
Pleural Fluid Resolution Is Associated with Improved Survival in Patients with Malignant Pleural Effusion
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population Data Collected
2.2. Study Endpoints
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Predictors of Survival in Patients with Newly Diagnosed MPE
3.3. Predictors of Pleural Fluid Resolution
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antony, V.B. American Thoracic Society Guideline for Management of Malignant Pleural Effusions. Am. J. Respir. Crit. Care Med. 2000, 162, 1987–2001. [Google Scholar]
- Chernow, B. Carcinomatous involvement of the pleura: An analysis of 96 patients. Am. J. Med. 1977, 63, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Zamboni, M.M.; da Silva, C.T., Jr.; Baretta, R.; Cunha, E.T.; Cardoso, G.P. Important prognostic factors for survival in patients with malignant pleural effusion. BMC Pulm. Med. 2015, 15, 29. [Google Scholar] [CrossRef] [PubMed]
- Clive, A.O.; Kahan, B.C.; Hooper, C.E.; Bhatnagar, R.; Morley, A.J.; Zahan-Evans, N.; Bintcliffe, O.J.; Boshuizen, R.C.; Fysh, E.T.; Tobin, C.L.; et al. Predicting survival in malignant pleural effusion: Development and validation of the LENT prognostic score. Thorax 2014, 69, 1098–1104. [Google Scholar] [CrossRef]
- Burrows, C.M.; Mathews, W.C.; Colt, H.G. Predicting Survival in Patients with Recurrent Symptomatic Malignant Pleural Effusions. Chest 2000, 117, 73–78. [Google Scholar] [CrossRef]
- Feller-Kopman, D.J.; Reddy, C.B.; DeCamp, M.M.; Diekemper, R.L.; Gould, M.K.; Henry, T.; Iyer, N.P.; Lee, Y.C.G.; Lewis, S.Z.; Maskell, N.A.; et al. Management of Malignant Pleural Effusions. An Official ATS/STS/STR Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Panadero, F.; Lopez-Mejias, J. Survival time of patients with pleural metastatic carcinoma predicted by glucose and pH studies. Chest 1989, 95, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Bielsa, S.; Salud, A.; Martinez, M.; Esquerda, A.; Martin, A.; Rodriguez-Panadero, F.; Porcel, J.M. Prognostic significance of pleural fluid data in patients with malignant effusion. Eur. J. Intern. Med. 2008, 19, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Heffner, J.E.; Nietert, P.J.; Barbieri, C. Pleural Fluid pH as a Predictor of Survival for Patients with Malignant Pleural Effusions. Chest 2000, 117, 79–86. [Google Scholar] [CrossRef]
- Anevlavis, S.; Kouliatsis, G.; Sotiriou, I.; Koukourakis, M.I.; Archontogeorgis, K.; Karpathiou, G.; Giatromanolaki, A.; Froudarakis, M.E. Prognostic factors in patients presenting with pleural effusion revealing malignancy. Respir. Int. Rev. Thorac. Dis. 2014, 87, 311–316. [Google Scholar] [CrossRef]
- Verma, A.; Phua, C.K.; Sim, W.Y.; Algoso, R.E.; Tee, K.S.; Lew, S.J.; Lim, A.Y.; Goh, S.K.; Tai, D.Y.; Kor, A.C.; et al. Pleural LDH as a prognostic marker in adenocarcinoma lung with malignant pleural effusion. Medicine 2016, 95, e3996. [Google Scholar] [CrossRef] [PubMed]
- Galloway, K.C.; Chen, Y.; Templeton, E.; Rife, B.; Godage, I.S.; Barth, E.J. Fiber Optic Shape Sensing for Soft Robotics. Soft Robot. 2019, 6, 671–684. [Google Scholar] [CrossRef]
- Psallidas, I.; Kanellakis, N.I.; Gerry, S.; Thezenas, M.L.; Charles, P.D.; Samsonova, A.; Schiller, H.B.; Fischer, R.; Asciak, R.; Hallifax, R.J.; et al. Development and validation of response markers to predict survival and pleurodesis success in patients with malignant pleural effusion (PROMISE): A multicohort analysis. Lancet Oncol. 2018, 19, 930–939. [Google Scholar] [CrossRef]
- Sugiura, S.; Ando, Y.; Minami, H.; Ando, M.; Sakai, S.; Shimokata, K. Prognostic value of pleural effusion in patients with non-small cell lung cancer. Clin. Cancer Res. 1997, 3, 47–50. [Google Scholar]
- Ost, D.E.; Niu, J.; Zhao, H.; Grosu, H.B.; Giordano, S.H. Quality Gaps and Comparative Effectiveness of Management Strategies for Recurrent Malignant Pleural Effusions. Chest 2018, 153, 438–452. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.G.; Yu, C.J.; Tsai, M.F.; Liao, W.Y.; Yang, C.H.; Jan, I.S.; Yang, P.C.; Shih, J.Y. Survival of lung adenocarcinoma patients with malignant pleural effusion. Eur. Respir. J. 2013, 41, 1409–1418. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.W.; Nakagawa, K.; Seto, T.; Crino, L.; Ahn, M.J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef]
- Timm, A.; Kolesar, J.M. Crizotinib for the treatment of non-small-cell lung cancer. Am. J. Health Syst. Pharm. 2013, 70, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Bibby, A.C.; Dorn, P.; Psallidas, I.; Porcel, J.M.; Janssen, J.; Froudarakis, M.; Subotic, D.; Astoul, P.; Licht, P.; Schmid, R.; et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur. J. Cardiothorac. Surg. 2018, 52, 1800349. [Google Scholar] [CrossRef]
- Lee, Y.S.; Nam, H.S.; Lim, J.H.; Kim, J.S.; Moon, Y.; Cho, J.H.; Ryu, J.S.; Kwak, S.M.; Lee, H.L. Prognostic impact of a new score using neutrophil-to-lymphocyte ratios in the serum and malignant pleural effusion in lung cancer patients. BMC Cancer 2017, 17, 557. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Toki, M.I.; Mani, N.; Smithy, J.W.; Liu, Y.; Altan, M.; Wasserman, B.; Tuktamyshov, R.; Schalper, K.; Syrigos, K.N.; Rimm, D.L. Immune Marker Profiling and Programmed Death Ligand 1 Expression Across NSCLC Mutations. J. Thorac. Oncol. 2018, 13, 1884–1896. [Google Scholar] [CrossRef]
- Sacher, A.G.; Gandhi, L. Biomarkers for the Clinical Use of PD-1/PD-L1 Inhibitors in Non-Small-Cell Lung Cancer: A Review. JAMA Oncol. 2016, 2, 1217–1222. [Google Scholar] [CrossRef]
- Schalper, K.A.; Carvajal-Hausdorf, D.; McLaughlin, J.; Altan, M.; Velcheti, V.; Gaule, P.; Sanmamed, M.F.; Chen, L.; Herbst, R.S.; Rimm, D.L. Differential Expression and Significance of PD-L1, IDO-1, and B7-H4 in Human Lung Cancer. Clin. Cancer Res. 2017, 23, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Bustamante-Teixeira, M.T.; Faerstein, E.; Latorre Mdo, R. [Survival analysis techniques]. Cad. Saude Publica 2002, 18, 579–594. [Google Scholar] [CrossRef]
- Mallett, S.; Royston, P.; Waters, R.; Dutton, S.; Altman, D.G. Reporting performance of prognostic models in cancer: A review. BMC Med. 2010, 8, 21. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographic Variables | N | |
|---|---|---|
| Age at diagnosis (years) | 123 | 64.4 (62.3–66.5) † |
| Female | 123 | 71 (58%) |
| ECOG performance score ^ | 58 | 0 (n = 10; 17.2%) |
| 1 (n = 28; 48.2%) | ||
| 2 (n = 12; 20.7%) | ||
| 3 (n = 5; 8.6%) | ||
| 4 (n = 3; 5.2%) | ||
| History of tobacco use | 122 | 72 (59%) |
| IPC placed | 123 | 63 (51.2%) |
| Pleural fluid values | ||
| pH | 25 | 7.5 (7.4–7.5) † |
| % eosinophils | 74 | 0 (0–1.0) * |
| % neutrophils | 100 | 7.5 (2.0–18.5) * |
| % monocytes/macrophages | 102 | 10.5 (5.0–20.0) * |
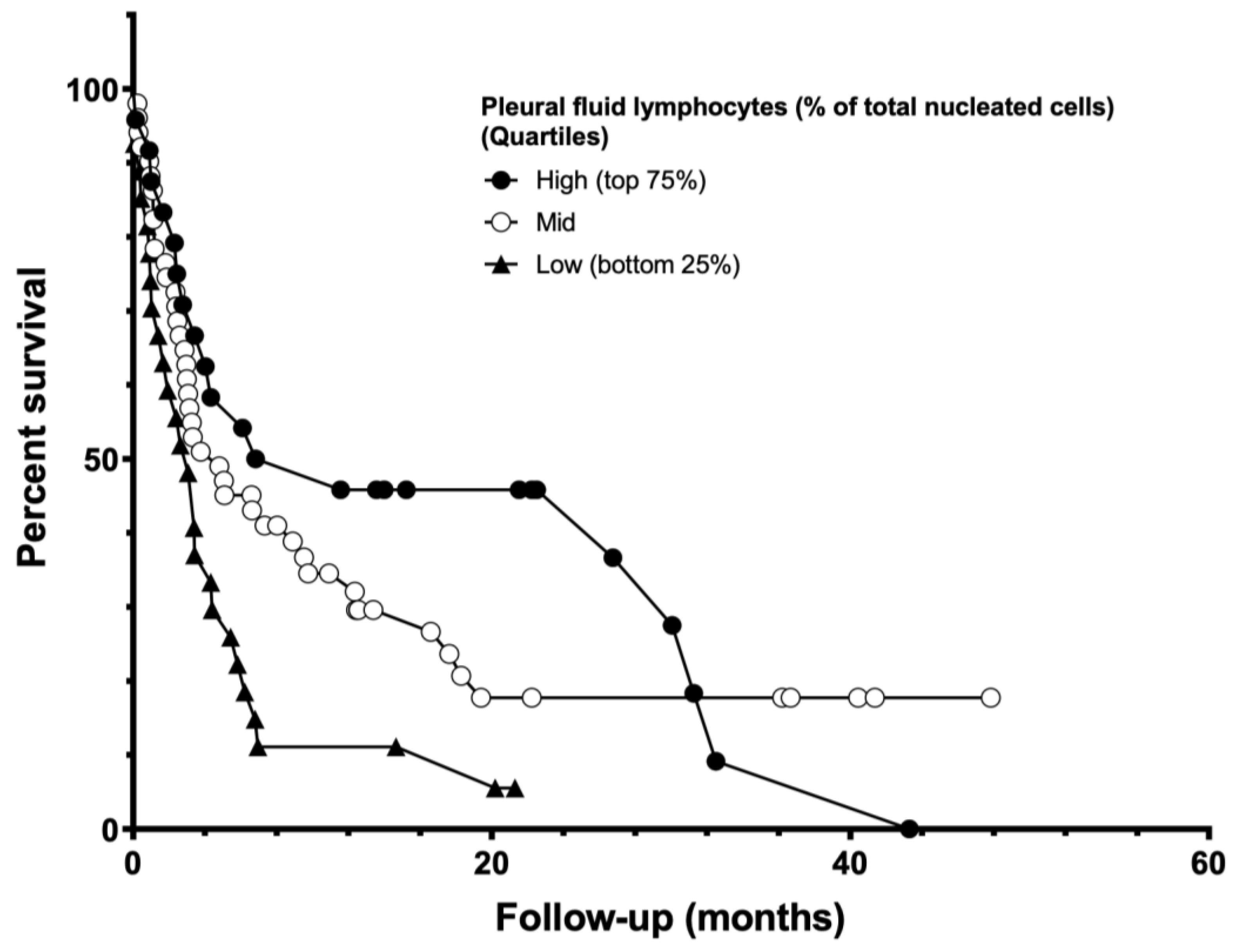
| % lymphocytes | 103 | 43 (18.0–68.0) * |
| Glucose (mg/dL) | 100 | 93.5 (77.5–113.0) * |
| Protein (g/dL) | 104 | 4 (3.8–4.2) † |
| lactate dehydrogenase (U/L) | 107 | 760 (446.0–1411.0) * |
| Presence of mutation or PD-L1 ≥ 50% | 104 | 60 (57.7%) |
| Spontaneous Pleurodesis = N | Spontaneous Pleurodesis = Y | |
|---|---|---|
| Number of rows | 123 | 123 |
| rows with impossible data | 1 | 0 |
| censored subjects | 18 | 10 |
| deaths/events | 81 | 13 |
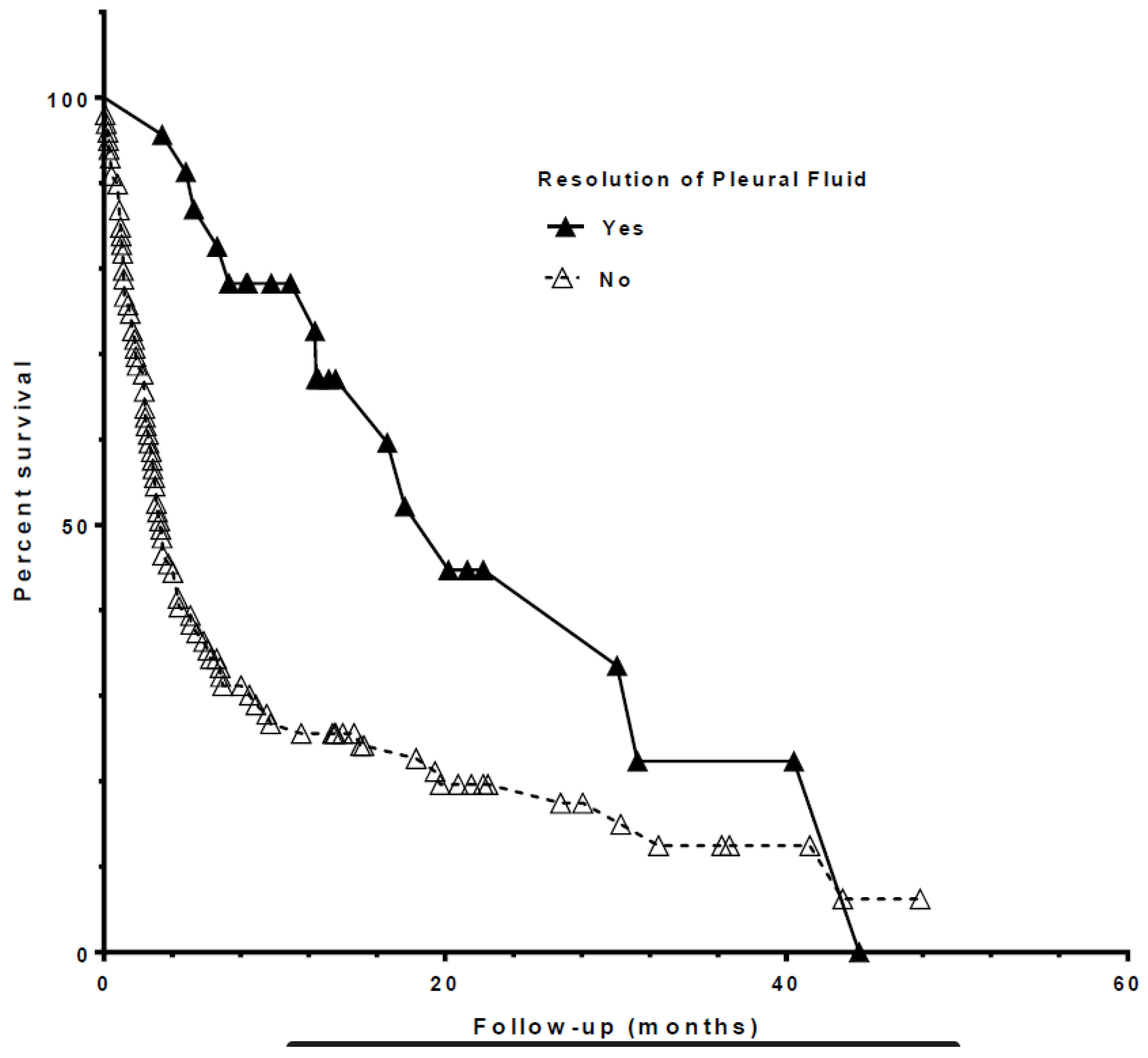
| Median survival (months) | 3.3333 | 20.2 |
| Variable | Hazard Ratio (95% CI) | p Value |
|---|---|---|
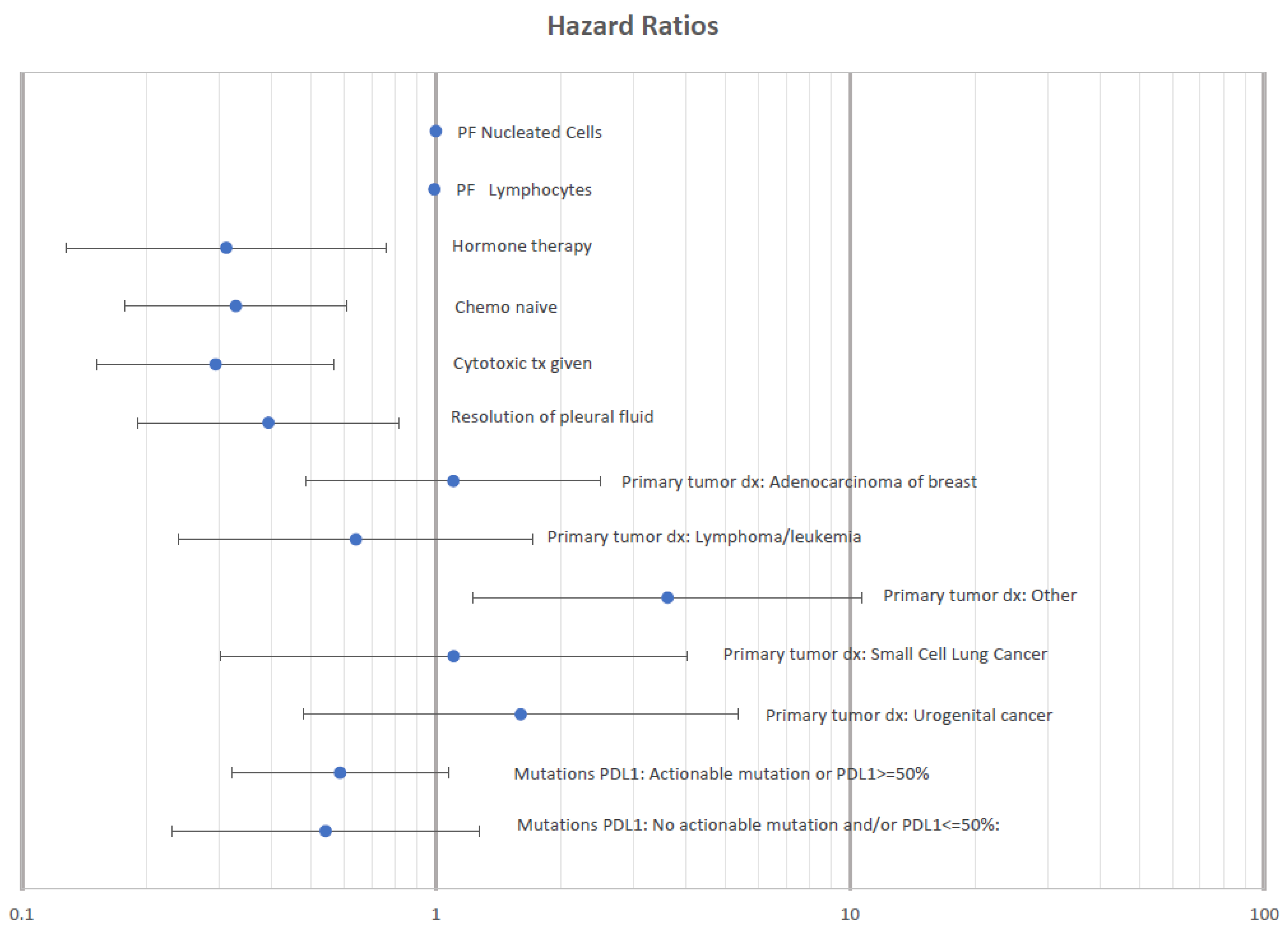
| Resolution of pleural fluid accumulation | 0.382 (0.2112–0.688) | 0.0014 |
| Intrapleural catheter placed | 1.231 (0.819–1.849) | 0.317 |
| Performance score | 1.714 (1.252–2.347) | 0.0008 |
| Actionable target and/or PD-L1 ≥ 50% | 0.633 (0.399–1.004) | 0.0518 |
| Systemic cancer treatment given | 0.175 (0.098–0.31) | <0.0001 |
| Cytotoxic therapy | 0.579 (0.378–0.885) | 0.0116 |
| Hormone therapy | 0.619 (0.361–1.064) | 0.0824 |
| Targeted therapy | 0.632 (0.376–1.06) | 0.0822 |
| Immunotherapy | 0.782 (0.448–1.364) | 0.3859 |
| PF Cytology Group—Breast Cancer | 0.755 (0.452–1.33) | |
| PF Cytology Group—Lymphoma/Leukemia | 0.876 (0.387–1.981) | |
| PF Cytology Group—Non-small Cell Lung Cancer | 0.843 (0.258–2.76) | 0.041 |
| PF Cytology Group—Small Cell Lung Cancer | 1.7 (0.662–4.366) | |
| PF Cytology Group—Urogenital Cancer | 1.287 (0.594–2.791) | |
| PF Cytology Group—Other Cancer | 2.331 (1.278–4.249) | |
| PF LDH (per 100 units) | 1.011 (1.001–1.022) | 0.0373 |
| PF Protein | 0.738 (0.589–0.924) | 0.0081 |
| PF Albumin | 0.44 (0.279–0.693) | 0.0004 |
| PF % lymphocytes | 0.988 (0.97–0.997) | 0.0038 |
| PF % neutrophils | 1.014 (1.003–1.025) | 0.0155 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacRosty, C.R.; Wright, A.; Ceppe, A.; Ghosh, S.; Burks, A.C.; Akulian, J.A. Pleural Fluid Resolution Is Associated with Improved Survival in Patients with Malignant Pleural Effusion. Life 2023, 13, 1163. https://doi.org/10.3390/life13051163
MacRosty CR, Wright A, Ceppe A, Ghosh S, Burks AC, Akulian JA. Pleural Fluid Resolution Is Associated with Improved Survival in Patients with Malignant Pleural Effusion. Life. 2023; 13(5):1163. https://doi.org/10.3390/life13051163
Chicago/Turabian StyleMacRosty, Christina R., Amber Wright, Agathe Ceppe, Sohini Ghosh, A. Cole Burks, and Jason A. Akulian. 2023. "Pleural Fluid Resolution Is Associated with Improved Survival in Patients with Malignant Pleural Effusion" Life 13, no. 5: 1163. https://doi.org/10.3390/life13051163