
Association between Sarcopenia and Reduced Bone Mass: Is Osteosarcopenic Obesity a New Phenotype to Consider in Weight Management Settings?
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Design of the Study
2.2. Body Weight and Height
2.3. Body Composition
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Findings and Concordance with Previous Studies
4.2. Study Strengths and Limitations
4.3. Potential Clinical Implications in Practice and New Directions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front. Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef] [PubMed]
- Masih, D.; Rakhra, G.; Vats, A.; Verma, S.K.; Singh, V.K.; Kirar, V.; Tripathi, J.K.; Singh, S.N. Optimal Cut-Off Values for Body Mass Index and Fat Mass Index Based on Age in Physically Active Males Using Receiver Operating Characteristic Curve. Diseases 2023, 11, 137. [Google Scholar] [CrossRef] [PubMed]
- Silveira, E.A.; Pagotto, V.; Barbosa, L.S.; Oliveira, C.; Pena, G.D.G.; Velasquez-Melendez, G. Accuracy of BMI and waist circumference cut-off points to predict obesity in older adults. Cienc. Saude Colet. 2020, 25, 1073–1082. [Google Scholar] [CrossRef]
- Fruh, S.M. Risk factors, complications, and strategies for sustainable long-term weight management. J. Am. Assoc. Nurse Pract. 2017, 29, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X. The Medical Risks of Obesity. Postgrad. Med. 2009, 121, 21–33. [Google Scholar] [CrossRef]
- Batsis, J.A.; Zbehlik, A.J.; Barre, L.K.; Bynum, J.P.; Pidgeon, D.; Bartels, S.J. Impact of obesity on disability, function, and physical activity: Data from the Osteoarthritis Initiative. Scand. J. Rheumatol. 2015, 44, 495–502. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Polonsky, H.M. The Psychosocial Burden of Obesity. Endocrinol. Metab. Clin. N. Am. 2016, 45, 677–688. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Kasen, S.; Cohen, P.; Chen, H.; Must, A. Obesity and psychopathology in women: A three decade prospective study. Int. J. Obes. 2008, 32, 558–566. [Google Scholar] [CrossRef]
- Roberts, R.E.; Deleger, S.; Strawbridge, W.J.; Kaplan, G.A. Prospective association between obesity and depression: Evidence from the Alameda County Study. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 514–521. [Google Scholar] [CrossRef]
- Tsan-Hon, L.; Pi-Sunyer, F.X.; Laferrère, B. Physical disability and obesity. Nutr. Rev. 2005, 63, 321–331. [Google Scholar]
- Abdelaal, M.; le Roux, C.W.; Docherty, N.G. Morbidity and mortality associated with obesity. Ann. Transl. Med. 2017, 5, 161. [Google Scholar] [CrossRef] [PubMed]
- Boutari, C.; Mantzoros, C.S. A 2022 update on the epidemiology of obesity and a call to action: As its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 2022, 133, 155217. [Google Scholar] [CrossRef] [PubMed]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H.; Obesity Management Task Force of the European Association for the Study of Obesity. European Guidelines for Obesity Management in Adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Hainer, V.; Basdevant, A.; Finer, N.; Fried, M.; Mathus-Vliegen, E.; Micic, D.; Maislos, M.; Roman, G.; Schutz, Y.; et al. Obesity Management Task Force of the European Association for the Study of Obesity. Management of obesity in adults: European clinical practice guidelines. Obes. Facts 2008, 1, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Hassapidou, M.; Vlassopoulos, A.; Kalliostra, M.; Govers, E.; Mulrooney, H.; Ells, L.; Salas, X.R.; Muscogiuri, G.; Darleska, T.H.; Busetto, L.; et al. European Association for the Study of Obesity Position Statement on Medical Nutrition Therapy for the Management of Overweight and Obesity in Adults Developed in Collaboration with the European Federation of the Associations of Dietitians. Obes. Facts 2023, 16, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Ciudin, A.; Simó-Servat, A.; Palmas, F.; Barahona, M.J. Sarcopenic obesity: A new challenge in the clinical practice. Endocrinol. Diabetes Nutr. Engl. Ed. 2020, 67, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Johnson Stoklossa, C.A.; Sharma, A.M.; Forhan, M.; Siervo, M.; Padwal, R.S.; Prado, C.M. Prevalence of Sarcopenic Obesity in Adults with Class II/III Obesity Using Different Diagnostic Criteria. J. Nutr. Metab. 2017, 2017, 7307618. [Google Scholar] [CrossRef]
- Pellegrini, M.; Itani, L.; Rossi, A.P.; Kreidieh, D.; El Masri, D.; Tannir, H.; El Ghoch, M. Approaching Sarcopenic Obesity in Young and Middle-Aged Female Adults in Weight Management Settings: A Narrative Review. Healthcare 2022, 10, 2042. [Google Scholar] [CrossRef]
- El Ghoch, M.; Pellegrini, M. Why should sarcopenic obesity be included in a routine assessment during weight-management programmes? Front. Endocrinol. 2022, 13, 962895. [Google Scholar] [CrossRef]
- Ormsbee, M.J.; Prado, C.M.; Ilich, J.Z.; Purcell, S.; Siervo, M.; Folsom, A.; Panton, L. Osteosarcopenic obesity: The role of bone, muscle, and fat on health. J. Cachexia Sarcopenia Muscle 2014, 5, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Kelly, O.J.; Gilman, J.C.; Boschiero, D.; Ilich, J.Z. Osteosarcopenic Obesity: Current Knowledge, Revised Identification Criteria and Treatment Principles. Nutrients 2019, 11, 747. [Google Scholar] [CrossRef] [PubMed]
- Perna, S.; Rondanelli, M. The Role of Nutrition in Osteosarcopenic Obesity: Lessons Learned during the Last 10 Years and Future Horizons. Nutrients 2023, 15, 2188. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Kong, C.; Yu, H.; Gong, J.; Lan, L.; Zhou, L.; Gong, J.; Liu, P.; Xu, L.; Deng, Q. Association between osteosarcopenic obesity and hypertension among four minority populations in China: A cross-sectional study. BMJ Open 2019, 9, e026818. [Google Scholar] [CrossRef] [PubMed]
- Ilich, J.; Kelly, O.J.; Inglis, J.E. Osteosarcopenic Obesity Syndrome: What Is It and How Can It Be Identified and Diagnosed? Curr. Gerontol. Geriatr. Res. 2016, 2016, 7325973. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.M.; Cruz-Jentoft, A.J.; Fielding, R.A.; Kanis, J.A.; Reginster, J.-Y.; Bruyère, O.; Cesari, M.; Chapurlat, R.; Al-Daghri, N.; Dennison, E.; et al. Is There Enough Evidence for Osteosarcopenic Obesity as a Distinct Entity? A Critical Literature Review. Calcif. Tissue Int. 2019, 105, 109–124. [Google Scholar] [CrossRef]
- Casadei, K.; Kiel, J. Anthropometric Measurement; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Di Daniele, N.; Petramala, L.; Di Renzo, L.; Sarlo, F.; Della Rocca, D.G.; Rizzo, M.; Fondacaro, V.; Iacopino, L.; Pepine, C.; De Lorenzo, A. Body composition changes and cardiometabolic benefits of a balanced Italian Mediterranean Diet in obese patients with metabolic syndrome. Acta Diabetol. 2012, 50, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Mackenzie, T.A.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity, and functional impairments in older adults: National Health and Nutrition Examination Surveys 1999–2004. Nutr. Res. 2015, 35, 1031–1039. [Google Scholar] [CrossRef]
- Cossio-Bolanos, M.; Vidal-Espinoza, R.; Fuentes-Lopez, J.; Castelli Correia de Campos, L.F.; Andruske, C.L.; Urra-Albornoz, C.; Alvear Vasquez, F.; Gomez-Campos, R. Reference values for bone density and bone mineral content from 5 to 80 years old in a province of Chile. PeerJ 2022, 10, e13092. [Google Scholar] [CrossRef]
- Kreidieh, D.; Itani, L.; El Masri, D.; Tannir, H.; Citarella, R.; El Ghoch, M. Association between Sarcopenic Obesity, Type 2 Diabetes, and Hypertension in Overweight and Obese Treatment-Seeking Adult Women. J. Cardiovasc. Dev. Dis. 2018, 5, 51. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Pellegrini, M.; Gualtieri, P.; Itani, L.; El Ghoch, M.; Di Renzo, L. The Risk of Sarcopenia among Adults with Normal-Weight Obesity in a Nutritional Management Setting. Nutrients 2022, 14, 5295. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Sun, S.; Zhang, S.; Hao, Q.; Zhu, B.; Teng, Y.; Long, Q.; Li, S.; Lv, Y.; Yue, Q.; et al. A pooled analysis of the association between sarcopenia and osteoporosis. Medicine 2022, 101, e31692. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Yu, K.; Shyh-Chang, N.; Jiang, Z.; Liu, T.; Ma, S.; Luo, L.; Guang, L.; Liang, K.; Ma, W.; et al. Pathogenesis of sarcopenia and the relationship with fat mass: Descriptive review. J. Cachexia Sarcopenia Muscle 2022, 13, 781–794. [Google Scholar] [CrossRef]
- Hu, K.; Deya Edelen, E.; Zhuo, W.; Khan, A.; Orbegoso, J.; Greenfield, L.; Rahi, B.; Griffin, M.; Ilich, J.Z.; Kelly, O.J. Understanding the Consequences of Fatty Bone and Fatty Muscle: How the Osteosarcopenic Adiposity Phenotype Uncovers the Deterioration of Body Composition. Metabolites 2023, 13, 1056. [Google Scholar] [CrossRef] [PubMed]
- Epsley, S.; Tadros, S.; Farid, A.; Kargilis, D.; Mehta, S.; Rajapakse, C.S. The Effect of Inflammation on Bone. Front. Physiol. 2021, 11, 511799. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.H.; Hwang, H.J.; Shin, H.-Y.; Han, C.H. Association between Sarcopenic Obesity and Bone Mineral Density in Middle-Aged and Elderly Korean. Ann. Nutr. Metab. 2015, 68, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of Sarcopenia among the Elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou-Marketou, N.; Papageorgiou, A.; Chrousos, G.P. Chronic Stress-Related Osteosarcopenic Obesity: A Common Modern Syndrome Requiring Sustained Lifestyle Changes and Stress Management. Endocrines 2023, 4, 378–393. [Google Scholar] [CrossRef]
- Fukuda, T.; Bouchi, R.; Takeuchi, T.; Tsujimoto, K.; Minami, I.; Yoshimoto, T.; Ogawa, Y. Sarcopenic obesity assessed using dual energy X-ray absorptiometry (DXA) can predict cardiovascular disease in patients with type 2 diabetes: A retrospective observational study. Cardiovasc. Diabetol. 2018, 17, 55. [Google Scholar] [CrossRef]
- El Ghoch, M.; Rossi, A.P.; Calugi, S.; Rubele, S.; Soave, F.; Zamboni, M.; Chignola, E.; Mazzali, G.; Bazzani, P.V.; Dalle Grave, R. Physical performance measures in screening for reduced lean body mass in adult females with obesity. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 917–921. [Google Scholar] [CrossRef]
- Deng, H.-W.; Xu, F.-H.; Davies, K.M.; Heaney, R.; Recker, R.R. Differences in bone mineral density, bone mineral content, and bone areal size in fracturing and non-fracturing women, and their interrelationships at the spine and hip. J. Bone Miner. Metab. 2002, 20, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Vucic, V.; Ristic-Medic, D.; Arsic, A.; Petrovic, S.; Paunovic, M.; Vasiljevic, N.; Ilich, J.Z. Nutrition and Physical Activity as Modulators of Osteosarcopenic Adiposity: A Scoping Review and Recommendations for Future Research. Nutrients 2023, 15, 1619. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, S.; Massaro, C.; Landi, F. Preventing Osteoporosis, Sarcopenia and Obesity to Care about Quality of Life. Ann. Geriatr. Med. Res. 2023, 27, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; Giustina, A.; Rovere-Querini, P.; Conte, C. Vitamin D in Osteosarcopenic Obesity. Nutrients 2022, 14, 1816. [Google Scholar] [CrossRef]
- Pang, B.W.J.; Wee, S.L.; Chen, K.K.; Lau, L.K.; Jabbar, K.A.; Seah, W.T.; Ng, D.H.M.; Tan, Q.L.L.; Jagadish, M.U.; Ng, T.P. Coexistence of osteoporosis, sarcopenia and obesity in community-dwelling adults—The Yishun Study. Osteoporos. Sarcopenia 2021, 7, 17–23. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Total (n = 2604) | Non-SO (n = 1703) | SO (n = 901) | Significance * |
|---|---|---|---|---|
| Age | 48.44 (14.31) | 45.77 (13.53) | 53.48 (14.38) | p < 0.01 |
| Sex | X2 = 18.21; p < 0.01 | |||
| Males | 1112 (42.7) | 676 (39.7) | 436 (48.4) | |
| Females | 1492 (57.3) | 1027 (60.3) | 465 (51.6) | |
| Weight (kg) | 93.03 (13.23) | 94.41 (12.8) | 90.41 (13.59) | p < 0.01 |
| Height (m) | 1.65 (0.10) | 1.68 (0.09) | 1.61 (0.10) | p < 0.01 |
| BMI (kg/m2) | 33.87 (2.73) | 33.53 (2.62) | 34.52 (2.82) | p < 0.01 |
| BF (kg) | 39.57 (7.42) | 39.02 (7.37) | 40.61 (7.40) | p < 0.01 |
| BF (%) | 42.87 (7.31) | 41.65 (7.31) | 45.18 (6.72) | p < 0.01 |
| LBM (kg) | 50.71 (11.44) | 52.54 (11.48) | 47.25 (10.53) | p < 0.01 |
| LBM (%) | 54.16 (7.12) | 55.32 (7.10) | 51.98 (6.64) | p < 0.01 |
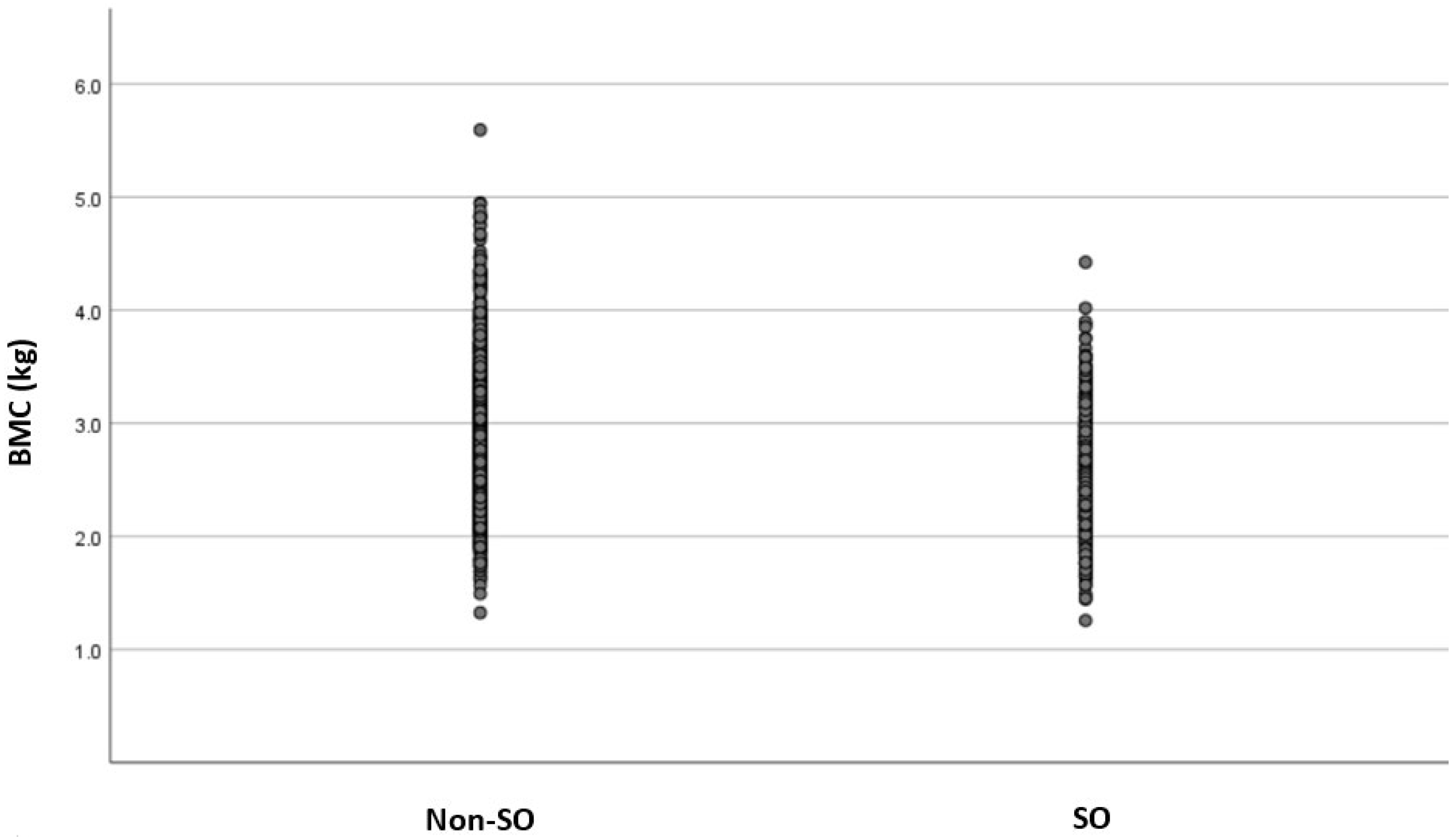
| BMC (kg) | 2.75 (0.56) | 2.85 (0.57) | 2.56 (0.46) | p < 0.01 |
| BMC/h (kg/m) | 1.65 (0.26) | 1.69 (0.27) | 1.58 (0.23) | p < 0.01 |
| X2 = 121.34; p < 0.01 | ||||
| Low BMC | 867 (33.3) | 441 (25.9) | 426 (47.3) | |
| Normal BMC | 1737 (66.7) | 1262 (74.1) | 475 (52.7) |
| Simple Model | Adjusted Model | |||
|---|---|---|---|---|
| Variables | OR | 95%CI | OR | 95%CI |
| Age (years) | 1.05 | 1.04–1.06 | 1.04 | 1.03–1.05 |
| Weight (kg) | 0.97 | 0.97–0.98 | 0.98 | 0.98–0.99 |
| BF (%) | 1.02 | 1.01–1.03 | 0.99 | 0.98–1.01 |
| SO | ||||
| Non-SO | 1.00 | 1 | ||
| SO | 2.57 | 2.17–3.04 | 1.92 | 1.60–2.31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Lorenzo, A.; Itani, L.; Gualtieri, P.; Pellegrini, M.; El Ghoch, M.; Di Renzo, L. Association between Sarcopenia and Reduced Bone Mass: Is Osteosarcopenic Obesity a New Phenotype to Consider in Weight Management Settings? Life 2024, 14, 21. https://doi.org/10.3390/life14010021
De Lorenzo A, Itani L, Gualtieri P, Pellegrini M, El Ghoch M, Di Renzo L. Association between Sarcopenia and Reduced Bone Mass: Is Osteosarcopenic Obesity a New Phenotype to Consider in Weight Management Settings? Life. 2024; 14(1):21. https://doi.org/10.3390/life14010021
Chicago/Turabian StyleDe Lorenzo, Antonino, Leila Itani, Paola Gualtieri, Massimo Pellegrini, Marwan El Ghoch, and Laura Di Renzo. 2024. "Association between Sarcopenia and Reduced Bone Mass: Is Osteosarcopenic Obesity a New Phenotype to Consider in Weight Management Settings?" Life 14, no. 1: 21. https://doi.org/10.3390/life14010021