
Differences in Hemodynamic Response to Passive Leg Raising Tests during the Day in Healthy Individuals: The Question of Normovolemia

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Protocol
2.3. Statistical Analysis
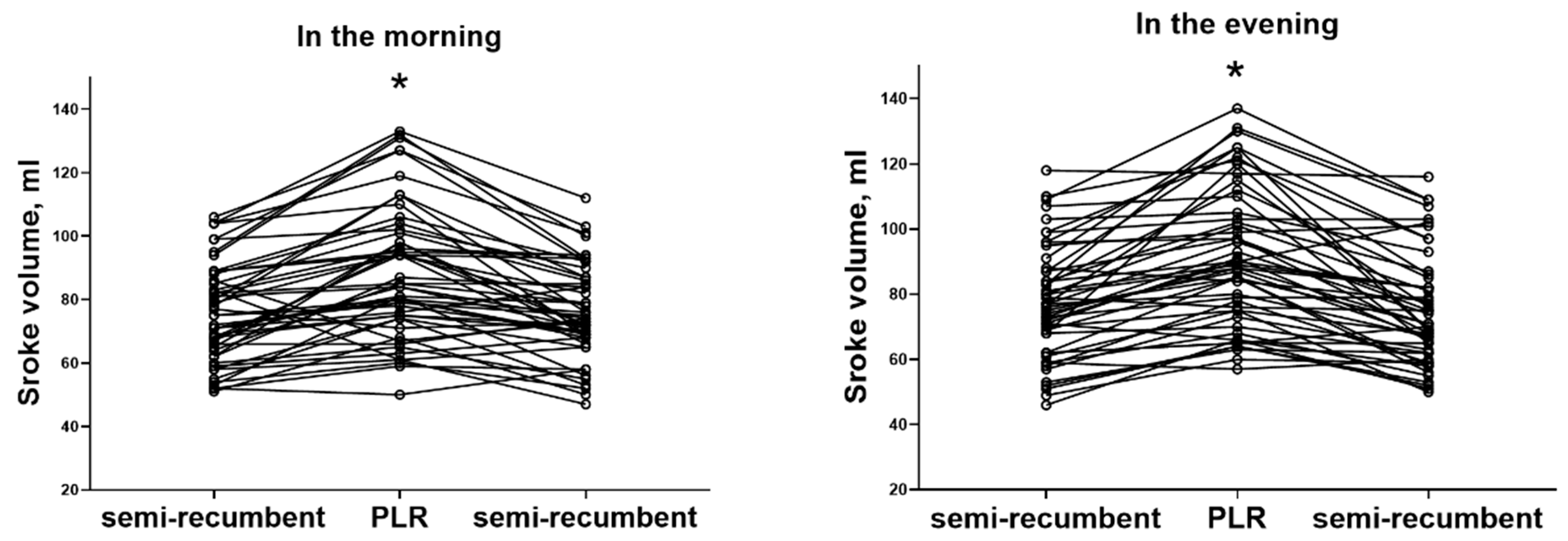
3. Results
Preload Responsiveness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Monnet, X.; Teboul, J.L. Passive leg raising. Intensive Care Med. 2008, 34, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Teboul, J. Passive leg raising: Five rules, not a drop of fluid! Crit. Care 2015, 19, 18. [Google Scholar] [CrossRef] [Green Version]
- London, G.M.; Pannier, B.M.; Laurent, S.; Lacolley, P.; Safar, M.E. Brachial artery diameter changes associated with cardiopulmonary baroreflex activation in humans. Am. J. Physiol. 1990, 258, 773. [Google Scholar] [CrossRef] [PubMed]
- Jermendy, G.; Kammerer, L.; Koltai, Z.M.; Cserhalmi, L.; Szelenyi, J.; Tichy, M.; Pogatsa, G. Preclinical abnormality of left ventricular performance in patients with insulin-dependent diabetes mellitus. Acta Diabetol. Lat. 1983, 20, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Kamran, H.; Salciccioli, L.; Namana, V.; Venkatesan, B.; Santana, C.; Stewart, M.; Lazar, J.M. Passive leg raising induced brachial artery dilation: Is an old technique a simpler method to measure endothelial function? Atherosclerosis 2010, 212, 188–192. [Google Scholar] [CrossRef]
- Jabot, J.; Teboul, J.L.; Richard, C.; Monnet, X. Passive leg raising for predicting fluid responsiveness: Importance of the postural change. Intensive Care Med. 2009, 35, 85–90. [Google Scholar] [CrossRef]
- Marik, P.E.; Lemson, J. Fluid responsiveness: An evolution of our understanding. Br. J. Anaesth. 2014, 112, 617–620. [Google Scholar] [CrossRef] [Green Version]
- Michard, F.; Teboul, J. Predicting fluid responsiveness in ICU patients: A critical analysis of the evidence. Chest 2002, 121, 2000–2008. [Google Scholar] [CrossRef] [Green Version]
- Monnet, X.; Marik, P.; Teboul, J. Passive leg raising for predicting fluid responsiveness: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 1935–1947. [Google Scholar] [CrossRef]
- Cherpanath, T.G.V.; Hirsch, A.; Geerts, B.F.; Lagrand, W.K.; Leeflang, M.M.; Schultz, M.J.; Groeneveld, A.B.J. Predicting Fluid Responsiveness by Passive Leg Raising: A Systematic Review and Meta-Analysis of 23 Clinical Trials. Crit. Care Med. 2016, 44, 981–991. [Google Scholar] [CrossRef] [Green Version]
- Messmer, A.S.; Zingg, C.; Muller, M.; Gerber, J.L.; Schefold, J.C.; Pfortmueller, C.A. Fluid Overload and Mortality in Adult Critical Care Patients-A Systematic Review and Meta-Analysis of Observational Studies. Crit. Care Med. 2020, 48, 1862–1870. [Google Scholar] [CrossRef] [PubMed]
- Boulain, T.; Achard, J.M.; Teboul, J.L.; Richard, C.; Perrotin, D.; Ginies, G. Changes in BP induced by passive leg raising predict response to fluid loading in critically ill patients. Chest 2002, 121, 1245–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elwan, M.H.; Roshdy, A.; Reynolds, J.A.; Elsharkawy, E.M.; Eltahan, S.M.; Coats, T.J. What is the normal haemodynamic response to passive leg raise? A study of healthy volunteers. Emerg. Med. J. 2018, 35, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Hu, K.; Scheer, F.A.J.L.; Laker, M.; Smales, C.; Shea, S.A. Endogenous circadian rhythm in vasovagal response to head-up tilt. Circulation 2011, 123, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Scherhag, A.; Kaden, J.J.; Kentschke, E.; Sueselbeck, T.; Borggrefe, M. Comparison of impedance cardiography and thermodilution-derived measurements of stroke volume and cardiac output at rest and during exercise testing. Cardiovasc. Drugs Ther. 2005, 19, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Borzage, M.; Heidari, K.; Chavez, T.; Seri, I.; Wood, J.C.; Bluml, S. Measuring Stroke Volume: Impedance Cardiography vs. Phase-Contrast Magnetic Resonance Imaging. Am. J. Crit. Care 2017, 26, 408–415. [Google Scholar] [CrossRef]
- Lorne, E.; Mahjoub, Y.; Diouf, M.; Sleghem, J.; Buchalet, C.; Guinot, P.; Petiot, S.; Kessavane, A.; Dehedin, B.; Dupont, H. Accuracy of impedance cardiography for evaluating trends in cardiac output: A comparison with oesophageal Doppler. Br. J. Anaesth. 2014, 113, 596–602. [Google Scholar] [CrossRef] [Green Version]
- Kaszuba, E.; Scheel, S.; Odeberg, H.; Halling, A. Comparing impedance cardiography and echocardiography in the assessment of reduced left ventricular systolic function. BMC Res. Notes 2013, 6, 114. [Google Scholar] [CrossRef] [Green Version]
- Keller, G.; Cassar, E.; Desebbe, O.; Lehot, J.; Cannesson, M. Ability of pleth variability index to detect hemodynamic changes induced by passive leg raising in spontaneously breathing volunteers. Crit. Care 2008, 12, R37. [Google Scholar] [CrossRef] [Green Version]
- Koopmans, N.K.; Stolmeijer, R.; Sijtsma, B.C.; van Beest, P.A.; Boerma, C.E.; Veeger, N.J.; Ter Avest, E. Non-invasive assessment of fluid responsiveness to guide fluid therapy in patients with sepsis in the emergency department: A prospective cohort study. Emerg. Med. J. 2021, 38, 416–422. [Google Scholar] [CrossRef]
- Rameau, A.; de With, E.; Boerma, E.C. Passive leg raise testing effectively reduces fluid administration in septic shock after correction of non-compliance to test results. Ann. Intensive Care. 2017, 7, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Sejersen, C.; Christiansen, T.; Secher, N.H. To identify normovolemia in humans: The stroke volume response to passive leg raising vs. head-down tilt. Physiol. Rep. 2022, 10, e15216. [Google Scholar] [CrossRef]
- Bundgaard-Nielsen, M.; Jorgensen, C.C.; Secher, N.H.; Kehlet, H. Functional intravascular volume deficit in patients before surgery. Acta Anaesthesiol. Scand. 2010, 54, 464–469. [Google Scholar] [CrossRef]
- Holte, K.; Kehlet, H. Compensatory fluid administration for preoperative dehydration--does it improve outcome? Acta Anaesthesiol. Scand. 2002, 46, 1089–1093. [Google Scholar] [CrossRef] [Green Version]
- Muller, L.; Briere, M.; Bastide, S.; Roger, C.; Zoric, L.; Seni, G.; de La Coussaye, J.; Ripart, J.; Lefrant, J. Preoperative fasting does not affect haemodynamic status: A prospective, non-inferiority, echocardiography study. Br. J. Anaesth. 2014, 112, 835–841. [Google Scholar] [CrossRef] [Green Version]
- Godfrey, G.E.P.; Dubrey, S.W.; Handy, J.M. A prospective observational study of stroke volume responsiveness to a passive leg raise manoeuvre in healthy non-starved volunteers as assessed by transthoracic echocardiography. Anaesthesia 2014, 69, 306–313. [Google Scholar] [CrossRef]
- Chopra, S.; Thompson, J.; Shahangian, S.; Thapamagar, S.; Moretta, D.; Gasho, C.; Cohen, A.; Nguyen, H.B. Precision and consistency of the passive leg raising maneuver for determining fluid responsiveness with bioreactance non-invasive cardiac output monitoring in critically ill patients and healthy volunteers. PLoS ONE 2019, 14, e0222956. [Google Scholar] [CrossRef]
- Elwan, M.H.; Roshdy, A.; Elsharkawy, E.M.; Eltahan, S.M.; Coats, T.J. The haemodynamic dilemma in emergency care: Is fluid responsiveness the answer? A systematic review. Scand. J. Trauma. Resusc. Emerg. Med. 2017, 25, 25. [Google Scholar] [CrossRef] [Green Version]
- Marik, P.E.; Levitov, A.; Young, A.; Andrews, L. The use of bioreactance and carotid Doppler to determine volume responsiveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients. Chest 2013, 143, 364–370. [Google Scholar] [CrossRef]
- Biais, M.; Vidil, L.; Sarrabay, P.; Cottenceau, V.; Revel, P.; Sztark, F. Changes in stroke volume induced by passive leg raising in spontaneously breathing patients: Comparison between echocardiography and Vigileo/FloTrac device. Crit. Care 2009, 13, R195. [Google Scholar] [CrossRef] [Green Version]
- Summers, R.L.; Shoemaker, W.C.; Peacock, W.F.; Ander, D.S.; Coleman, T.G. Bench to bedside: Electrophysiologic and clinical principles of noninvasive hemodynamic monitoring using impedance cardiography. Acad. Emerg. Med. 2003, 10, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Chaves, R.C.d.F.; Correa, T.D.; Neto, A.S.; Bravim, B.d.A.; Cordioli, R.L.; Moreira, F.T.; Timenetsky, K.T.; de Assuncao, M.S.C. Assessment of fluid responsiveness in spontaneously breathing patients: A systematic review of literature. Ann. Intensive Care. 2018, 8, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geerts, B.F.; van den Bergh, L.; Stijnen, T.; Aarts, L.P.H.J.; Jansen, J.R.C. Comprehensive review: Is it better to use the Trendelenburg position or passive leg raising for the initial treatment of hypovolemia? J. Clin. Anesth. 2012, 24, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, F.A.; Bastian, B.C.; Thal, E.R.; Atkins, J.M.; Blomqvist, C.G. Passive leg raising does not produce a significant or sustained autotransfusion effect. J. Trauma 1982, 22, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Sondergaard, S. Observational study on passive leg raising and the autonomic nervous system. Physiol. Rep. 2022, 10, e15537. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.H.; O’Connor, D.; Tremper, K.K.; Zaccari, J.; Thompson, P.; Hill, D. Changes in cardiac output after acute blood loss and position change in man. Crit. Care Med. 1989, 17, 979–983. [Google Scholar] [CrossRef]
- Marques, N.R.; Martinello, C.; Kramer, G.C.; Costantine, M.M.; Vadhera, R.B.; Saade, G.R.; Hankins, G.D.; Pacheco, L.D. Passive leg raising during pregnancy. Am. J. Perinatol. 2015, 32, 393–398. [Google Scholar] [CrossRef]
- Barbieri, R.; Triedman, J.K.; Saul, J.P. Heart rate control and mechanical cardiopulmonary coupling to assess central volume: A systems analysis. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2002, 283, 1210. [Google Scholar] [CrossRef] [Green Version]
- Suehiro, K. Assessing fluid responsiveness during spontaneous breathing. J. Anesth. 2022, 36, 579–582. [Google Scholar] [CrossRef]
- Caplan, M.; Durand, A.; Bortolotti, P.; Colling, D.; Goutay, J.; Duburcq, T.; Drumez, E.; Rouze, A.; Nseir, S.; Howsam, M.; et al. Measurement site of inferior vena cava diameter affects the accuracy with which fluid responsiveness can be predicted in spontaneously breathing patients: A post hoc analysis of two prospective cohorts. Ann. Intensive Care. 2020, 10, 168. [Google Scholar] [CrossRef]
- Preau, S.; Bortolotti, P.; Colling, D.; Dewavrin, F.; Colas, V.; Voisin, B.; Onimus, T.; Drumez, E.; Durocher, A.; Redheuil, A.; et al. Diagnostic Accuracy of the Inferior Vena Cava Collapsibility to Predict Fluid Responsiveness in Spontaneously Breathing Patients with Sepsis and Acute Circulatory Failure. Crit. Care Med. 2017, 45, e290–e297. [Google Scholar] [CrossRef]
- Hong, D.M.; Lee, J.M.; Seo, J.H.; Min, J.J.; Jeon, Y.; Bahk, J.H. Pulse pressure variation to predict fluid responsiveness in spontaneously breathing patients: Tidal vs. forced inspiratory breathing. Anaesthesia 2014, 69, 717–722. [Google Scholar] [CrossRef] [Green Version]
- Mukai, A.; Suehiro, K.; Kimura, A.; Kodama, S.; Tanaka, K.; Mori, T.; Nishikawa, K. Impact of deep breathing on predictability of stroke volume variation in spontaneous breathing patients. Acta Anaesthesiol. Scand. 2020, 64, 648–655. [Google Scholar] [CrossRef]
- Bronzwaer, A.G.T.; Ouweneel, D.M.; Stok, W.J.; Westerhof, B.E.; van Lieshout, J.J. Arterial Pressure Variation as a Biomarker of Preload Dependency in Spontaneously Breathing Subjects—A Proof of Principle. PLoS ONE 2015, 10, e0137364. [Google Scholar] [CrossRef]
- Van Dongen, H.P.; Maislin, G.; Kerkhof, G.A. Repeated assessment of the endogenous 24-hour profile of blood pressure under constant routine. Chronobiol. Int. 2001, 18, 85–98. [Google Scholar] [CrossRef]
- Shea, S.A.; Hilton, M.F.; Hu, K.; Scheer, F.A.J.L. Existence of an endogenous circadian blood pressure rhythm in humans that peaks in the evening. Circ. Res. 2011, 108, 980–984. [Google Scholar] [CrossRef]
- Thosar, S.S.; Berman, A.M.; Herzig, M.X.; McHill, A.W.; Bowles, N.P.; Swanson, C.M.; Clemons, N.A.; Butler, M.P.; Clemons, A.A.; Emens, J.S.; et al. Circadian Rhythm of Vascular Function in Midlife Adults. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1203–1211. [Google Scholar] [CrossRef] [Green Version]
- Smolensky, M.H.; Hermida, R.C.; Portaluppi, F. Circadian mechanisms of 24-hour blood pressure regulation and patterning. Sleep Med. Rev. 2017, 33, 4–16. [Google Scholar] [CrossRef]
- He, H. Passive Leg Raising in Intensive Care Medicine. Chin. Med. J. 2016, 129, 1755–1758. [Google Scholar] [CrossRef]
- Vartun, A.; Flo, K.; Acharya, G. Effect of passive leg raising on systemic hemodynamics of pregnant women: A dynamic assessment of maternal cardiovascular function at 22–24 weeks of gestation. PLoS ONE 2014, 9, e94629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sayed, H.; Hainsworth, R. Relationship between plasma volume, carotid baroreceptor sensitivity and orthostatic tolerance. Clin. Sci. 1995, 88, 463–470. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 50) | In the Morning | In the Evening | |||
|---|---|---|---|---|---|
| Responders (n = 32) | Non-Responders (n = 18) | Responders (n = 33) | Non-Responders (n = 17) | ||
| Gender, female, n (%) | 34 (68) | 21 (66) | 13 (72) | 22 (67) | 12 (71) |
| Age, years | 23 (22–24) | 23 (22–24) | 23 (22–23) | 23 (23–24) | 23 (22–24) |
| Body mass index, kg/m2 | 21.8 (20.0–23.8) | 22.0 (20.2–24.1) | 21.5 (19.8–22.7) | 21.9 (20.0–24.3) | 21.7 (20.1–23.3) |
| Stroke volume, mL | 74 (64–87) | 71 (63–87) | 76 (65–87) | 75 (60–84) | 79 (69–98) |
| Cardiac output, L/min | 5.9 (5.3–6.7) | 5.9 (4.9–6.5) | 6.1 (5.5–6.8) | 6.2 (5.3–6.8) | 6.8 (5.8–7.5) |
| Heart rate, beats/min | 81 (70–90) | 80 (69–90) | 83 (70–90) | 84 (73–92) | 81 (69–96) |
| In the Morning | In the Evening | |||||
|---|---|---|---|---|---|---|
| Before PLR | PLR | After PLR | Before PLR | PLR | After PLR | |
| Heart rate, beats/min | 81 (70–90) | 78 (69–85) a | 74 (64–85) ac | 82 (72–92) | 81 (70–89) b | 79 (68–88) b |
| Cardiac output, L/min | 5.9 (5.3–6.7) | 6.6 (5.8–7.6) a | 5.4 (4.8–6.3) c | 6.3 (5.4–7.1) a | 7.2 (6.0–8.1) b | 5.6 (5.0–6.4) bd |
| Stroke volume, mL | 74 (64–87) | 85 (74–101) a | 74 (68–88) c | 77 (62–87) | 89 (75–106) b | 71 (62–86) d |
| In the Morning | In the Evening | |||||
|---|---|---|---|---|---|---|
| Before PLR | After PLR | p | Before PLR | After PLR | p | |
| MAP, mmHg | 92 (88–100) | 91 (86–97) | 0.010 | 96 (92–103) a | 95 (89–101) | 0.004 |
| SVRI | 2158 (1950–2447) | 2221 (1827–2576) | 0.696 | 2157 (1851–2374) | 2147 (1964–2562) | 0.120 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pranskunas, A.; Gulbinaite, E.; Navickaite, A.; Pranskuniene, Z. Differences in Hemodynamic Response to Passive Leg Raising Tests during the Day in Healthy Individuals: The Question of Normovolemia. Life 2023, 13, 1606. https://doi.org/10.3390/life13071606
Pranskunas A, Gulbinaite E, Navickaite A, Pranskuniene Z. Differences in Hemodynamic Response to Passive Leg Raising Tests during the Day in Healthy Individuals: The Question of Normovolemia. Life. 2023; 13(7):1606. https://doi.org/10.3390/life13071606
Chicago/Turabian StylePranskunas, Andrius, Egle Gulbinaite, Aiste Navickaite, and Zivile Pranskuniene. 2023. "Differences in Hemodynamic Response to Passive Leg Raising Tests during the Day in Healthy Individuals: The Question of Normovolemia" Life 13, no. 7: 1606. https://doi.org/10.3390/life13071606