
Sensitivity Analysis and Uncertainty Quantification of Nanoparticle Deposition from Tongue Morphological Variations


Abstract
:1. Introduction
- Developing oropharyngeal models with varying tongue positions.
- Conducting high-fidelity CFD simulations to build a database.
- Preprocessing the database to ensure balanced data representation.
- Training the surrogate model and validating it against new CFD predictions.
- Conducting input sensitivity analysis and dosimetry uncertainty quantification.
2. Materials and Methods
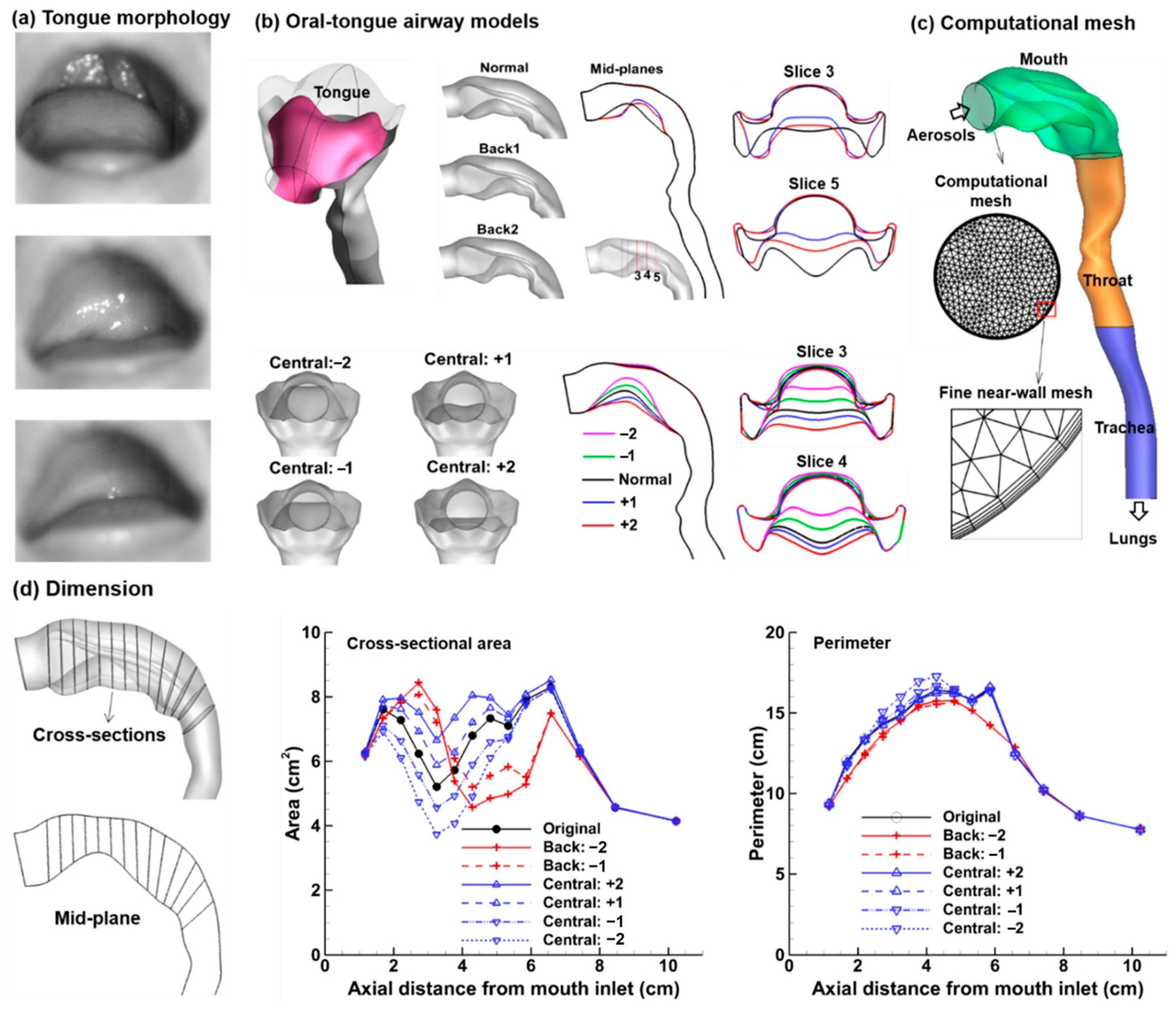
2.1. Mouth-Throat Models with Varying Tongue Postures
2.2. Study Design
2.3. CFD Simulations for Database Development
2.4. Surrogate Model Training, Validation, and Uncertainty Quantification
3. Results
3.1. Airflow and Particle Deposition Simulations: Developing Datase
3.1.1. Airflow
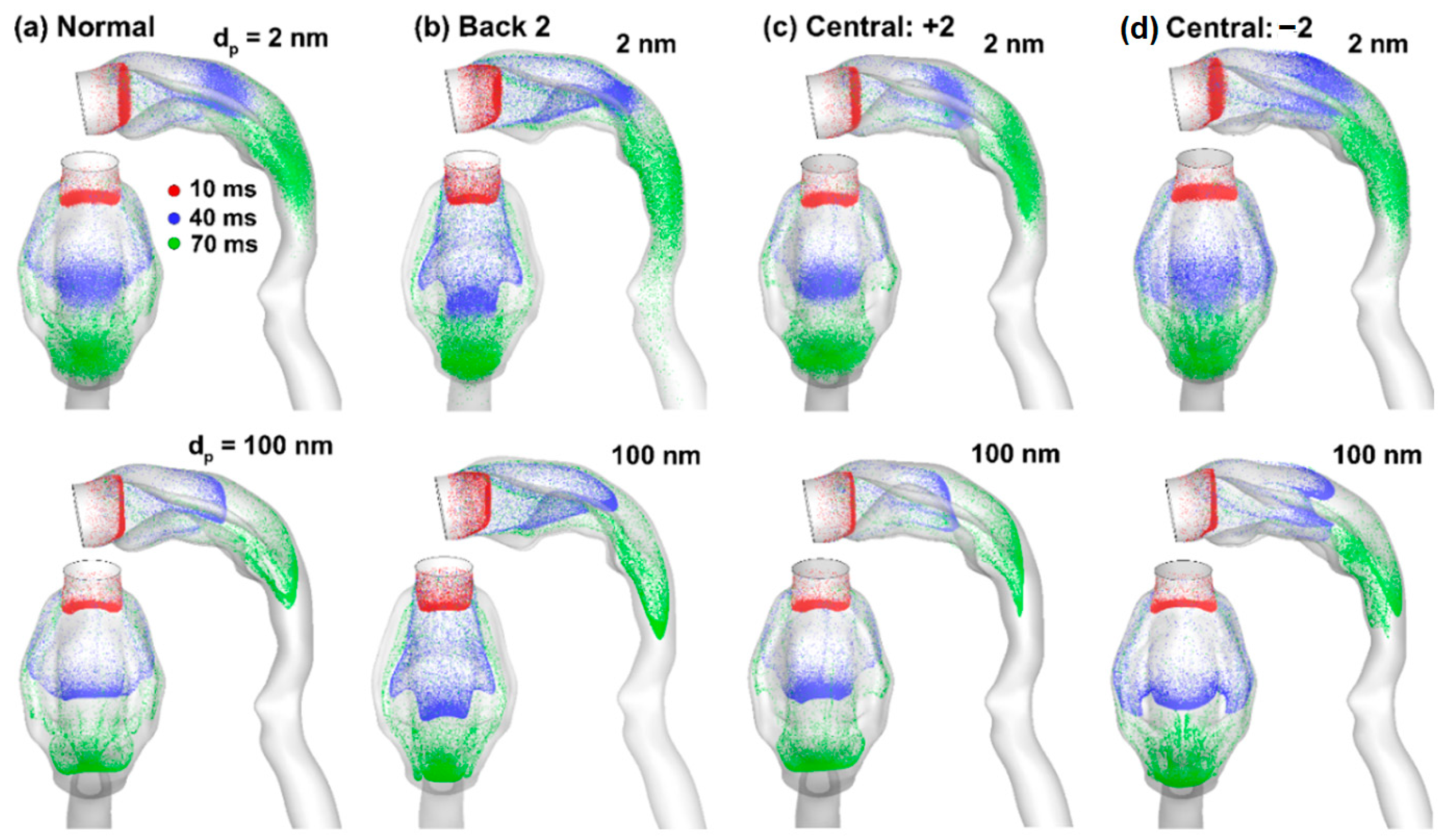
3.1.2. Nanoparticle Dynamics
3.1.3. Nanoparticle Deposition
3.2. Training Dataset Preprocessing
3.2.1. Deposition Data Evaluation
3.2.2. Deposition Data in Log-Log Plot
3.3. Surrogate Model Development and Validation
3.3.1. Model Development
3.3.2. Model Validation
3.4. Sensitivity Analysis (SA) and Uncertainty Quantification (UQ)
3.4.1. Input Sensitivity Analysis
3.4.2. Deposition Uncertainty Quantification
4. Discussion
4.1. Input Sensitivity Analysis and Interaction-Associated Complexity
4.2. Output Uncertainty Quantification (UQ)
4.3. Limitations and Future Studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walenga, R.L.; Butler, C.; Craven, B.A.; Longest, P.W.; Mohamed, R.; Newman, B.; Olsson, B.; Hochhaus, G.; Li, B.V.; Luke, M.C.; et al. Mechanistic modeling of generic orally inhaled drug products: A workshop summary report. CPT Pharmacomet. Syst. Pharmacol. 2023, 12, 560–574. [Google Scholar] [CrossRef] [PubMed]
- Capecelatro, J.; Longest, W.; Boerman, C.; Sulaiman, M.; Sundaresan, S. Recent developments in the computational simulation of dry powder inhalers. Adv. Drug Deliv. Rev. 2022, 188, 114461. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, E. Biological obstacles for identifying in vitro-in vivo correlations of orally inhaled formulations. Pharmaceutics 2019, 11, 316. [Google Scholar] [CrossRef]
- Nováková, A.; Šíma, M.; Slanař, O. Factors affecting drug exposure after inhalation. Prague Med. Rep. 2022, 123, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Walenga, R.L.; Longest, P.W.; Kaviratna, A.; Hindle, M. Aerosol drug delivery during noninvasive positive pressure ventilation: Effects of intersubject variability and excipient enhanced growth. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 190–205. [Google Scholar] [CrossRef] [PubMed]
- Sanchis, J.; Gich, I.; Pedersen, S. Systematic review of errors in inhaler use: Has patient technique improved over time? Chest 2016, 150, 394–406. [Google Scholar] [CrossRef]
- Patil, P.P.; Pawar, A.P.; Mahadik, K.R.; Gaikwad, V.L. An overview of regulations for bioequivalence assessment of locally acting orally inhaled drug products for the United States, Europe, Canada, and India. Expert Opin. Drug Deliv. 2021, 18, 1843–1855. [Google Scholar] [CrossRef]
- Lu, D.; Lee, S.L.; Lionberger, R.A.; Choi, S.; Adams, W.; Caramenico, H.N.; Chowdhury, B.A.; Conner, D.P.; Katial, R.; Limb, S.; et al. International guidelines for bioequivalence of locally acting orally inhaled drug products: Similarities and differences. AAPS J. 2015, 17, 546–557. [Google Scholar] [CrossRef]
- Arieta, A.G. Establishing bioequivalence for orally inhaled drug products. Expert Opin. Drug Deliv. 2011, 8, 1533–1534. [Google Scholar] [CrossRef]
- Selmani, A.; Kovačević, D.; Bohinc, K. Nanoparticles: From synthesis to applications and beyond. Adv. Colloid Interface Sci. 2022, 303, 102640. [Google Scholar] [CrossRef]
- Lu, J.; Xi, J.; Langenderfer, J.E. Sensitivity analysis and uncertainty quantification in pulmonary drug delivery of orally inhaled pharmaceuticals. J. Pharm. Sci. 2017, 106, 3303–3315. [Google Scholar] [CrossRef]
- Xi, J.; Wang, Z.; Si, X.A.; Zhou, Y. Nasal dilation effects on olfactory deposition in unilateral and bi-directional deliveries: In vitro tests and numerical modeling. Eur. J. Pharm. Sci. 2018, 118, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Kim, J.; Si, X.A.; Corley, R.A.; Kabilan, S.; Wang, S. CFD modeling and image analysis of exhaled aerosols due to a growing bronchial tumor: Towards non-invasive diagnosis and treatment of respiratory obstructive diseases. Theranostics 2015, 5, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Zhao, W. Correlating exhaled aerosol images to small airway obstructive diseases: A study with dynamic mode decomposition and machine learning. PLoS ONE 2019, 14, e0211413. [Google Scholar] [CrossRef]
- Garcia, G.J.; Schroeter, J.D.; Segal, R.A.; Stanek, J.; Foureman, G.L.; Kimbell, J.S. Dosimetry of nasal uptake of water-soluble and reactive gases: A first study of interhuman variability. Inhal. Toxicol. 2009, 21, 607–618. [Google Scholar] [CrossRef]
- Schroeter, J.D.; Garcia, G.J.; Kimbell, J.S. A computational fluid dynamics approach to assess interhuman variability in hydrogen sulfide nasal dosimetry. Inhal. Toxicol. 2010, 22, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Borojeni, A.A.T.; Gu, W.; Asgharian, B.; Price, O.; Kuprat, A.P.; Singh, R.K.; Colby, S.; Corley, R.A.; Darquenne, C. In silico quantification of intersubject variability on aerosol deposition in the oral airway. Pharmaceutics 2023, 15, 160. [Google Scholar] [CrossRef]
- Hussain, M.; Renate, W.H.; Werner, H. Effect of intersubject variability of extrathoracic morphometry, lung airways dimensions and respiratory parameters on particle deposition. J. Thorac. Dis. 2011, 3, 156–170. [Google Scholar] [PubMed]
- Zhou, X.; Li, Y.; Miao, H.; Zhang, Y.; Yu, A.; Huang, F.; Li, R.; Tong, Z. Numerical study on the effect of the realistic mouth-inhaler positions on orally inhaled drug delivery in pediatric intersubject upper airways. Powder Technol. 2024, 432, 119163. [Google Scholar] [CrossRef]
- Wedel, J.; Steinmann, P.; Štrakl, M.; Hriberšek, M.; Cui, Y.; Ravnik, J. Anatomy matters: The role of the subject-specific respiratory tract on aerosol deposition—A CFD study. Comput. Methods Appl. Mech. Eng. 2022, 401, 115372. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W. Transport and deposition of micro-aerosols in realistic and simplified models of the oral airway. Ann. Biomed. Eng. 2007, 35, 560–581. [Google Scholar] [CrossRef] [PubMed]
- Xi, J.; Yang, T. Variability in oropharyngeal airflow and aerosol deposition due to changing tongue positions. J. Drug Deliv. Sci. Technol. 2019, 49, 674–682. [Google Scholar] [CrossRef]
- Geiser, M.; Kreyling, W.G. Deposition and biokinetics of inhaled nanoparticles. Part. Fibre Toxicol. 2010, 7, 2. [Google Scholar] [CrossRef]
- Jakobsson, J.K.F.; Aaltonen, H.L.; Nicklasson, H.; Gudmundsson, A.; Rissler, J.; Wollmer, P.; Löndahl, J. Altered deposition of inhaled nanoparticles in subjects with chronic obstructive pulmonary disease. BMC Pulm. Med. 2018, 18, 129. [Google Scholar] [CrossRef]
- Xi, J.; Hu, Q.; Zhao, L.; Si, X.A. Molecular binding contributes to concentration dependent acrolein deposition in rat upper airways: CFD and molecular dynamics analyses. Int. J. Mol. Sci. 2018, 19, 997. [Google Scholar] [CrossRef] [PubMed]
- Dandekar, P.; Venkataraman, C.; Mehra, A. Pulmonary targeting of nanoparticle drug matrices. J. Aerosol Med. Pulm. Drug Deliv. 2010, 23, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Talaat, M.; Si, X.A.; Dong, H.; Xi, J. Leveraging statistical shape modeling in computational respiratory dynamics: Nanomedicine delivery in remodeled airways. Comput. Methods Progr. Biomed. 2021, 204, 106079. [Google Scholar] [CrossRef]
- Wilcox, D. Formulation of the k-omega turbulence model revisited. AIAA J. 2008, 46, 2823–2838. [Google Scholar] [CrossRef]
- Longest, P.W.; Vinchurkar, S. Inertial deposition of aerosols in bifurcating models during steady expiratory flow. J. Aerosol Sci. 2009, 40, 370–378. [Google Scholar] [CrossRef]
- Li, A.; Ahmadi, G. Dispersion and deposition of spherical particles from point sources in a turbulent channel flow. Aerosol Sci. Technol. 1992, 16, 209–226. [Google Scholar] [CrossRef]
- Xi, J.; Longest, P.W.; Martonen, T.B. Effects of the laryngeal jet on nano- and microparticle transport and deposition in an approximate model of the upper tracheobronchial airways. J. Appl. Physiol. 2008, 104, 1761–1777. [Google Scholar] [CrossRef]
- Xi, J.; Yuan, J.E.; Yang, M.; Si, X.; Zhou, Y.; Cheng, Y.-S. Parametric study on mouth–throat geometrical factors on deposition of orally inhaled aerosols. J. Aerosol Sci. 2016, 99, 94–106. [Google Scholar] [CrossRef]
- Taher-Ghahramani, F.; Zheng, F.; Eisfeld, A. Gaussian process regression for absorption spectra analysis of molecular dimers. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2022, 275, 121091. [Google Scholar] [CrossRef]
- Bajer, L.; Pitra, Z.; Repický, J.; Holeňa, M. Gaussian process surrogate models for the CMA evolution strategy. Evol. Comput. 2019, 27, 665–697. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zeng, J. Fast learning with polynomial kernels. IEEE Trans. Cybern. 2019, 49, 3780–3792. [Google Scholar] [CrossRef]
- Tong, H. A note on support vector machines with polynomial kernels. Neural Comput. 2016, 28, 71–88. [Google Scholar] [CrossRef] [PubMed]
- Politis, N.P.; Colombo, P.; Colombo, G.; Dimitrios, M.R. Design of experiments (DoE) in pharmaceutical development. Drug Dev. Ind. Pharm. 2017, 43, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Tavares Luiz, M.; Santos Rosa Viegas, J.; Palma Abriata, J.; Viegas, F.; Testa Moura de Carvalho Vicentini, F.; Lopes Badra Bentley, M.V.; Chorilli, M.; Maldonado Marchetti, J.; Tapia-Blácido, D.R. Design of experiments (DoE) to develop and to optimize nanoparticles as drug delivery systems. Eur. J. Pharm. Biopharm. 2021, 165, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Kumari, M.; Gupta, S.K. Response surface methodological (RSM) approach for optimizing the removal of trihalomethanes (THMs) and its precursor’s by surfactant modified magnetic nanoadsorbents (sMNP)—An endeavor to diminish probable cancer risk. Sci. Rep. 2019, 9, 18339. [Google Scholar] [CrossRef]
- Veza, I.; Spraggon, M.; Fattah, I.M.R.; Idris, M. Response surface methodology (RSM) for optimizing engine performance and emissions fueled with biofuel: Review of RSM for sustainability energy transition. Results Eng. 2023, 18, 101213. [Google Scholar] [CrossRef]
- Hadiyat, M.A.; Sopha, B.M.; Wibowo, B.S. Response surface methodology using observational data: A systematic literature review. Appl. Sci. 2022, 12, 10663. [Google Scholar] [CrossRef]
- Burmeister Getz, E.; Carroll, K.J.; Christopher, J.D.; Morgan, B.; Haughie, S.; Cavecchi, A.; Wiggenhorn, C.; Beresford, H.; Strickland, H.; Lyapustina, S. Performance of multiple-batch approaches to pharmacokinetic bioequivalence testing for orally inhaled drug products with batch-to-batch variability. AAPS PharmSciTech 2021, 22, 225. [Google Scholar] [CrossRef]
- Hofmann, W.; Winkler-Heil, R.; Balásházy, I. The effect of morphological variability on surface deposition densities of inhaled particles in human bronchial and acinar airways. Inhal. Toxicol. 2006, 18, 809–819. [Google Scholar] [CrossRef]
- Martonen, T.; Fleming, J.; Schroeter, J.; Conway, J.; Hwang, D. In silico modeling of asthma. Adv. Drug Deliv. Rev. 2003, 55, 829–849. [Google Scholar] [CrossRef]
- Amirav, I.; Newhouse, M.T. Deposition of small particles in the developing lung. Paediatr. Respir. Rev. 2012, 13, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Zhao, J.; Chen, X.; Lin, J. An in silico subject-variability study of upper airway morphological influence on the airflow regime in a tracheobronchial tree. Bioengineering 2017, 4, 90. [Google Scholar] [CrossRef]
- Jiang, J.; Zhao, K. Airflow and nanoparticle deposition in rat nose under various breathing and sniffing conditions: A computational evaluation of the unsteady effect. J. Aerosol Sci. 2010, 41, 1030–1043. [Google Scholar] [CrossRef] [PubMed]
- Naseri, A.; Shaghaghian, S.; Abouali, O.; Ahmadi, G. Numerical investigation of transient transport and deposition of microparticles under unsteady inspiratory flow in human upper airways. Respir. Physiol. Neurobiol. 2017, 244, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Paul, G.; Ong, H.X.; Young, P.M.; Gu, Y.T.; Saha, S.C. A review of respiratory anatomical development, air flow characterization and particle deposition. Int. J. Environ. Res. Public Health 2020, 17, 380. [Google Scholar] [CrossRef]
- Ehtezazi, T.; Horsfield, M.A.; Barry, P.W.; O’Callaghan, C. Dynamic change of the upper airway during inhalation via aerosol delivery devices. J. Aerosol Med. 2004, 17, 325–334. [Google Scholar] [CrossRef]
- Amann, A.; Corradi, M.; Mazzone, P.; Mutti, A. Lung cancer biomarkers in exhaled breath. Expert Rev. Mol. Diagn. 2011, 11, 207–217. [Google Scholar] [CrossRef]
- Li, J.; Ma, J.; Dong, J.; Yang, W.; Tu, J.; Tian, L. Total and regional microfiber transport characterization in a 15th—Generation human respiratory airway. Comput. Biol. Med. 2023, 163, 107180. [Google Scholar] [CrossRef] [PubMed]
- Su, W.-C.; Cheng, Y.S. Estimation of carbon nanotubes deposition in a human respiratory tract replica. J. Aerosol Sci. 2015, 79, 72–85. [Google Scholar] [CrossRef]
- Mercel, A.I.; Marulanda, K.; Gillis, D.C.; Sun, K.; Clemons, T.D.; Willcox, S.; Griffith, J.; Peters, E.B.; Karver, M.R.; Tsihlis, N.D.; et al. Development of novel nanofibers targeted to smoke-injured lungs. Biomaterials 2021, 274, 120862. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, Y.; Ran, F.; Cui, Y.; Liu, C.; Zhao, Q.; Gao, Y.; Wang, D.; Wang, S. A comparison between sphere and rod nanoparticles regarding their in vivo biological behavior and pharmacokinetics. Sci. Rep. 2017, 7, 4131. [Google Scholar] [CrossRef]
- Zhu, J.; Zhang, S.; Zhang, K.; Wang, X.; Mays, J.W.; Wooley, K.L.; Pochan, D.J. Disk-cylinder and disk-sphere nanoparticles via a block copolymer blend solution construction. Nat. Commun. 2013, 4, 2297. [Google Scholar] [CrossRef]
- Ahookhosh, K.; Pourmehran, O.; Aminfar, H.; Mohammadpourfard, M.; Sarafraz, M.M.; Hamishehkar, H. Development of human respiratory airway models: A review. Eur. J. Pharm. Sci. 2020, 145, 105233. [Google Scholar] [CrossRef]
- Cidem, A.; Bradbury, P.; Traini, D.; Ong, H.X. Modifying and integrating in vitro and ex vivo respiratory models for inhalation drug screening. Front. Bioeng. Biotechnol. 2020, 8, 581995. [Google Scholar] [CrossRef]
- Sakagami, M. In vitro, ex vivo and in vivo methods of lung absorption for inhaled drugs. Adv. Drug Deliv. Rev. 2020, 161–162, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.C.; Luo, Y.X.; Xu, Y.Q. Study on deposition characteristics of microparticles in terminal pulmonary acini by IB-LBM. Micromachines 2021, 12, 957. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Cui, H.; Chen, L.; Sun, K.; Liu, Z. Effects of airway deformation and alveolar pores on particle deposition in the lungs. Sci. Total Environ. 2022, 831, 154931. [Google Scholar] [CrossRef]
- Banat, H.; Ambrus, R.; Csóka, I. Drug combinations for inhalation: Current products and future development addressing disease control and patient compliance. Int. J. Pharm. 2023, 643, 123070. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.T.V.; Tayara, H.; Chong, K.T. Artificial intelligence in drug metabolism and excretion prediction: Recent advances, challenges, and future perspectives. Pharmaceutics 2023, 15, 1260. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Peng, H.H.; Yang, Z.; Ma, X.; Sahakijpijarn, S.; Moon, C.; Ouyang, D.; Williams Iii, R.O. The applications of Machine learning (ML) in designing dry powder for inhalation by using thin-film-freezing technology. Int. J. Pharm. 2022, 626, 122179. [Google Scholar] [CrossRef] [PubMed]
- Calmet, H.; Dosimont, D.; Oks, D.; Houzeaux, G.; Almirall, B.V.; Inthavong, K. Machine learning and sensitivity analysis for predicting nasal drug delivery for targeted deposition. Int. J. Pharm. 2023, 642, 123098. [Google Scholar] [CrossRef] [PubMed]
- Kolluri, S.; Lin, J.; Liu, R.; Zhang, Y.; Zhang, W. Machine learning and artificial intelligence in pharmaceutical research and development: A review. AAPS J. 2022, 24, 19. [Google Scholar] [CrossRef]
- Vora, L.K.; Gholap, A.D.; Jetha, K.; Thakur, R.R.S.; Solanki, H.K.; Chavda, V.P. Artificial intelligence in pharmaceutical technology and drug delivery design. Pharmaceutics 2023, 15, 1916. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | Back 1 | Back 2 | C−2 | C−1 | C+1 | C+2 | |
|---|---|---|---|---|---|---|---|
| Volume, V (cm3) | 49.8 | 48.3 | 47.2 | 44.6 | 47.1 | 51.7 | 53.9 |
| Vol change (%) | 0.0 | −2.96 | −5.20 | −10.48 | −5.54 | 3.79 | 8.17 |
| Surface area, A (cm2) | 107.8 | 106.4 | 108.0 | 112.0 | 109.2 | 107.3 | 106.1 |
| Surface area change (%) | 0.0 | −1.28 | 0.23 | 3.92 | 1.26 | −0.48 | −1.55 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Flow rate (L/min) | 46.7 | 20.6 | 32.9 | 48.5 | 56.4 | 41.5 | 17.4 | 45.1 | 43.4 | 58.5 |
| Particle size (nm) | 10.3 | 5.7 | 2.0 | 5.7 | 13.5 | 70.2 | 1.3 | 11.0 | 1.7 | 2.3 |
| Particle Size | Flow Rate | Back Tongue | Central Tongue | Glottis Area | ||
|---|---|---|---|---|---|---|
| All regions | Main | 0.93706 | 0.01156 | 0.00288 | 0.00476 | 0.00260 |
| Total | 0.98178 | 0.04095 | 0.00709 | 0.01411 | 0.00555 | |
| Ratio * | 0.05 | 2.54 | 1.47 | 1.96 | 1.13 | |
| Mouth | Main | 0.88512 | 0.00758 | 0.00204 | 0.02321 | 0.00164 |
| Total | 0.96728 | 0.03610 | 0.01458 | 0.07058 | 0.00661 | |
| Ratio * | 0.09 | 3.76 | 6.15 | 2.04 | 3.03 | |
| Throat | Main | 0.72473 | 0.00661 | 0.00451 | 0.00670 | 0.00908 |
| Total | 0.97685 | 0.04019 | 0.12131 | 0.08676 | 0.07096 | |
| Ratio * | 0.35 | 5.08 | 25.90 | 11.95 | 6.81 | |
| Trachea | Main | 0.89502 | 0.0174 | 0.0049 | 0.00904 | 0.00624 |
| Total | 0.96469 | 0.0510 | 0.0159 | 0.03486 | 0.01868 | |
| Ratio * | 0.08 | 1.93 | 2.24 | 2.86 | 1.99 |
| Inputs with Normal Distributions | Predicted Output (DF) Uncertainty (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Flow (L/min) | Particle Size (nm) | Back_T ∆V/V0 (%) | Central_T ∆V/V0 (%) | Glottis ∆A/A0 | Total | Mouth | Throat | Trachea |
| 30 ± 9 | 2 ± 1.25 | −1.5 ± 0.5 | 0 ± 1.0 | 0 ± 0.05 | 16.5 ± 5.6 | 8.2 ± 2.9 | 5.0 ± 1.5 | 3.1 ± 1.2 |
| 30 ± 9 | 100 ± 30 | −1.5 ± 0.5 | 0 ± 1.0 | 0 ± 0.05 | 1.5 ± 0.5 | 0.6 ± 0.4 | 0.9 ± 0.3 | 0.2 ± 0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Si, X.; Xi, J. Sensitivity Analysis and Uncertainty Quantification of Nanoparticle Deposition from Tongue Morphological Variations. Life 2024, 14, 406. https://doi.org/10.3390/life14030406
Yang T, Si X, Xi J. Sensitivity Analysis and Uncertainty Quantification of Nanoparticle Deposition from Tongue Morphological Variations. Life. 2024; 14(3):406. https://doi.org/10.3390/life14030406
Chicago/Turabian StyleYang, Tiancheng, Xiuhua Si, and Jinxiang Xi. 2024. "Sensitivity Analysis and Uncertainty Quantification of Nanoparticle Deposition from Tongue Morphological Variations" Life 14, no. 3: 406. https://doi.org/10.3390/life14030406