%) | |
| Unknown | 4 (4%) | |
| Histology | ARMS | 50 (44%) |
| ERMS | 55 (62%) | |
| SRMS, PRMS | 9 (8%) | |
| Fusion Status | PAX3/7-FOXO1 + | 40 (35%) |
| PAX3/7-FOXO1 − | 74 (65%) | |
| Clinical Features | # of Cases | Univ. P-Value | HR | CI 95% | |
|---|---|---|---|---|---|
| Gender | Male | 14 | 0.283 | ||
| Female | 16 | ||||
| Age | <10 years | 13 | 0.191 | ||
| ≥10 years | 17 | ||||
| Site | Favorable | 4 | 0.614 | ||
| Unfavorable | 24 | ||||
| Size | ≤5 cm | 10 | 0.112 | ||
| >5 cm | 17 | ||||
| IGFBP2 Abs | >1808 ng/mL | 18 | 0.27 | ||
| ≤1808 ng/mL | 12 | ||||
| IGFBP2 | >290,55 ng/mL | 15 | 0.004 | 3.718 | 1.52–9.09 |
| ≤290,55 ng/mL | 15 | ||||
| Histology | ERMS | 8 | 0.212 | ||
| SRMS, PRMS | 2 | 0.668 | |||
| ARMS | 20 | ||||
| Fusion Status | PAX-FOXO1 + | 20 | 0.201 | ||
| PAX-FOXO1 − | 10 |
| Clinical Features | # of Cases | Univ. P-Value | Multiv. P-Value | HR | CI 95% | |
|---|---|---|---|---|---|---|
| Gender | Male | 14 | 0.163 | |||
| Female | 16 | |||||
| Age | <10 years | 13 | 0.745 | |||
| ≥10 years | 17 | |||||
| Tumor Site | Favourable | 4 | 0.53 | |||
| Unfavourable | 24 | |||||
| Tumor Size | ≤5 cm | 10 | 0.895 | |||
| >5 cm | 17 | |||||
| IGFBP2 Abs | >1808 ng/mL | 18 | 0.04 | 0.037 | 3.102 | 1.069–8.999 |
| ≤1808 ng/mL | 12 | |||||
| IGFBP2 | >316,24 ng/mL | 15 | 0.026 | 0.024 | 2.872 | 1.146–7.20 |
| ≤316,24 ng/mL | 15 | |||||
| Histology | ERMS | 8 | 0.427 | |||
| SRMS, PRMS | 2 | |||||
| ARMS | 20 | 0.822 | ||||
| Fusion Status | PAX-FOXO1 + | 20 | 0.506 | |||
| PAX-FOXO1 − | 10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poli, E.; Zin, A.; Cattelan, M.; Tombolan, L.; Zanetti, I.; Scagnellato, A.; Bonvini, P.; Bisogno, G. Prognostic Value of Circulating IGFBP2 and Related Autoantibodies in Children with Metastatic Rhabdomyosarcomas. Diagnostics 2020, 10, 115. https://doi.org/10.3390/diagnostics10020115
Poli E, Zin A, Cattelan M, Tombolan L, Zanetti I, Scagnellato A, Bonvini P, Bisogno G. Prognostic Value of Circulating IGFBP2 and Related Autoantibodies in Children with Metastatic Rhabdomyosarcomas. Diagnostics. 2020; 10(2):115. https://doi.org/10.3390/diagnostics10020115
Chicago/Turabian StylePoli, Elena, Angelica Zin, Manuela Cattelan, Lucia Tombolan, Ilaria Zanetti, Angela Scagnellato, Paolo Bonvini, and Gianni Bisogno. 2020. "Prognostic Value of Circulating IGFBP2 and Related Autoantibodies in Children with Metastatic Rhabdomyosarcomas" Diagnostics 10, no. 2: 115. https://doi.org/10.3390/diagnostics10020115