
Impact of Patient Blood Management on Red Blood Cell Utilization in an Urban Community Teaching Hospital: A Seven-Year Retrospective Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hypothesis
2.1.1. Aim
2.1.2. Data Selection Criteria
2.1.3. Study Endpoints
- Average (and median) of pre-transfusion Hgb levels that triggered the RBC transfusion orders.
- Volume of RBC transfusion units.
- Annual volume of RBC transfusion units when the pre-transfusion Hgb level was ≥ 7 g/dL (thereafter referred to as # Hb le7).
- Annual percentage of RBC transfusion units when the pre-transfusion Hgb level was ≥ 7 g/dL (thereafter referred to as % Hb le7).
- 5.
- The number of two-unit RBC transfusion orders.
- 6.
- When Hgb ≥ 7 g/dL, the number and percentage of two-unit orders of RBC transfusion.
- 7.
- Overall rate of RBC transfusions.
- 8.
- Length of stay (LOS).
- 9.
- Potential cost savings from reducing unnecessary RBC transfusions.This estimation is based on a reduction of % Hb le7.Calculation steps (see Table 1):
- (1)
- Number of transfused RBC units.
- (2)
- Number of RBC units transfused when Hgb triggers ≥ 7 g/dL.
- (3)
- % of RBC units transfused when Hgb trigger ≥ 7 g/dL.
- (4)
- Potential reduction of RBC units = ((3) of year 2013 (3) of year of interest (yi)) × (1) of yi.
- (5)
- Potential cost savings of yi = (4) potential reduced RBC units of yi × USD 1000/unit.
2.1.4. Statistics
3. Results
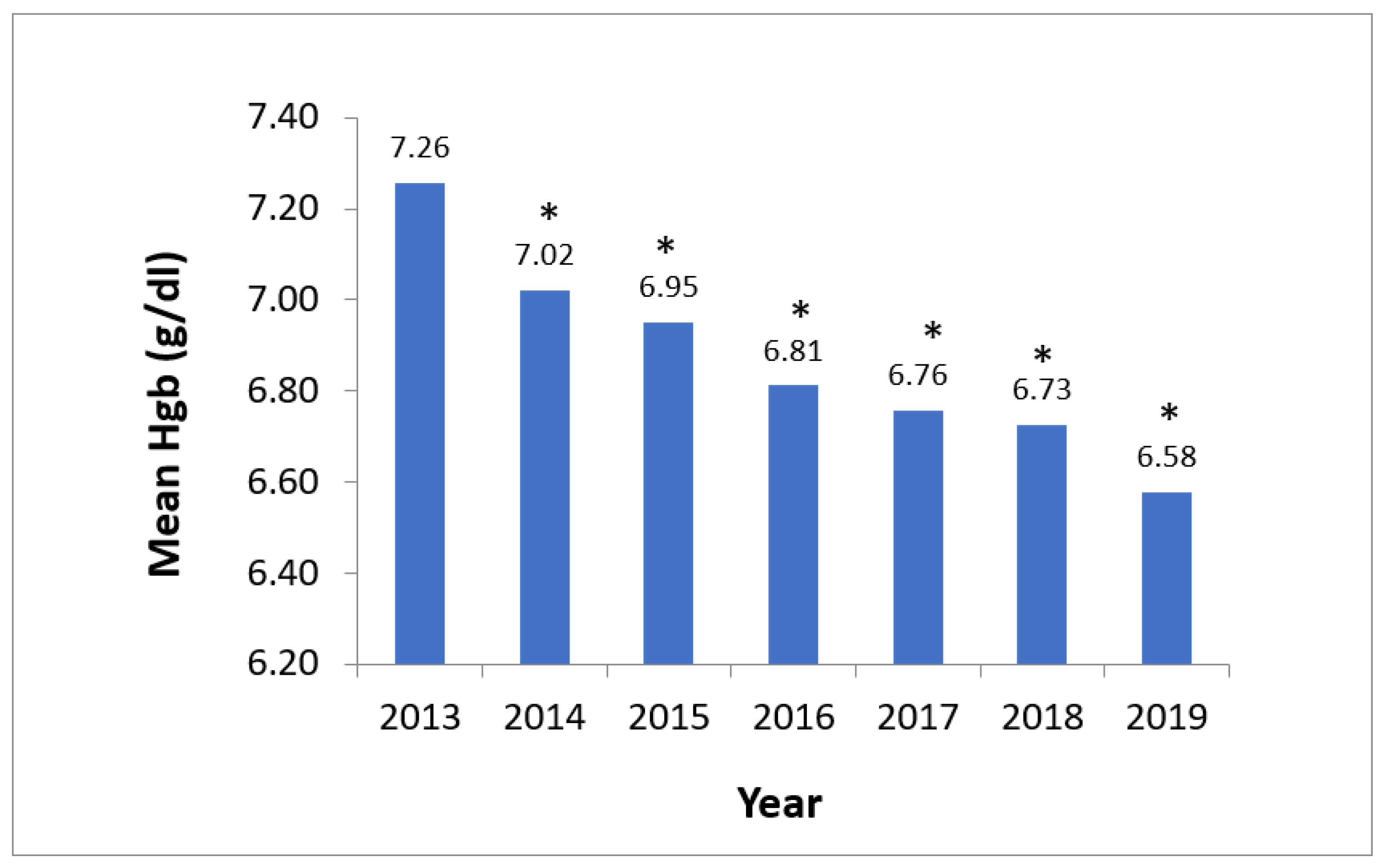
- Mean pre-transfusion Hgb for RBC transfusion orders consistently decreased year-over-year after PBM program implementation, comparing a nadir of 6.58 g/dL in 2019 to 7.26 g/dL in 2013 (p < 0.0001) (Figure 1).
- Median Hgb for RBC transfusion orders revealed the same trend (Supplementary Data Figure S1).
- During the same six-year period (2014–2019), the number of annual transfused RBC units showed a significant decrease of 34% compared to the one in 2013 (Table 1; (2061–1350) ÷ 2061 = 34%).
- Similarly, the absolute number and percentage of transfused RBC units with Hgb trigger ≥ 7 g/dL significantly decreased year-over-year, reaching a nadir in 2019 compared to 2013 (310 units vs. 1210 units, respectively, p < 0.0001, and 23.0% vs. 58.7%, respectively) (Table 1). This reflects a significant reduction (by 35.7%) of unnecessary RBC transfusions consistently year after year. 58.7% − 23.0% = 35.7%.
- The number of two-unit RBC transfusion orders decreased from 150 to 42 post-intervention (Figure 2).
- When Hgb trigger ≥ 7 g/dL, the number and percentage of two-unit orders for RBC transfusions decreased from 65 (3.4% of RBC transfusions) to 3 (0.2%) post-intervention (p < 0.0001), as shown in Figure 3.
- The annual overall rate of RBC transfusion without exclusion per 1000 patient days decreased from 21.9 in 2013 to 16.1 in 2019 (Figure 4), demonstrating a 26% reduction.
- Minimal change in the mean and median inpatient LOS over seven years suggested no hospital patient harm caused by the restrictive PBM program (Table 2).
- This RBC usage reduction translates into approximately 2115 units of RBC saved during the six-year post-launch period (2014–2019). Based on a cost of ~USD 1000 per unit [4], the potential cost savings peaked at ~USD 482,000 in 2019, with total savings of ~USD 2.1 million during the six years of PBM implementation (Table 1).
- The data presented in this paper are original.
4. Discussion
- Transfusion reactions and complications: Receiving unnecessary blood transfusions increases the risk of adverse reactions, which can range from mild to severe transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), allergic reactions, hemolytic reactions, and transfusion-transmitted infections, among others.
- Potential for adverse outcomes: Overtransfusion may not improve patient outcomes and can potentially lead to increased morbidity and mortality in certain cases [6].
- Increased healthcare costs: Blood transfusions are costly and can substantially contribute to healthcare expenses. Unnecessary transfusions lead to increased healthcare spending without providing commensurate benefits to the patient.
- Resource utilization: Inappropriate blood use leads to a strain on blood bank resources, potentially resulting in shortages for patients who genuinely require transfusions.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shander, A.; Lobel, G.P.; Javidroozi, M. Anesthesia for Patients with Anemia. Anesth. Clin. 2016, 34, 711–730. [Google Scholar] [CrossRef]
- Chau, M.; Cohil, D.; Schofield, N.; Abevsiri, S.; Klein, A.; Richards, T. Development and feasibility of a Patient Blood Management implementation programme in vascular surgery. Vasc. Med. 2020, 25, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Warner, M.A.; Schaefer, K.K.; Madde, N.; Burt, J.M.; Higgins, A.A.; Kor, D.J. Improvements in red blood cell transfusion utilization following implementation of a single-unit default for electronic ordering. Transfusion 2019, 59, 2218–2222. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, N.; Kirkley, S.A.; Heal, J.M. A cost analysis of autologous and allogeneic transfusions in hip-replacement surgery. Am J Surg. 1996, 171, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Shander, A.; Hofmann, A.; Ozawa, S.; Theusinger, O.M.; Gombotz, H.; Spahn, D.R. Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfusion 2010, 50, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Shander, A. Transfusion Overuse Exposing an International Problem and Patient Safety Issue. Available online: https://www.sabm.org/assets/pdfs/SABM-Transfusion-Overuse-2019.pdf (accessed on 12 April 2022).
- Jenkins, I.; Doucet, J.J.; Clay, B.; Kopko, P.; Fipps, D.; Hemmen, E.; Paulson, D. Transfusing Wisely: Clinical Decision Support Improves Blood Transfusion Practices. Jt. Comm. J. Qual. Patient Saf. 2017, 43, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Warner, M.A.; Schulte, P.J.; Hanson, A.C.; Madde, N.R.; Burt, J.M.; Higgins, A.A.; Andrijasevic, N.M.; Kreuter, J.D.; Jacob, E.K.; Stubbs, J.R.; et al. Implementation of a Comprehensive Patient Blood Management Program for Hospitalized Patients at a Large United States Medical Center. Mayo Clin. Proc. 2021, 96, 2980–2990. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A.; Spahn, D.R.; Holtorf, A.P. Making patient blood management the new norm(al) as experienced by implementors in diverse countries. BMC Health Serv. Res. 2021, 21, 634. [Google Scholar] [CrossRef] [PubMed]
- Podlasek, S.J.; Thakkar, R.N.; Rotello, L.C.; Fleury, T.A.; Demski, R.J.; Ness, P.M.; Frank, S.M.; Thakkar, R.D. Implementing a “Why give 2 when 1 will do?” Choosing Wisely campaign. Transfusion 2016, 56, 2164. [Google Scholar] [CrossRef] [PubMed]
- Fischer, D.P.; Zacharowski, K.D.; Müller, M.M.; Geisen, C.; Seifried, E.; Müller, H.; Meybohm, P. Patient blood management implementation strategies and their effect on physicians’ risk perception, clinical knowledge and perioperative practice—The frankfurt experience. Transfus. Med. Hemother. 2015, 42, 91–97. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Urgent need to implement patient blood management: Policy brief. 19 October 2021. Available online: https://www.who.int/publications/i/item/9789240035744 (accessed on 3 March 2022).
- Leahy, M.F.; Hofmann, A.; Towler, S.; Trentino, K.M.; Burrows, S.A.; Swain, S.G.; Hamdorf, J.; Gallagher, T.; Koay, A.; Geelhoed, G.C.; et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion 2017, 57, 1347–1358. [Google Scholar] [CrossRef] [PubMed]
- Goodnough, L.T.; Hollenhorst, M.A. Clinical decision support and improved blood use in patient blood management. Hematol. Am. Soc. Hematol. Educ. Program 2019, 2019, 577–582. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | Total |
|---|---|---|---|---|---|---|---|---|
| (1) Number of transfused RBC units | 2061 | 1762 * | 1460 * | 1514 * | 1251 * | 1286 * | 1350 * | |
| (2) Number of RBC units transfused when Hgb trigger ≥ 7 g/dL | 1210 | 830 * | 572 * | 517 * | 371 * | 357 * | 310 * | |
| (3) % of RBC units transfused when Hgb trigger ≥ 7 g/dL = (2) ÷ (1) | 58.7 | 47.1 | 39.2 | 34.1 | 30.0 | 27.8 | 23.0 | |
| (4) Potential reduction of RBC units = ((3) of year 2013 − (3) of this year) × (1) of the year) ** | 0 | 204 | 285 | 372 | 375 | 397 | 482 | 2115 |
| (5) Potential cost saving (USD) = (4) × USD 1000/ unit | 0 | 204K | 285K | 372K | 375K | 398K | 482K | USD 2.1 million |
| LOS (Days) | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 |
| Mean (Days) | 5.1 | 4.9 | 5.5 | 5.5 | 5.2 | 5.3 | 5.5 |
| Standard deviation (Days) | 13.1 | 9.3 | 12.5 | 8.7 | 10.8 | 10.5 | 11.2 |
| Median (Days) | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 |
| Education and training | Start by educating staff, including physicians, nurses, and other healthcare professionals, about the principles and benefits of PBM. Utilize internal expertise that may offer free or low-cost educational materials and training sessions. |
| Clinical guidelines and pathways | Develop and implement evidence-based clinical guidelines and pathways that emphasize conservative blood management strategies. These guidelines can include practices such as minimizing unnecessary blood tests, optimizing hemoglobin levels pre-operatively, and employing blood conservation techniques during surgery. |
| Utilize existing resources | Assess and optimize the use of existing resources within the hospital. Work with the laboratory and clinical staff to reduce unnecessary blood tests, adopt restrictive transfusion thresholds, and explore alternatives to transfusions, such as iron supplementation or medications that reduce bleeding. |
| Quality improvement initiatives | Implement quality improvement initiatives aimed at reducing blood product waste, improving blood utilization practices, and ensuring that transfusions are given based on the established clinical criteria rather than routine practice. |
| Collaboration and partnerships | Collaborate with blood banks, regional blood centers, or other healthcare facilities in the area to explore cost-sharing opportunities, joint training programs, or information sharing related to best practices in blood management. |
| Utilize data and analytics | Leverage data analytics to monitor blood utilization patterns, transfusion rates, and associated costs. This information can help identify areas for improvement and guide decision making to optimize blood utilization without requiring additional funds. |
| Engage stakeholders | Involve stakeholders across different departments and specialties in discussions about PBM. Encourage collaborative efforts to implement changes and promote a culture of responsible blood use throughout the hospital. |
| Adopt technology solutions | Implement electronic health record (EHR) systems or clinical decision support tools that can help clinicians adhere to evidence-based transfusion guidelines, thereby reducing unnecessary blood transfusions. |
| Evaluate and Adjust | Continuously monitor the impact of PBM initiatives on patient outcomes, transfusion rates, and associated costs. Use these data to refine strategies and make the necessary adjustments to improve the effectiveness of PBM practices. |
| Seek Grants or collaborative opportunities | Look for grants or collaborative opportunities within the healthcare community that support PBM initiatives or projects aimed at improving blood management. Participating in such programs can provide additional resources and support without requiring a separate budget allocation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, D.W.; Friedman, M.T.; Lombardi, D.P.; Hwang, R.; Sender, J.; Cobaj, V.; Niazi, M.; Li, Y.; Karpinos, R. Impact of Patient Blood Management on Red Blood Cell Utilization in an Urban Community Teaching Hospital: A Seven-Year Retrospective Study. Life 2024, 14, 232. https://doi.org/10.3390/life14020232
Wu DW, Friedman MT, Lombardi DP, Hwang R, Sender J, Cobaj V, Niazi M, Li Y, Karpinos R. Impact of Patient Blood Management on Red Blood Cell Utilization in an Urban Community Teaching Hospital: A Seven-Year Retrospective Study. Life. 2024; 14(2):232. https://doi.org/10.3390/life14020232
Chicago/Turabian StyleWu, Ding Wen, Mark T. Friedman, Daniel P. Lombardi, Richard Hwang, Joel Sender, Valdet Cobaj, Masooma Niazi, Yanhua Li, and Robert Karpinos. 2024. "Impact of Patient Blood Management on Red Blood Cell Utilization in an Urban Community Teaching Hospital: A Seven-Year Retrospective Study" Life 14, no. 2: 232. https://doi.org/10.3390/life14020232