
SARS-CoV-2 Infection—A Trigger Factor for Telogen Effluvium: Review of the Literature with a Case-Based Guidance for Clinical Evaluation

 , ,
, ,
Abstract
:1. Introduction
- -
- maculopapular lesions,
- -
- urticaria-like rash (average duration of four days),
- -
- morbilliform rash (average duration of seven days),
- -
- papulosquamous eruption (average duration of 20 days),
- -
- pityriasis rosea Gibert,
- -
- erythema multiforme-like rash,
- -
- varicella-like rash,
- -
- transient livedo reticularis,
- -
- -
- urticaria,
- -
- angioedema,
- -
- erythroderma,
- -
- generalized pustular reactions after the administration of Hydroxychloroquine,
- -
- drug toxidermia,
- -
- Stevens–Johnson syndrome or toxic epidermal necrolysis syndrome [5].
2. A Case-Based Guidance for Clinical Evaluation
- -
- restrictive diets,
- -
- medications (for ten years, she had been treated with venotonics and converting enzyme inhibitors; for COVID-19 infection, she only took antipyretic drugs),
- -
- chemical substances that can be involved in shortening the duration of the anagen phase,
- -
- other stressful events outside of the COVID-19 infection (surgical interventions, mental, or physical stress, etc.),
- -
- menstrual cycle disorders (to confirm or exclude other endocrinological causes that could be the basis of excessive hair loss).
- -
- Anamnesis: In the last two months, she had a moderate form of SARS-CoV-2 infection;
- -
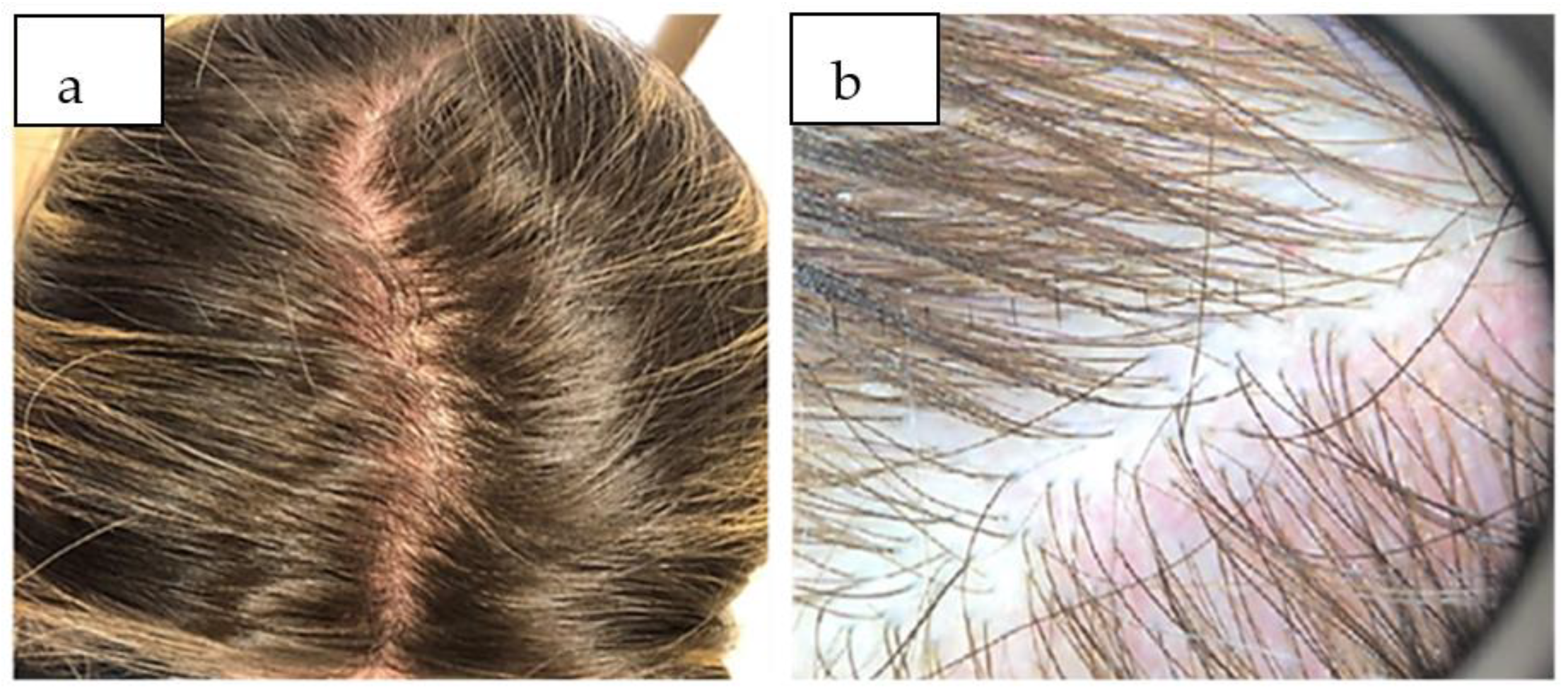
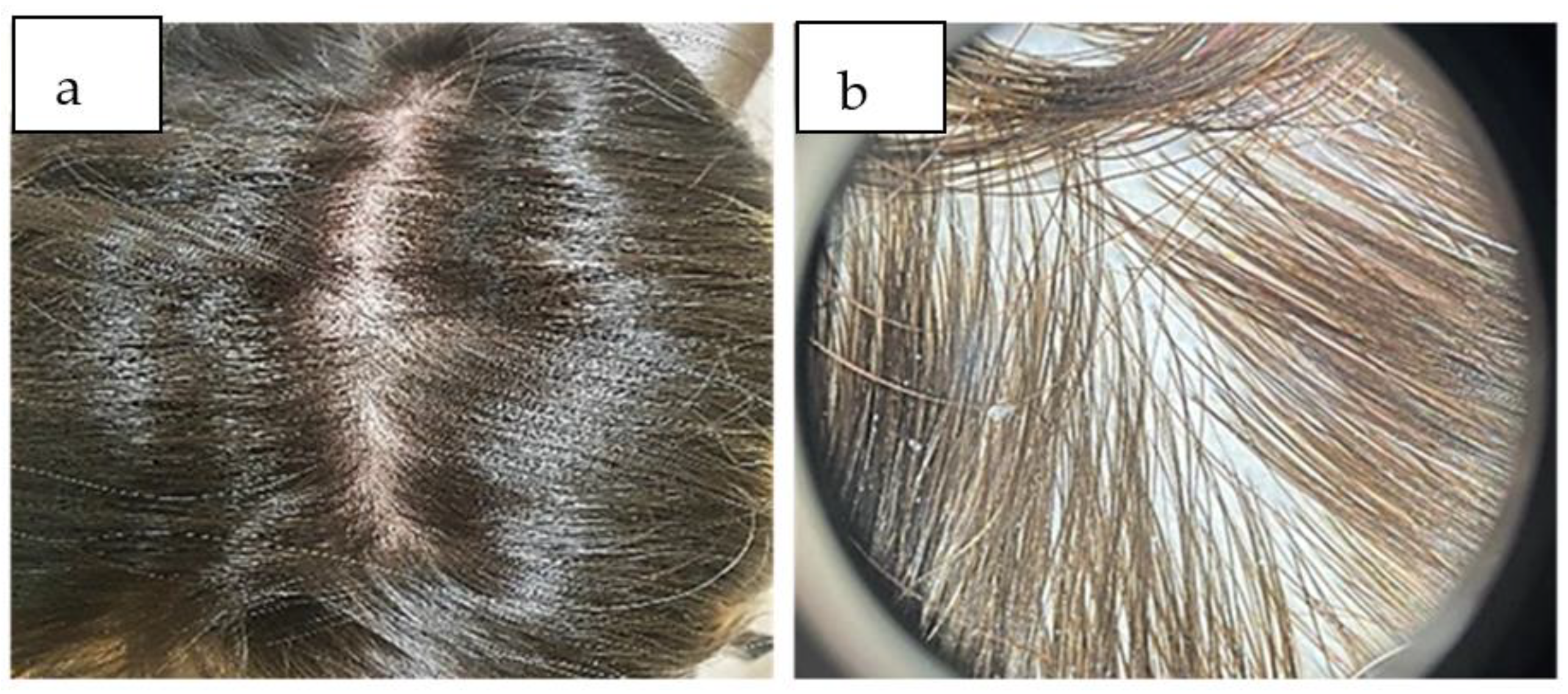
- The dermatological examination: This was a diffusely low density of hairs, normal scalp skin, and no subjective symptomatology. The hair pull test was positive;
- -
- Trichoscopy: There was a diffuse decrease in hair density; in some places were bare follicles at the level of the affected areas, without scales on the examined fields (Figure 1b), which confirmed the diagnosis of telogen effluvium and excluded other conditions that evolve with non-scarring alopecia.
- -
- Alopecia areata, in which circumscribed, non-scarring, noninflammatory, asymptomatic alopecia plaques appear. Trichoscopically noted features are present exclamation mark hairs, yellow or black dots, and smaller vellus hair. Spontaneous recovery is obtained in most cases after the elimination of the causative agent [23,24].
- -
- Androgenetic alopecia in women with a diffuse decrease in hair volume, wherein the frontoparietal area of the scalp is the most affected, but with the frontal line remains intact. Associated clinical signs of hyperandrogenism may be present (hirsutism and menstrual cycle disorders). Trichoscopy shows follicular miniaturization, the presence of yellow dots, and perifollicular pigmentation, and the ratio of telogen/anagen strands is <3:1 [25,26].
- -
- Secondary syphilis, in which the alopecia may have a moth-eaten (parieto-occipital region) or a diffuse or mixed appearance. Trichoscopy is non-specific and may reveal empty hair follicles and smaller hairs follicles (TE-like), broken hairs, black dots (tinea capitis-like), zigzag hairs (alopecia areata-like), etc. The skin of the scalp is unaffected, and the serology for treponema pallidum is positive [27,28].
- -
- Noninflammatory tinea capitis, in which the alopecia plaques extend to the periphery, are itchy, have scales on the surface, and the parasitic hairs break at the level of the scalp at the opening of the follicles with the appearance of black dots (tinea capitis caused by trichophyton) or at 1–3 mm above the scalp (tinea capitis caused by microsporum). Trichoscopy reveals black dots and/or comma hair and/or short, broken hair with perifollicular scaling. The mycological examination confirms the diagnosis, thus specifying the mycotic etiology [29,30].
- -
- Drug-induced alopecia, which highlights a causal association or relationship between the administration and a new drug [31].
- -
- Trichotillomania is an obsessive-compulsive psychiatric disorder characterized by repeatedly pulling out one’s hair from any region of the body. The pull-test is negative and tricoschopically may present a V-sign, trichoptilosis, hook hairs, broken hair, flame hairs, coiled hair, tulip hairs, hair powder, follicular micro-hemorrhages, etc. [32,33].
3. Discussion
- -
- -
- The severe systemic inflammation triggered by the virus influences the appearance of this condition. Because matrix cells are destroyed during the immune response, the cytokine storm can trigger telogen effluvium, and its presence correlates with a higher risk of TE;
- -
- Perifollicular inflammation manifested by the accumulation of activated macrophages and mast cell degranulation in the context of psychological stress [1]. The role of follicular monocytes in triggering the mechanisms of initiation of telogen effluvium is recognized, which determines a transient monocytopenia during the recovery period [41];
- -
- -
- A higher incidence of telogen effluvium among women. The studies conducted by Seyfi et al. on 465 patients COVID-19 who tested positive for telogen effluvium showed that 67.5% were women, and the average age was 44 years [34]. In a group of 30 patients, Abrantes et al. highlighted a preponderance of this pathology in women (70%) [35]. Similar data were obtained by Hussein et al. (67.5% women) [19]. Considering the predominance of the condition in women, we can consider that estrogens and progesterone may be involved in the pathogenesis of telogen effluvium. Their effects are immunomodulatory and anti-inflammatory, thus protecting the hair follicle. Estradiol alters the hair follicle growth and cycle through its receptors. Progesterone decreases the conversion of testosterone to dihydrotestosterone, with effects on the hair cycle, thereby shortening the anagen phase. Thus, hair loss in women infected with COVID-19 may be due to the viral infection causing a significant reduction in systemic estrogen and progesterone levels [39]. In a viral context, SARS-CoV-2 increases the level of pro-inflammatory cytokines (IL6—interleukin 6, TNFα—tumor necrosis factor α, and IL1β—interleukin 1β), decreases various growth factors (IGF1—insulin-like growth factor 1, TGF β1—transforming growth factor β1, VEGF—vascular endothelial growth factor, and FGF β—fibroblastic growth factor β), with the result being the apoptosis of follicular keratinocytes.
- -
- The onset of the condition two months after infection: Our patient presented excessive hair loss two months after the SARS-CoV-2 infection. Studies show that 62.5% of patients developed TE within the first month of being diagnosed with COVID-19. and 47.8% developed TE after 12 weeks or more [34].
- -
- Alopecia patterns are diffuse and non-scarring. In our case, the alopecia was diffuse and more evident in the frontoparietal region, in accordance with data from the literature.
- -
- The psycho-emotional implications are significant, especially in female patients. This also motivated our patient to search for a specialized medical service. In addition, the therapeutic response was increased by correcting the emotional component of the patient by correctly informing her about the self-limited and reversible character of this pathology.
- -
- The evolution of the condition is self-limited, with full recovery within a few months of onset. Hussain et al. observed that telogen effluvium is self-limiting, with remission in 3–6 months from the beginning of the onset [19]. However, Seyfi et al. highlighted that excessive, continuous hair loss might occur for over six months [34]. Most patients are concerned that they will gradually lose all the hair on their scalp, and it is important to note that this is not expected, as it has been proven that loss affects up to 30% of scalp hair [46]. The duration and severity of the COVID-19 episode, as well as the severity and the type of hair loss, must also be taken into account, as these are associated with a greater severity of the COVID-19 infection [39]. Considering the importance of the psycho-emotional factor in the etiopathogenesis of this condition, it is of real benefit to inform patients that hair loss is temporary, but, in some cases, it can take up to 18 months for the thickness and density of the hair to return to its original appearance [19].
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ohyama, M.; Matsudo, K.; Fujita, T. Management of hair loss after severe acute respiratory syndrome coronavirus 2 infection: Insight into the pathophysiology with implication for better management. J. Dermatol. 2022, 49, 939–947. [Google Scholar] [CrossRef] [PubMed]
- Abdulwahab, R.A.; Aldajani, B.M.; Natto, N.K.; Janabi, A.M.; Alhijaili, O.I.; Faqih, N.T.; Alharbi, A. Prevalence of Hair Loss after COVID-19 Infection in Makkah Region, Saudi Arabia. Cureus 2022, 14, e29285. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Magri, F.; Sernicola, A.; Michelini, S.; Caro, G.; Muscianese, M.; Di Fraia, M.; Chello, C.; Fortuna, M.C.; Grieco, T. Telogen Effluvium after SARS-CoV-2 Infection: A Series of Cases and Possible Pathogenetic Mechanisms. Skin. Appendage Disord. 2021, 21, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Birlutiu, V.; Birlutiu, R.M.; Iancu, G.M. Pityriasis rosea Gibert triggered by SARS-CoV-2 infection: A case report. Medicine 2021, 100, e25352. [Google Scholar] [CrossRef]
- Birlutiu, V.; Feiereisz, A.I.; Oprinca, G.; Dobritoiu, S.; Rotaru, M.; Birlutiu, R.M.; Iancu, G.M. Cutaneous manifestations associated with anosmia, ageusia and enteritis in SARS-CoV-2 infection—A possible pattern? Observational study and review of the literature. Int. J. Infect. Dis. 2021, 107, 72–77. [Google Scholar] [CrossRef]
- Iancu, G.M.; Solomon, A.; Birlutiu, V. Viral exanthema as manifestation of SARS-CoV-2 infection: A case report. Medicine 2020, 99, e21810. [Google Scholar] [CrossRef]
- McMahon, D.E.; Gallman, A.E.; Hruza, G.J.; Rosenbach, M.; Lipoff, J.B.; Desai, S.R.; French, L.E.; Lim, H.; Cyster, J.G.; Fox, L.P.; et al. Long COVID in the skin: A registry analysis of COVID-19 dermatological duration. Lancet Infect. Dis. 2021, 21, 313–314. [Google Scholar] [CrossRef]
- Galván Casas, C.; Català, A.; Carretero Hernández, G.; Rodríguez-Jiménez, P.; Fernández-Nieto, D.; Rodríguez-Villa Lario, A.; Navarro Fernández, I.; Ruiz-Villaverde, R.; Falkenhain-López, D.; Llamas Velasco, M.; et al. Classification of the cutaneous manifestations of COVID-19: A rapid prospective nationwide consensus study in Spain with 375 cases. Br. J. Dermatol. 2020, 183, 71–77. [Google Scholar] [CrossRef]
- Kumar, T.; Dutta, S.; Sahai, R.; Khasbage, S.; Kumar, R.; Banerjee, S. Dermatological Manifestations of COVID-19: A Review Based on Existing Reports. Int. J. Cur Res. Rev. 2020, 12, 65–68. [Google Scholar] [CrossRef]
- Sahara, T.; Yokota, K. Livedo reticularis associated with COVID-19. Intern. Med. 2022, 61, 441. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, L.; Nisticò, S.P.; Dastoli, S.; Provenzano, E.; Napolitano, M.; Silvestri, M.; Passante, M.; Patruno, C. Erythema Multiforme and COVID-19: What Do We Know? Medicina 2021, 57, 828. [Google Scholar] [CrossRef] [PubMed]
- Marzano, A.V.; Genovese, G.; Fabbrocini, G.; Pigatto, P.; Monfrecola, G.; Piraccini, B.M.; Veraldi, S.; Rubegni, P.; Cusini, M.; Caputo, V.; et al. Varicella-like exanthem as a specific COVID-19-associated skin manifestation: Multicenter case series of 22 patients. J. Am. Acad. Dermatol. 2020, 83, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Seirafianpour, F.; Sodagar, S.; Pour Mohammad, A.; Panahi, P.; Mozafarpoor, S.; Almasi, S.; Goodarzi, A. Cutaneous manifestations and considerations in COVID-19 pandemic: A systematic review. Dermatol. Ther. 2020, 33, e13986. [Google Scholar] [CrossRef] [PubMed]
- Potekaev, N.N.; Zhukova, O.V.; Protsenko, D.N.; Demina, O.M.; Khlystova, E.A.; Bogin, V. Clinical characteristics of dermatologic manifestations of COVID-19 infection: Case series of 15 patients, review of literature, and proposed etiological classification. Int. J. Dermatol. 2020, 59, 1000–1009. [Google Scholar] [CrossRef]
- Masood, W.; Ahmad, S.; Khan, N.A.; Shakir, A.; Rokni, G.R.; Gold, M.H.; Cockerell, C.J.; Schwartz, R.A.; Goldust, M. Pathobiology of Cutaneous Manifestations Associated with COVID-19 and Their Management. Viruses 2022, 14, 1972. [Google Scholar] [CrossRef]
- Recalcati, S. Cutaneous manifestations in COVID-19: A first perspective. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1–5. [Google Scholar] [CrossRef]
- Gargiulo, L.; Ibba, L.; Vignoli, C.A.; Piscazzi, F.; Cortese, A.; Fiorillo, G.; Toso, F.; Pavia, G.; Valent, M. New-onset and flares of psoriasis after COVID-19 infection or vaccination successfully treated with biologics: A case series. J. Dermatol. Treat. 2023, 34, 2198050. [Google Scholar] [CrossRef]
- Hussain, N.; Agarwala, P.; Iqbal, K.; Omar, H.M.S.; Jangid, G.; Patel, V.; Rathore, S.S.; Kumari, C.; Velasquez-Botero, F.; López, G.A.B.; et al. A systematic review of acute telogen effluvium, a harrowing post-COVID-19 manifestation. J. Med. Virol. 2022, 94, 1391–1401. [Google Scholar] [CrossRef]
- Monari, P.; Gualdi, G.; Bettoni, G.; Costa, R.; Ragni, G.; Zani, F.; Bianchi, G.; Casella, S.; Casella, E.; Crippa, M.; et al. Post-SARS-CoV-2 Acute Telogen Effluvium: An Expected Complication. J. Clin. Med. 2022, 11, 1234. [Google Scholar] [CrossRef]
- Inamadar, A.C. Covid Induced Telogen Effluvium (CITE): An Insight. Indian. Dermatol. Online J. 2022, 13, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Gentile, P. Hair Loss and Telogen Effluvium Related to COVID-19: The Potential Implication of Adipose-Derived Mesenchymal Stem Cells and Platelet-Rich Plasma as Regenerative Strategies. Int. J. Mol. Sci. 2022, 23, 9116. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Quispe, H.; Muñoz Moreno-Arrones, O.; Hermosa-Gelbard, A.; Vañó-Galván, S.; Saceda-Corralo, D. Trichoscopy in alopecia areata. Actas Dermo-Sifiliográficas 2023, 114, 25–32. [Google Scholar] [CrossRef]
- Pratt, C.H.; King, L.E.; Messenger, A.G.; Christiano, A.M.; Sundberg, J.P. Alopecia areata. Nat. Rev. Dis. Primers 2017, 3, 17011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, N.; Doshi, B.; Khopkar, U. Trichoscopy in alopecias: Diagnosis simplified. Int. J. Trichol. 2013, 5, 170–178. [Google Scholar]
- Fabbrocini, G.; Cantelli, M.; Masarà, A.; Annunziata, M.C.; Marasca, C.; Cacciapuoti, S. Female pattern hair loss: A clinical, pathophysiologic, and therapeutic review. Int. J. Womens Dermatol. 2018, 4, 203–211. [Google Scholar] [CrossRef]
- Pomsoong, C.; Sukanjanapong, S.; Ratanapokasatit, Y.; Suchonwanit, P. Epidemiological, Clinical, and Trichoscopic Features of Syphilitic Alopecia: A Retrospective Analysis and Systematic Review. Front. Med. 2022, 9, 890206. [Google Scholar] [CrossRef]
- Bi, M.Y.; Cohen, P.R.; Robinson, F.W.; Gray, J.M. Alopecia syphilitica-report of a patient with secondary syphilis presenting as moth-eaten alopecia and a review of its common mimickers. Dermatol. Online J. 2009, 15, 6. [Google Scholar] [CrossRef]
- Kumar, P.; Pandhi, D.; Bhattacharya, S.N.; Das, S. Trichoscopy as a Diagnostic Tool for Tinea Capitis: A Prospective, Observational Study. Int. J. Trichology 2020, 12, 68–74. [Google Scholar]
- Hay, R.J. Tinea Capitis: Current Status. Mycopathologia 2017, 182, 87–93. [Google Scholar] [CrossRef] [Green Version]
- Pate, S.; Tosti, A. An overview of management of drug-induced hair and nail disorders. Clin. Pract. 2014, 11, 327–339. [Google Scholar] [CrossRef]
- Kaczorowska, A.; Rudnicka, L.; Stefanato, C.M.; Waskiel-Burnat, A.; Warszawik-Hendzel, O.; Olszewska, M.; Rakowska, A. Diagnostic Accuracy of Trichoscopy in Trichotillomania: A Systematic Review. Acta Derm. Venereol. 2021, 101, adv00565. [Google Scholar] [CrossRef] [PubMed]
- Pereyra, A.D.; Saadabadi, A. Trichotillomania. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493186/ (accessed on 10 June 2023).
- Seyfi, S.; Alijanpour, R.; Aryanian, Z.; Ezoji, K.; Mahmoudi, M. Prevalence of telogen effluvium hair loss in COVID-19 patients and its relationship with disease severity. J. Med. Life 2022, 15, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Abrantes, T.F.; Artounian, K.A.; Falsey, R.; Simão João, C.L.; Vañó-Galván, S.; Ferreira, S.B.; Davis, T.L.; Ridenour, W.; Goren, A.; Tosti, A.; et al. Time of onset and duration of post-COVID-19 acute telogen effluvium. J. Am. Acad. Dermatol. 2021, 85, 975–976. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Arrones, O.M.; Lobato-Berezo, A.; Gomez-Zubiaur, A.; Arias-Santiago, S.; Saceda-Corralo, D.; Bernardez-Guerra, C.; Grimalt, R.; Fernandez-Crehuet, P.; Ferrando, J.; Gil, R.; et al. SARS-CoV-2-induced telogen effluvium: A multicentric study. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e181–e183. [Google Scholar] [CrossRef] [PubMed]
- Bostan, E.; Cakir, A. Effect of COVID-19 on Hair Diseases Observed by Health Care Providers: Analysis of 513 participants. Dermatol. Pract. Concept. 2023, 13, e2023036. [Google Scholar] [CrossRef]
- Aksoy, H.; Yıldırım, U.M.; Ergen, P.; Gürel, M.S. COVID-19 induced telogen effluvium. Dermatol. Ther. 2021, 34, e15175. [Google Scholar] [CrossRef] [PubMed]
- Czech, T.; Sugihara, S.; Nishimura, Y. Characteristics of hair loss after COVID-19: A systematic scoping review. J. Cosmet. Dermatol. 2022, 21, 3655–3662. [Google Scholar] [CrossRef]
- Leach, D.A.; Mohr, A.; Giotis, E.S.; Cil, E.; Isac, A.M.; Yates, L.L.; Barclay, W.S.; Zwacka, R.M.; Bevan, L.; Brooke, G.N. The antiandrogen enzalutamide downregulates TMPRSS2 and reduces cellular entry of SARS-CoV-2 in human lung cells. Nat. Commun. 2021, 12, 4068. [Google Scholar] [CrossRef]
- Koç Yıldırım, S.; Erbağcı, E.; Demirel Öğüt, N. Evaluation of patients with telogen effluvium during the pandemic: May the monocytes be responsible for post COVID-19 telogen effluvium? J. Cosmet. Dermatol. 2022, 21, 1809–1815. [Google Scholar] [CrossRef]
- Starace, M.; Iorizzo, M.; Sechi, A.; Alessandrini, A.M.; Carpanese, M.; Bruni, F.; Vara, G.; Apalla, Z.; Asz-Sigall, D.; Barruscotti, S.; et al. Trichodynia and telogen effluvium in COVID-19 patients: Results of an international expert opinion survey on diagnosis and management. JAAD Int. 2021, 5, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Watras, M.M.; Patel, J.P.; Arya, R. Traditional Anticoagulants and Hair Loss: A Role for Direct Oral Anticoagulants? A Review of the Literature. Drugs Real World Outcomes 2016, 3, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alharbi, M. Telogen effluvium after COVID-19 vaccination among public in Saudi Arabia. J. Family Med. Prim. Care 2022, 11, 6056–6060. [Google Scholar] [CrossRef]
- Rotaru, M.; Iancu, G.; Farhat, R. Androgenetic Alopecia: Predictive Factor for COVID-19 severity. EMJ Dermatol. 2021, 9, 51–52, abstract review no.AR1. [Google Scholar]
- Popescu, M.N.; Berteanu, M.; Beiu, C.; Popa, L.G.; Mihai, M.M.; Iliescu, M.G.; Stănescu, A.M.A.; Ionescu, A.M. Complementary Strategies to Promote Hair Regrowth in Post-COVID-19 Telogen Effluvium. Clin. Cosmet. Investig. Dermatol. 2022, 15, 735–743. [Google Scholar] [CrossRef]
- Mahadi, A.R.; Rafi, M.A.; Shahriar, T.; Seemanta, S.; Rabbani, M.G.; Akter, M.; Majumder, M.I.; Hasan, M.T. Association between Hair Diseases and COVID-19 Pandemic-Related Stress: A Cross-Sectional Study Analysis. Front. Med. 2022, 9, 876561. [Google Scholar] [CrossRef]
- Olds, H.; Liu, J.; Luk, K.; Lim, H.W.; Ozog, D.; Rambhatla, P.V. Telogen effluvium associated with COVID-19 infection. Dermatol. Ther. 2021, 34, e14761. [Google Scholar] [CrossRef] [PubMed]
- Saki, N.; Aslani, F.S.; Sepaskhah, M.; Shafiei, M.; Alavizadeh, S.; Hosseini, S.A.; Asl, F.A.; Ahramiyanpour, N. Intermittent chronic telogen effluvium with an unusual dermoscopic finding following COVID-19. Clin. Case Rep. 2022, 10, e6228. [Google Scholar] [CrossRef]
- Lv, S.; Wang, L.; Zou, X.; Wang, Z.; Qu, B.; Lin, W.; Yang, D. A Case of Acute Telogen Effluvium after SARS-CoV-2 Infection. Clin. Cosmet. Investig. Dermatol. 2021, 14, 385–387. [Google Scholar] [CrossRef]
- Rizzeto, G.; Diotallevi, F.; Campanati, A.; Radi, G.; Binachelli, T.; Molinelli, E.; Mazzanti, S.; Offdani, A. Telogen effluvium related to post severe SARS-CoV-2 infection: Clinical aspects and our management experience. Dermatol. Ther. 2021, 34, e14547. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Authors | Years | Number of Patients | Treatment Options |
|---|---|---|---|---|
| 1. | Ohyama et al. [1] | 2022 | Meta-analysis | Oral or topical minoxidil Oral supplements with biotin, iron, and vitamin D Iontophoresis with growth factors Microneedles |
| 2. | Hussain et al. [19] | 2022 | 465 (meta-analysis) | Oral supplements with sulfur amino acid/vitamin B6, iron, and vitamin D |
| 3. | Saki et al. [49] | 2022 | 1 | Oral supplements with vitamin D3 Intramuscular biotin |
| 4. | Lv et al. [50] | 2022 | 1 | Topical minoxidil 5% Topical halcinonide lotion Shampoo with selenium sulfide |
| 5. | Olds et al. [48] | 2021 | 10 | Oral supplements with biotin, iron, and vitamin D Topical minoxidil 5% Topical corticosteroids |
| 6. | Rizzeto et al. [51] | 2021 | 3 | Oral supplements with sulfur amino acid/vitamin B6 Topical peptide (hair growth factor-like) Topical minoxidil 5% |
| 7. | Rossi et al. [4] | 2021 | 14 | Oral supplements with biotin, alpha-lipoic acid, iron, vitamin D3 and B5, and topical corticosteroids |
| 8. | Starace et al. [42] | 2021 | 128 | Oral supplements with amino acids and vitamins Topical corticosteroids Topical minoxidil Topical hair growth promoters |
| 9. | Moreno-Arrones et al. [36] | 2020 | 214 (meta-analysis) | Oral or topical minoxidil (2% or 5%) Oral supplements Platelet-rich plasma treatment |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iancu, G.M.; Molnar, E.; Ungureanu, L.; Șenilă, S.C.; Hașegan, A.; Rotaru, M. SARS-CoV-2 Infection—A Trigger Factor for Telogen Effluvium: Review of the Literature with a Case-Based Guidance for Clinical Evaluation. Life 2023, 13, 1576. https://doi.org/10.3390/life13071576
Iancu GM, Molnar E, Ungureanu L, Șenilă SC, Hașegan A, Rotaru M. SARS-CoV-2 Infection—A Trigger Factor for Telogen Effluvium: Review of the Literature with a Case-Based Guidance for Clinical Evaluation. Life. 2023; 13(7):1576. https://doi.org/10.3390/life13071576
Chicago/Turabian StyleIancu, Gabriela Mariana, Estera Molnar, Loredana Ungureanu, Simona Corina Șenilă, Adrian Hașegan, and Maria Rotaru. 2023. "SARS-CoV-2 Infection—A Trigger Factor for Telogen Effluvium: Review of the Literature with a Case-Based Guidance for Clinical Evaluation" Life 13, no. 7: 1576. https://doi.org/10.3390/life13071576