

Is There Still a Place for Surgery in Patients with PCOS? A Review
 , , ,
, , ,
Abstract
:1. Introduction
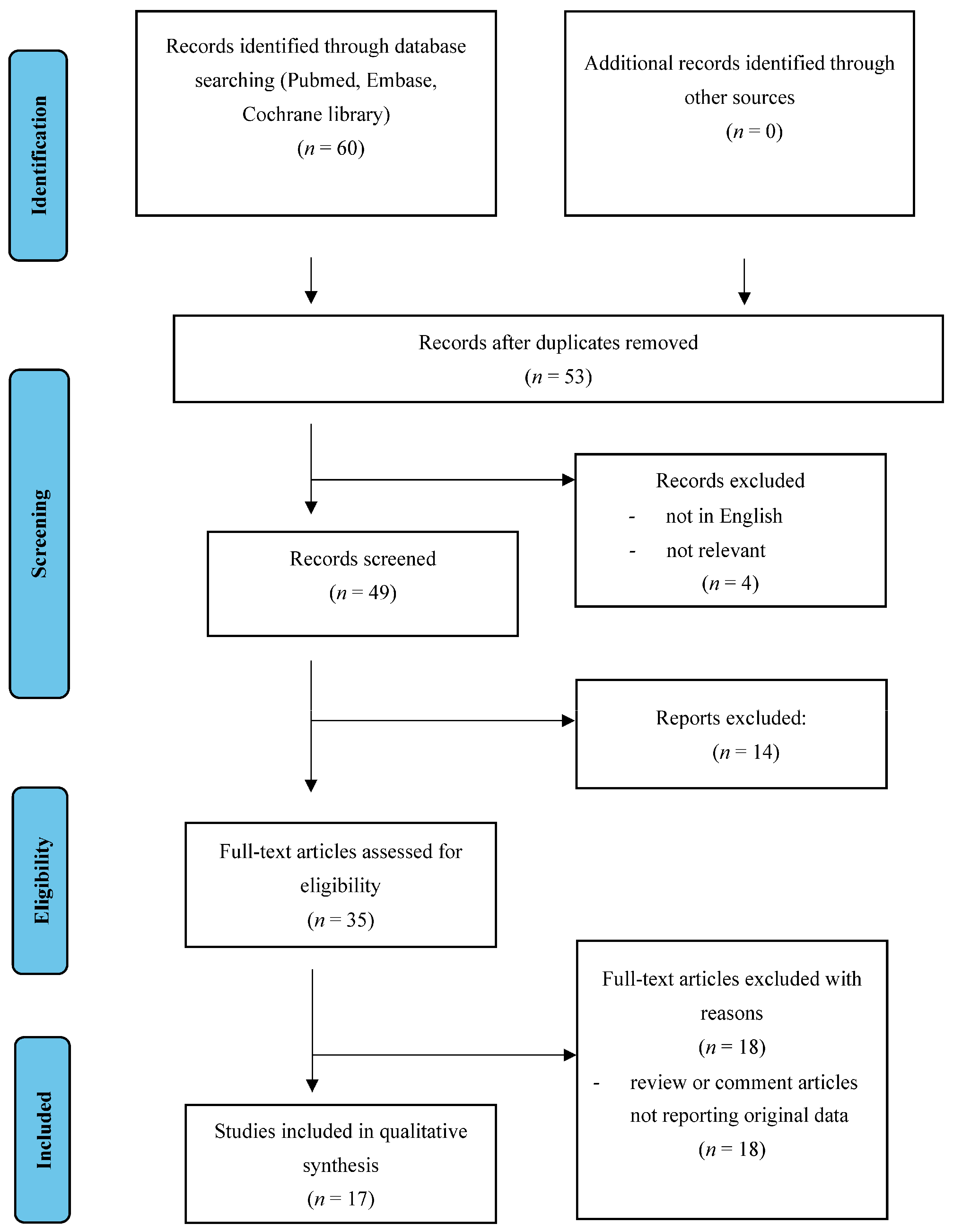
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wołczyński, S.; Zgliczyński, W. Abnormalities of the menstrual cycle. In Large Interna—Endocrinology, 2nd ed.; Medical Tribune: Warsaw, Poland, 2012; pp. 561–567. [Google Scholar]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Giampaolino, P.; Della Corte, L.; De Rosa, N.; Mercorio, A.; Bruzzese, D.; Bifulco, G. Ovarian volume and PCOS: A controversial issue. Gynecol. Endocrinol. 2017, 34, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Milewicz, A. Reimbursement of metformin for polycystic ovary syndrome. Endokrynol. Pol. 2013, 64, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Traub, M.L. Assessing and treating insulin resistance in women with polycystic ovarian syndrome. World J. Diabetes 2011, 2, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Fica, S.; Albu, A.; Constantin, M.; Dobri, G. Insulin resistance and fertility in polycystic ovary syndrome. J. Med. Life 2008, 1, 415–422. [Google Scholar]
- Krępuła, K.; Bidzińska-Speichert, B.; Lenarcik, A.; Tworowska-Bardzińska, U. Psychiatric disorders related to polycystic ovary syndrome. Endokrynol. Pol. 2012, 63, 488–491. [Google Scholar]
- Oppelt, P.G.; Mueller, A.; Jentsch, K.; Kronawitter, D.; Reissmann, C.; Dittrich, R.; Beckmann, M.W.; Cupisti, S. The Effect of metformin treatment for 2 years without caloric restriction on endocrine and metabolic parameters in women with polycystic ovary syndrome. Exp. Clin. Endocrinol. Diabetes 2009, 118, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Balen, A.H.; Morley, L.C.; Misso, M.; Franks, S.; Legro, R.S.; Wijeyaratne, C.N.; Stener-Victorin, E.; Fauser, B.C.; Norman, R.J.; Teede, H. The management of anovulatory infertility in women with polycystic ovary syndrome: An analysis of the evidence to support the development of global WHO guidance. Hum. Reprod. Update 2016, 22, 687–708. [Google Scholar] [CrossRef]
- Mercorio, A.; Della Corte, L.; De Angelis, M.C.; Buonfantino, C.; Ronsini, C.; Bifulco, G.; Giampaolino, P. Ovarian Drilling: Back to the Future. Medicina 2022, 58, 1002. [Google Scholar] [CrossRef]
- Seow, K.-M.; Chang, Y.-W.; Chen, K.-H.; Juan, C.-C.; Huang, C.-Y.; Lin, L.-T.; Tsui, K.-H.; Chen, Y.-J.; Lee, W.-L.; Wang, P.-H. Molecular Mechanisms of Laparoscopic Ovarian Drilling and Its Therapeutic Effects in Polycystic Ovary Syndrome. Int. J. Mol. Sci. 2020, 21, 8147. [Google Scholar] [CrossRef]
- Lebbi, I.; Ben Temime, R.; Fadhlaoui, A.; Feki, A. Ovarian Drilling in PCOS: Is it Really Useful? Front. Surg. 2015, 2, 30. [Google Scholar] [CrossRef] [PubMed]
- Giampaolino, P.; Morra, I.; Della Corte, L.; Sparice, S.; Di Carlo, C.; Nappi, C.; Bifulco, G. Serum anti-Mullerian hormone levels after ovarian drilling for the second-line treatment of polycystic ovary syndrome: A pilot-randomized study comparing lapa-roscopy and transvaginal hydrolaparoscopy. Gynecol. Endocrinol. 2017, 33, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A scale for the quality assessment of narrative review articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef]
- Gjønnaess, H. Ovarian electrocautery in the treatment of women with polycystii ovary syndrome (PCOS): Factors affecting the results. Acta Obstet. Gynecol. Scand. 1994, 73, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Li, T.C.; Saravelos, H.; Chow, M.S.; Chisabingo, R.; Cooke, I.D. Factors affecting the outcome of laparoscopic ovarian drilling for polycystic ovarian syndrome in women with anovulatory infertility. BJOG Int. J. Obstet. Gynaecol. 1998, 105, 338–344. [Google Scholar] [CrossRef]
- Kriplani, A.; Manchanda, R.; Agarwal, N.; Nayar, B. Laparoscopic ovarian drilling in clomiphene citrate-resistant women with polycystic ovary syndrome. J. Am. Assoc. Gynecol. Laparosc. 2001, 8, 511–518. [Google Scholar] [CrossRef]
- Fernandez, H.; Alby, J.-D.; Gervaise, A.; de Tayrac, R.; Frydman, R. Operative transvaginal hydrolaparoscopy for treatment of polycystic ovary syndrome: A new minimally invasive surgery. Fertil. Steril. 2001, 75, 607–611. [Google Scholar] [CrossRef]
- Al-Ojaimi, E.H. Laparoscopic Ovarian Drilling for Polycystic Ovarian Syndrome in Clomiphene Citrate-Resistant Women with Anovulatory Infertility. Bahrain Med. Bull. 2003, 2, 1–14. [Google Scholar]
- Duleba, A.J.; Banaszewska, B.; Spaczynski, R.Z.; Pawelczyk, L. Success of laparoscopic ovarian wedge resection is related to obesity, lipid profile, and insulin levels. Fertil. Steril. 2003, 79, 1008–1014. [Google Scholar] [CrossRef]
- Stegmann, B.J.; Craig, H.R.; Bay, R.C.; Coonrod, D.V.; Brady, M.J.; Garbaciak, J.A., Jr. Characteristics predictive of response to ovarian diathermy in women with polycystic ovarian syndrome. Am. J. Obstet. Gynecol. 2003, 188, 1171–1173. [Google Scholar] [CrossRef]
- Amer, S.A.; Li, T.C.; Ledger, W.L. Ovulation induction using laparoscopic ovarian drilling in women with polycystic ovarian syndrome: Predictors of success. Hum. Reprod. 2004, 19, 1719–1724. [Google Scholar] [CrossRef] [PubMed]
- Van Wely, M.; Bayram, N.; van der Veen, F.; Bossuyt, P.M. Predictors for treatment failure after laparoscopic electrocautery of the ovaries in women with clomiphene citrate resistant polycystic ovary syndrome. Hum. Reprod. 2005, 20, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Falbo, A.; Orio, F., Jr.; Russo, T.; Sbano, F.; D’Alessandro, P.; Cariati, F.; Tolino, A.; Colao, A.; Zullo, F. Efficacy of laparoscopic ovarian diathermy in clomiphene citrate-resistant women with polycystic ovary syndrome: Relationships with chronological and ovarian age. Gynecol. Endocrinol. 2006, 22, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Amer, S.A.; Li, T.C.; Ledger, W.L. The value of measuring anti-Mullerian hormone in women with anovulatory polycystic ovary syndrome undergoing laparoscopic ovarian diathermy. Hum. Reprod. 2009, 24, 2760–2766. [Google Scholar] [CrossRef]
- Gordts, S.; Puttemans, P.; Valkenburg, M.; Campo, R.; Brosens, I. Transvaginal hydrolaparoscopy in the treatment of polycystic ovary syndrome. Fertil. Steril. 2009, 91, 2520–2526. [Google Scholar] [CrossRef]
- Ott, J.; Wirth, S.; Nouri, K.; Kurz, C.; Mayerhofer, K.; Huber, J.C.; Tempfer, C.B. Luteinizing hormone and androstendione are independent predictors of ovulation after laparoscopic ovarian drilling: A retrospective cohort study. Reprod. Biol. Endocrinol. 2009, 7, 153. [Google Scholar] [CrossRef]
- Kaur, M.; Pranesh, G.; Mittal, M.; Gahlan, A.; Deepika, K.; Shashikala, T.; Rao, K. Outcome of Laparoscopic Ovarian Drilling in Patients of Clomiphene Resistant Polycystic Ovarian Syndrome in a Tertiary Care Center. Int. J. Infertil. Fetal Med. 2013, 4, 39–44. [Google Scholar] [CrossRef]
- Giampaolino, P.; De Rosa, N.; Della Corte, L.; Morra, I.; Mercorio, A.; Nappi, C.; Bifulco, G. Operative transvaginal hydrolaparoscopy improve ovulation rate after clomiphene failure in polycystic ovary syndrome. Gynecol. Endocrinol. 2017, 34, 32–35. [Google Scholar] [CrossRef]
- Gordts, S.; Puttemans, P.; Segaert, I.; Valkenburg, M.; Campo, R. Systematic use of transvaginal hydrolaparoscopy as a minimally invasive procedure in the exploration of the infertile patient: Results and reflections. Facts Views Vis. Obgyn 2021, 13, 131–140. [Google Scholar] [CrossRef]
- Giampaolino, P.; Morra, I.; Tommaselli, G.A.; Di Carlo, C.; Nappi, C.; Bifulco, G. Post-operative ovarian adhesion formation after ovarian drilling: A randomized study comparing conventional laparoscopy and transvaginal hydrolaparoscopy. Arch. Gynecol. Obstet. 2016, 294, 791–796. [Google Scholar] [CrossRef]
- Collée, J.; Mawet, M.; Tebache, L.; Nisolle, M.; Brichant, G. Polycystic ovarian syndrome and infertility: Overview and insights of the putative treatments. Gynecol. Endocrinol. 2021, 37, 869–874. [Google Scholar] [CrossRef]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; De Rosa, P.; Strina, I.; Palomba, S.; Vallone, R.; Gizzo, S.; Borrelli, R.; Andersen, C.Y.; De Placido, G.; et al. The Distribution of Stroma and Antral Follicles Differs between Insulin-Resistance and Hyperandrogenism-Related Polycystic Ovarian Syndrome. Front. Endocrinol. 2017, 8, 117. [Google Scholar] [CrossRef]
- Dumesic, D.A.; Oberfield, S.E.; Stener-Victorin, E.; Marshall, J.C.; Laven, J.S.; Legro, R.S. Scientific Statement on the Diagnostic Criteria, Epidemiology, Pathophysiology, and Molecular Genetics of Polycystic Ovary Syndrome. Endocr. Rev. 2015, 36, 487–525. [Google Scholar] [CrossRef] [PubMed]
- Messinis, I.E.; Messini, C.I.; Anifandis, G.; Dafopoulos, K. Polycystic ovaries and obesity. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Costello, M.F.; Garad, R.M.; Hart, R.; Homer, H.; Johnson, L.; Jordan, C.; Mocanu, E.; Qiao, J.; Rombauts, L.; Teede, H.J.; et al. A Review of Second- and Third-line Infertility Treatments and Supporting Evidence in Women with Polycystic Ovary Syndrome. Med. Sci. 2019, 7, 75. [Google Scholar] [CrossRef]
- Tanbo, T.; Mellembakken, J.R.; Bjercke, S.; Ring, E.; Åbyholm, T.; Fedorcsak, P. Ovulation induction in polycystic ovary syndrome. Acta Obstet. Gynecol. Scand. 2018, 97, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Morgante, G.; Massaro, M.G.; Di Sabatino, A.; Cappelli, V.; De Leo, V. Therapeutic approach for metabolic disorders and infertility in women with PCOS. Gynecol. Endocrinol. 2017, 34, 4–9. [Google Scholar] [CrossRef]
- Wallach, E.E.; Hammond, M.G. Monitoring techniques for improved pregnancy rates during clomiphene ovulation induction. Fertil. Steril. 1984, 42, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E. Polycystic ovarian syndrome: Pathophysiology, molecular aspects and clinical implications. Expert Rev. Mol. Med. 2008, 10, e3. [Google Scholar] [CrossRef]
- Laven, J.S.E. Follicle Stimulating Hormone Receptor (FSHR) Polymorphisms and Polycystic Ovary Syndrome (PCOS). Front. Endocrinol. 2019, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, L.; Foreste, V.; Barra, F.; Gustavino, C.; Alessandri, F.; Centurioni, M.G.; Ferrero, S.; Bifulco, G.; Giampaolino, P. Current and experimental drug therapy for the treatment of polycystic ovarian syndrome. Expert Opin. Investig. Drugs 2020, 29, 819–830. [Google Scholar] [CrossRef] [PubMed]
- Giampaolino, P.; Foreste, V.; Di Filippo, C.; Gallo, A.; Mercorio, A.; Serafino, P.; Improda, F.P.; Verrazzo, P.; Zara, G.; Buonfantino, C.; et al. Microbiome and PCOS: State-of-Art and Future Aspects. Int. J. Mol. Sci. 2021, 22, 2048. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Country | Type of Study | Sample Size, n° | Age (Years—Mean ± SD or Median (Range)) | Symptoms and Signs (n—%) | BMI (kg/m2) (Mean ± SD) | Medical Treatment, (n) | Surgical Treatment | Hormonal Levels in Plasma before Treatment (Mean ± SD or Median (Range)) | Ovarian Volume (mL—Mean ± SD) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LH (IU/L) | FSH (IU/L) | LH:FSH Ratio | AMH (ng/mL) | Testosterone (nmol/L) | ||||||||||
| Gjønnaess, 1994 [15] | Norway | Retrospective study | 109 | NR | NS: oligomenorrhea and cystic glandular hyperplasia of the endometrium | 58.7 ± 6.2 | CC (109) | Ovarian electrocautery | 14.6 | 6.3 | NR | NR | 2.7 | NR |
| Li et al., 1998 [16] | Japan | Retrospective study | 111 | 28.6 ± 3.9 | 24 (22) hirsutism 80 (72) oligomenorrhea 17 (15) amenorrhea | 26.0 ± 4.8 | CC (87) | LOD | 15.4 ± 9.1 | 5.4 ± 1.9 | 2.5 ± 2.1 | NR | NR | NR |
| Kriplani et al., 2001 [17] | India | Prospective study | 70 | 26.4 | 59 (84.3) oligomenorrhea 11 (15.7) secondary amenorrhea | <29 kg/m2 in 42 (60%) | CC (70) | LOD | >10 IU/L in 42 (60%) | NR | >2 in 32 (45.7%) | NR | NR | NR |
| Fernandez et al., 2001 [18] | France | Prospective study | 13 | 28.5 ± 3.9 | 2 (15.3) hirsutism 3 (23.07) oligomenorrhea 1 (7.69) amenorrhea | 24.1 ± 4.5 | CC (12) | THL | NR | NR | 2.0 ± 0.8 | NR | NR | NR |
| Al Ojaimi, 2003 [19] | Asia | Prospective study | 198 | 30.5 ± 5.7 | 132 (66.7) oligomenorrhea 41 (20.7) amenorrhea | 29.8 | CC (184) and additional gonadotrophin therapy (72) | LOD | 13.3 ± 5.6 | 6.1 ± 3.0 | 2.3 ± 1.1 | NR | 2.4 ± 1.3 | NR |
| Duleba et al., 2003 [20] | Poland | Prospective study | 33 | 26.8 | NS: oligomenorrhea, hirsutism, or acne | 29.3 | NR | Laparoscopic ovarian wedge resection using harmonic scalpel | 13.4 | 5.9 | 2.33 | NR | 0.8 | 12.6 |
| Stegmann et al., 2003 [21] | Arizona | Prospective study | 86 | 30.2 | 49 endometriosis 54 adhesions NS hirsutism NS acanthosis | 29.35 | CC (NS) | LOD | NR | NR | 1.94 | NR | 17.39 | 4.2 (median left ovary) 4.3 (median right ovary) |
| Amer et al., 2004 [22] | UK | Prospective study | 200 | 28.9 [3.9] | 149 (74) oligomenorrhoea 36 (18) amenorrhea 70 (35) hirsutism | 27.1 ± 4.9 | CC (200) | LOD | 14.2 ± 6.6 | 5.2 ± 1.4 | 2.8 ± 1.2 | NR | 2.6 ± 1.2 | 11.4 ± 3.6 |
| Van Wely et al., 2005 [23] | Netherlands | Prospective study | 83 | 28.5 [1.0] | 35 (42.1) amenorrhea 47 (56.6) oligomenorrhea | 27 ± 6.2 | CC (83) | Ovarian electrocautery | NR | NR | NR | NR | NR | NR |
| Palomba et al., 2006 [24] | Italy | Prospective study | 60 | 29.3 [5.2] | NS | 27.6 ± 1.9 | CC (60) | LOD | 18.0 ± 4.1 | 8.9 ± 3.4 | NR | NR | 3.8 ± 1.2 | NR |
| Amer et al., 2009 [25] | UK | Prospective study | 47 | 28.4 [0.9] | NS—oligo/amenorrhea and/or hyperandrogenemia | 26.9 ± 0.6 | CC (18) | LOD (29/47) | 11.7 (4.6–23.7) | 5.1 (2.9–8.2) | 6.1 (1.0–21.0) | 2.5 (1.0–4.0) | 11.9 ± 1.1 | |
| Gordts et al., 2009 [26] | Belgium | Retrospective study | 39 | 30.4 [3.8] | NS—amenorrhea or oligomenorrhea, with or without hirsuitism | 29.4 ± 9.7 | CC (16) | THL | 15 ± 10 | 5.5 ± 2 | 2.7 | NR | 1.7 ± 1.2 | NR |
| Ott et al., 2009 [27] | Austria | Retrospective cohort study | 100 | 28.2 | NS—anovulation, oligomenorrhea, hirsutism, acne, and infertility | 26.5 | CC (100) | LOD | 15.1 (6.0) | 6.2 (1.7) | NR | NR | 0.8 (0.4) | NR |
| Kaur et al., 2013 [28] | India | Observational retrospective study | 100 | 27 [3.2] | NS- anovulation, oligomenorrhea, hirsutism, acne, and infertility | 26.6 ± 4.2 | CC (100) | LOD | NR | NR | 2.1 (1.1) | NR | NR | NR |
| Giampaolino et al., 2016 [31] | Italy | Prospective randomized study | 123 | 27.5 ± 6.8 | NR | 27.3 ± 5.6 | CC (123) | THL | NR | NR | NR | 5.84 ± 1.16 | 1.2 ± 0.3 | NR |
| 123 | 30.1 ± 7.5 | NR | 25.9 ± 7.1 | CC (123) | LOD | NR | NR | NR | 6.06 ± 1.18 | 1.6 ± 0.2 | NR | |||
| Giampaolino et al., 2017 [29] | Italy | Prospective observational study | 117 | 29.5 [3.9] | NS—oligomenorrhea and amenorrhea, hyperandrogenism, acne, hyrsutism, and androgenic alopecia | NR | CC (117) | THL | 8.85 (1.39) | 5.35 (0.71) |
1.68
(0.35) | NR | NR | 11.78 (1.61) |
| Gordts et al., 2021 [30] | Belgium | Retrospective cohort study | 2288 | 31.25 [3.8] | 366 (15.9) endometriosis 144 (6.3) adhesions | - | CC (NS) | THL | NR | NR | NR | NR | NR | NR |
| Menstrual Cycle Pattern, n (%) | Ovulation, n (%) | Pregnancy Outcomes, n (%) | Hormonal Levels in Plasma Post-LOD Treatment Mean ± SD or Median (Range) | |||||
|---|---|---|---|---|---|---|---|---|
| LH (IU/L) | FSH (IU/L) | LH/FSH Ratio | AMH (ng/mL) | Testosterone (nmol/L) | ||||
| Gjønnaess 1994 [15] | NR | 105 (96.3) | 76 (69.7) | NR | ||||
| Li et al., 1998 [16] | 160 (88) regular 23 (21) irregular | 74 (67) spontaneously 22 (20) via CC 15 (13) none | 58 (52) ongoing/delivery 7 (6) miscarriages 2 (2) ectopic 44 (40) none | 7.7 (1) vs. 10 (1.3) * | 5.6 (0.6) vs. 6.9 (1.7) * | NR | NR | NR |
| Kriplani et al., 2001 [17] | NR | 54 (81.8) spontaneously 6 (9.1) via CC 2 (3) via gonadotropins | 50 (71.4):
| NR | ||||
| Al Ojaimi et al., 2003 [19] | 160 (88.4) regular 21 (11.6) irregular | 127 (70.1) spontaneously 51 (28.2) via CC 3 (1.7) none | 120 (66.3) ongoing/delivery 31 (17.2) miscarriages 2 (1.1) ectopic 28 (15.5) none | 13.3 (5.6) | 6.1 (3.0) | 2.3 (1.1) | NR | NR |
| Duleba et al., 2003 [20] | NR | NR | 22 (67) | 8.9 (1.9) | 5.8 (0.6) | 1.4 (0.3) | NR | 0.47 (0.04) |
| Stegmann et al., 2003 [21] | 57 (66) regular | (>50) spontaneously | 43 (89.6), of which 9 by IVF 1 (2.1) ectopic 1 (2.1) triplet gestation abortion 3 (6.2) miscarriages | NR | ||||
| Amer et al., 2004 [22] | 15 (8) regular 185 (92) irregular | 113 (57) spontaneously 43 (21) by CC 44 (22) none | 86 (45) ongoing/delivery 9 (4) miscarriages 2 (1) ectopic 96 (50) none |
| NR |
| NR |
|
| Van Wely et al., 2005 [23] | NR | 38 (46) spontaneously 21 (25) via CC 24 (29) none | 41 (49) ongoing/delivery | 11.5 (5.6) | 6.1 (2.1) | 2.0 (9.6) | NR | 4.0 (1.7) |
| Palomba et al., 2006 [24] | NR | 3 (0.5%) | 33 (60) | A 19.0 (3.7) B 17.6 (4.2) C 18.1 (3.9) D 18.4 (4.9) *** | A 7.6 (1.6) B 8.6 (3.1) C 9.3 (3.4) D 10.6 (4.7) *** | NR | NR | A 3.7 (1.2) B 3.9 (3.2) C 3.8 (1.1) D 3.8 (1.3) *** |
| Amer et al., 2009 [25] | NR | 24 (83) 5 (17) none | 15 (52) | 7.9 (1.9–21.0) | 5.5 (1.7–7.7) | NR | 4.3 (0.3–15.1) | 2.2 (1.1–3.6) |
| Ott et al., 2009 [27] | NR | 71 (71) 29 (29) none | 36 (36) ongoing/delivery | 6.4 ± 4.0 | NR | NR | NR | NR |
| Kaur et al., 2013 [28] | 18 (18) regular 82 (82) irregular | NR | 35 (85.4) ongoing/delivery 5 (12.2) miscarriages 1 (2.4) ectopic | NR | NR | 2.1 ± 1.1 | NR | NR |
| Giampaolino et al., 2016 [31] | NR | NR | (68—cumulative rate) | NR | ||||
| Ovulation, n (%) | Pregnancy, n (%) | Hormonal Levels in Plasma Post-THL Treatment Mean ± SD or Median (Range) | |||||
|---|---|---|---|---|---|---|---|
| LH (IU/L) | FSH (IU/L) | LH/FSH Ratio | AMH (ng/mL) | Testosterone (nmol/L) | |||
| Fernandez et al., 2001 [18] | 6/13 (46) regular 5/13 (39) amenorrhea 2/13 (15) immediately pregnant | 6/13 (46):
| NR | ||||
| Gordts et al., 2009 [26] | 12/28 (43) spontaneously 16/18 (57) by CC plus hMG | 25/33 (76)
| 8 ± 3 | 6.1 ± 1.5 | 1.3 | NR | 1.1 ± 0.7 |
| Giampaolino et al., 2016 [31] | NR | (68—cumulative rate) | NR | ||||
| Giampaolino et al., 2017 [29] | 64.1% after 1 month 79.5% after 3 months 82.9% after 6 months | (70.1) | NR | ||||
| Gordts et al., 2021 [30] | NR | (25.6) | NR | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Corte, L.; Boccia, D.; Palumbo, M.; Mercorio, A.; Ronsini, C.; Bifulco, G.; Giampaolino, P. Is There Still a Place for Surgery in Patients with PCOS? A Review. Life 2023, 13, 1270. https://doi.org/10.3390/life13061270
Della Corte L, Boccia D, Palumbo M, Mercorio A, Ronsini C, Bifulco G, Giampaolino P. Is There Still a Place for Surgery in Patients with PCOS? A Review. Life. 2023; 13(6):1270. https://doi.org/10.3390/life13061270
Chicago/Turabian StyleDella Corte, Luigi, Dominga Boccia, Mario Palumbo, Antonio Mercorio, Carlo Ronsini, Giuseppe Bifulco, and Pierluigi Giampaolino. 2023. "Is There Still a Place for Surgery in Patients with PCOS? A Review" Life 13, no. 6: 1270. https://doi.org/10.3390/life13061270