
The Diagnostic Performance of a Clinical Diagnosis of Diabetic Kidney Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Diagnosis of DKD and NDKD
2.2.1. Clinical Diagnosis of DKD and NDKD
2.2.2. Biopsy Diagnosis of DKD and NDKD
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
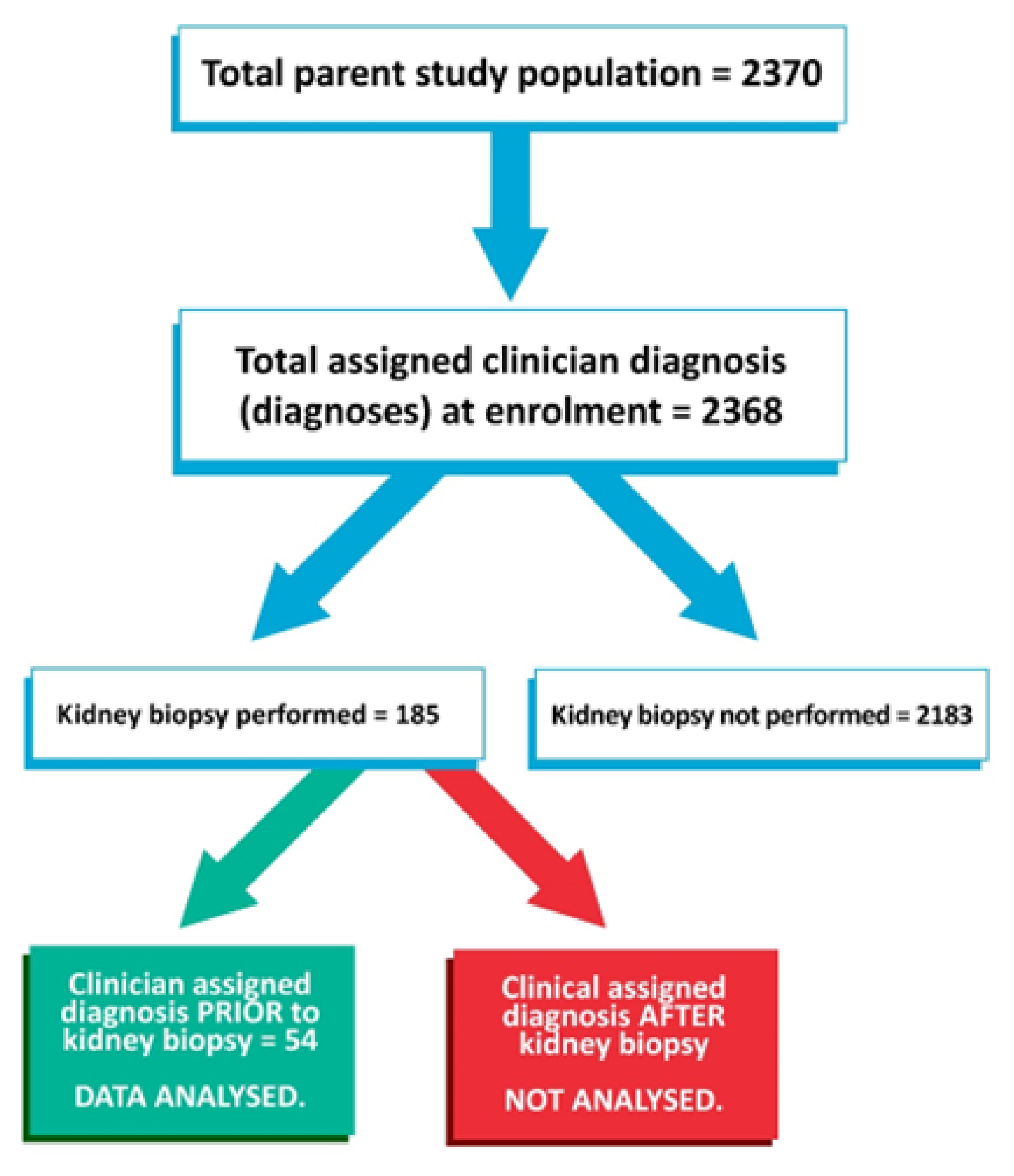
3.1. Overview of Study Population and Flow
3.2. Baseline Characteristics
- Cardiac:
- Acute coronary syndrome.
- Coronary revascularization event—elective or emergency (but not including diagnostic angiogram).
- Heart failure.
- Cerebrovascular:
- Cerebrovascular accident (not including transient ischaemic attack).
- Carotid artery revascularization (elective or emergency).
- Other vascular:
- Gangrene requiring limb/digit amputation.
- Peripheral artery revascularization procedure (elective/emergency) not including diagnostic angiogram.
- Aortic aneurysm hospitalization for rupture or leak or repair (elective or emergency)—not including incidental discovery during admission or outpatient clinic review.
- Bowel infarction—confirmed via the histology of resected bowel or relevant history and imaging (if managed conservatively).
3.3. Biopsy Diagnoses
3.4. Diagnostic Performance of Clinically Diagnosed DKD
- Excluding four patients with a second listed clinical diagnosis of DKD (presuming that these were patients in whom there was less confidence in the diagnosis)—the results are summarized in Table 5.Sensitivity (97.1%), positive predictive value (83.2%), negative predictive value (93.2%), and diagnostic accuracy (85.9%) were essentially unchanged, although specificity (66.7%) had improved somewhat.
- Excluding the 14 patients who had DKD as a shared pathology at biopsy—the results are summarized in Table 5.Sensitivity and negative predictive value had increased to 100%, whilst positive predictive value had improved to 86.1%. Specificity remained steady at 62.5%, as did diagnostic accuracy at 86.1%.
3.5. Associations of Biopsy Diagnosis with Proteinuria
3.6. Associations of Biopsy Diagnosis with Microscopic Haematuria
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IDF Diabetes Atlas. International Diabetes Federation; c2022; IDF Diabetes Atlas 2021. International Diabetes Federation, Brussels, Belgium. Available online: https://diabetesatlas.org/atlas/tenth-edition/ (accessed on 28 May 2023).
- American Diabetes Association Professional Practice Committee. Chronic kidney disease and risk management: Standards of medical care in Diabetes. Diabetes Care 2022, 45 (Suppl. S1), S175–S184. [Google Scholar] [CrossRef] [PubMed]
- Tervaert, T.W.C.; Mooyaart, A.L.; Amann, K.; Cohen, A.H.; Cook, H.T.; Drachenberg, C.B.; Bruijn, J.A. Pathologic classification of diabetic nephropathy. J. Am. Soc. Nephrol. 2010, 21, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Fiorentino, M.; Bolignano, D.; Tesar, V.; Pisano, A.; Van Biesen, W.; Tripepi, G.; ERA-EDTA Immunonephrology Working Group. Renal biopsy in patients with diabetes: A pooled meta-analysis of 48 studies. Nephrol. Dial. Transpl. 2017, 32, 97–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biesenbach, G.; Bodlaj, G.; Pieringer, H.; Sedlak, M. Clinical versus histological diagnosis of diabetic nephropathy—Is renal biopsy required in type 2 diabetic patients with renal disease? QJM Int. J. Med. 2011, 104, 771–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, K.; Akai, Y.; Sumida, K.; Yoshikawa, M.; Takahashi, H.; Yamaguchi, Y.; Saito, Y. Significance of renal biopsy in patients with presumed diabetic nephropathy. J. Diabetes Investig. 2013, 4, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Tong, X.; Yu, Q.; Ankawi, G.; Pang, B.; Yang, B.; Yang, H. Insights into the role of renal biopsy in patients with T2DM: A literature review of global renal biopsy results. Diabetes Ther. 2020, 11, 1938–1999. [Google Scholar] [CrossRef]
- Venuthurupalli, S.K.; Hoy, W.E.; Healy, H.G.; Cameron, A.; Fassett, R.G. CKD.QLD: Establishment of a chronic kidney disease [CKD] registry in Queensland, Australia. BMC Nephrol. 2017, 18, 189. [Google Scholar] [CrossRef]
- Venuthurupalli, S.K.; Hoy, W.E.; Healy, H.G.; Salisbury, A.; Fasset, R.G. CKD.QLD: Chronic kidney disease surveillance and research in Queensland Australia. Nephrol. Dial. Transpl. 2012, 27 (Suppl. S3), iii139–iii145. [Google Scholar] [CrossRef] [Green Version]
- ANZDATA Registry. Adelaide SA: ANZDATA; c2022; New Patient Registration Form. Australia and New Zealand Dialysis and Transplant Registry, Adelaide, Australia. 2022. Available online: https://www.anzdata.org.au/anzdata/services/data-management/data-forms/ (accessed on 21 June 2022).
- Mercaldo, N.D.; Lau, K.F.; Zhou, X.H. Confidence intervals for predictive values with an emphasis to case-control studies. Stat. Med. 2007, 26, 2170–2183. [Google Scholar] [CrossRef]
- Phamaceutical Benefits Scheme. Commonwealth of Australia; c2023; Dapagliflozin, Tablet, 10mg Forxiga®—July 2013. Australian Department of Health and Aged Care, Canberra, Australia. 2013. Available online: https://www.pbs.gov.au/pbs/industry/listing/elements/pbac-meetings/psd/2013-07/dapagliflozin (accessed on 17 June 2023).
- NPS Medicinewise. NPS MedicineWise; c2022; SGLT2 Inhibitor Listings: Indications and Combinations. Australian Commission on Safety and Quality in Health Care, Sydney, Australia. 1 April 2015. Available online: https://www.nps.org.au/radar/articles/sglt2-inhibitor-listings-indications-and-combinations (accessed on 17 June 2023).
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 3, 19–150. [Google Scholar]
- Singh, S.; Patel, P.S.; Archana, A. Heterogeneity in Kidney Histology and Its Clinical Indicators in Type 2 Diabetes Mellitus: A Retrospective Study. J. Clin. Med. 2023, 12, 1778. [Google Scholar] [CrossRef]
- Basu, M.; Pulai, S.; Neogi, S.; Banerjee, M.; Bhattacharya, N.P.; Sengupta, S.; Ghosh, S. Prevalence of non-diabetic kidney disease and inability of clinical predictors to differentiate it from diabetic kidney disease: Results from a prospectively performed renal biopsy study. BMJ Open Diabetes Res. Care 2022, 10, e003058. [Google Scholar] [CrossRef]
- Zeng, Y.; Yang, Y.; Guan, C.; Guo, Z.; Li, B.; Yu, H.Y.; Yan, R. Clinical predictors for nondiabetic kidney diseases in patients with type 2 diabetes mellitus: A retrospective study from 2017 to 2021. BMC Endocr. Disord. 2022, 22, 168. [Google Scholar] [CrossRef]
- Chemouny, J.M.; Bobot, M.; Sannier, A.; Maisons, V.; Jourde-Chiche, N.; Ferriere, E.; Vrtovsnik, F. Kidney biopsy in type 2 diabetes: A multicenter cross-sectional study. Am. J. Nephrol. 2021, 52, 131–140. [Google Scholar] [CrossRef]
- Sanghavi, S.; Roark, T.; Zelnick, L.R.; Najafian, B.; Nadeen, N.K.; Alpers, C.E.; de Boer, I.H. Histopathologic and Clinical Features in Patients with Diabetes and Kidney Disease. Kidney360 2020, 1, 1217–1225. [Google Scholar] [CrossRef]
- Bermejo, S.; González, E.; López-Revuelta, K.; Ibernon, M.; López, D.; Martín-Gómez, A.; Soler, M.J. Risk factors for non-diabetic renal disease in diabetic patients. Clin. Kidney J. 2020, 13, 380–388. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.Z.; Choo, J.C.J.; Fook-Chong, S.; Chin, Y.M.; Chan, C.M.; Tan, C.S.; Kwek, J.L. Development and validation of a novel nomogram to predict diabetic kidney disease in patients with type 2 diabetic mellitus and proteinuric kidney disease. Int. Urol. Nephrol. 2023, 55, 191–200. [Google Scholar] [CrossRef]
- Hui, D.; Sun, Y.; Xu, S.; Liu, J.; He, P.; Deng, Y.; Li, R. Analysis of clinical predictors of kidney diseases in type 2 diabetes patients based on machine learning. Int. Urol. Nephrol. 2023, 55, 687–696. [Google Scholar] [CrossRef]
- Zhou, D.; Wei, J.; Zhang, T.; Shen, F.; Yang, J. Establishment and validation of a nomogram model for prediction of diabetic nephropathy in type 2 diabetic patients with proteinuria. Diabetes Metab. Syndr. Obes. 2022, 15, 1101–1110. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.F.; Wheeler, D.C. Dapagliflozin in patients with CKD. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Stefansson, B.V.; Batiushin, M.; Bilchenko, O.; Cherney, D.Z.I.; Chertow, G.M.; Heerspink, H.J. The dapagliflozin and prevention of adverse outcomes in chronic kidney disease (DAPA-CKD) trial: Baseline characteristics. Nephrol. Dial. Transpl. 2020, 35, 1700–1711. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.C.; Stefánsson, B.V.; Jongs, N.; Chertow, G.M.; Greene, T.; Hou, F.F.; Heerspink, H.J. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: A prespecified analysis from the DAPA-CKD trial. Lancet Diabetes Endocrinol. 2021, 9, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Corapi, K.M.; Chen, J.L.; Balk, E.M.; Gordon, C.E. Bleeding complications of native kidney biopsy: A systematic review and meta-analysis. Am. J. Kidney Dis. 2012, 60, 62–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorentino, M.; Bolignano, D.; Tesar, V.; Pisano, A.; Van Biesen, W.M.; D’Arrigo, G.; ERA-EDTA Immunonephrology Working Group. Renal biopsy in 2015—From epidemiology to evidence-based indications. Am. J. Nephrol. 2016, 43, 1–19. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Summary Statistic Value |
|---|---|
| Age (years) | Mean 58.2 (SD 11.5) |
| Gender | Male = 27 (50%) |
| BMI (information available for 46 patients) | Median 32.1 (IQR 30.2; 36.7) |
| Treatment for DM | |
| Insulin (+/− a oral hypoglycaemic agent (OHA)) | 32 (59.3%) |
| OHA only | 18 (33.3%) |
| Diet only | 4 (7.4%) |
| DM type 1 | 6 (11.1%) |
| HbA1c | Median 7.4% (IQR 6.6; 8.8) |
| CKD-EPI eGFR (mL/min/1.73 m2) | Median 38.5 (IQR 29; 50) |
| b Proteinuria category | |
| 1 (albumin:creatinine (ACR) < 3 or protein:creatinine < 15 mg/mmol) | 4 (7.4%) |
| 2 (ACR ≥ 3 but <30 or protein:creatinine ≥ 15 but <50 mg/mmol) | 4 (7.4%) |
| 3 (ACR ≥ 30 but <220 or protein:creatinine ≥ 50 but <300 mg/mmol) | 20 (37.0%) |
| 4 (ACR ≥ 220 or protein:creatinine ≥ 300 mg/mmol) | 26 (48.1%) |
| c RAAS blocker therapy | 50 (92.6%) |
| Clinical diagnosis includes DKD | 43 (79.6%) |
| Hypertension (information available for 52 patients) | 44 (84.6%) |
| d Previous history of MACE at enrolment | 15 (27.8%) |
| Co-Existing Pathology | n (Total = 14) |
|---|---|
| Secondary FSGS | 5 |
| IgA nephropathy | 2 |
| ANCA associated vasculitis (microscopic polyangiitis). | 2 |
| Membranoproliferative/mesangiocapillary GN (type 1) | 1 |
| Hypertensive nephrosclerosis. | 1 |
| Immunoglobulin light chain deposition disease | 1 |
| Sjogren’s syndrome | 1 |
| Lupus nephritis (ISN/RPN Class III) | 1 |
| NDKD Pathology | n (Total = 16) |
|---|---|
| a FSGS | 4 |
| Acute tubular necrosis | 3 |
| Hypertensive nephrosclerosis. | 1 |
| IgA nephropathy | 2 |
| Membranoproliferative/mesangiocapillary GN (type not specified) | 1 |
| Myeloma | 1 |
| Acute interstitial nephritis | 1 |
| Ischaemic nephrosclerosis | 2 |
| Anti-glomerular basement membrane disease | 1 |
| DKD Present at Biopsy | Biopsy-Proven NDKD Only | |
|---|---|---|
| Clinically diagnosed DKD | 37 | 6 |
| Clinically diagnosed NDKD | 1 | 10 |
| Sensitivity analysis 1: Excluding patients with DKD as second listed clinical diagnosis (n = 50). | DKD present at biopsy | Biopsy proven NDKD only |
| Clinically diagnosed DKD | 34 | 5 |
| Clinically diagnosed NDKD | 1 | 10 |
| Sensitivity analysis 2: Excluding patients with DKD as a shared pathology at biopsy (n = 40). | DKD only present at biopsy | Biopsy proven NDKD only |
| Clinically diagnosed DKD | 24 | 6 |
| Clinically diagnosed DKD | 0 | 10 |
| Proteinuria Category a | DKD Present at Biopsy | Biopsy-Proven NDKD Only |
|---|---|---|
| 1 | 1 (2.6%) | 3 (18.8%) |
| 2 | 2 (5.3%) | 2 (12.5%) |
| 3 | 11 (28.9%) | 9 (56.3%) |
| 4 | 24 (63.2%) | 2 (12.5%) |
| Microscopic Haematuria Present a | DKD Present at Biopsy | Biopsy-Proven NDKD Only |
|---|---|---|
| Yes | 14 (36.8%) | 3 (18.8%) |
| No | 24 (63.2%) | 13 (81.2%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, K.-S.; McDonald, S.; Hoy, W. The Diagnostic Performance of a Clinical Diagnosis of Diabetic Kidney Disease. Life 2023, 13, 1492. https://doi.org/10.3390/life13071492
Tan K-S, McDonald S, Hoy W. The Diagnostic Performance of a Clinical Diagnosis of Diabetic Kidney Disease. Life. 2023; 13(7):1492. https://doi.org/10.3390/life13071492
Chicago/Turabian StyleTan, Ken-Soon, Stephen McDonald, and Wendy Hoy. 2023. "The Diagnostic Performance of a Clinical Diagnosis of Diabetic Kidney Disease" Life 13, no. 7: 1492. https://doi.org/10.3390/life13071492