Hybrid Operating Room System for the Treatment of Thoracic and Abdominal Aortic Aneurysms: Evaluation of the Radiation Dose Received by Patients

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Features of the HORS
2.2. Statistics
3. Results
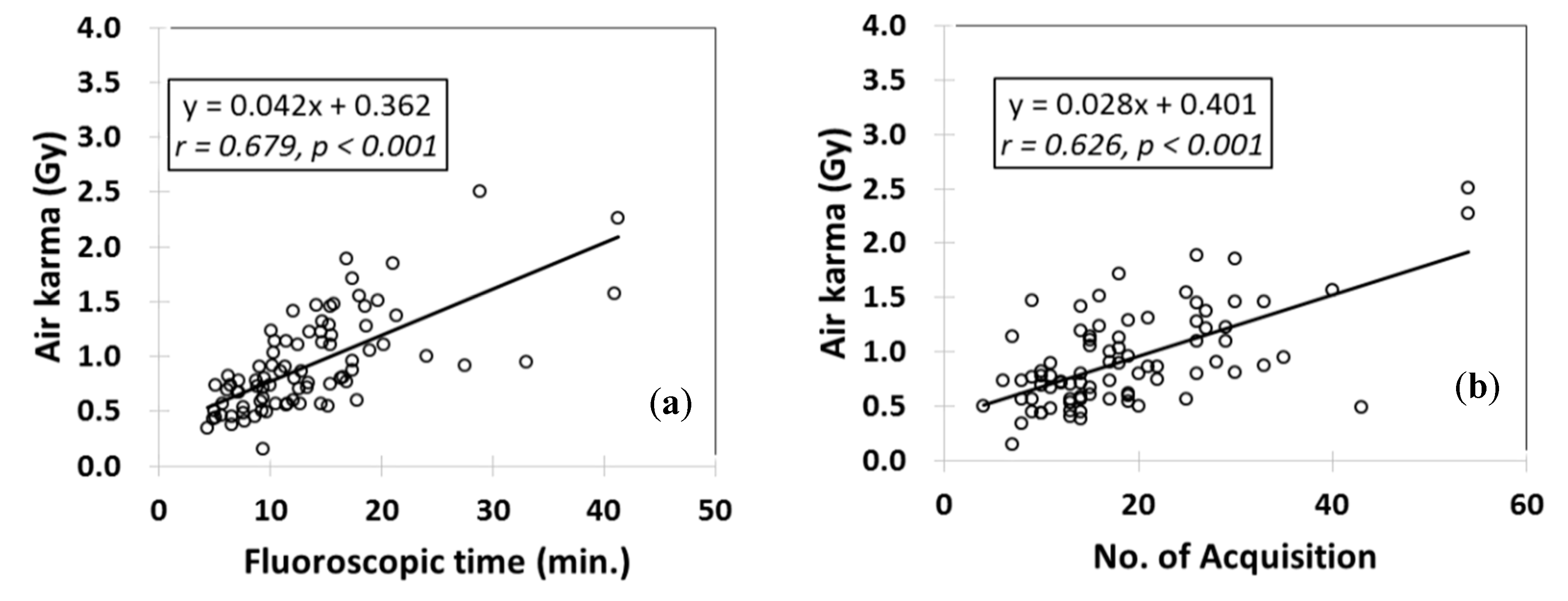
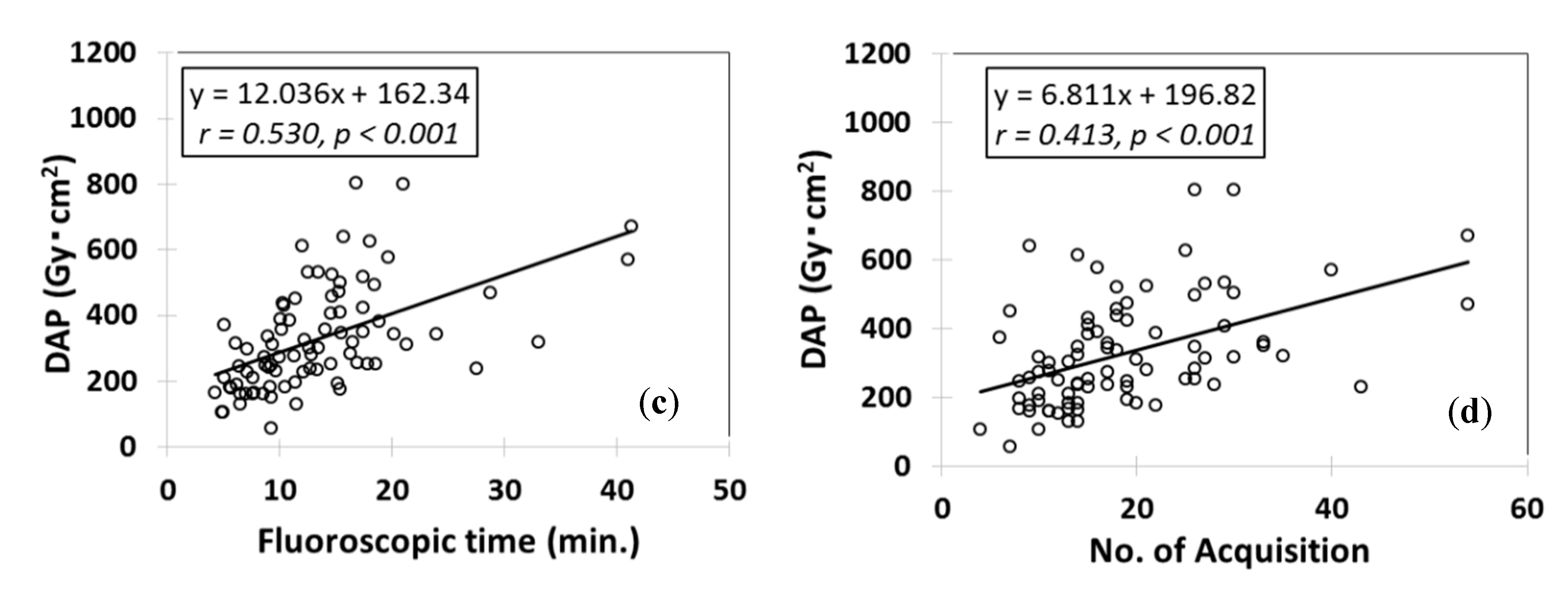
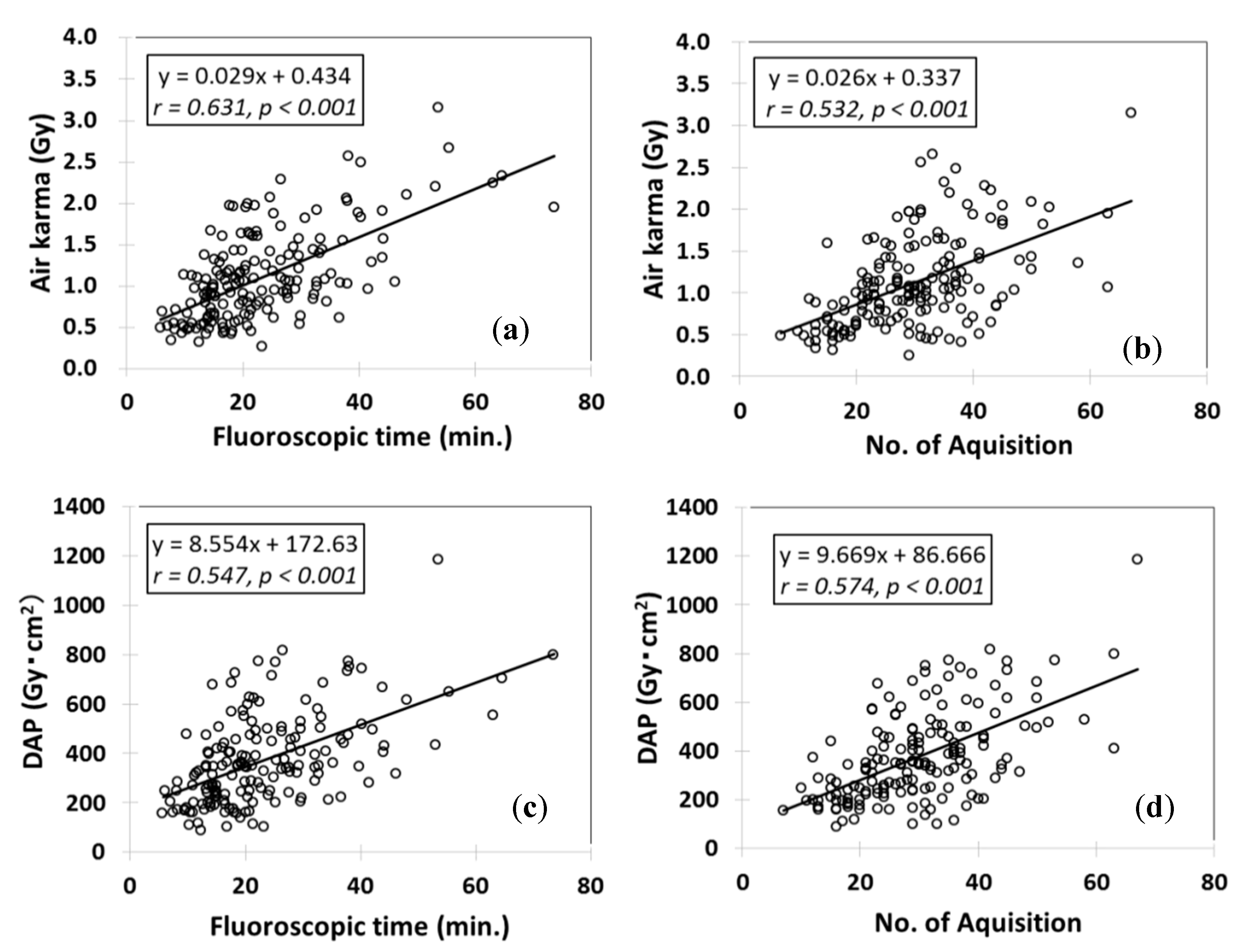
3.1. Radiation Doses Associated with TEVAR and EVAR
3.2. TEVAR and EVAR (Literature Review) [1,2,9,10,15,16,17,18,19,22,26,27,28]
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blaszak, M.A.; Majewska, N.; Juszkat, R.; Majewski, W. Dose-area product to patients during stent-graft treatment of thoracic and abdominal aortic aneurysms. Health Phys. 2009, 97, 206–211. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.M.; Scali, S.T.; Feezor, R.J.; Neal, D.; Huber, T.S.; Beck, A.W. Three-dimensional fusion computed tomography decreases radiation exposure, procedure time, and contrast use during fenestrated endovascular aortic repair. J. Vasc. Surg. 2015, 61, 309–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chida, K.; Kaga, Y.; Haga, Y.; Kataoka, N.; Kumasaka, E.; Meguro, T.; Zuguchi, M. Occupational Dose in Interventional Radiology Procedures. Am. J. Roentgenol. 2013, 200, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Attigah, N.; Oikonomou, K.; Hinz, U.; Knoch, T.; Demirel, S.; Verhoeven, E.; Böckler, D. Radiation exposure to eye lens and operator hands during endovascular procedures in hybrid operating rooms. J. Vasc. Surg. 2016, 63, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.P.; Miller, D.L.; Balter, S.; Kleinerman, R.A.; Linet, M.S.; Kwon, D.; Simon, S.L. Occupational radiation doses to operators performing cardiac catheterization procedures. Health Phys. 2008, 94, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chida, K.; Kobayashi, R.; Haga, Y.; Zuguchi, M. Radiation dose of cardiac IVR x-ray systems: A comparison of present and past. Acta Cardiol. 2015, 70, 299–306. [Google Scholar] [CrossRef]
- Haga, Y.; Chida, K.; Inaba, Y.; Kaga, Y.; Meguro, T.; Zuguchi, M. A Rotatable Quality Control Phantom for Evaluating the Performance of Flat Panel Detectors in Imaging Moving Objects. J. Digit. Imaging 2015, 29, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Chida, K.; Kaga, Y.; Haga, Y.; Takeda, K.; Zuguchi, M. Quality Control Phantom for Flat Panel Detector X-ray Systems. Health Phys. 2013, 104, 97–101. [Google Scholar] [CrossRef]
- Hertault, A.; Maurel, B.; Sobocinski, J.; Gonzalez, T.M.; Le Roux, M.; Azzaoui, R.; Midulla, M.; Haulon, S. Impact of Hybrid Rooms with Image Fusion on Radiation Exposure during Endovascular Aortic Repair. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 382–390. [Google Scholar] [CrossRef] [Green Version]
- Haak, R.V.D.; Hamans, B.; Zuurmond, K.; Verhoeven, B.; Koning, O.H. Significant Radiation Dose Reduction in the Hybrid Operating Room Using a Novel X-ray Imaging Technology. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 480–486. [Google Scholar] [CrossRef] [Green Version]
- Chida, K.; Inaba, Y.; Masuyama, H.; Yanagawa, I.; Mori, I.; Saito, H.; Maruoka, S.; Zuguchi, M. Evaluating the performance of a MOSFET dosimeter at diagnostic X-ray energies for interventional radiology. Radiol. Phys. Technol. 2009, 2, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Inaba, Y.; Kobayashi, R.; Nakamura, M.; Abe, Y.; Zuguchi, M. Real-time patient radiation dosimeter for use in interventional radiology. Phys. Medica 2016, 32, 1475–1478. [Google Scholar] [CrossRef] [PubMed]
- Kuhelj, D.; Zdesar, U.; Jevtić, V.; Škrk, D.; Omahen, G.; Zontar, D.; Surlan, M.; Glusic, M.; Popović, P.; Kocijančič, I.J.; et al. Risk of deterministic effects during endovascular aortic stent graft implantation. Br. J. Radiol. 2010, 83, 958–963. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, D.J.; Pipinos, I.I.; Longo, G.M.; Lynch, T.G.; Rutar, F.J.; Johanning, J.M. Direct and Indirect Measurement of Patient Radiation Exposure during Endovascular Aortic Aneurysm Repair. Ann. Vasc. Surg. 2008, 22, 723–729. [Google Scholar] [CrossRef]
- Panuccio, G.; Greenberg, R.K.; Wunderle, K.; Mastracci, T.M.; Eagleton, M.G.; Davros, W. Comparison of indirect radiation dose estimates with directly measured radiation dose for patients and opetators during complex endovascular procedures. J Vasc. Surg. 2011, 53, 885–894. [Google Scholar] [CrossRef] [Green Version]
- Zoli, S.; Trabattoni, P.; Dainese, L.; Annoni, A.D.; Saccu, C.; Fumagalli, M.; Spirito, R.; Biglioli, P. Cumulative radiation exposure during thoracic endovascular aneurysm repair and subsequent follow-up. Eur. J. Cardio-Thorac. Surg. 2012, 42, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Mohapatra, A.; Greenberg, R.K.; Mastracci, T.M.; Eagleton, M.J.; Thornsberry, B. Radiation exposure to operating room personnel and patients during endovascular procedures. J. Vasc. Surg. 2013, 58, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Kirkwood, M.L.; Arbique, G.M.; Guild, J.B.; Timaran, C.; Chung, J.; Anderson, J.A.; Valentine, R.J. Surgeon education decreases radiation dose in complex endovascular procedures and improves patient safety. J. Vasc. Surg. 2013, 58, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Majewska, N.; Stanisic, M.G.; Blaszak, M.A.; Juszkat, R.; Frankiewicz, M.; Krasiński, Z.; Makalowski, M.; Majewski, W. Clinical factors increasing radiation doses to patients undergoing long-lasting procedures: Abdominal stent-graft implantation. Med. Sci. Monit. 2011, 17, MT97–MT103. [Google Scholar] [CrossRef] [Green Version]
- Weerakkody, R.A.; Walsh, S.; Cousins, C.; Goldstone, K.E.; Tang, T.Y.; Gaunt, M.E. Radiation exposure during endovascular aneurysm repair. BJS 2008, 95, 699–702. [Google Scholar] [CrossRef]
- De Ruiter, Q.M.B.; Reitsma, J.B.; Moll, F.L.; Van Herwaarden, J.A. Meta-analysis of Cumulative Radiation Duration and Dose During EVAR Using Mobile, Fixed, or Fixed/3D Fusion C-Arms. J. Endovasc. Ther. 2016, 23, 944–956. [Google Scholar] [CrossRef] [PubMed]
- Varu, V.; Greenberg, J.; Lee, J. Improved Efficiency and Safety for EVAR with Utilization of a Hybrid Room. Eur. J. Vasc. Endovasc. Surg. 2013, 46, 675–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monastiriotis, S.; Comito, M.; Labropoulos, N. Radiation exposure in endovascular repair of abdominal and thoracic aortic aneurysms. J. Vasc. Surg. 2015, 62, 753–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauer, L.T.; Thornton, R.H.; Hay, J.L.; Balter, R.; Williamson, M.J.; Germain, J.S. Fears, Feelings, and Facts: Interactively Communicating Benefits and Risks of Medical Radiation with Patients. Am. J. Roentgenol. 2011, 196, 756–761. [Google Scholar] [CrossRef] [Green Version]
- Rolls, A.; Rosen, S.; Constantinou, J.; Davis, M.; Cole, J.; Desai, M.; Stoyanov, D.; Mastracci, T. Introduction of a Team Based Approach to Radiation Dose Reduction in the Enhancement of the Overall Radiation Safety Profile of FEVAR. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Tacher, V.; Lin, M.; Desgranges, P.; Deux, J.-F.; Grünhagen, T.; Becquemin, J.-P.; Luciani, A.; Rahmouni, A.; Kobeiter, H. Image Guidance for Endovascular Repair of Complex Aortic Aneurysms: Comparison of Two-dimensional and Three-dimensional Angiography and Image Fusion. J. Vasc. Interv. Radiol. 2013, 24, 1698–1706. [Google Scholar] [CrossRef] [Green Version]
- Panuccio, G.; Bisdas, T.; Berekoven, B.; Torsello, G.; Austermann, M. Performance of Bridging Stent Grafts in Fenestrated and Branched Aortic Endografting. Eur. J. Vasc. Endovasc. Surg. 2015, 50, 60–70. [Google Scholar] [CrossRef] [Green Version]
- Sailer, A.M.; Schurink, G.W.H.; Bol, M.E.; De Haan, M.W.; Van Zwam, W.H.; Wildberger, J.E.; Jeukens, C. Occupational Radiation Exposure During Endovascular Aortic Repair. Cardiovasc. Interv. Radiol. 2014, 38, 827–832. [Google Scholar] [CrossRef]
- Chida, K.; Saito, H.; Zuguchi, M.; Shirotori, K.; Kumagai, S.; Nakayama, H.; Matsubara, K.; Kohzuki, M. Does Digital Acquisition Reduce Patients’ Skin Dose in Cardiac Interventional Procedures? An Experimental Study. Am. J. Roentgenol. 2004, 183, 1111–1114. [Google Scholar] [CrossRef]
- Chida, K.; Saito, H.; Otani, H.; Kohzuki, M.; Takahashi, S.; Yamada, S.; Shirato, K.; Zuguchi, M. Relationship Between Fluoroscopic Time, Dose–Area Product, Body Weight, and Maximum Radiation Skin Dose in Cardiac Interventional Procedures. Am. J. Roentgenol. 2006, 186, 774–778. [Google Scholar] [CrossRef]
- Chida, K.; Kagaya, Y.; Saito, H.; Takai, Y.; Takahashi, S.; Yamada, S.; Kohzuki, M.; Zuguchi, M. Total Entrance Skin Dose: An Effective Indicator of Maximum Radiation Dose to the Skin During Percutaneous Coronary Intervention. Am. J. Roentgenol. 2007, 189, 224–227. [Google Scholar] [CrossRef]
- Chida, K.; Inaba, Y.; Saito, H.; Ishibashi, T.; Takahashi, S.; Kohzuki, M.; Zuguchi, M. Radiation Dose of Interventional Radiology System Using a Flat-Panel Detector. Am. J. Roentgenol. 2009, 193, 1680–1685. [Google Scholar] [CrossRef]
- Chida, K.; Ohno, T.; Kakizaki, S.; Takegawa, M.; Yuuki, H.; Nakada, M.; Takahashi, S.; Zuguchi, M. Radiation Dose to the Pediatric Cardiac Catheterization and Intervention Patient. Am. J. Roentgenol. 2010, 195, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Haga, Y.; Chida, K.; Kaga, Y.; Sota, M.; Meguro, T.; Zuguchi, M. Occupational eye dose in interventional cardiology procedures. Sci. Rep. 2017, 7, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chida, K.; Inaba, Y.; Morishima, Y.; Taura, M.; Ebata, A.; Yanagawa, I.; Takeda, K.; Zuguchi, M. Comparison of dose at an interventional reference point between the displayed estimated value and measured value. Radiol. Phys. Technol. 2011, 4, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Morishima, Y.; Chida, K.; Watanabe, H. Estimation of the Dose of Radiation Received by Patient and Physician During a Videofluoroscopic Swallowing Study. Dysphagia 2016, 31, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Nakamura, M.; Chida, K.; Zuguchi, M. Effectiveness of a novel real-time dosimeter in interventional radiology: A comparison of new and old radiation sensors. Radiol. Phys. Technol. 2018, 11, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Nakamura, M.; Zuguchi, M.; Chida, K. Development of Novel Real-Time Radiation Systems Using 4-Channel Sensors. Sensors 2020, 20, 2741. [Google Scholar] [CrossRef]
- Kato, M.; Chida, K.; Nakamura, M.; Toyoshima, H.; Terata, K.; Abe, Y. New real-time patient radiation dosimeter for use in radiofrequency catheter ablation. J. Radiat. Res. 2019, 60, 215–220. [Google Scholar] [CrossRef] [Green Version]
- Kawauchi, S.; Chida, K.; Moritake, T.; Matsumaru, Y.; Hamada, Y.; Sakuma, H.; Yoda, S.; Sun, L.; Sato, M.; Tsuruta, W. Estimation of patient lens dose associated with c-arm cone-beam computed tomography usage during interventional neuroradiology. Radiat. Prot. Dosim. 2018, 184, 138–147. [Google Scholar] [CrossRef]
- Nemoto, M.; Chida, K. Reducing the Breast Cancer Risk and Radiation Dose of Radiography for Scoliosis in Children: A Phantom Study. Diagnostics 2020, 10, 753. [Google Scholar] [CrossRef] [PubMed]
- Chida, K.; Kato, M.; Kagaya, Y.; Zuguchi, M.; Saito, H.; Ishibashi, T.; Takahashi, S.; Yamada, S.; Takai, Y. Radiation dose and radiation protection for patients and physicians during interventional procedure. J. Radiat. Res. 2010, 51, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentin, J. Abstract: Avoidance of radiation injuries from medical interventional procedures, ICRP Publication 85. Ann. ICRP 2000, 30, 7. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| X-ray Conditions | Fluoroscopy | D A | D S A |
|---|---|---|---|
| Typical tube voltage (kV) | 80 | 80 | 80 |
| Typical tube current (mA) | 50 | 400 | 125 |
| Typical pulse widths (ms) | 6 | 8 | 45 |
| Pulse rate (p/s) | 7.5 | 10 | 10 |
| Additional filter | 0.2mm Cu | 0.3mm Cu | 1.5mm Al |
| Contrast Conditions | |||
| Injection method | — | Manual injection | Automatic injection |
| Flow rate (mL/sec) | — | ≈ 0.2 | 10 |
| Injection volume (mL) | — | ≈ 5 | 20 |
| Contrast agent | — | Iopamidol | Iopamidol |
| Iodine content (mg/mL) | — | 370 | 370 |
| Cu: Copper, Al: Aluminum | |||
| Aneurysm Types of TEVAR | No. of Cases n = 84 | Ratio (%) |
|---|---|---|
| Zone 0 | 27 | 32% |
| Zone 1 | 11 | 13% |
| Zone 2 | 15 | 18% |
| Zones 3–4 | 31 | 37% |
| Aneurysm types of EVAR | n = 172 | |
| infrarenal AAA | 172 | 100% |
| TEVAR | EVAR | p-Value (TEVAR vs. EVAR) | |
|---|---|---|---|
| No. of Cases | 84 | 172 | |
| Age (years) | 69.8 ± 10.8 | 73.8 ± 9.4 | p < 0.01 |
| Male-to-female ratio | 72:12 | 147:25 | n. s. |
| Height (cm) | 163.2 ± 8.8 | 162.3 ± 7.9 | n. s. |
| Weight (kg) | 64.4 ± 10.5 | 62.1 ± 10.2 | n. s. |
| FT (min.) | 13.4 ± 7.1 | 23.2 ± 11.7 | p < 0.01 |
| AK (Gy) | 0.92 ± 0.44 | 1.11 ± 0.54 | p < 0.01 |
| DAP (Gy·cm2) | 323.7 ± 161.0 | 371.3 ± 186.0 | p < 0.05 |
| No. of acquisitions | 18.7 ± 9.8 | 29.8 ± 11.0 | p < 0.01 |
| No. of stents | 1.81 ± 0.65 | 2.49 ± 0.81 | p < 0.01 |
| Study of TEVAR | No. of Cases | Median FT (min.) | Median AK (Gy) | Median DAP (Gy·cm2) |
|---|---|---|---|---|
| Blaszak M A. [1], 2009 | 39 | 11.8 (13.4 ± 8.3) | 0.87 (0.94 ± 0.56) | 385.9 (452.3 ± 275.4) |
| Hertault A. [9], 2014 | 14 | 0.9 (—) | — | 26.0 (—) |
| Panuccio G. [15], 2011 | 46 | 82.7 (111.3 ± 55.1) | 6.30 (12.7 ± 4.4) | 696.6 (1327.0 ± 469.9) |
| Zoli S. [16], 2012 | 48 | 12.3 (15.7 ± 11.4) | — | 41.3 (56.7 ± 45.2) |
| Mohapatra A. [17], 2013 | 39 | — (71.1) | — (7.0) | — (540.9) |
| Kirkwood M.L. [18], 2013 | 25 | — | 0.9 (—) | — |
| Sailer A.M. [28], 2015 | 11 | — (9.7 ± 7.3) | — | — (62.0 ± 46.0) |
| Our study | 84 | 12.1 (13.4 ± 7.1) | 0.80 (0.92 ± 0.44) | 299.7 (323.7 ± 161.0) |
| Study of EVAR | No. of Cases | Median FT (min.) | Median AK (Gy) | Median DAP (Gy·cm2) |
|---|---|---|---|---|
| Blaszak M.A. [1], 2009 | 39 | 19.6 (22.8 ± 14.2) | 1.11 (1.12 ± 0.70) | 354.9 (380.9 ± 285.3) |
| Hertault A. [9], 2014 | 44 | 10.6 (—) | — | 12.2 (—) |
| Van den Haak R.F. [10], 2015 | 18 | — (13.6 ± 8.6) | 1.26 (—) | 224.4 (—) |
| 19 | — (13.1 ± 6.1) | 0.56 (—) | 95.8 (—) | |
| McNally M.M. [2], 2015 | 41 | — (84.0 ± 36.0) | — (5.00 ± 0.28) | — |
| 31 | — (55.0 ± 21.0) | — (2.30 ± 1.30) | — | |
| Kirkwood M.L. [18], 2013 | 22 | — | 1.00 (—) | — |
| Majewska N. [19], 2011 | 92 | 13 (16.3) | 0.63 (0.80) | 456 (626) |
| Varu VN. [22], 2013 | 51 | — (24.9 ± 12.4) | — | — |
| Tacher V. [26], 2013 | 9 | — (82.0 ± 46.0) | — | — (1188.0 ± 1067.0) |
| 14 | — (42.0 ± 22.0) | — | — (984.0 ± 581.0) | |
| 14 | — (80.0 ± 36.0) | — | — (656.0 ± 457.0) | |
| Panuccio G. [27], 2015 | 150 | — (89.0 ± 33.0) | — | — (60.7 ± 84.9) |
| Sailer A.M. [28], 2015 | 22 | — (19.8 ± 8.4) | — | — (116.0 ± 122.0) |
| 11 | — (49.1± 21.8) | — | — (217.0 ± 159.0) | |
| Our study | 172 | 20.5 (23.2 ± 11.7) | 1.02 (1.11 ± 0.54) | 345.3 (371.3 ± 186.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haga, Y.; Chida, K.; Sota, M.; Kaga, Y.; Abe, M.; Inaba, Y.; Suzuki, M.; Meguro, T.; Zuguchi, M. Hybrid Operating Room System for the Treatment of Thoracic and Abdominal Aortic Aneurysms: Evaluation of the Radiation Dose Received by Patients. Diagnostics 2020, 10, 846. https://doi.org/10.3390/diagnostics10100846
Haga Y, Chida K, Sota M, Kaga Y, Abe M, Inaba Y, Suzuki M, Meguro T, Zuguchi M. Hybrid Operating Room System for the Treatment of Thoracic and Abdominal Aortic Aneurysms: Evaluation of the Radiation Dose Received by Patients. Diagnostics. 2020; 10(10):846. https://doi.org/10.3390/diagnostics10100846
Chicago/Turabian StyleHaga, Yoshihiro, Koichi Chida, Masahiro Sota, Yuji Kaga, Mitsuya Abe, Yohei Inaba, Masatoshi Suzuki, Taiichiro Meguro, and Masayuki Zuguchi. 2020. "Hybrid Operating Room System for the Treatment of Thoracic and Abdominal Aortic Aneurysms: Evaluation of the Radiation Dose Received by Patients" Diagnostics 10, no. 10: 846. https://doi.org/10.3390/diagnostics10100846