A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurement Protocol
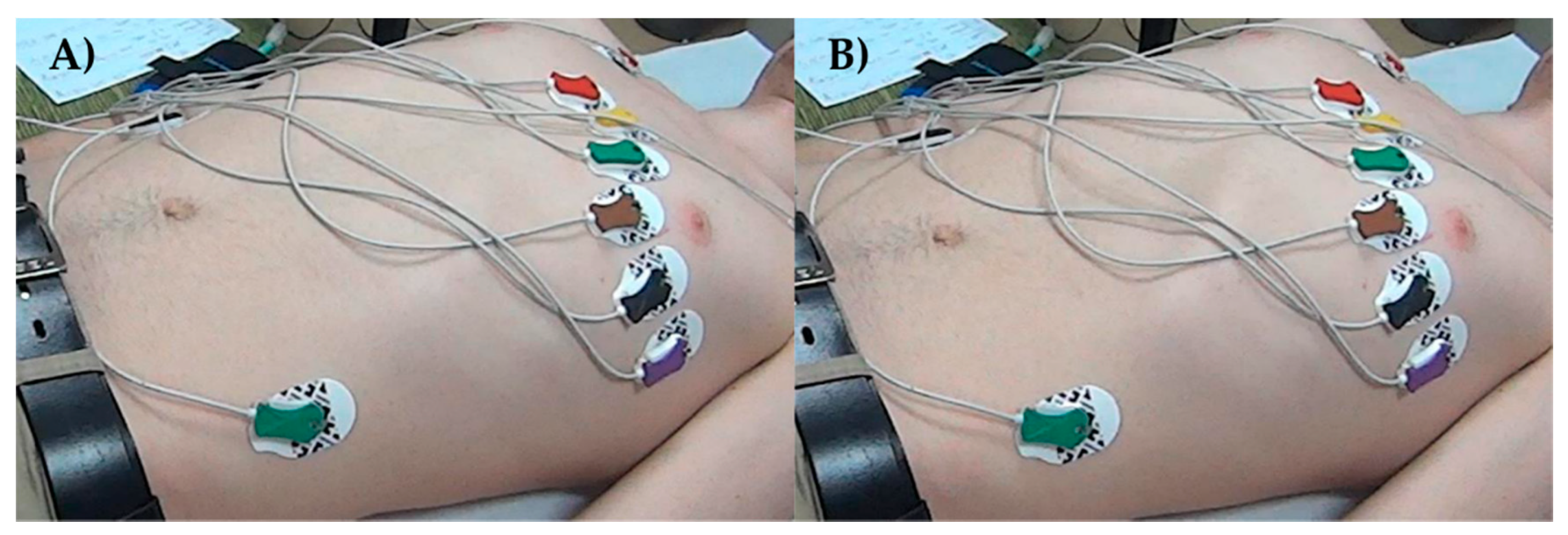
2.3. Electrocardiography (ECG) Acquisition
2.4. Respiratory Rate
2.5. HRV Analysis
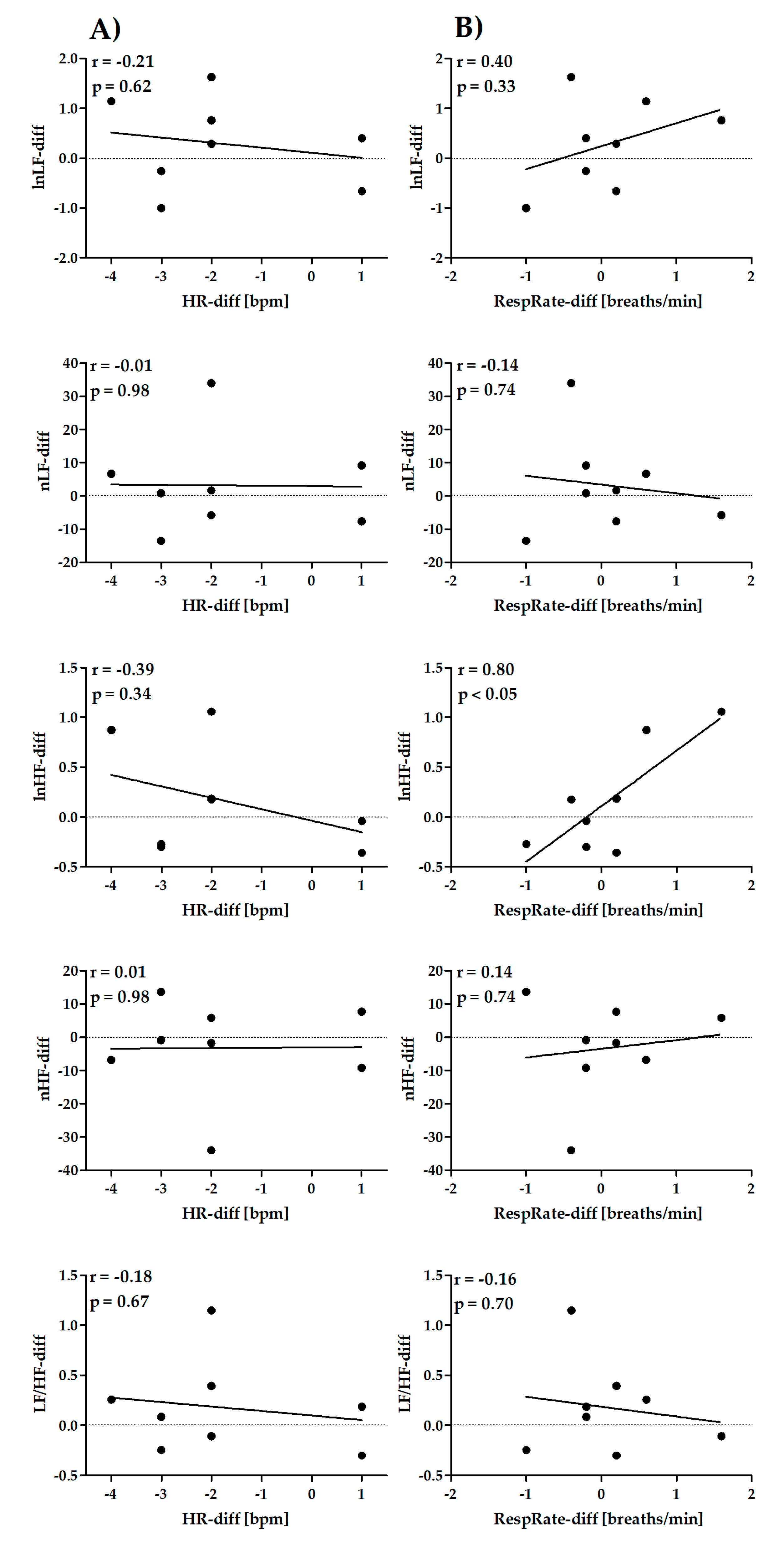
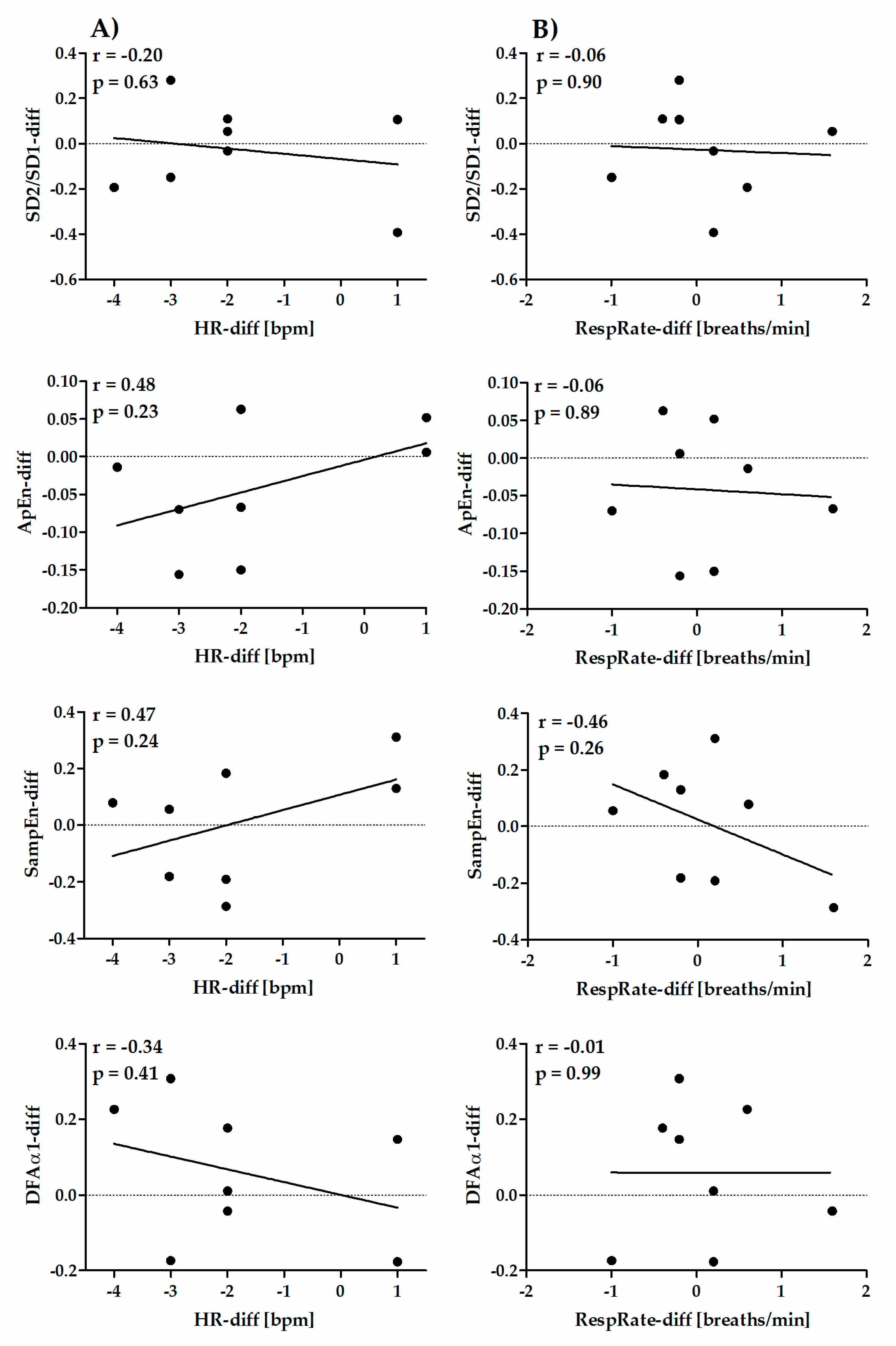
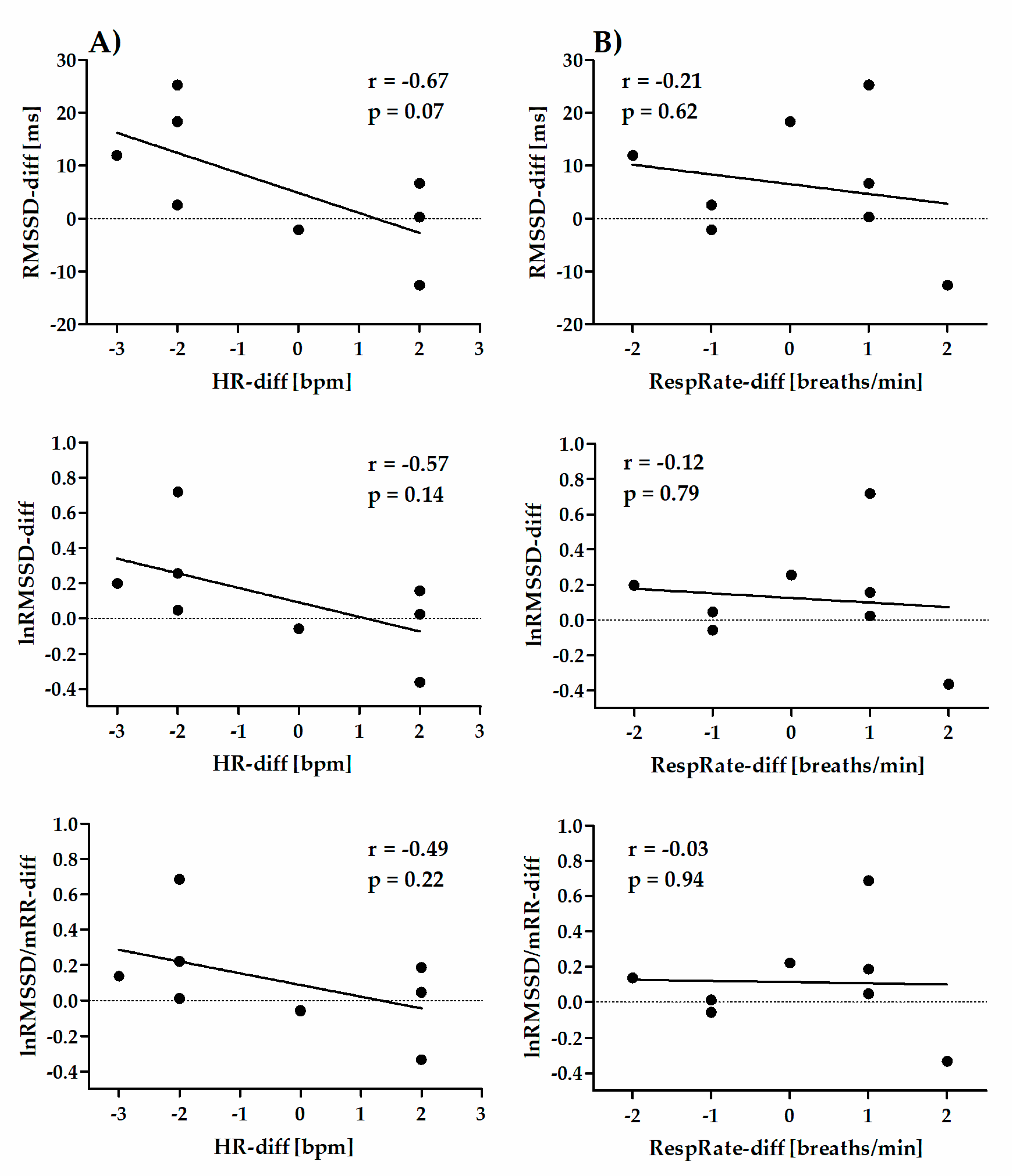
2.6. Relationships between Differences in HR and RespRate and Differences in HRV Parameters
2.7. Statistical Analysis
2.7.1. Reliability Statistics
2.7.2. Agreement Statistics
3. Results
3.1. Participants
3.2. Reliability of Short-Term (5 min) HR, RespRate and HRV Parameters
3.3. Reliability of Ultra-Short-Term (1 min) HR, RespRate, RMSSD, lnRMSSD and lnRMSSD/mRR
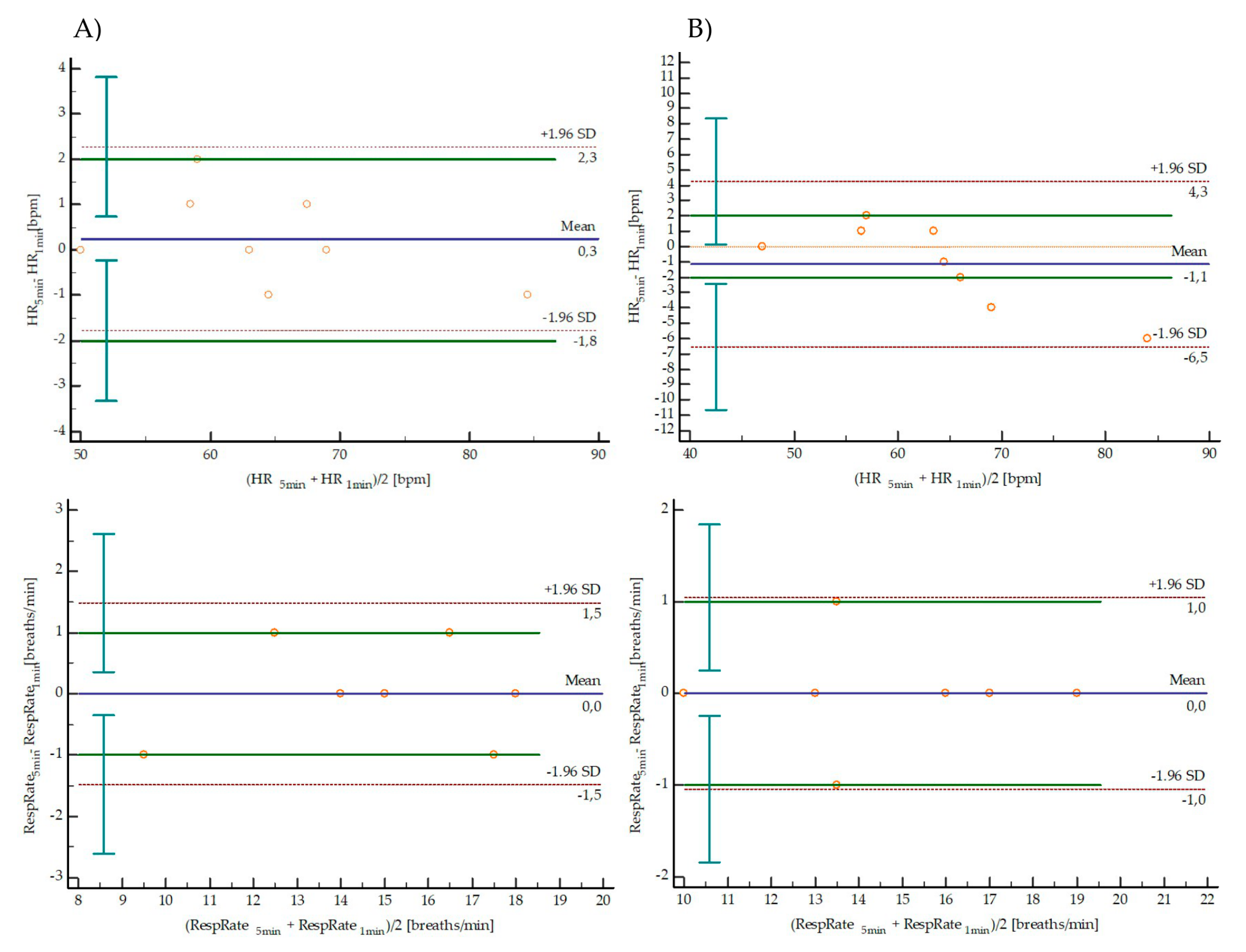
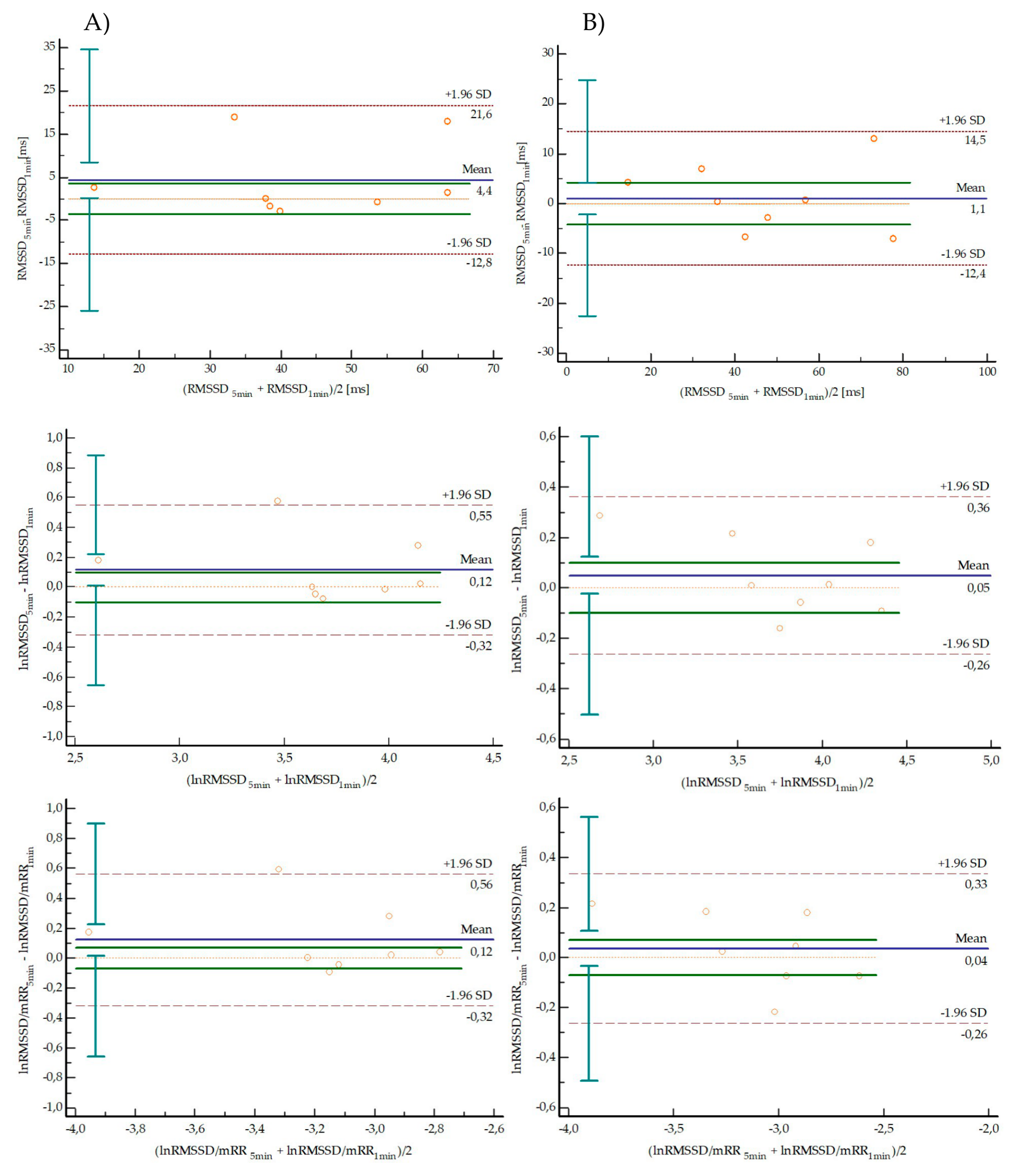
3.4. Agreement between Short-Term and Ultra-Short-Term Parameters
3.5. Correlation between Differences in HR or RespRate and Differences in HRV Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Meeusen, R.; Duclos, M.; Foster, C.; Fry, A.; Gleeson, M.; Nieman, D.; Raglin, J.; Rietjens, G.; Steinacker, J.; Urhausen, A.; et al. Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med. Sci. Sports Exerc. 2013, 45, 186–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellenger, C.R.; Fuller, J.T.; Thomson, R.L.; Davison, K.; Robertson, E.Y.; Buckley, J.D. Monitoring Athletic Training Status Through Autonomic Heart Rate Regulation: A Systematic Review and Meta-Analysis. Sports Med. 2016, 46, 1461–1486. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M.; Bertollo, M.; Bosquet, L.; Brink, M.; Coutts, A.J.; Duffield, R.; Erlacher, D.; Halson, S.L.; Hecksteden, A.; Heidari, J.; et al. Recovery and Performance in Sport: Consensus Statement. Int. J. Sports Physiol. Perform. 2018, 13, 240–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.; Hanakam, F.; Wiewelhove, T.; Döweling, A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Heart Rate Monitoring in Team Sports-A Conceptual Framework for Contextualizing Heart Rate Measures for Training and Recovery Prescription. Front. Physiol. 2018, 9, 639. [Google Scholar] [CrossRef] [Green Version]
- Młyńczak, M.; Krysztofiak, H. Cardiorespiratory Temporal Causal Links and the Differences by Sport or Lack Thereof. Front. Physiol. 2019, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Młyńczak, M.; Krysztofiak, H. Discovery of Causal Paths in Cardiorespiratory Parameters: A Time-Independent Approach in Elite Athletes. Front. Physiol. 2018, 9, 1455. [Google Scholar] [CrossRef] [Green Version]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring Athlete Training Loads: Consensus Statement. Int. J. Sports Physiol. Perform. 2017, 12, S2161–S2170. [Google Scholar] [CrossRef]
- Gabbett, T.J.; Nassis, G.P.; Oetter, E.; Pretorius, J.; Johnston, N.; Medina, D.; Rodas, G.; Myslinski, T.; Howells, D.; Beard, A.; et al. The athlete monitoring cycle. A practical guide to interpreting and applying training monitoring data. Br. J. Sports Med. 2017, 51, 1451–1452. [Google Scholar] [CrossRef] [Green Version]
- Heidari, J.; Beckmann, J.; Bertollo, M.; Brink, M.; Kallus, W.; Robazza, C.; Kellmann, M. Multidimensional Monitoring of Recovery Status and Implications for Performance. Int. J. Sports Physiol. Perform. 2018, 1–24. [Google Scholar] [CrossRef]
- Buchheit, M.; Chivot, A.; Parouty, J.; Mercier, D.; Al Haddad, H.; Laursen, P.B.; Ahmaidi, S. Monitoring endurance running performance using cardiac parasympathetic function. Eur. J. Appl. Physiol. 2010, 108, 1153–1167. [Google Scholar] [CrossRef]
- Al Haddad, H.; Laursen, P.B.; Chollet, D.; Ahmaidi, S.; Buchheit, M. Reliability of resting and postexercise heart rate measures. Int. J. Sports Med. 2011, 32, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Daanen, H.A.; Lamberts, R.P.; Kallen, V.L.; Jin, A.; van Meeteren, N.L. A systematic review on heart-rate recovery to monitor changes in training status in athletes. Int. J. Sports Physiol. Perform. 2012, 7, 251–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, J.; Peake, J.M.; Buchheit, M. Cardiac parasympathetic reactivation following exercise: Implications for training prescription. Sports Med. 2013, 43, 1259–1277. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Kilding, A.E.; Buchheit, M. Heart rate variability in elite triathletes, is variation in variability the key to effective training? A case comparison. Eur. J. Appl. Physiol. 2012, 112, 3729–3741. [Google Scholar] [CrossRef] [PubMed]
- Plews, D.J.; Laursen, P.B.; Stanley, J.; Kilding, A.E.; Buchheit, M. Training adaptation and heart rate variability in elite endurance athletes: Opening the door to effective monitoring. Sports Med. 2013, 43, 773–781. [Google Scholar] [CrossRef]
- Plews, D.J.; Laursen, P.B.; Le Meur, Y.; Hausswirth, C.; Kilding, A.E.; Buchheit, M. Monitoring training with heart rate-variability. How much compliance is needed for valid assessment? Int. J. Sports Physiol. Perform. 2014, 9, 783–790. [Google Scholar] [CrossRef]
- Saboul, D.; Pialoux, V.; Hautier, C. The impact of breathing on HRV measurements: Implications for the longitudinal follow-up of athletes. Eur. J. Sport Sci. 2013, 13, 534–542. [Google Scholar] [CrossRef]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Koenig, J.; Jarczok, M.N.; Wasner, M.; Hillecke, T.K.; Thayer, J.F. Heart rate variability and swimming. Sports Med. 2014, 44, 1377–1391. [Google Scholar] [CrossRef]
- Da Silva, V.P.; de Oliveira, N.A.; Silveira, H.; Mello, R.G.; Deslandes, A.C. Heart rate variability indexes as a marker of chronic adaptation in athletes: A systematic review. Ann. Noninvasive Electrocardiol. 2015, 20, 108–118. [Google Scholar] [CrossRef]
- Schmitt, L.; Regnard, J.; Millet, G.P. Monitoring fatigue status with hrv measures in elite athletes: An avenue beyond rmssd? Front. Physiol. 2015, 6, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flatt, A.A.; Esco, M.R. Heart rate variability stabilization in athletes: Towards more convenient data acquisition. Clin. Physiol. Funct. Imaging 2016, 36, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Kiss, O.; Sydó, N.; Vargha, P.; Vágó, H.; Czimbalmos, C.; Édes, E.; Zima, E.; Apponyi, G.; Merkely, G.; Sydó, T.; et al. Detailed heart rate variability analysis in athletes. Clin. Auton. Res. 2016, 26, 245–252. [Google Scholar] [CrossRef]
- Saboul, D.; Balducci, P.; Millet, G.; Pialoux, V.; Hautier, C. A pilot study on quantification of training load: The use of HRV in training practice. Eur. J. Sport Sci. 2016, 16, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Bourdillon, N.; Schmitt, L.; Yazdani, S.; Vesin, J.M.; Millet, G.P. Minimal Window Duration for Accurate HRV Recording in Athletes. Front. Neurosci. 2017, 11, 456. [Google Scholar] [CrossRef]
- Lachin, J.M. The role of measurement reliability in clinical trials. Clin. Trials 2004, 1, 553–566. [Google Scholar] [CrossRef]
- Matheson, G.J. We need to talk about reliability: Making better use of test-retest studies for study design and interpretation. Peer J. 2019, 7, e6918. [Google Scholar] [CrossRef] [Green Version]
- Esco, M.R.; Flatt, A.A. Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: Evaluating the agreement with accepted recommendations. J. Sports Sci. Med. 2014, 13, 535–541. [Google Scholar]
- Nakamura, F.Y.; Flatt, A.A.; Pereira, L.A.; Ramirez-Campillo, R.; Loturco, I.; Esco, M.R. Ultra-Short-Term Heart Rate Variability is Sensitive to Training Effects in Team Sports Players. J. Sports Sci. Med. 2015, 14, 602–605. [Google Scholar]
- Nakamura, F.Y.; Pereira, L.A.; Esco, M.R.; Flatt, A.A.; Moraes, J.A.; Cal Abad, C.C.; Loturco, I. Intraday and Interday Reliability of Ultra-Short-Term Heart Rate Variability in Rugby Union Players. J. Strength Cond. Res. 2017, 31, 548–551. [Google Scholar] [CrossRef]
- Pereira, L.A.; Flatt, A.A.; Ramirez-Campillo, R.; Loturco, I.; Nakamura, F.Y. Assessing Shortened Field-Based Heart-Rate-Variability-Data Acquisition in Team-Sport Athletes. Int. J. Sports Physiol. Perform. 2016, 11, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Esco, M.R.; Williford, H.N.; Flatt, A.A.; Freeborn, T.J.; Nakamura, F.Y. Ultra-shortened time-domain HRV parameters at rest and following exercise in athletes: An alternative to frequency computation of sympathovagal balance. Eur. J. Appl. Physiol. 2018, 118, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Vescovi, J.D. Intra-Individual Variation of HRV during Orthostatic Challenge in Elite Male Field Hockey Players. J. Med. Syst. 2019, 43, 328. [Google Scholar] [CrossRef] [PubMed]
- Hung, C.H.; Clemente, F.M.; Bezerra, P.; Chiu, Y.W.; Chien, C.H.; Crowley-McHattan, Z.; Chen, Y.S. Post-Exercise Recovery of Ultra-Short-Term Heart Rate Variability after Yo-Yo Intermittent Recovery Test and Repeated Sprint Ability Test. Int. J. Environ. Res. Public Health 2020, 17, 4070. [Google Scholar] [CrossRef] [PubMed]
- Le Meur, Y.; Hausswirth, C.; Abbiss, C.; Baupi, Y.; Dorel, S. Performance factors in the new combined event of modern pentathlon. J. Sports Sci. 2010, 28, 1111. [Google Scholar] [CrossRef] [PubMed]
- Le Meur, Y.; Dorel, S.; Baup, Y.; Guvomarch, J.P.; Roudaut, C.; Hausswirth, C. Physiological demand and pacing strategy during the new combined event in elite pentathletes. Eur. J. Appl. Physiol. 2012, 112, 2583–2593. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, L.A.; Porto, C.P.; Pierucci, A.P. Critical evaluation of food intake and energy balance in young modern pentathlon athletes: A cross-sectional study. J. Int. Soc. Sports Nutr. 2016, 13, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loureiro, L.L.; Fonseca, S., Jr.; Castro, N.G.; Dos Passos, R.B.; Porto, C.P.; Pierucci, A.P. Basal Metabolic Rate of Adolescent Modern Pentathlon Athletes: Agreement between Indirect Calorimetry and Predictive Equations and the Correlation with Body Parameters. PLoS ONE 2015, 10, e0142859. [Google Scholar] [CrossRef]
- Sadowska, D.; Lichota, M.; Sacewicz, T.; Krzepota, J. Influence of Running Phases on the Postural Balance of Modern Pentathlon Athletes in a Laser Run Event. Int. J. Environ. Res. Public Health 2019, 16, 4440. [Google Scholar] [CrossRef] [Green Version]
- Sadowska, D.; Sacewicz, T.; Lichota, M.; Krzepota, J.; Ładyga, M. Static Postural Balance in Modern Pentathletes: A Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 1760. [Google Scholar] [CrossRef] [Green Version]
- Chirico, A.; Fegatelli, D.; Galli, F.; Mallia, L.; Alivernini, F.; Cordone, S.; Giancamilli, F.; Pecci, S.; Tosi, G.M.; Giordano, A.; et al. A study of quiet eye’s phenomenon in the shooting section of “laser run” of modern pentathlon. J. Cell Physiol. 2019, 234, 9247–9254. [Google Scholar] [CrossRef] [PubMed]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task force of the European society of cardiology and the North American society of pacing and electrophysiology. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Heathers, J.A.J. Everything Hertz: Methodological issues in short-term frequency domain HRV. Front. Physiol. 2014, 5, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintana, D.S.; Heathers, J.A.J. Considerations in the assessment of heart rate variability in biobehavioral research. Front. Psychol. 2014, 5, 805. [Google Scholar] [CrossRef]
- Billman, G.E.; Huikuri, H.V.; Sacha, J.; Trimmel, K. An introduction to heart rate variability: Methodological considerations and clinical applications. Front. Physiol. 2015, 6, 55. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Ernst, G. Heart-Rate Variability—More than Heart Beats? Front. Public Health 2017, 5, 240. [Google Scholar] [CrossRef]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Froelicher, V.; Plews, D. Heart Rate Variability: An Old Metric with New Meaning in the Era of Using mHealth technologies for Health and Exercise Training Guidance. Part Two: Prognosis and Training. Arrhythmia. Electrophysiol. Rev. 2018, 7, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthr. 2019, 38, 3. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Rüdiger, H.; Ziemssen, F. Spectral Analysis of Heart Rate Variability: Time Window Matters. Front. Neurol. 2019, 10, 545. [Google Scholar] [CrossRef] [Green Version]
- Malik, M.; Hnatkova, K.; Huikuri, H.V.; Lombardi, F.; Schmid, R.M.; Zabel, M. CrossTalk proposal: Heart rate variability is a valid measure of cardiac autonomic responsiveness. J. Physiol. 2019, 597, 2595–2598. [Google Scholar] [CrossRef] [PubMed]
- Quintana, D.S.; Alvares, G.A.; Heathers, J.A.J. Guidelines for Reporting Articles on Psychiatry and Heart rate variability (GRAPH): Recommendations to advance research communication. Transl. Psychiatry 2016, 6, e803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gąsior, J.S.; Zamunér, A.R.; Silva, L.E.V.; Williams, C.A.; Baranowski, R.; Sacha, J.; Machura, P.; Kochman, W.; Werner, B. Heart Rate Variability in Children and Adolescents with Cerebral Palsy-A Systematic Literature Review. J. Clin. Med. 2020, 9, 1141. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, S.; Meylan, A.; Rudolph, U. Reliability of short-term measurements of heart rate variability: Findings from a longitudinal study. Biol. Psychol. 2020, 154, 107905. [Google Scholar] [CrossRef] [PubMed]
- Araújo, C.G.; Scharhag, J. Athlete: A working definition for medical and health sciences research. Scand. J. Med. Sci. Sports 2016, 26, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research–Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 8, 89. [Google Scholar] [CrossRef] [Green Version]
- Lucini, D.; Marchetti, I.; Spataro, A.; Malacarne, M.; Benzi, M.; Tamorri, S.; Sala, R.; Pagani, M. Heart rate variability to monitor performance in elite athletes: Criticalities and avoidable pitfalls. Int. J. Cardiol. 2017, 240, 307–312. [Google Scholar] [CrossRef]
- Peltola, M.A. Role of Editing of R–R Intervals in the Analysis of Heart Rate Variability. Front. Physiol. 2012, 3, 148. [Google Scholar] [CrossRef] [Green Version]
- Tarvainen, M.P.; Lipponen, J.; Niskanen, J.P.; Ranta-Aho, P.O. Kubios HRV (ver. 3.0.2). User’s Guide. 2017. Available online: http://www.kubios.com/downloads/Kubios_HRV_Users_Guide.pdf (accessed on 21 July 2020).
- Tarvainen, M.P.; Niskanen, J.P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV-heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Ranta-Aho, P.O.; Karjalainen, P.A. An advanced detrending method with application to HRV analysis. IEEE Trans. Biomed. Eng. 2002, 49, 172–175. [Google Scholar] [CrossRef]
- Sacha, J.; Pluta, W. Different methods of heart rate variability analysis reveal different correlations of heart rate variability spectrum with average heart rate. J. Electrocardiol. 2005, 38, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Sacha, J.; Pluta, W. Alterations of an average heart rate change heart rate variability due to mathematical reasons. Int. J. Cardiol. 2008, 128, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The effect of heart rate on the heart rate variability response to autonomic interventions. Front. Physiol. 2013, 4, 222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagard, R. Athlete’s heart. Heart 2003, 89, 1455–1461. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, A.; Sharma, S.; Boyett, M.R. CrossTalk opposing view: Bradycardia in the trained athlete is attributable to a downregulation of a pacemaker channel in the sinus node. J. Physiol. 2015, 593, 1749–1751. [Google Scholar] [CrossRef]
- Sacha, J.; Barabach, S.; Statkiewicz-Barabach, G.; Sacha, K.; Müller, A.; Piskorski, J.; Barthel, P.; Schmidt, G. How to strengthen or weaken the HRV dependence on heart rate—Description of the method and its perspectives. Int. J. Cardiol. 2013, 168, 1660–1663. [Google Scholar] [CrossRef] [PubMed]
- Monfredi, O.; Lyashkov, A.E.; Johnsen, A.B.; Inada, S.; Schneider, H.; Wang, R.; Nirmalan, M.; Wisloff, U.; Maltsev, V.A.; Lakatta, E.G.; et al. Biophysical characterization of the underappreciated and important relationship between heart rate variability and heart rate. Hypertension 2014, 64, 1334–1343. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, W.G. A New View of Statistics. 2000. Available online: http://sportsci.org/resource/stats (accessed on 3 August 2020).
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, G.; Nevill, A.M. Statistical Methods for Assessing Measurement Error (Reliability) in Variables Relevant to Sports Medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistics Notes: Measurement error proportional to the mean. Br. Med. J. 1996, 313, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: London, UK, 1988; pp. 179–206. [Google Scholar]
- Altman, D.G.; Bland, J.M. Measurement in medicine: The analysis of method comparison studies. Statistician 1983, 32, 307–317. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Abu-Arafeh, A.; Jordan, H.; Drummond, G. Reporting of method comparison studies: A review of advice, an assessment of current practice, and specific suggestions for future reports. Br. J. Anaesth. 2016, 117, 569–575. [Google Scholar] [CrossRef] [Green Version]
- Gerke, O. Reporting Standards for a Bland-Altman Agreement Analysis: A Review of Methodological Reviews. Diagnostics 2020, 10, 334. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Measures of agreement. Perspect. Clin. Res. 2017, 8, 187–191. [Google Scholar] [CrossRef]
- Buchheit, M. Magnitudes matter more than Beetroot Juice. Sport Perform. Sci. Rep. 2018, 1, 1–3. [Google Scholar]
- Gąsior, J.S.; Sacha, J.; Jeleń, P.J.; Zieliński, J.; Przybylski, J. Heart Rate and Respiratory Rate Influence on Heart Rate Variability Repeatability: Effects of the Correction for the Prevailing Heart Rate. Front. Physiol. 2016, 7, 356. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.E.; Beightol, L.A.; Koh, J.; Eckberg, D.L. Important influence of respiration on human R-R interval power spectra is largely ignored. J. Appl. Physiol. 1993, 75, 2310–2317. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, L.; Wdowczyk-Szulc, J.; Valenti, C.; Castoldi, S.; Passino, C.; Spadacini, G.; Sleight, P. Effects of controlled breathing, mental activity and mental stress with or without verbalization on heart rate variability. J. Am. Coll. Cardiol. 2000, 35, 1462–1469. [Google Scholar] [CrossRef] [Green Version]
- Młyńczak, M.; Niewiadomski, W.; Żyliński, M.; Cybulski, G. Ambulatory devices measuring cardiorespiratory activity with motion. In Proceedings of the 10th International Joint Conference on Biomedical Engineering Systems and Technologies, Porto, Portugal, 21–23 February 2017; pp. 91–97. [Google Scholar]
- Młyńczak, M.; Niewiadomski, W.; Żyliński, M.; Cybulski, G.P. Ambulatory Impedance Pneumography Device for Quantitative Monitoring of Volumetric Parameters in Respiratory and Cardiac Applications. In Proceedings of the Computing in Cardiology Conference (CinC), Cambridge, MA, USA, 7–10 September 2014. [Google Scholar]
- Huikuri, H.V.; Mäkikallio, T.H.; Peng, C.K.; Goldberger, A.L.; Hintze, U.; Møller, M. Fractal correlation properties of R-R interval dynamics and mortality in patients with depressed left ventricular function after an acute myocardial infarction. Circulation 2000, 101, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Mäkikallio, T.H.; Huikuri, H.V.; Hintze, U.; Videbæk, J.; Mitrani, R.D.; Castellanos, A.; Myerburg, R.J.; Møller, M. Fractal analysis and time-and frequency-domain measures of heart rate variability as predictors of mortality in patients with heart failure. Am. J. Cardiol. 2001, 87, 178–182. [Google Scholar] [CrossRef]
- Goldberger, A. Complex systems. Proc. Am. Thorac. Soc. 2006, 3, 467–471. [Google Scholar] [CrossRef] [Green Version]
- Huikuri, H.V.; Stein, P.K. Heart rate variability in risk stratification of cardiac patients. Prog. Cardiovasc. Dis. 2013, 56, 153–159. [Google Scholar] [CrossRef]
- Fazan, F.S.; Brognara, F.; Fazan Junior, R.; Murta Junior, L.O.; Silva, L.E.V. Changes in the Complexity of Heart Rate Variability with Exercise Training Measured by Multiscale Entropy-Based Measurements. Entropy 2018, 20, 47. [Google Scholar] [CrossRef] [Green Version]
- Michael, S.; Graham, K.S.; Davis Oam, G.M. Cardiac Autonomic Responses during Exercise and Post-exercise Recovery Using Heart Rate Variability and Systolic Time Intervals-A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef] [Green Version]
- Flatt, A.A.; Esco, M.R. Validity of the ithlete™ Smart Phone Application for Determining Ultra-Short-Term Heart Rate Variability. J. Hum. Kinet. 2013, 39, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Perrotta, A.S.; Jeklin, A.T.; Hives, B.A.; Meanwell, L.E.; Warburton, D.E.R. Validity of the Elite HRV Smartphone Application for Examining Heart Rate Variability in a Field-Based Setting. J. Strength Cond. Res. 2017, 31, 2296–2302. [Google Scholar] [CrossRef] [PubMed]
- Hernando, D.; Garatachea, N.; Almeida, R.; Casajús, J.A.; Bailón, R. Validation of Heart Rate Monitor Polar RS800 for Heart Rate Variability Analysis During Exercise. J. Strength Cond. Res. 2018, 32, 716–725. [Google Scholar] [CrossRef]
- Jakubiak, A.A.; Konopka, M.; Bursa, D.; Król, W.; Anioł-Strzyżewska, K.; Burkhard-Jagodzińska, K.; Sitkowski, D.; Kuch, M.; Braksator, W. Benefits and limitations of electrocardiographic and echocardiographic screening in top level endurance athletes. Biol. Sport 2020, 38, 71–79. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Mean ± SD | Retest Mean ± SD | p | Cohen′s d (95% CI) | ICC (95% CI) | WSCV% (95% CI) | |
|---|---|---|---|---|---|---|
| HR [bpm] | 64.6 ± 9.8 | 62.9 ± 9.7 | 0.73 | −0.18 (−0.35–−0.04) | 0.97 (0.71–0.99) | 2.8 (1.2–4.6) |
| RespRate [breaths/min] | 15 ± 3 | 15 ± 3 | 0.94 | 0.04 (−0.18–0.33) | 0.96 (0.84–0.99) | 3.4 (1.4–5.4) |
| SDNN [ms] | 43.3 ± 16.6 | 45.9 ± 20.0 | 0.78 | 0.14 (−0.11–0.36) | 0.96 (0.81–0.99) | 7.5 (3.0–12.2) |
| RMSSD [ms] | 45.2 ± 17.9 | 48.2 ± 21.1 | 0.76 | 0.15 (0.01–0.33) | 0.97 (0.81–0.99) | 6.7 (2.7–10.9) |
| lnRMSSD | 3.72 ± 0.48 | 3.78 ± 0.49 | 0.83 | 0.11 (−0.05–0.25) | 0.98 (0.89–0.99) | 1.8 (0.7–2.9) |
| lnRMSSD/mRR | −3.12 ± 0.35 | −3.09 ± 0.35 | 0.88 | 0.08 (−0.08–0.20) | 0.99 (0.94–1.00) | 1.4 (0.6–2.2) |
| pNN50 | 21.9 ± 16.6 | 32.1 ±17.3 | 0.25 | 0.60 (−0.03–1.37) | 0.61 (−0.02–0.90) | 152.4 (46.0–336.2) |
| lnLF | 6.22 ± 1.05 | 6.51 ± 1.11 | 0.60 | 0.27 (−0.50–1.24) | 0.66 (0.03–0.92) | 10.4 (4.1–17.1) |
| nLF [nu] | 44.8 ± 20.4 | 48.0 ± 21.7 | 0.77 | 0.15 (−0.21–0.95) | 0.78 (0.23–0.95) | 31.2 (11.8–54.1) |
| lnHF | 6.43 ± 0.94 | 6.60 ± 1.02 | 0.74 | 0.17 (−0.27–0.86) | 0.86 (0.47–0.97) | 6.1 (2.4–9.8) |
| nHF [nu] | 55.2 ± 20.3 | 52.0 ± 21.7 | 0.77 | −0.15 (−0.95–0.21) | 0.78 (0.23–0.95) | 18.9 (7.4–31.8) |
| LF/HF | 1.17 ± 1.17 | 1.35 ± 1.28 | 0.78 | 0.15 (−0.10–0.89) | 0.93 (0.71–0.98) | 55.2 (19.7–101.3) |
| SD2/SD1 | 1.69 ± 0.37 | 1.66 ± 0.42 | 0.89 | −0.07 (−0.55–0.37) | 0.87 (0.48–0.97) | 8.9 (3.5–14.5) |
| ApEn | 1.09 ± 0.11 | 1.05 ± 0.09 | 0.42 | −0.42 (−0.91–0.33) | 0.63 (0.02–0.91) | 6.1 (2.5–9.9) |
| SampEn | 1.67 ± 0.20 | 1.69 ± 0.29 | 0.92 | 0.05 (−0.63–0.74) | 0.67 (−0.05–0.93) | 9.1 (3.6–14.9) |
| DFAα1 | 0.87 ± 0.23 | 0.93 ± 0.31 | 0.67 | 0.23 (−0.34–0.82) | 0.77 (0.26–0.95) | 17.2 (6.7–28.7) |
| Test Mean ± SD | Retest Mean ± SD | p | Cohen’s d | ICC (95% CI) | WSCV% (95% CI) | |
|---|---|---|---|---|---|---|
| HR [bpm] | 64.4 ± 10.3 | 64.0 ± 11.9 | 0.63 | −0.03 (−0.24–0.15) | 0.98 (0.92–0.99) | 2.5 (1.0–3.9) |
| RespRate [breaths/min] | 14.6 ± 2.8 | 14.8 ± 2.8 | 0.80 | 0.05 (−0.36–0.46) | 0.89 (0.56–0.98) | 6.3 (2.5–10.2) |
| RMSSD [ms] | 40.8 ± 16.7 | 47.1 ± 21.7 | 0.18 | 0.33 (−0.15–0.86) | 0.78 (0.29–0.95) | 24.8 (9.5–42.2) |
| lnRMSSD | 3.61 ± 0.53 | 3.73 ± 0.58 | 0.30 | 0.22 (−0.21–0.85) | 0.84 (0.45–0.97) | 6.3 (2.5–10.2) |
| lnRMSSD/mRR | −3.24 ± 0.40 | −3.13 ± 0.44 | 0.31 | 0.27 (−0.26–1.01) | 0.75 (0.23–0.94) | 6.7 (2.7–10.9) |
| Parameter | Mean ± SD 5 min | Mean ± SD 1 min | p | Mean Difference (95% CI) | SWC | LoA | 95% CI for Lower; Upper LoA | ICC (95% CI) | |
|---|---|---|---|---|---|---|---|---|---|
| Test | HR [bpm] | 64.6 ± 9.8 | 64.4 ± 10.3 | 0.52 | 0.2 (−0.6–1.1) | 2.0 | −1.8–2.3 | −3.3–−0.2; 0.7–3.8 | 0.99 (0.98–0.99) |
| RespRate [breaths/min] | 15 ± 3 | 15 ± 3 | 0.50 | 0.0 (−0.6–0.6) | 1.0 | −1.5–1.5 | −2.6–−0.4; 0.4–2.6 | 0.97 (0.85–0.99) | |
| RMSSD [ms] | 45.2 ± 17.9 | 40.8 ± 16.7 | 0.20 | 4.4 (−2.9–11.7) | 3.6 | −12.8–21.6 | −25.9–0.3; 8.5–34.7 | 0.86 (0.48–0.97) | |
| lnRMSSD | 3.72 ± 0.48 | 3.61 ± 0.53 | 0.18 | 0.12 (−0.07–0.30) | 0.10 | −0.32–0.55 | −0.65–0.01; 0.22–0.88 | 0.89 (0.58–0.98) | |
| lnRMSSD/mRR | −3.12 ± 0.35 | −3.24 ± 0.40 | 0.17 | 0.12 (−0.07–0.31) | 0.07 | −0.32–0.56 | −0.66–0.02; 0.23–0.90 | 0.80 (0.32–0.96) | |
| Retest | HR [bpm] | 62.9 ± 9.7 | 64.0 ± 11.9 | 0.29 | −1.1 (−3.4–1.2) | 2.0 | −6.5–4.3 | −10.6–−2.4; 0.2–8.4 | 0.97 (0.86–0.99) |
| RespRate [breaths/min] | 15 ± 3 | 15 ± 3 | 0.36 | 0.0 (−0.5–0.5) | 1.0 | −1.1–1.1 | −1.9–−0.3; 0.3–1.9 | 0.98 (0.92–0.99) | |
| RMSSD [ms] | 48.2 ± 21.1 | 47.1 ± 21.7 | 0.68 | 1.1 (−4.7–6.8) | 4.2 | −12.4–14.5 | −22.6–−2.1; 4.2–24.7 | 0.95 (0.79–0.99) | |
| lnRMSSD | 3.78 ± 0.49 | 3.73 ± 0.58 | 0.42 | 0.05 (−0.09–0.18) | 0.10 | −0.26–0.36 | −0.50–−0.03; 0.12–0.60 | 0.96 (0.82–0.99) | |
| lnRMSSD/mRR | −3.09 ± 0.35 | −3.13 ± 0.44 | 0.53 | 0.04 (−0.09–0.16) | 0.07 | −0.26–0.33 | −0.49–−0.04; 0.11–0.56 | 0.93 (0.71–0.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoffmann, B.; Flatt, A.A.; Silva, L.E.V.; Młyńczak, M.; Baranowski, R.; Dziedzic, E.; Werner, B.; Gąsior, J.S. A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes. Diagnostics 2020, 10, 833. https://doi.org/10.3390/diagnostics10100833
Hoffmann B, Flatt AA, Silva LEV, Młyńczak M, Baranowski R, Dziedzic E, Werner B, Gąsior JS. A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes. Diagnostics. 2020; 10(10):833. https://doi.org/10.3390/diagnostics10100833
Chicago/Turabian StyleHoffmann, Bartosz, Andrew A. Flatt, Luiz Eduardo Virgilio Silva, Marcel Młyńczak, Rafał Baranowski, Ewelina Dziedzic, Bożena Werner, and Jakub S. Gąsior. 2020. "A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes" Diagnostics 10, no. 10: 833. https://doi.org/10.3390/diagnostics10100833