Urinary MicroRNA-21-5p as Potential Biomarker of Interstitial Fibrosis and Tubular Atrophy (IFTA) in Kidney Transplant Recipients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. MicroRNA Analysis
2.3. Statistical Analysis
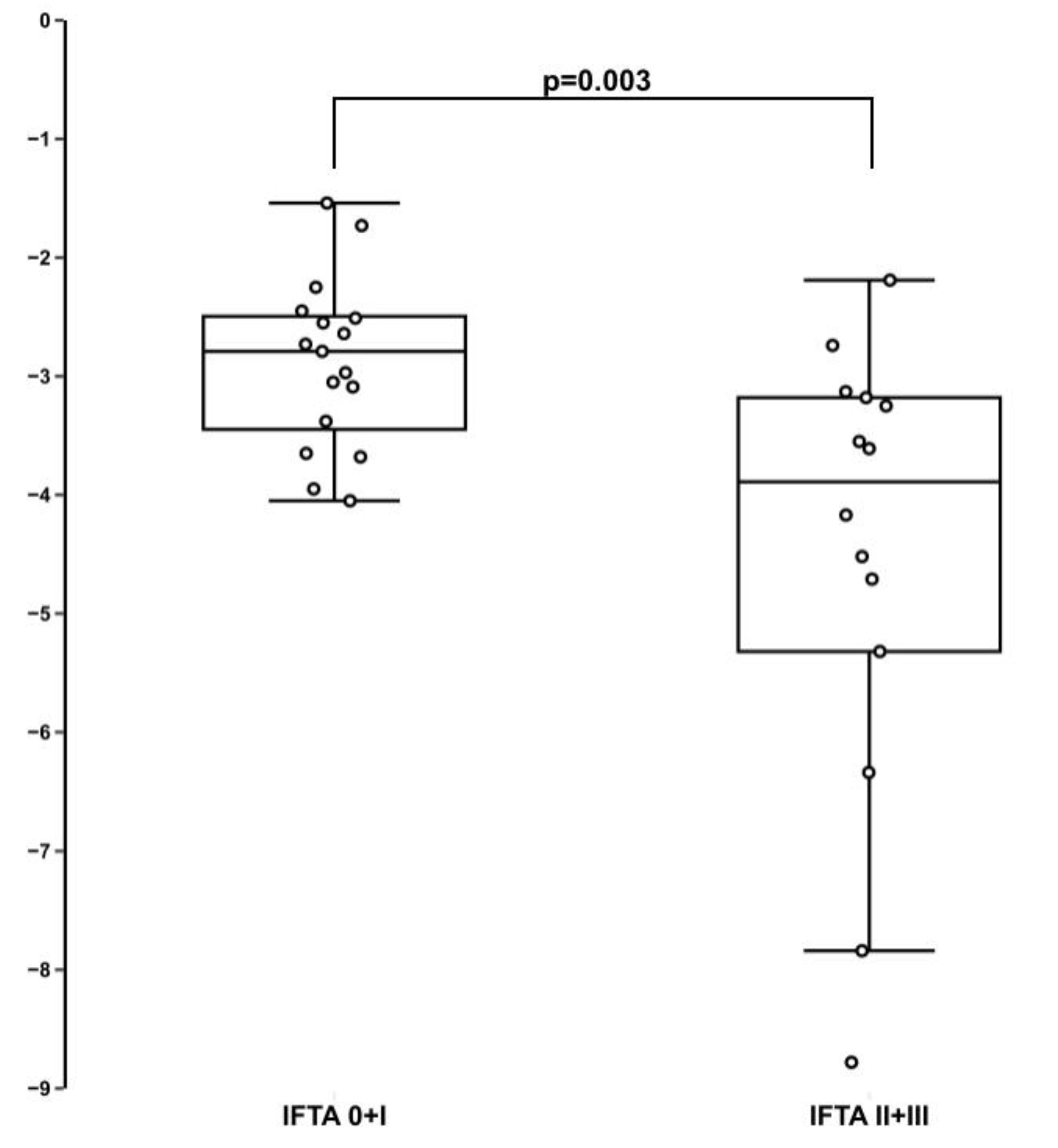
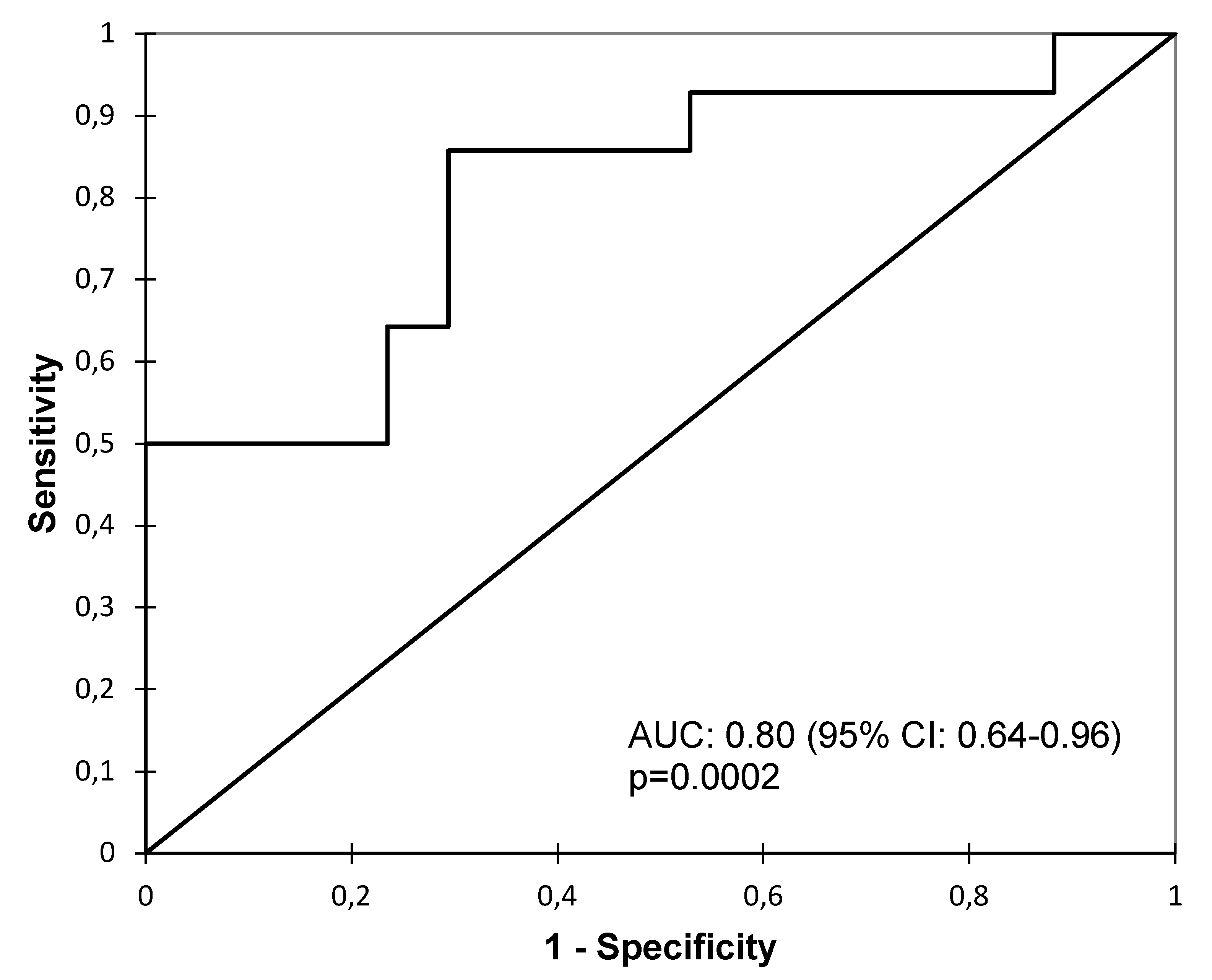
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Voora, S.; Adey, D.B. Management of Kidney Transplant Recipients by General Nephrologists: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 73, 866–879. [Google Scholar] [CrossRef]
- Racusen, L.C.; Regele, H. The pathology of chronic allograft dysfunction. Kidney Int. Suppl. 2010. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, R.J.; Weng, F.L.; Kandula, P. Acute and Chronic Allograft Dysfunction in Kidney Transplant Recipients. Med. Clin. N. Am. 2016, 100, 487–503. [Google Scholar] [CrossRef]
- Pascual, J.; Perez-Saez, M.J.; Mir, M.; Crespo, M. Chronic renal allograft injury: Early detection, accurate diagnosis and management. Transplant. Rev. 2012, 26, 280–290. [Google Scholar] [CrossRef]
- Chand, S.; Atkinson, D.; Collins, C.; Briggs, D.; Ball, S.; Sharif, A.; Skordilis, K.; Vydianath, B.; Neil, D.; Borrows, R. The Spectrum of Renal Allograft Failure. PLoS ONE 2016, 11, e0162278. [Google Scholar] [CrossRef] [PubMed]
- Roufosse, C.; Simmonds, N.; Clahsen-van Groningen, M.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasinska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, B.M.; Haylor, J. Biological pathways and potential targets for prevention and therapy of chronic allograft nephropathy. Biomed. Res. Int. 2014, 2014, 482438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giral, M.; Renaudin, K.; Naesens, M.; Luning, R.; Anglicheau, D.; Morelon, E.; Huneau, A.; Paul, C.; Brouard, S.; Couvrat-Desvergnes, G.; et al. The 1-year Renal Biopsy Index: A scoring system to drive biopsy indication at 1-year post-kidney transplantation. Transpl. Int. 2018. [Google Scholar] [CrossRef] [Green Version]
- Henderson, L.K.; Nankivell, B.J.; Chapman, J.R. Surveillance protocol kidney transplant biopsies: Their evolving role in clinical practice. Am. J. Transplant. 2011, 11, 1570–1575. [Google Scholar] [CrossRef]
- Morgan, T.A.; Chandran, S.; Burger, I.M.; Zhang, C.A.; Goldstein, R.B. Complications of Ultrasound-Guided Renal Transplant Biopsies. Am. J. Transplant. 2016, 16, 1298–1305. [Google Scholar] [CrossRef]
- Brachemi, S.; Bollee, G. Renal biopsy practice: What is the gold standard? World J. Nephrol. 2014, 3, 287–294. [Google Scholar] [CrossRef]
- Scian, M.J.; Maluf, D.G.; David, K.G.; Archer, K.J.; Suh, J.L.; Wolen, A.R.; Mba, M.U.; Massey, H.D.; King, A.L.; Gehr, T.; et al. MicroRNA profiles in allograft tissues and paired urines associate with chronic allograft dysfunction with IF/TA. Am. J. Transplant. 2011, 11, 2110–2122. [Google Scholar] [CrossRef]
- Van de Vrie, M.; Deegens, J.K.; Eikmans, M.; van der Vlag, J.; Hilbrands, L.B. Urinary MicroRNA as Biomarker in Renal Transplantation. Am. J. Transplant. 2017, 17, 1160–1166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, D.P. MicroRNAs: Target recognition and regulatory functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staszel, T.; Zapala, B.; Polus, A.; Sadakierska-Chudy, A.; Kiec-Wilk, B.; Stepien, E.; Wybranska, I.; Chojnacka, M.; Dembinska-Kiec, A. Role of microRNAs in endothelial cell pathophysiology. Pol. Arch. Med. Wewn 2011, 121, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Wan, X.; Ruan, Q. The MicroRNA-21 in Autoimmune Diseases. Int. J. Mol. Sci. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Akker, E.K.; Dor, F.J.; JN, I.J.; de Bruin, R.W. MicroRNAs in Kidney Transplantation: Living up to Their Expectations? J. Transplant. 2015, 2015, 354826. [Google Scholar] [CrossRef] [Green Version]
- Glowacki, F.; Savary, G.; Gnemmi, V.; Buob, D.; Van der Hauwaert, C.; Lo-Guidice, J.M.; Bouye, S.; Hazzan, M.; Pottier, N.; Perrais, M.; et al. Increased circulating miR-21 levels are associated with kidney fibrosis. PLoS ONE 2013, 8, e58014. [Google Scholar] [CrossRef]
- Hennino, M.F.; Buob, D.; Van der Hauwaert, C.; Gnemmi, V.; Jomaa, Z.; Pottier, N.; Savary, G.; Drumez, E.; Noel, C.; Cauffiez, C.; et al. miR-21-5p renal expression is associated with fibrosis and renal survival in patients with IgA nephropathy. Sci. Rep. 2016, 6, 27209. [Google Scholar] [CrossRef] [Green Version]
- Lakhia, R.; Hajarnis, S.; Williams, D.; Aboudehen, K.; Yheskel, M.; Xing, C.; Hatley, M.E.; Torres, V.E.; Wallace, D.P.; Patel, V. MicroRNA-21 Aggravates Cyst Growth in a Model of Polycystic Kidney Disease. J. Am. Soc. Nephrol. 2016, 27, 2319–2330. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Li, X. Key Genes Involved in Diabetic Nephropathy Investigated by Microarray Analysis. J. Comput. Biol. 2019, 26, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Nalewajska, M.; Gurazda, K.; Styczynska-Kowalska, E.; Marchelek-Mysliwiec, M.; Pawlik, A.; Dziedziejko, V. The Role of MicroRNAs in Selected Forms of Glomerulonephritis. Int. J. Mol. Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, B.; Jin, Y.; Zhang, H.; Zhao, R.; Sun, M.; Sun, M.; Yuan, X.; Wang, W.; Wang, X.; Chen, Z.; et al. MicroRNA21 contributes to renal cell carcinoma cell invasiveness and angiogenesis via the PDCD4/cJun (AP1) signalling pathway. Int. J. Oncol. 2020, 56, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Khalid, U.; Newbury, L.J.; Simpson, K.; Jenkins, R.H.; Bowen, T.; Bates, L.; Sheerin, N.S.; Chavez, R.; Fraser, D.J. A urinary microRNA panel that is an early predictive biomarker of delayed graft function following kidney transplantation. Sci. Rep. 2019, 9, 3584. [Google Scholar] [CrossRef]
- Zununi Vahed, S.; Poursadegh Zonouzi, A.; Ghanbarian, H.; Ghojazadeh, M.; Samadi, N.; Omidi, Y.; Ardalan, M. Differential expression of circulating miR-21, miR-142-3p and miR-155 in renal transplant recipients with impaired graft function. Int. Urol. Nephrol. 2017, 49, 1681–1689. [Google Scholar] [CrossRef]
- Stegall, M.D.; Park, W.D.; Larson, T.S.; Gloor, J.M.; Cornell, L.D.; Sethi, S.; Dean, P.G.; Prieto, M.; Amer, H.; Textor, S.; et al. The histology of solitary renal allografts at 1 and 5 years after transplantation. Am. J. Transplant. 2011, 11, 698–707. [Google Scholar] [CrossRef]
- Egidi, M.G.; Cochetti, G.; Guelfi, G.; Zampini, D.; Diverio, S.; Poli, G.; Mearini, E. Stability Assessment of Candidate Reference Genes in Urine Sediment of Prostate Cancer Patients for miRNA Applications. Dis. Mark. 2015, 2015, 973597. [Google Scholar] [CrossRef]
- Beltrami, C.; Simpson, K.; Jesky, M.; Wonnacott, A.; Carrington, C.; Holmans, P.; Newbury, L.; Jenkins, R.; Ashdown, T.; Dayan, C.; et al. Association of Elevated Urinary miR-126, miR-155, and miR-29b with Diabetic Kidney Disease. Am. J. Pathol. 2018, 188, 1982–1992. [Google Scholar] [CrossRef]
- Zhou, X.; Marian, C.; Makambi, K.H.; Kosti, O.; Kallakury, B.V.; Loffredo, C.A.; Zheng, Y.L. MicroRNA-9 as potential biomarker for breast cancer local recurrence and tumor estrogen receptor status. PLoS ONE 2012, 7, e39011. [Google Scholar] [CrossRef]
- Sun, I.O.; Lerman, L.O. Urinary microRNA in kidney disease: Utility and roles. Am. J. Physiol. Ren. Physiol. 2019, 316, F785–F793. [Google Scholar] [CrossRef]
- Verhoeven, J.; Boer, K.; Van Schaik, R.H.N.; Manintveld, O.C.; Huibers, M.M.H.; Baan, C.C.; Hesselink, D.A. Liquid Biopsies to Monitor Solid Organ Transplant Function: A Review of New Biomarkers. Ther. Drug Monit. 2018, 40, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Ben-Dov, I.Z.; Muthukumar, T.; Morozov, P.; Mueller, F.B.; Tuschl, T.; Suthanthiran, M. MicroRNA sequence profiles of human kidney allografts with or without tubulointerstitial fibrosis. Transplantation 2012, 94, 1086–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, B.N.; Xin, C.; Hartner, J.; Ren, S.; Castano, A.P.; Linn, G.; Li, J.; Tran, P.T.; Kaimal, V.; Huang, X.; et al. MicroRNA-21 promotes fibrosis of the kidney by silencing metabolic pathways. Sci. Transl. Med. 2012, 4, 121ra118. [Google Scholar] [CrossRef] [Green Version]
- Lyu, H.; Li, X.; Wu, Q.; Hao, L. Overexpression of microRNA-21 mediates Ang II-induced renal fibrosis by activating the TGF-beta1/Smad3 pathway via suppressing PPARalpha. J. Pharmacol. Sci. 2019, 141, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Xu, T.; Chen, Y.; Qu, W.; Sun, D.; Song, X.; Yuan, Q.; Yao, L. Pioglitazone attenuates kidney fibrosis via miR-21-5p modulation. Life Sci. 2019, 232, 116609. [Google Scholar] [CrossRef] [PubMed]
- Vandenbussche, C.; Van der Hauwaert, C.; Dewaeles, E.; Franczak, J.; Hennino, M.F.; Gnemmi, V.; Savary, G.; Tavernier, Q.; Nottet, N.; Paquet, A.; et al. Tacrolimus-induced nephrotoxicity in mice is associated with microRNA deregulation. Arch. Toxicol. 2018, 92, 1539–1550. [Google Scholar] [CrossRef]
- Chen, J.; Zmijewska, A.; Zhi, D.; Mannon, R.B. Cyclosporine-mediated allograft fibrosis is associated with micro-RNA-21 through AKT signaling. Transpl. Int. 2015, 28, 232–245. [Google Scholar] [CrossRef]
- Dey, N.; Ghosh-Choudhury, N.; Kasinath, B.S.; Choudhury, G.G. TGFbeta-stimulated microRNA-21 utilizes PTEN to orchestrate AKT/mTORC1 signaling for mesangial cell hypertrophy and matrix expansion. PLoS ONE 2012, 7, e42316. [Google Scholar] [CrossRef]
- McClelland, A.D.; Herman-Edelstein, M.; Komers, R.; Jha, J.C.; Winbanks, C.E.; Hagiwara, S.; Gregorevic, P.; Kantharidis, P.; Cooper, M.E. miR-21 promotes renal fibrosis in diabetic nephropathy by targeting PTEN and SMAD7. Clin. Sci. 2015, 129, 1237–1249. [Google Scholar] [CrossRef]
- Zununi Vahed, S.; Omidi, Y.; Ardalan, M.; Samadi, N. Dysregulation of urinary miR-21 and miR-200b associated with interstitial fibrosis and tubular atrophy (IFTA) in renal transplant recipients. Clin. Biochem. 2017, 50, 32–39. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| IFTA 0 + I (n = 17) | IFTA II + III (n = 14) | p Value | |
|---|---|---|---|
| Age at biopsy, years, mean (SD) | 54.76 (10.74) | 48.38 (14.95) | 0.18 |
| Male sex, n (%) | 12 (70.59) | 8 (57.14) | 0.31 |
| Body mass index, kg/m2, mean (SD) | 25.48 (3.48) | 23.58 (4.06) | 0.18 |
| First transplantation, n (%) | 15 (88.24) | 14 (100.00) | 0.49 |
| Cold ischemia time, min, mean (SD) | 1249.33 (420.32) | 1262.14 (530.34) | 0.95 |
| Warm ischemia time, min, mean (SD) | 35.08 (7.47) | 32.08 (5.33) | 0.25 |
| Delayed graft function, n (%) | 5 (29.41) | 5 (35.71) | 0.71 |
| Time of biopsy after transplantation | 0.82 | ||
| 1 year, n (%) | 9 (52.94) | 8 (57.14) | |
| 2 years, n (%) | 8 (47.06) | 6 (42.86) | |
| Serum creatinine, mg/dl, mean (SD) | 1.31 (0.28) | 1.62 (0.35) | 0.01 |
| eGFR (CKD-EPI), mg/dl/1.72 m2, mean (SD) | 58.82 (14.99) | 46.50 (11.77) | 0.02 |
| Human leukocyte antigen (HLA) mismatches, mean (Q1–Q3) | 3.59 (2.50–5.00) | 3.29 (3.00–4.00) | 0.52 |
| Immunosuppressive therapy (tacrolimus, mycophenolate mofetil and corticosteroids), n (%) | 17 (100) | 14 (100) | 1.00 |
| Blood tacrolimus level, ng/mL, mean (SD) | 6.02 (1.79) | 5.72 (1.43) | 0.48 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gniewkiewicz, M.S.; Paszkowska, I.; Gozdowska, J.; Czerwinska, K.; Sadowska-Jakubowicz, A.; Deborska-Materkowska, D.; Perkowska-Ptasinska, A.; Kosieradzki, M.; Durlik, M. Urinary MicroRNA-21-5p as Potential Biomarker of Interstitial Fibrosis and Tubular Atrophy (IFTA) in Kidney Transplant Recipients. Diagnostics 2020, 10, 113. https://doi.org/10.3390/diagnostics10020113
Gniewkiewicz MS, Paszkowska I, Gozdowska J, Czerwinska K, Sadowska-Jakubowicz A, Deborska-Materkowska D, Perkowska-Ptasinska A, Kosieradzki M, Durlik M. Urinary MicroRNA-21-5p as Potential Biomarker of Interstitial Fibrosis and Tubular Atrophy (IFTA) in Kidney Transplant Recipients. Diagnostics. 2020; 10(2):113. https://doi.org/10.3390/diagnostics10020113
Chicago/Turabian StyleGniewkiewicz, Michal S., Izabela Paszkowska, Jolanta Gozdowska, Katarzyna Czerwinska, Anna Sadowska-Jakubowicz, Dominika Deborska-Materkowska, Agnieszka Perkowska-Ptasinska, Maciej Kosieradzki, and Magdalena Durlik. 2020. "Urinary MicroRNA-21-5p as Potential Biomarker of Interstitial Fibrosis and Tubular Atrophy (IFTA) in Kidney Transplant Recipients" Diagnostics 10, no. 2: 113. https://doi.org/10.3390/diagnostics10020113