A Performance Comparison between Automated Deep Learning and Dental Professionals in Classification of Dental Implant Systems from Dental Imaging: A Multi-Center Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Classification of DISs
- Astra OsseoSpeed® TX (Dentsply IH AB, Molndal, Sweden), with a diameter of 4.5–5.0 mm and a length of 9–13 mm;
- Implantium® (Dentium, Seoul, Korea), with a diameter of 3.6–5.0 mm and a length of 8–12 mm;
- Superline® (Dentium, Seoul, Korea), with a diameter of 3.6–5.0 mm and a length of 8–12 mm;
- TSIII® (Osstem, Seoul, Korea), with a diameter of 3.5–5.0 mm and a length of 7–13 mm;
- SLActive® BL (Institut Straumann AG, Basel, Switzerland), with a diameter of 3.3–4.8 mm and a length of 8–12 mm;
- SLActive® BLT (Institut Straumann AG, Basel, Switzerland), with a diameter of 3.3–4.8 mm and a length of 8–12 mm.
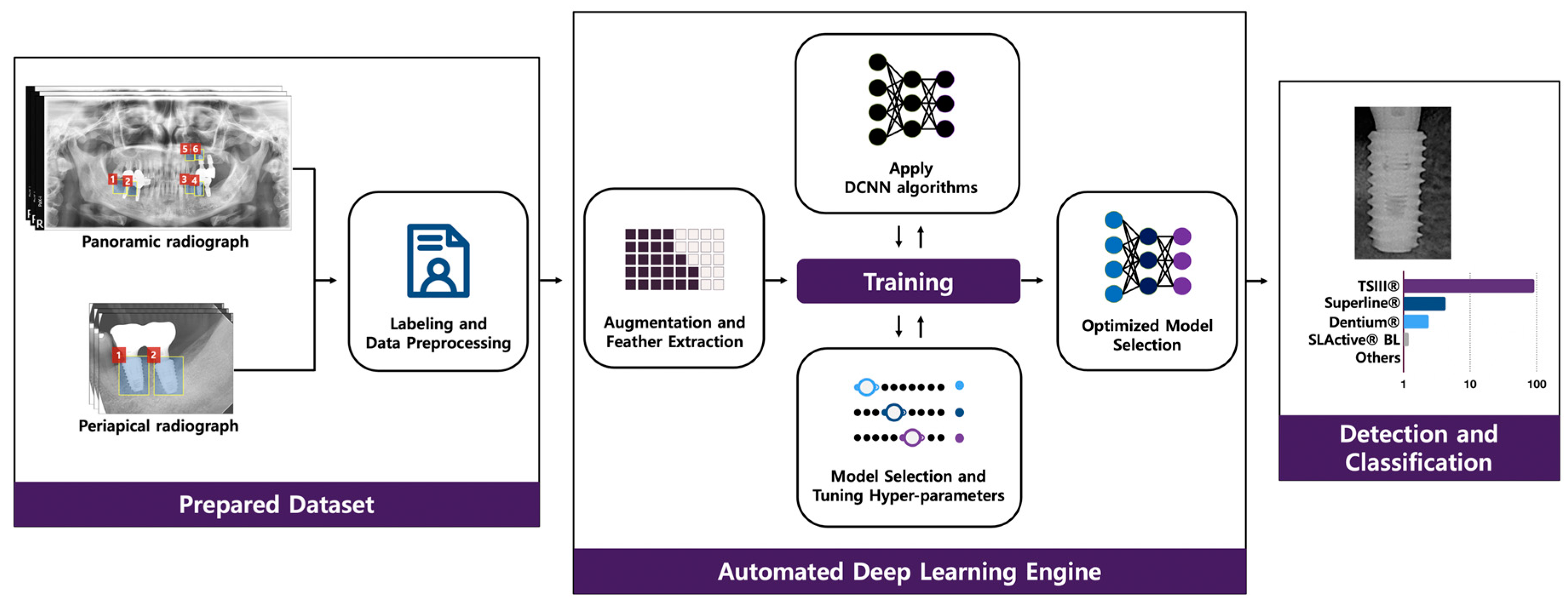
2.3. Data Preparation
2.4. Automated DCNN
2.5. Comparing the Performance of the Automated DCNN to that of Dental Professionals
2.6. Statistical Analysis
3. Results
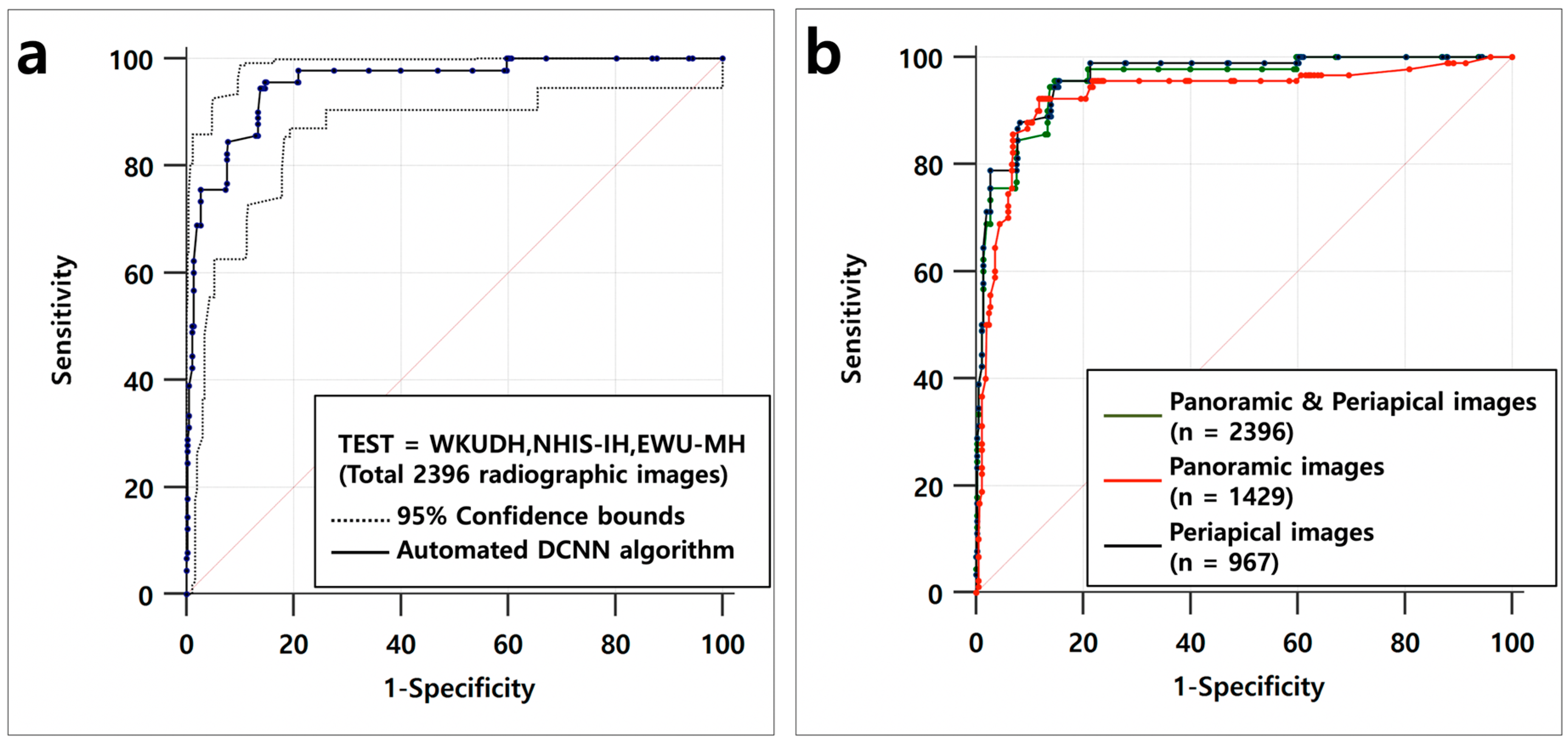
3.1. Outcomes of Automated DCNN on the Test Dataset
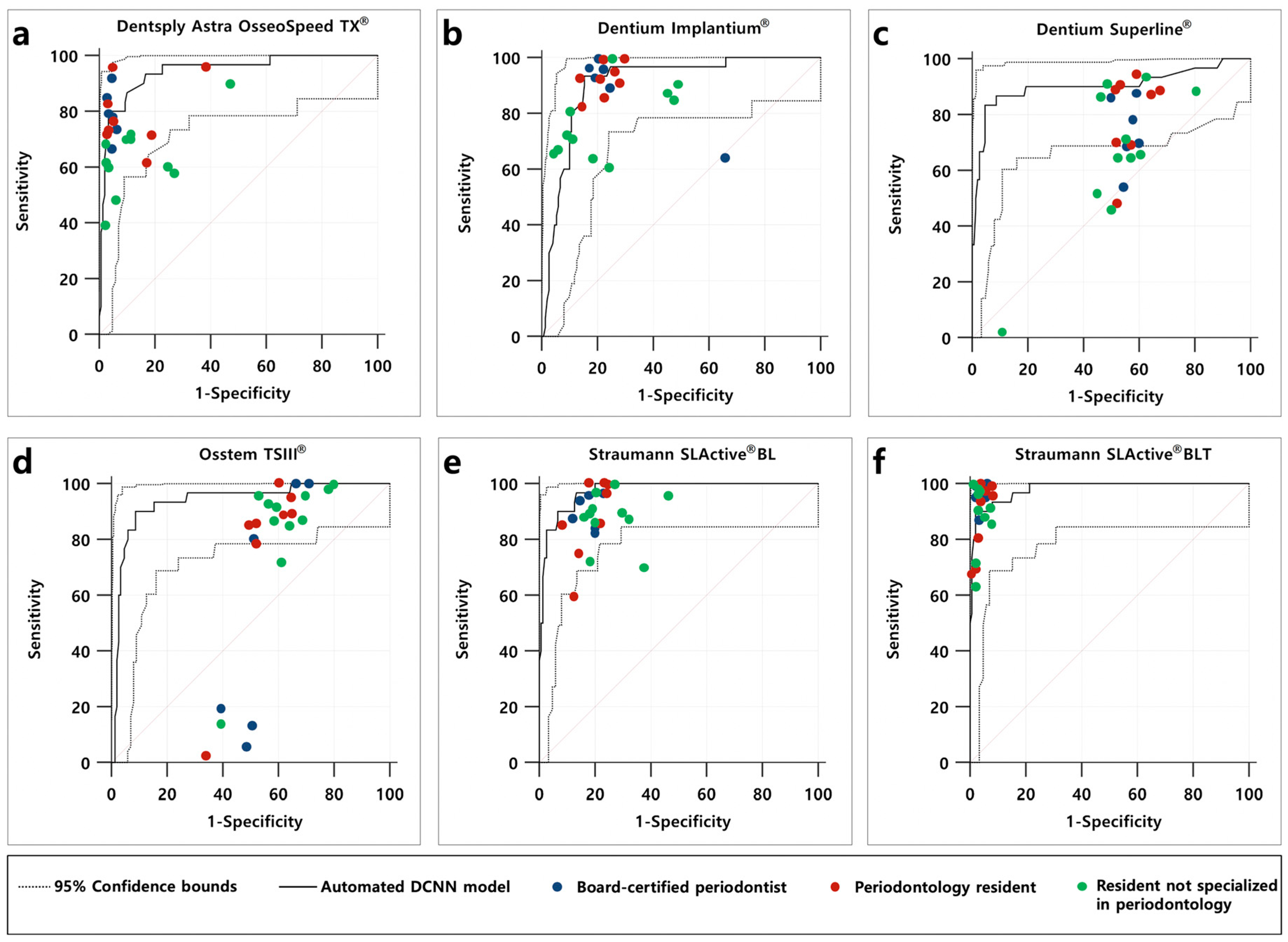
3.2. Outcomes for Automated DCNN Algorithm Compared to that of Dental Professionals
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Esposito, M.; Coulthard, P.; Thomsen, P.; Worthington, H.V. The role of implant surface modifications, shape and material on the success of osseointegrated dental implants. A cochrane systematic review. Eur. J. Prosthodont. Restor. Dent. 2005, 13, 15–31. [Google Scholar] [PubMed]
- Jokstad, A.; Braegger, U.; Brunski, J.B.; Carr, A.B.; Naert, I.; Wennerberg, A. Quality of dental implants. Int. Dent. J. 2003, 53, 409–443. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Ardebili, Y.; Worthington, H.V. Interventions for replacing missing teeth: Different types of dental implants. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Poubel, L.A.; Ferreira, V.F.; Barboza Edos, S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, M.; Meyer, S.; Mombelli, A.; Muller, F. Dental implants in the elderly population: A systematic review and meta-analysis. Clin. Oral Implants Res. 2017, 28, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Degidi, M.; Iezzi, G.; Petrone, G.; Piattelli, A. Correlation between implant stability quotient and bone-implant contact: A retrospective histological and histomorphometrical study of seven titanium implants retrieved from humans. Clin. Implant Dent. Relat. Res. 2006, 8, 218–222. [Google Scholar] [CrossRef]
- Jaarda, M.J.; Razzoog, M.E.; Gratton, D.G. Geometric comparison of five interchangeable implant prosthetic retaining screws. J. Prosthet. Dent. 1995, 74, 373–379. [Google Scholar] [CrossRef]
- Al-Wahadni, A.; Barakat, M.S.; Abu Afifeh, K.; Khader, Y. Dentists’ most common practices when selecting an implant system. J. Prosthodont. 2018, 27, 250–259. [Google Scholar] [CrossRef]
- Nuzzolese, E.; Lusito, S.; Solarino, B.; Di Vella, G. Radiographic dental implants recognition for geographic evaluation in human identification. J. Forensic Odontostomatol. 2008, 26, 8–11. [Google Scholar] [PubMed]
- Berketa, J.W.; Hirsch, R.S.; Higgins, D.; James, H. Radiographic recognition of dental implants as an aid to identifying the deceased. J. Forensic Sci. 2010, 55, 66–70. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Diagnosis and prediction of periodontally compromised teeth using a deep learning-based convolutional neural network algorithm. J. Periodontal Implant Sci. 2018, 48, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Detection and diagnosis of dental caries using a deep learning-based convolutional neural network algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N. Diagnosis of cystic lesions using panoramic and cone beam computed tomographic images based on deep learning neural network. Oral Dis. 2020, 26, 152–158. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine learning in medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Stead, W.W. Clinical implications and challenges of artificial intelligence and deep learning. JAMA 2018, 320, 1107–1108. [Google Scholar] [CrossRef]
- Faes, L.; Wagner, S.K.; Fu, D.J.; Liu, X.; Korot, E.; Ledsam, J.R.; Back, T.; Chopra, R.; Pontikos, N.; Kern, C.; et al. Automated deep learning design for medical image classification by health-care professionals with no coding experience: A feasibility study. Lancet Digit. Health 2019, 1, e232–e242. [Google Scholar] [CrossRef] [Green Version]
- Waring, J.; Lindvall, C.; Umeton, R. Automated machine learning: Review of the state-of-the-art and opportunities for healthcare. Artif. Intell. Med. 2020, 104, 101822. [Google Scholar] [CrossRef]
- Shin, H.C.; Roth, H.R.; Gao, M.; Lu, L.; Xu, Z.; Nogues, I.; Yao, J.; Mollura, D.; Summers, R.M. Deep convolutional neural networks for computer-aided detection: Cnn architectures, dataset characteristics and transfer learning. IEEE Trans. Med. Imaging 2016, 35, 1285–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahiwal, I.G.; Woody, R.D.; Benson, B.W.; Guillen, G.E. Radiographic identification of nonthreaded endosseous dental implants. J. Prosthet. Dent. 2002, 87, 552–562. [Google Scholar] [CrossRef] [Green Version]
- Michelinakis, G.; Sharrock, A.; Barclay, C.W. Identification of dental implants through the use of implant recognition software (irs). Int. Dent. J. 2006, 56, 203–208. [Google Scholar] [CrossRef]
- Kim, J.E.; Nam, N.E.; Shim, J.S.; Jung, Y.H.; Cho, B.H.; Hwang, J.J. Transfer learning via deep neural networks for implant fixture system classification using periapical radiographs. J. Clin. Med. 2020, 9, 1117. [Google Scholar] [CrossRef] [Green Version]
- Sukegawa, S.; Yoshii, K.; Hara, T.; Yamashita, K.; Nakano, K.; Yamamoto, N.; Nagatsuka, H.; Furuki, Y. Deep neural networks for dental implant system classification. Biomolecules 2020, 10, 984. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, S.N. Efficacy of deep convolutional neural network algorithm for the identification and classification of dental implant systems, using panoramic and periapical radiographs: A pilot study. Medicine (Baltimore) 2020, 99, e20787. [Google Scholar] [CrossRef] [PubMed]
- Anthonappa, R.P.; King, N.M.; Rabie, A.B.; Mallineni, S.K. Reliability of panoramic radiographs for identifying supernumerary teeth in children. Int. J. Paediatr. Dent. 2012, 22, 37–43. [Google Scholar] [CrossRef]
- Geibel, M.A.; Carstens, S.; Braisch, U.; Rahman, A.; Herz, M.; Jablonski-Momeni, A. Radiographic diagnosis of proximal caries-influence of experience and gender of the dental staff. Clin. Oral Investig. 2017, 21, 2761–2770. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Dataset | ||||||
|---|---|---|---|---|---|---|
| WKUDH | NHIS-IH | EWU-MH | ||||
| Dental Implant System | Panoramic images (n = 4989) | Periapical images (n = 3872) | Panoramic images (n = 1120) | Periapical images (n = 204) | Panoramic images (n = 1037) | Periapical images (n = 758) |
| Dentsply Astra OsseoSpeed TX® | 247 | 139 | 2 | - | - | - |
| Dentium Implantium® | 589 | 578 | 944 | 148 | 174 | 79 |
| Dentium Superline® | 1011 | 970 | 71 | 32 | 202 | 74 |
| Osstem TSIII® | 2788 | 1990 | 100 | 23 | 351 | 365 |
| Straumann SLActive® BL | 102 | 89 | 3 | 1 | 206 | 139 |
| Straumann SLActive® BLT | 252 | 106 | - | - | 104 | 101 |
| Difference between Areas | SE | 95% CI | p-Value | |
|---|---|---|---|---|
| Panoramic and periapical images vs. oeriapical images | 0.007 | 0.007 | −0.008–0.022 | 0.365 |
| Panoramic and periapical images vs. panoramic images | 0.025 | 0.021 | −0.016–0.067 | 0.235 |
| Panoramic images vs. oeriapical images | 0.032 | 0.020 | −0.006–0.072 | 0.106 |
| Variables | AUC | 95% CI | SE | Youden Index | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| Dentsply Astra OsseoSpeed TX® | ||||||
| Automated DCNN | 0.945 | 0.901–0.973 | 0.023 | 0.766 | 0.933 | 0.833 |
| Board-certified periodontists | 0.896 | 0.877–0.914 | 0.014 | 0.725 | 0.777 | 0.947 |
| Periodontology residents | 0.831 | 0.811–0.850 | 0.015 | 0.517 | 0.570 | 0.946 |
| Residents not specialized in periodontology | 0.777 | 0.758–0.795 | 0.014 | 0.425 | 0.493 | 0.931 |
| Dentium Implantium® | ||||||
| Automated DCNN | 0.908 | 0.856–0.946 | 0.026 | 0.780 | 0.933 | 0.847 |
| Board-certified periodontists | 0.791 | 0.766–0.815 | 0.013 | 0.733 | 0.966 | 0.766 |
| Periodontology residents | 0.806 | 0.785–0.826 | 0.011 | 0.682 | 0.912 | 0.770 |
| Residents not specialized in periodontology | 0.736 | 0.716–0.755 | 0.013 | 0.465 | 0.672 | 0.792 |
| Dentium Superline® | ||||||
| Automated DCNN | 0.903 | 0.850–0.942 | 0.041 | 0.786 | 0.833 | 0.954 |
| Board-certified periodontists | 0.537 | 0.507–0.567 | 0.016 | 0.333 | 0.778 | 0.588 |
| Periodontology residents | 0.534 | 0.508–0.560 | 0.015 | 0.330 | 0.945 | 0.384 |
| Residents not specialized in periodontology | 0.544 | 0.522–0.566 | 0.013 | 0.292 | 0.884 | 0.407 |
| Osstem TSIII® | ||||||
| Automated DCNN | 0.937 | 0.890–0.967 | 0.024 | 0.813 | 0.900 | 0.913 |
| Board-certified periodontists | 0.501 | 0.471–0.532 | 0.018 | 0.298 | 0.911 | 0.387 |
| Periodontology residents | 0.503 | 0.477–0.529 | 0.016 | 0.270 | 0.104 | 0.625 |
| Residents not specialized in periodontology | 0.556 | 0.534–0.578 | 0.014 | 0.215 | 0.821 | 0.394 |
| Straumann SLActive® BL | ||||||
| Automated DCNN | 0.974 | 0.938–0.992 | 0.010 | 0.833 | 0.967 | 0.867 |
| Board-certified periodontists | 0.759 | 0.732–0.784 | 0.015 | 0.661 | 0.888 | 0.772 |
| Periodontology residents | 0.753 | 0.730–0.775 | 0.014 | 0.650 | 0.870 | 0.779 |
| Residents not specialized in periodontology | 0.698 | 0.677–0.718 | 0.012 | 0.507 | 0.781 | 0.726 |
| Straumann SLActive® BLT | ||||||
| Automated DCNN | 0.981 | 0.949–0.996 | 0.009 | 0.880 | 0.900 | 0.980 |
| Board-certified periodontists | 0.968 | 0.955–0.977 | 0.011 | 0.951 | 0.955 | 0.995 |
| Periodontology residents | 0.915 | 0.899–0.929 | 0.014 | 0.851 | 0.866 | 0.985 |
| Residents not specialized in periodontology | 0.915 | 0.902–0.927 | 0.011 | 0.852 | 0.887 | 0.964 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-H.; Kim, Y.-T.; Lee, J.-B.; Jeong, S.-N. A Performance Comparison between Automated Deep Learning and Dental Professionals in Classification of Dental Implant Systems from Dental Imaging: A Multi-Center Study. Diagnostics 2020, 10, 910. https://doi.org/10.3390/diagnostics10110910
Lee J-H, Kim Y-T, Lee J-B, Jeong S-N. A Performance Comparison between Automated Deep Learning and Dental Professionals in Classification of Dental Implant Systems from Dental Imaging: A Multi-Center Study. Diagnostics. 2020; 10(11):910. https://doi.org/10.3390/diagnostics10110910
Chicago/Turabian StyleLee, Jae-Hong, Young-Taek Kim, Jong-Bin Lee, and Seong-Nyum Jeong. 2020. "A Performance Comparison between Automated Deep Learning and Dental Professionals in Classification of Dental Implant Systems from Dental Imaging: A Multi-Center Study" Diagnostics 10, no. 11: 910. https://doi.org/10.3390/diagnostics10110910