
Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022)

 ,
on behalf of The ATTICA Study Group
,
on behalf of The ATTICA Study Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
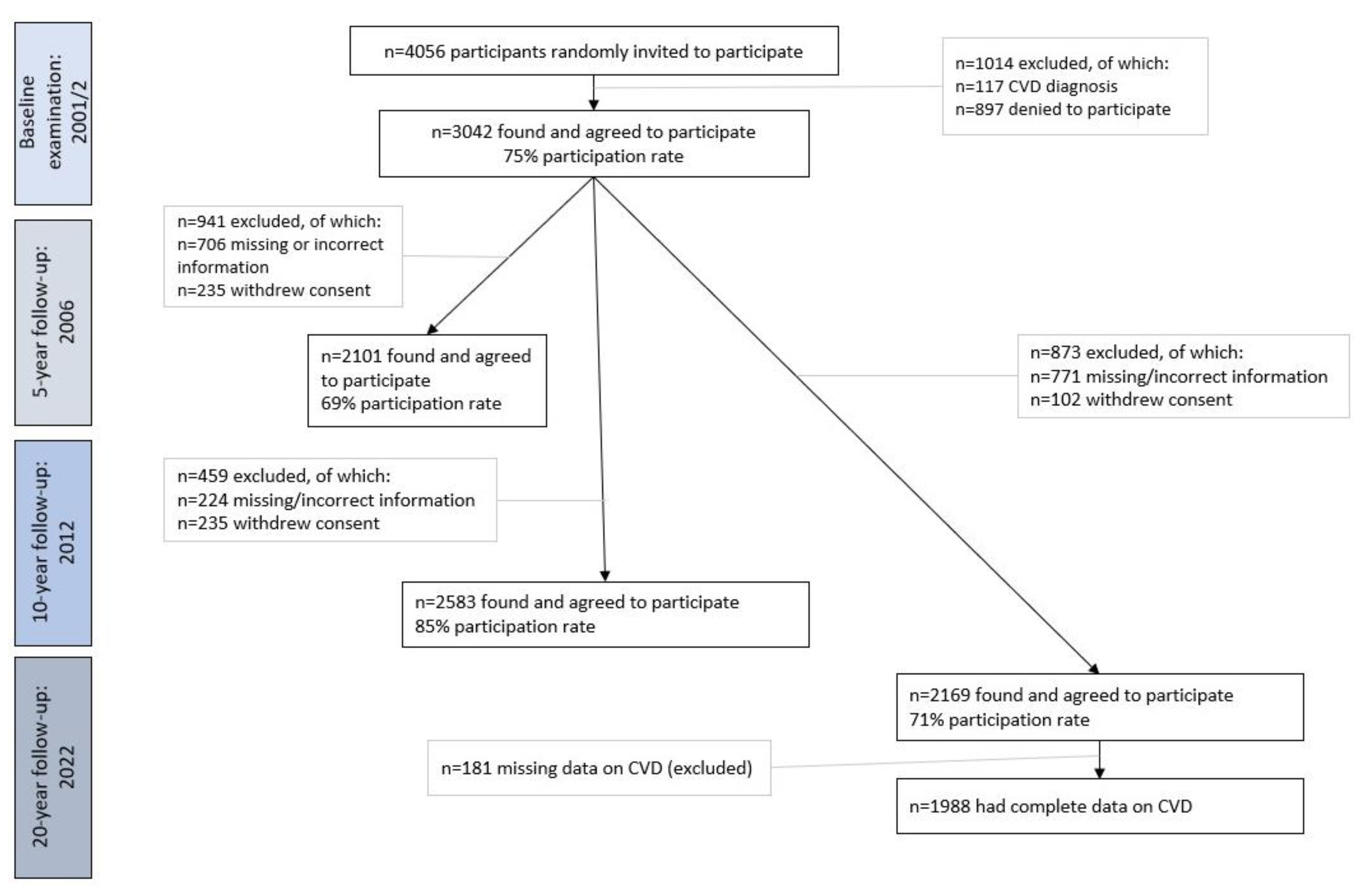
2.2. Setting and Participants
2.3. Endpoint and Follow-Up Examination
2.4. Bioethics
2.5. Baseline Assessment
2.5.1. Socio-Demographic Characteristics
2.5.2. Anthropometric Measurements
2.5.3. Biochemical Measurements and Clinical Characteristics
2.5.4. Lifestyle Characteristics
2.6. Trajectories of Lifestyle Parameters
2.7. Follow-Up Assessment
2.8. Statistical Analysis
3. Results
3.1. CVD Incidence and Mortality at 20-Year Follow-Up
3.2. Temporal Trends of Lifestyle and Clinical Features over the Past 20 Years (2002–2022)
3.3. Determinants of 20-Year CVD Incidence
3.4. Multi-Adjusted Analysis of 20-Year CVD Incidence and Attributable Risk
4. Discussion
4.1. CVD Epidemiology in Greece
4.2. Lifestyle Factors in Relation to CVD Incidence
4.3. Actions Needed to Reduce CVD Rates at the Population Level
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- Stampfer, M.J.; Hu, F.B.; Manson, J.E.; Rimm, E.B.; Willett, W.C. Primary Prevention of Coronary Heart Disease in Women through Diet and Lifestyle. N. Engl. J. Med. 2000, 343, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of Potentially Modifiable Risk Factors Associated with Myocardial Infarction in 52 Countries (the INTERHEART Study): Case-Control Study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef] [PubMed]
- European Heart Agency ESC Cardiovascular Realities 2022. An Illustrated Atlas of Key European Statistics/2022. Available online: https://www.flipsnack.com/escardio/esc-cardiovascular-realities-2022/full-view.html (accessed on 25 January 2023).
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice: Developed by the Task Force for Cardiovascular Disease Prevention in Clinical Practice with Representatives of the European Society of Cardiology and 12 Medical Societies with the Special Contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- SCORE2 Working Group and ESC Cardiovascular Risk Collaboration. SCORE2 Risk Prediction Algorithms: New Models to Estimate 10-Year Risk of Cardiovascular Disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- Pitsavos, C.; Panagiotakos, D.B.; Chrysohoou, C.; Stefanadis, C. Epidemiology of Cardiovascular Risk Factors in Greece: Aims, Design and Baseline Characteristics of the ATTICA Study. BMC Public Health 2003, 3, 32. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Georgousopoulou, E.N.; Pitsavos, C.; Chrysohoou, C.; Metaxa, V.; Georgiopoulos, G.A.; Kalogeropoulou, K.; Tousoulis, D.; Stefanadis, C. Ten-Year (2002–2012) Cardiovascular Disease Incidence and All-Cause Mortality, in Urban Greek Population: The ATTICA Study. Int. J. Cardiol. 2015, 180, 178–184. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Kushner, R.F. Clinical Assessment and Management of Adult Obesity. Circulation 2012, 126, 2870–2877. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Rimm, E.B.; Gnardellis, C.; Trichopoulos, D.; Polychronopoulos, E.; Trichopoulou, A. Reproducibility and Relative Validity of an Extensive Semi-Quantitative Food Frequency Questionnaire Using Dietary Records and Biochemical Markers among Greek Schoolteachers. Int. J. Epidemiol. 1997, 26, S118. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, G.; Georgoudis, G.; Papandreou, M.; Spyropoulos, P.; Georgakopoulos, D.; Kalfakakou, V.; Evangelou, A. Reliability Measures of the Short International Physical Activity Questionnaire (IPAQ) in Greek Young Adults. Hell. J. Cardiol. 2009, 50, 283–294. [Google Scholar]
- Kavouras, S.A.; Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Anastasiou, C.A.; Lentzas, Y.; Stefanadis, C. Physical Activity, Obesity Status, and Glycemic Control: The ATTICA Study. Med. Sci. Sport. Exerc. 2007, 39, 606. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, M.; Mensah, G.A.; Turco, J.V.; Fuster, V.; Roth, G.A. The Global Burden of Cardiovascular Diseases and Risk: A Compass for Future Health. J. Am. Coll. Cardiol. 2022, 80, 2361–2371. [Google Scholar] [CrossRef] [PubMed]
- Andersson, C.; Vasan, R.S. Epidemiology of Cardiovascular Disease in Young Individuals. Nat. Rev. Cardiol. 2018, 15, 230–240. [Google Scholar] [CrossRef]
- Brown, M.T.; Bussell, J.K. Medication Adherence: WHO Cares? Mayo Clin. Proc. 2011, 86, 304–314. [Google Scholar] [CrossRef]
- Alcalá, H.E.; Albert, S.L.; Roby, D.H.; Beckerman, J.; Champagne, P.; Brookmeyer, R.; Prelip, M.L.; Glik, D.C.; Inkelas, M.; Garcia, R.-E.; et al. Access to Care and Cardiovascular Disease Prevention. Medicine 2015, 94, e1441. [Google Scholar] [CrossRef]
- Magriplis, E.; Panagiotakos, D.; Mitsopoulou, A.-V.; Karageorgou, D.; Bakogianni, I.; Dimakopoulos, I.; Micha, R.; Michas, G.; Chourdakis, M.; Chrousos, G.P.; et al. Prevalence of Hyperlipidaemia in Adults and Its Relation to the Mediterranean Diet: The Hellenic National Nutrition and Health Survey (HNNHS). Eur. J. Prev. Cardiol. 2019, 26, 1957–1967. [Google Scholar] [CrossRef]
- Touloumi, G.; Karakosta, A.; Kalpourtzi, N.; Gavana, M.; Vantarakis, A.; Kantzanou, M.; Hajichristodoulou, C.; Chlouverakis, G.; Trypsianis, G.; Voulgari, P.V.; et al. High Prevalence of Cardiovascular Risk Factors in Adults Living in Greece: The EMENO National Health Examination Survey. BMC Public Health 2020, 20, 1665. [Google Scholar] [CrossRef] [PubMed]
- Liatis, S.; Dafoulas, G.E.; Kani, C.; Politi, A.; Litsa, P.; Sfikakis, P.P.; Makrilakis, K. The Prevalence and Treatment Patterns of Diabetes in the Greek Population Based on Real-World Data from the Nation-Wide Prescription Database. Diabetes Res. Clin. Pract. 2016, 118, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Ikonomidis, I.; Thymis, J.; Kourea, K.; Kostelli, G.; Neocleous, A.; Katogiannis, K.; Makavos, G.; Polyzogopoulou, E.; Plotas, P.; Lambadiari, V.; et al. Fagerstrom Score Predicts Smoking Status Six Months after Hospitalization for Acute Myocardial Infarction: A Prospective Study. Hell. J. Cardiol. 2022, 67, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Haß, U.; Pirlich, M. Malnutrition in Older Adults-Recent Advances and Remaining Challenges. Nutrients 2021, 13, 2764. [Google Scholar] [CrossRef]
- Talikka, M.; Sierro, N.; Ivanov, N.V.; Chaudhary, N.; Peck, M.J.; Hoeng, J.; Coggins, C.R.E.; Peitsch, M.C. Genomic Impact of Cigarette Smoke, with Application to Three Smoking-Related Diseases. Crit. Rev. Toxicol. 2012, 42, 877–889. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Georgousopoulou, E.N.; Pitsavos, C.; Chrysohoou, C.; Skoumas, I.; Pitaraki, E.; Georgiopoulos, G.A.; Ntertimani, M.; Christou, A.; Stefanadis, C. Exploring the Path of Mediterranean Diet on 10-Year Incidence of Cardiovascular Disease: The ATTICA Study (2002–2012). Nutr. Metab. Cardiovasc. Dis. 2015, 25, 327–335. [Google Scholar] [CrossRef]
- Georgoulis, M.; Georgousopoulou, E.N.; Chrysohoou, C.; Pitsavos, C.; Panagiotakos, D.B. Longitudinal Trends, Determinants, and Cardiometabolic Impact of Adherence to the Mediterranean Diet among Greek Adults. Foods 2022, 11, 2389. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.M.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide Adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72, 83–91. [Google Scholar] [CrossRef]
- Popkin, B.M.; Ng, S.W. The Nutrition Transition to a Stage of High Obesity and Noncommunicable Disease Prevalence Dominated by Ultra-Processed Foods Is Not Inevitable. Obes. Rev. 2022, 23, e13366. [Google Scholar] [CrossRef]
- Ding, X.; Fang, W.; Yuan, X.; Seery, S.; Wu, Y.; Chen, S.; Zhou, H.; Wang, G.; Li, Y.; Yuan, X.; et al. Associations Between Healthy Lifestyle Trajectories and the Incidence of Cardiovascular Disease with All-Cause Mortality: A Large, Prospective, Chinese Cohort Study. Front. Cardiovasc. Med. 2021, 8, 790497. [Google Scholar] [CrossRef]
- Tomar, S.L. Duration of Cigarette Smoking Is a Stronger Risk Factor Than Number of Cigarettes Smoked per Day for Head and Neck Cancer, and Quitting Dramatically Lowers the Risk. J. Evid. Based Dent. Pract. 2020, 20, 101419. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, L.; Golden, S.D.; Earp, J.A.L. Structural Approaches to Health Promotion: What Do We Need to Know About Policy and Environmental Change? Health Educ. Behav. 2013, 40, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Noncommunicable Diseases Global Monitoring Framework: Indicator Definitions and Specifications; World Health Organization: Geneva, Switzerland, 2014; Available online: https://www.who.int/publications-detail-redirect/ncd-surveillance-global-monitoring-framework (accessed on 18 November 2022).
- Bárcena, A.; Cimoli, M.; García-Buchaca, R.; Yáñez, L.F.; Pérez, R. The 2030 Agenda and the Sustainable Development Goals: An Opportunity for Latin America and the Caribbean; United Nations: Santiago, Chile, 2019; p. 94. [Google Scholar]
- Global Hearts Initiative. Available online: https://www.who.int/news/item/15-09-2016-global-hearts-initiative (accessed on 2 February 2023).
- Campbell, N.R.C.; Ordunez, P.; Giraldo, G.; Rodriguez Morales, Y.A.; Lombardi, C.; Khan, T.; Padwal, R.; Tsuyuki, R.T.; Varghese, C. WHO HEARTS: A Global Program to Reduce Cardiovascular Disease Burden: Experience Implementing in the Americas and Opportunities in Canada. Can. J. Cardiol. 2021, 37, 744–755. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 20-Year CVD Incidence, % (n) | Man-to-Woman CVD Incidence Ratio | |||
|---|---|---|---|---|
| Age at baseline | n | Men (n = 987) | Women (n = 1001) | |
| <35 y | 516 | 4.3% (17) | 3.1% (10) | 1.4 |
| 35–45 y | 565 | 7.1% (28) | 3.4% (11) | 2.1 |
| 45–55 y | 521 | 41% (164) | 34% (110) | 1.2 |
| 55–65 y | 226 | 26% (105) | 35% (113) | 0.74 |
| 65–75 y | 101 | 12% (48) | 17% (53) | 0.70 |
| 75+ y | 59 | 8.8% (35) | 7.5% (24) | 1.17 |
| Overall | 1988 | 40% (397) | 32% (321) | 1.25 |
| Year of Survey | Baseline (2001–2) | 5-Year Follow-Up (2007) | 10-Year Follow-Up (2011–12) | 20-Year Follow-Up (2022) | p for Linear Trend |
|---|---|---|---|---|---|
| Anthropometric factors | |||||
| Body weight, % Overweight/obese | 60 | 61 | 57 | 53 | 0.09 |
| Clinical factors | |||||
| CVD, % | - 1 | 9 | 16 | 36 | <0.001 |
| Hypertension, % | 31 | 41 | 50 | 53 | 0.04 |
| Hypercholesterolemia, % | 43 | 54 | 67 | 74 | 0.03 |
| Diabetes, % | 7 | 13 | 24 | 32 | <0.001 |
| Lifestyle factors | |||||
| Smoking Habits, % Current smoking | 41 | 40 | 41 | 29 | 0.09 |
| Adherence to the MD, % Poor level of adherence | 32 | 33 | 30 | 34 | 0.54 |
| Physical activity, % Low physical activity level | 59 | 71 | 77 | 69 | 0.43 |
| 20-Year Incident CVD Events | ||||
|---|---|---|---|---|
| Overall n = 1988 | No n = 1270 | Yes n = 718 | p | |
| Anthropometric characteristics | ||||
| Body mass index, kg/m2 | 26 (5) | 26 (4) | 28 (4) | <0.001 |
| Abnormal waist circumference (≥102 cm for men, ≥88 cm for women), % | 52 | 45 | 68 | <0.001 |
| Clinical characteristics | ||||
| Hypertension, % | 30 | 20 | 51 | <0.001 |
| Hypercholesterolemia, % | 41 | 30 | 65 | <0.001 |
| Diabetes, % | 6.6 | 1.4 | 17 | <0.001 |
| Family history of CVD, % | 37 | 36 | 39 | 0.210 |
| Lifestyle characteristics and trajectories | ||||
| Pack-years of cigarette smoking | 497 (501) | 375 (340) | 703 (633) | <0.001 |
| Smoking Habits (2002–2012), % | <0.001 | |||
| Never smokers | 54 | 56 | 50 | |
| Started smoking | 7 | 2 | 19 | |
| Quitted smoking | 23 | 32 | 4 | |
| Continued smoking | 16 | 10 | 28 | |
| Physical Activity (2002–2012), % | <0.001 | |||
| Inactive | 50 | 46 | 56 | |
| Remained active | 13 | 13 | 14 | |
| Became inactive | 28 | 27 | 29 | |
| Became active | 10 | 14 | 2 | |
| MedDietScore (0–55) | 26 (7) | 27 (6) | 23 (6) | <0.001 |
| Adherence to the Mediterranean Diet (2002–2012), % | <0.001 | |||
| Always away | 24 | 13 | 42 | |
| From away (2002) to Close (2012) | 9 | 5 | 16 | |
| From Close (2002) to away (2012) | 47 | 52 | 36 | |
| Always close | 20 | 29 | 5 | |
| Factors | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
|---|---|---|---|---|---|
| Age, per 1 year | 1.30 (1.27, 1.33) | 1.28 (1.25, 1.32) | 1.27 (1.23, 1.31) | 1.26 (1.23, 1.30) | 1.24 (1.21, 1.28) |
| Sex, men versus women | 1.89 (1.41, 2.54) | 1.71 (1.22 2.38) | 1.61 (1.11, 2.34) | 1.50 (1.03, 2.20) | 1.51 (1.04, 2.21) |
| Hypercholesterolemia, yes versus no | - | 2.49 (1.86, 3.85) | 2.44 (1.81, 3.80) | 2.22 (1.65, 3.59) | 2.23 (1.66, 3.58) |
| Hypertension, yes versus no | - | 1.87 (1.30, 2.70) | 1.85 (1.27, 2.68) | 1.86 (1.29, 2.70) | 1.87 (1.20, 2.71) |
| Diabetes, yes versus no | - | 5.40 (2.31, 12.9) | 5.45 (2.32, 13.0) | 5.70 (2.41, 13.0) | 5.70 (2.40, 13.1) |
| Abnormal waist circumference, yes versus no | - | 1.04 (1.03, 1.06) | 1.03 (1.01, 1.05) | 1.03 (1.00, 1.04) | 1.03 (1.01, 1.05) |
| Smoking habits (2002–2022) versus Never smokers | |||||
| Started smoking | - | - | 1.78 (0.79, 4.03) | 1.70 (0.71, 3.95) | 1.68 (0.69, 3.93) |
| Quitted smoking | - | - | 1.33 (0.63, 2.84) | 1.32 (0.62, 2.83) | 1.32 (0.62, 2.83) |
| Continued smoking | - | - | 3.02 (2.13, 4.27) | 2.80 (1.91, 4.05) | 2.77 (1.61, 4.02) |
| Mediterranean diet adherence (2002–2022) versus Always away | |||||
| From away to close | - | - | - | 0.97 (0.68, 1.39) | 0.83 (0.50, 1.37) |
| From close to away | - | - | - | 0.21 (0.17, 0.27) | 0.61 (0.42, 0.89) |
| Always close | - | - | - | 0.05 (0.03, 0.07) | 0.50 (0.27, 0.90) |
| Physical activity (2002–2022) versus Inactive | |||||
| Remained active | - | - | - | - | 0.90 (0.82, 0.97) |
| Became inactive | - | - | - | - | 0.93 (0.63, 1.36) |
| Became active | - | - | - | - | 0.82 (0.54, 1.27) |
| Attributable fraction * | 43% | 56% | 78% | 82% | 86% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damigou, E.; Kouvari, M.; Chrysohoou, C.; Barkas, F.; Kravvariti, E.; Pitsavos, C.; Skoumas, J.; Michelis, E.; Liberopoulos, E.; Tsioufis, C.; et al. Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022). Life 2023, 13, 1142. https://doi.org/10.3390/life13051142
Damigou E, Kouvari M, Chrysohoou C, Barkas F, Kravvariti E, Pitsavos C, Skoumas J, Michelis E, Liberopoulos E, Tsioufis C, et al. Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022). Life. 2023; 13(5):1142. https://doi.org/10.3390/life13051142
Chicago/Turabian StyleDamigou, Evangelia, Matina Kouvari, Christina Chrysohoou, Fotios Barkas, Evrydiki Kravvariti, Christos Pitsavos, John Skoumas, Evangelinos Michelis, Evangelos Liberopoulos, Costas Tsioufis, and et al. 2023. "Lifestyle Trajectories Are Associated with Incidence of Cardiovascular Disease: Highlights from the ATTICA Epidemiological Cohort Study (2002–2022)" Life 13, no. 5: 1142. https://doi.org/10.3390/life13051142