
Do Medical Universities Students Use Cognitive Enhancers while Learning?—Conclusions from the Study in Poland

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Study Design and the Sample Size Calculation
2.2. Ethical Approval
2.3. The Questionnaire Organization
2.4. Statistical Analysis
3. Results
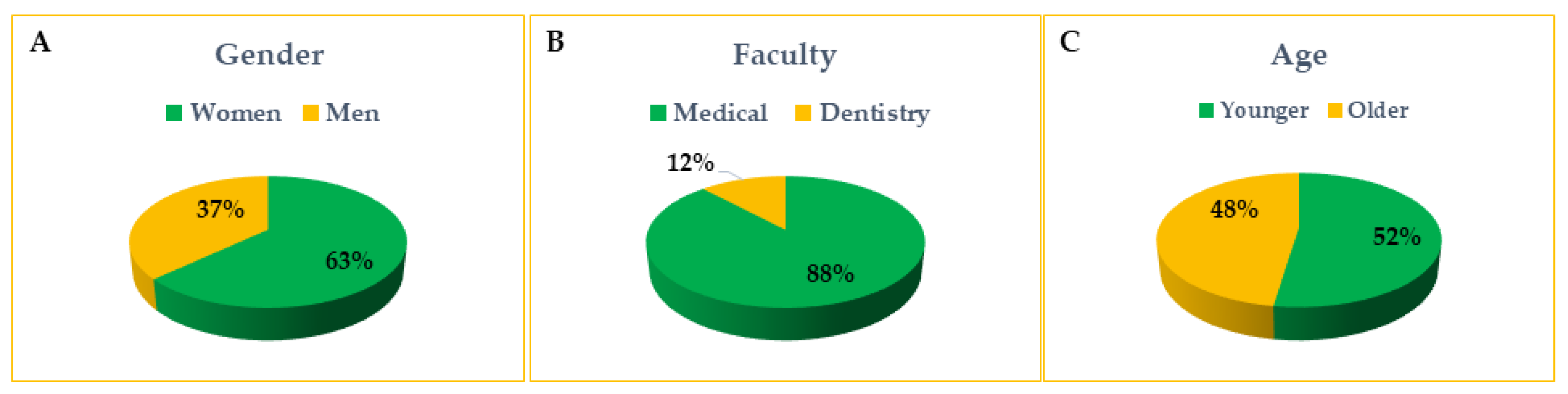
3.1. Demographic Data
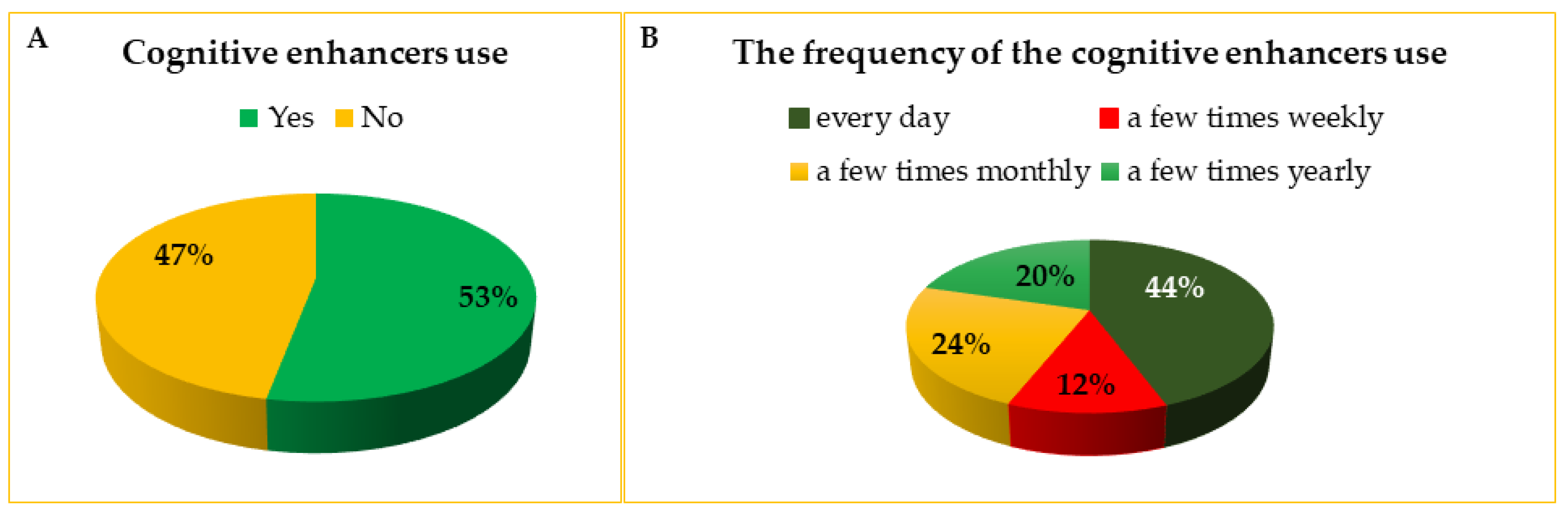
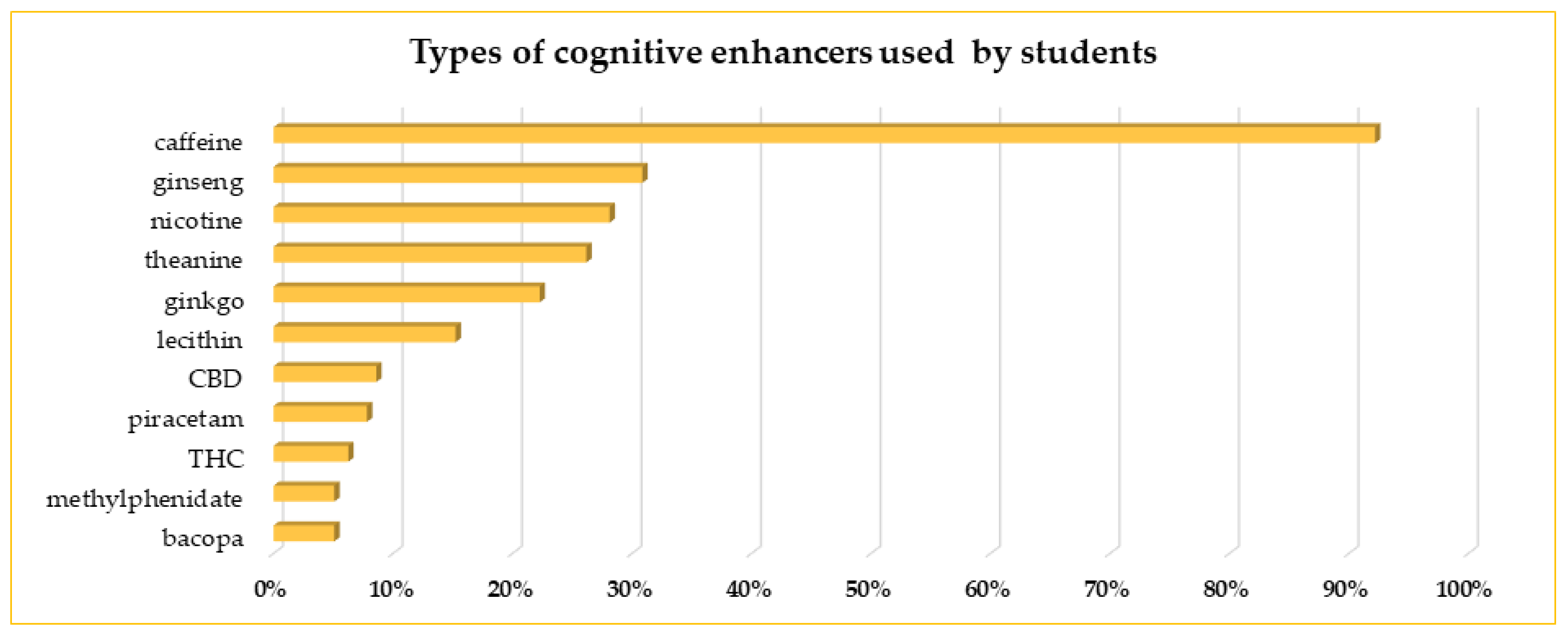
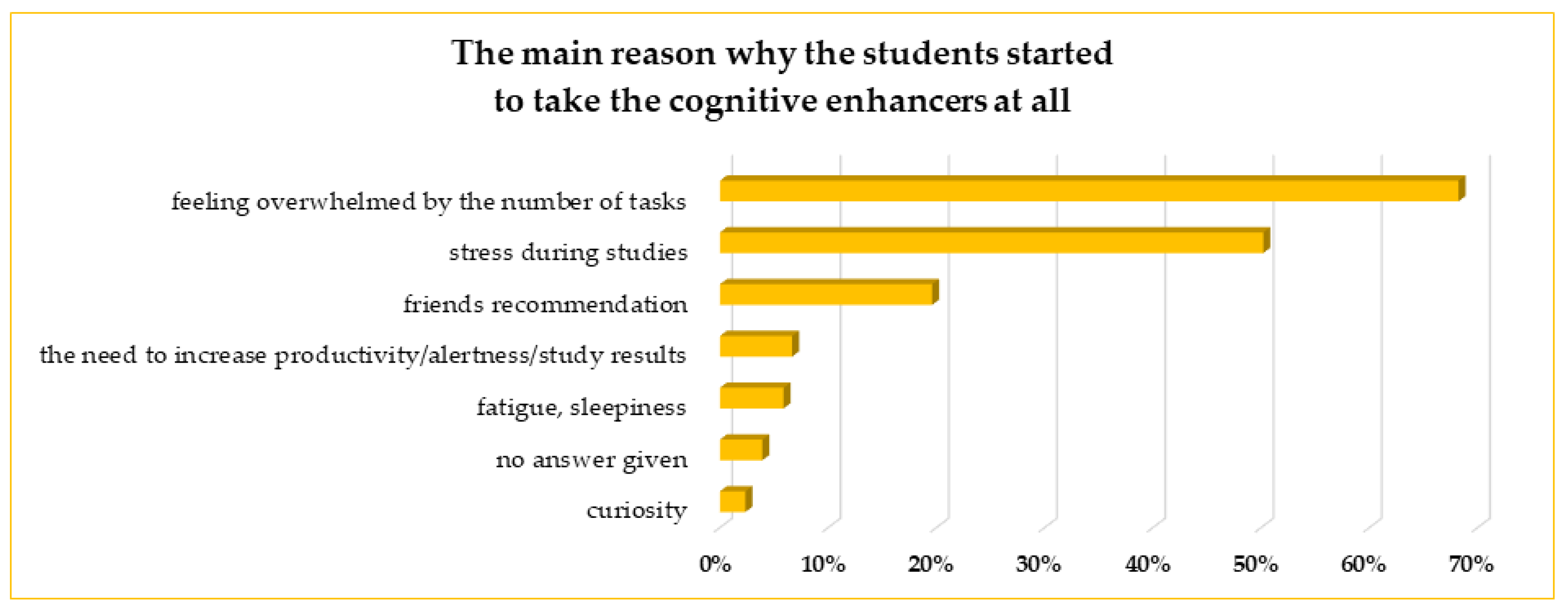
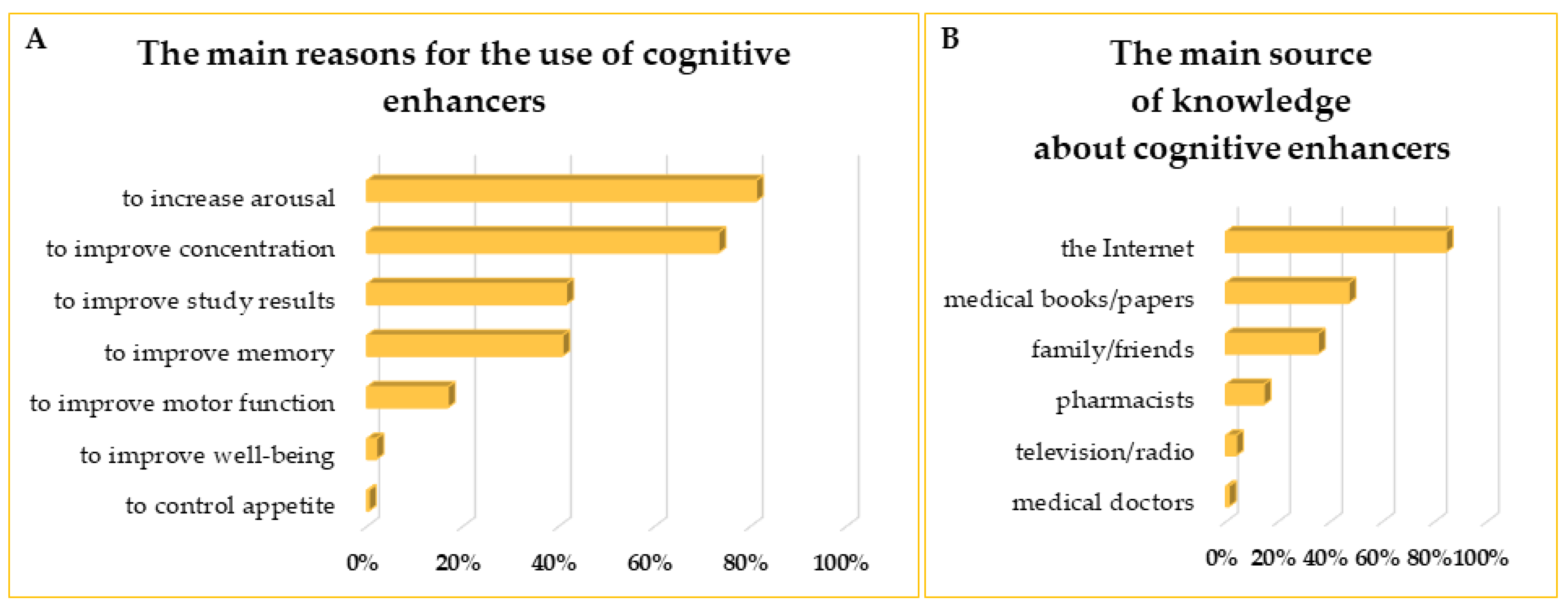
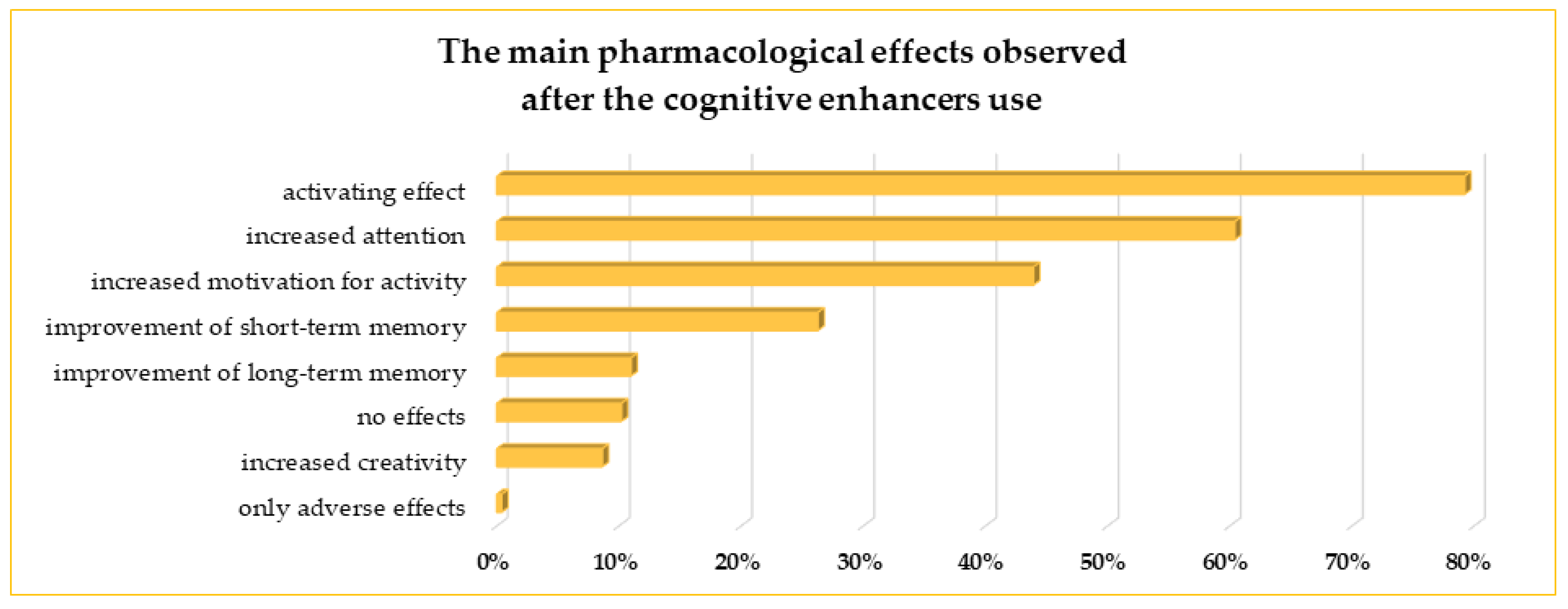
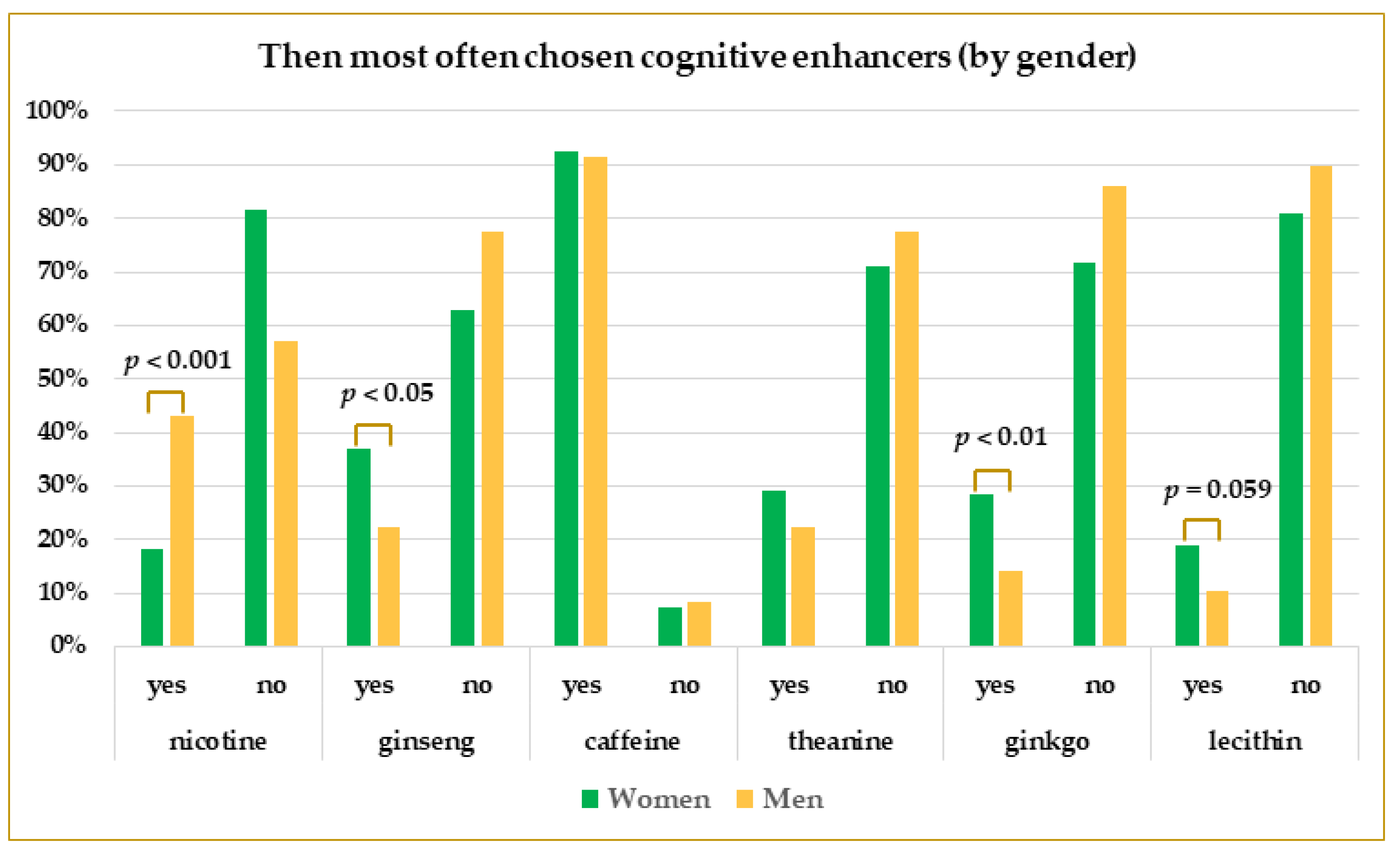
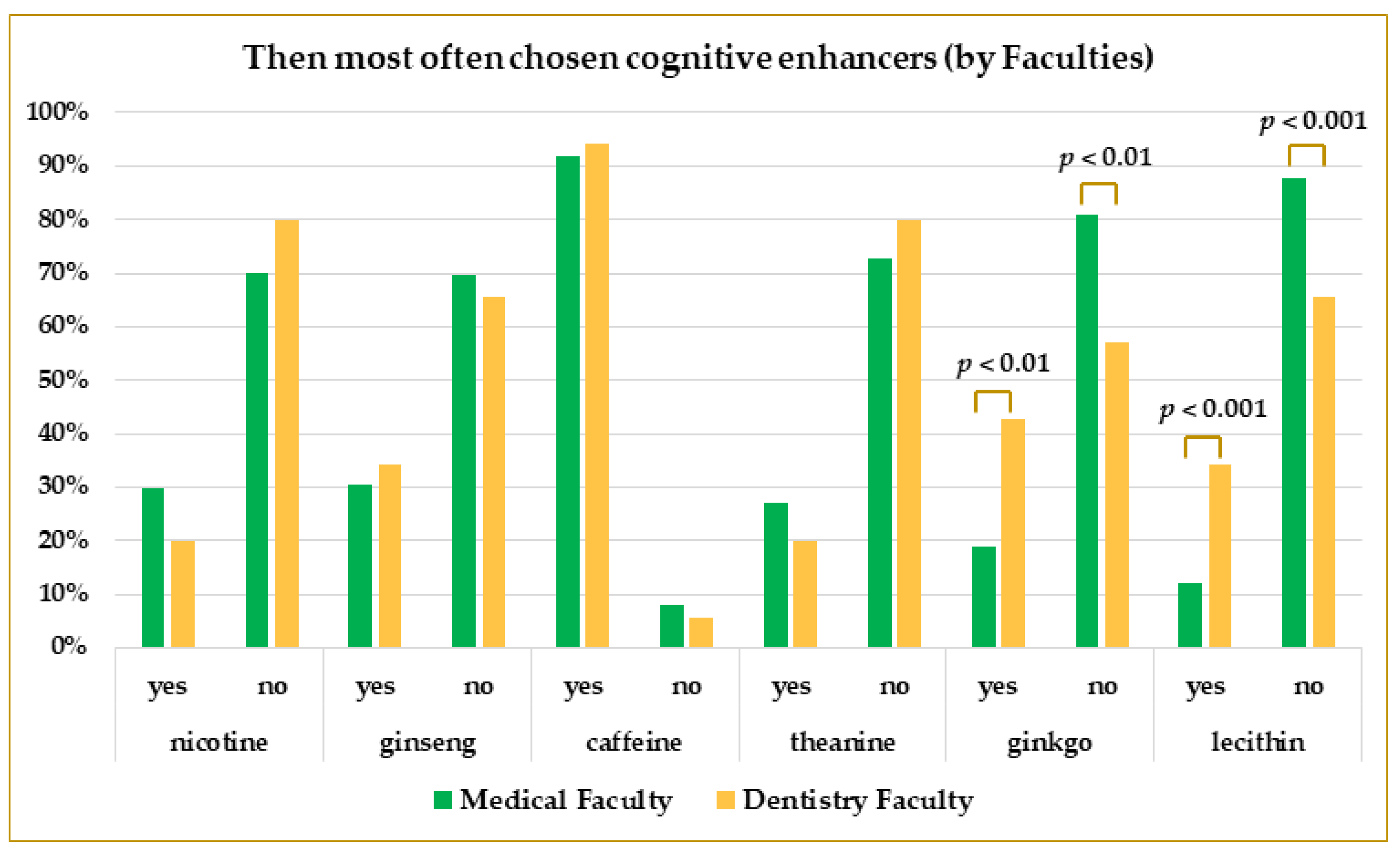
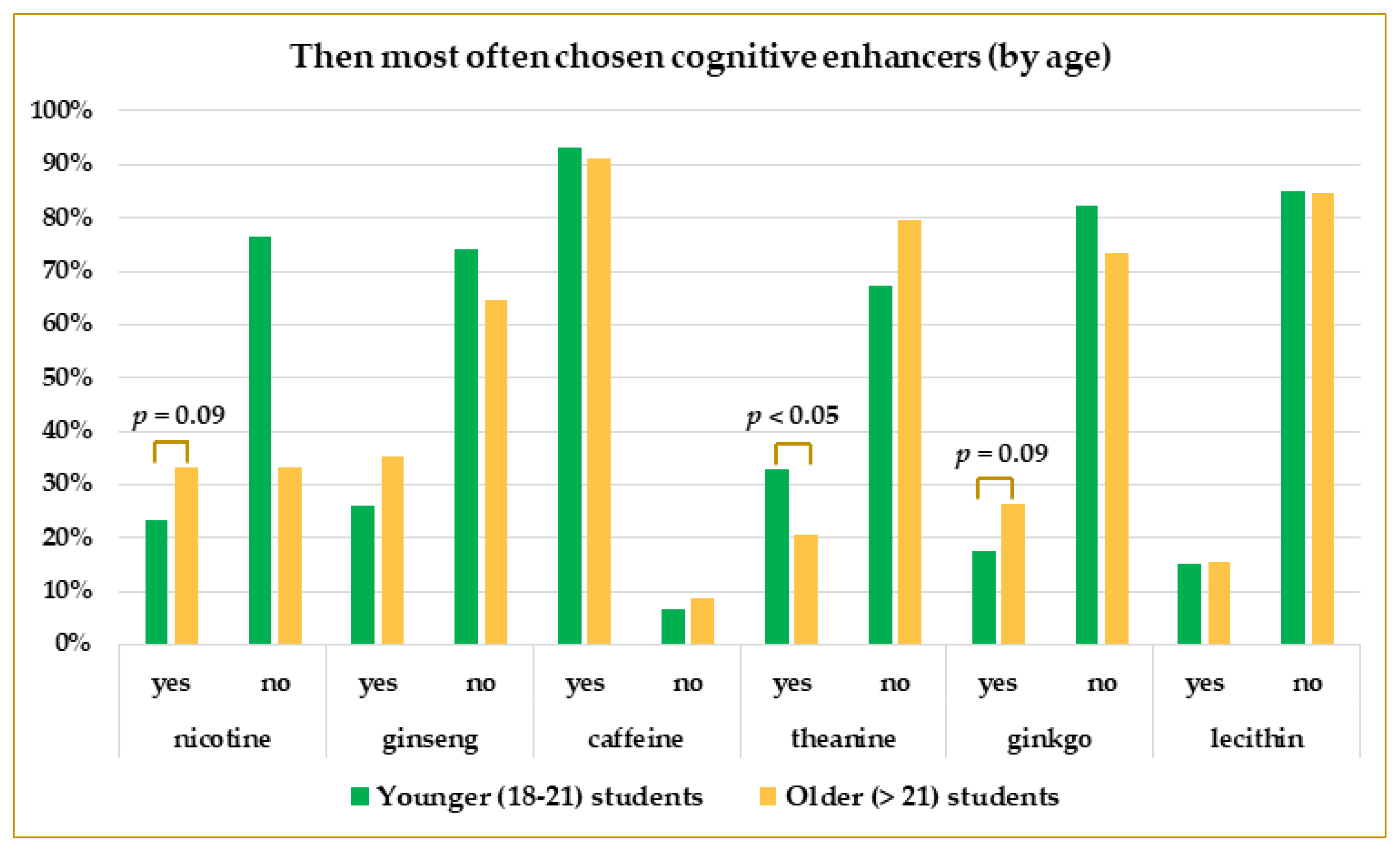
3.2. The Use of Cognitive Enhancers
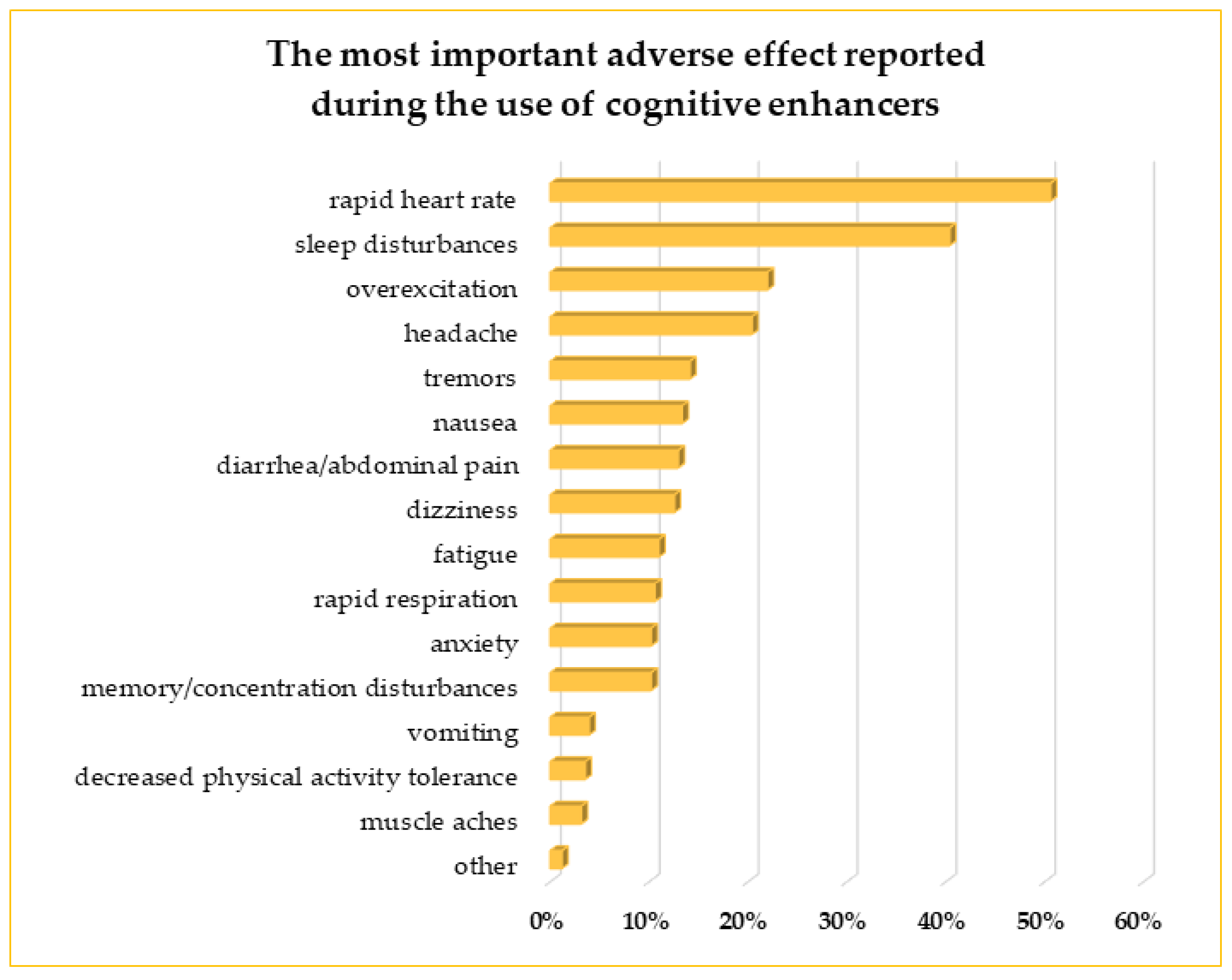
3.3. The Adverse Effects of CEs
3.4. The Impact of COVID-19 on the Use of CEs
4. Discussion
4.1. Demographic Data
4.2. The Use of Cognitive Enhancers
4.3. The Adverse Effects of CEs
4.4. The Impact of COVID-19 on CEs Use
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dresler, M.; Sandberg, A.; Ohla, K.; Bublitz, C.; Trenado, C.; Mroczko-Wąsowicz, A.; Kühn, S.; Repantis, D. Non-pharmacological cognitive enhancement. Neuropharmacology 2013, 64, 529–543. [Google Scholar] [CrossRef]
- Sachdeva, A.; Kumar, K.; Anand, K.S. Non Pharmacological cognitive enhancers–current perspectives. J. Clin. Diagn. Res. 2015, 9, VE01–VE06. [Google Scholar] [CrossRef]
- Ram, S.; Russell, B.; Kirkpatrick, C.; Stewart, K.; Scahill, S.; Henning, M.; Curley, L.; Hussainy, S. Professionals’ attitudes towards the use of cognitive enhancers in academic settings. PLoS ONE 2020, 15, e0241968. [Google Scholar] [CrossRef] [PubMed]
- Schelle, K.J.; Faulmüller, N.; Caviola, L.; Hewstone, M. Attitudes toward Pharmacological Cognitive Enhancement—A Review. Front. Syst. Neurosci. 2014, 8, 53. [Google Scholar] [CrossRef] [Green Version]
- Napoletano, F.; Schifano, F.; Corkery, J.M.; Guirguis, A.; Arillotta, D.; Zangani, C.; Vento, A. The psychonauts’ world of cognitive enhancers. Front. Psychiatry 2020, 11, 546796. [Google Scholar] [CrossRef]
- Biggs, J.M.; Morgan, J.A.; Lardieri, A.B.; Kishk, O.A.; Klein-Schwartz, W. Abuse and misuse of selected dietary supplements among adolescents: A look at poison center data. J. Pediatr. Pharmacol. Ther. 2017, 22, 385–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiba, T.; Kobayashi, E.; Okura, T.; Sekimoto, M.; Mizuno, H.; Saito, M.; Umegaki, K. An educational intervention improved knowledge of dietary supplements in college students. BMC Public Health 2020, 20, 633. [Google Scholar] [CrossRef] [PubMed]
- TNS study: A Quarter of Respondents Believe That the Supplement Cannot Be Overdosed [in Polish]. Available online: https://www.rynekzdrowia.pl/Farmacja/Badanie-TNS-jedna-czwarta-ankietowanych-sadzi-ze-suplementu-nie-mozna-przedawkowac,139554,6.html (accessed on 8 October 2022).
- Sandi, C. Stress and cognition. Wiley Interdiscip. Rev. Cogn. Sci. 2013, 4, 245–261. [Google Scholar] [CrossRef]
- Jahangeer, S.M.A.; Hamdan, M.; Ansari, U.S.; Khan, H.S.; Fatima, R. Cognition improvement strategies, study behaviors and stress among medical students of Dow University of Health Sciences: A cross-sectional study. J. Pak. Med. Assoc. 2022, 72, 1363–1368. [Google Scholar] [CrossRef]
- Kusturica, J.; Hajdarević, A.; Nikšić, H.; Skopljak, A.; Tafi, Z.; Kulo, A. Neuroenhancing substances use, exam anxiety and academic performance in Bosnian-Herzegovinian first-year university students. Acta Med. Acad. 2019, 48, 286–293. [Google Scholar] [CrossRef]
- Merwid-Ląd, A.; Szandruk-Bender, M.; Matuszewska, A.; Trocha, M.; Nowak, B.; Oster, M.; Szeląg, A. Factors that influence the use of dietary supplements among the students of Wroclaw Medical University in Poland during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2022, 19, 7485. [Google Scholar] [CrossRef]
- Racine, E.; Sattler, S.; Boehlen, W. Cognitive enhancement: Unanswered questions about human psychology and social behavior. Sci. Eng. Ethics 2021, 27, 19. [Google Scholar] [CrossRef]
- Erasmus, N.; Kotzé, C. Medical students’ attitudes towards pharmacological cognitive enhancement with methylphenidate. Acad. Psychiatry 2020, 44, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Ram, S.S.; Hussainy, S.; Henning, M.; Stewart, K.; Jensen, M.; Russell, B. Attitudes toward cognitive enhancer use among New Zealand tertiary students. Subst. Use Misuse 2017, 52, 1387–1392. [Google Scholar] [CrossRef] [PubMed]
- Forlini, C.; Racine, E. Autonomy and coercion in academic “cognitive enhancement” using methylphenidate: Perspectives of key stakeholders. Neuroethics 2009, 2, 163–177. [Google Scholar] [CrossRef]
- Carton, L.; Cabé, N.; Ménard, O.; Deheul, S.; Caous, A.-S.; Devos, D.; Cottencin, O.; Bordet, R. Pharmaceutical cognitive doping in students: A chimeric way to get-a-head? Therapie 2018, 73, 319–329, In French. [Google Scholar] [CrossRef]
- Cavaco, A.M.; Ribeiro, J.; Nørgaard, L.S. Exploring the use of cognitive enhancement substances among Portuguese University Students. Explor. Res. Clin. Soc. Pharm. 2022, 5, 100097. [Google Scholar] [CrossRef]
- Lengvenyte, A.; Strumila, R.; Grikiniene, J. Use of cognitive enhancers among medical students in Lithuania. Nord. Stud. Alcohol Drugs 2016, 33, 173–188. [Google Scholar] [CrossRef]
- Sample Size Calculator. Available online: https://www.calculator.net/sample-size-calculator.html?type=2&cl2=95&ss2=400&pc2=15&ps2=5200000&x=38&y=29#findci (accessed on 29 December 2022).
- Sample Size Formula-What Is Sample Size Formula? Examples. Available online: https://www.cuemath.com/sample-size-formula/ (accessed on 3 March 2023).
- GUS Higher Education in the Academic Year 2021/2022 (Preliminary Results) [in Polish]. Available online: https://stat.gov.pl/obszary-tematyczne/edukacja/edukacja/szkolnictwo-wyzsze-w-roku-akademickim-20212022-wyniki-wstepne,8,8.html (accessed on 29 December 2022).
- About the National Reconstruction Plan—National Reconstruction Plan—Gov.pl Website [in Polish]. Available online: https://www.gov.pl/web/planodbudowy/o-kpo (accessed on 29 December 2022).
- Gender Equality Plan for the WMU for 2022-2024 | Medical University of Silesian Piasts in Wrocław [in Polish]. Available online: https://www.umw.edu.pl/pl/aktualnosci/plan-rownosci-plci-dla-umw-na-lata-2022-2024 (accessed on 29 December 2022).
- Batisse, A.; Leger, S.; Vicaut, E.; Gerbaud, L.; Djezzar, S. Cognitive enhancement and consumption of psychoactive substances among youth students (COSYS): A cross-sectional study in France. Public Health 2021, 194, 75–78. [Google Scholar] [CrossRef]
- Heller, S.; Tibubos, A.N.; Hoff, T.A.; Werner, A.M.; Reichel, J.L.; Mülder, L.M.; Schäfer, M.; Pfirrmann, D.; Stark, B.; Rigotti, T.; et al. Potential risk groups and psychological, psychosocial, and health behavioral predictors of pharmacological neuroenhancement among university students in Germany. Sci. Rep. 2022, 12, 937. [Google Scholar] [CrossRef]
- Mousavi, F.; Shojaei, P.; Markeh, H.P. The Use of cognitive enhancers among medical students. Int. J. High Risk Behav. Addict. 2019, 8, e92377. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.T.; Rakow, T.; Gardner, B.; Dommett, E.J. Understanding the relationship between safety beliefs and knowledge for cognitive enhancers in UK university students. PLoS ONE 2021, 16, e0244865. [Google Scholar] [CrossRef] [PubMed]
- Sümbül-Şekerci, B.; Bildik, Ö.; Bektay, M.Y.; İzzettin, F.V. Attitudes of medicine, pharmacy, and dentistry students about psychostimulant use to enhance cognition. Int. J. Clin. Pract. 2021, 75, e14608. [Google Scholar] [CrossRef]
- Sharif, S.; Fergus, S.; Guirguis, A.; Smeeton, N.; Schifano, F. Assessing prevalence, knowledge and use of cognitive enhancers among university students in the United Arab Emirates: A quantitative study. PLoS ONE 2022, 17, e0262704. [Google Scholar] [CrossRef]
- Miranda, M.; Barbosa, M. Use of cognitive enhancers by Portuguese Medical Students: Do academic challenges matter? Acta Medica Port. 2022, 35, 257–263. [Google Scholar] [CrossRef] [PubMed]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A Review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef] [Green Version]
- Pighi, M.; Pontoni, G.; Sinisi, A.; Ferrari, S.; Mattei, G.; Pingani, L.; Simoni, E.; Galeazzi, G.M. Use and propensity to use substances as cognitive enhancers in Italian medical students. Brain Sci. 2018, 8, 197. [Google Scholar] [CrossRef] [Green Version]
- Plumber, N.; Majeed, M.; Ziff, S.; Thomas, S.E.; Bolla, S.R.; Gorantla, V.R. Stimulant usage by medical students for cognitive enhancement: A systematic review. Cureus 2021, 13, e15163. [Google Scholar] [CrossRef]
- Al Ghali, R.M.; Al Shaibi, H.; Al Majed, H.; Haroun, D. Caffeine consumption among Zayed University students in Dubai, United Arab Emirates: A cross-sectional study. Arab. J. Nutr. Exerc. (AJNE) 2017, 1, 131–141. [Google Scholar] [CrossRef] [Green Version]
- Ágoston, C.; Urbán, R.; Király, O.; Griffiths, M.D.; Rogers, P.J.; Demetrovics, Z. Why do you drink caffeine? The development of the Motives for Caffeine Consumption Questionnaire (MCCQ) and its relationship with gender, age and the types of caffeinated beverages. Int. J. Ment. Health. Addict. 2018, 16, 981–999. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.O.; Wightman, E.L. Mental performance and sport: Caffeine and co-consumed bioactive ingredients. Sports Med. 2022, 52, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Lho, S.K.; Kim, T.H.; Kwak, K.P.; Kim, K.; Kim, B.J.; Kim, S.G.; Kim, J.L.; Kim, T.H.; Moon, S.W.; Park, J.Y.; et al. Effects of lifetime cumulative ginseng intake on cognitive function in late life. Alzheimer’s Res. Ther. 2018, 10, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoklosa, M.; Pogorzelczyk, K.; Balwicki, Ł. Research: Tools to Reduce Tobacco Use Among Young People in Poland: Addressing Affordability and Accessibility of Tobacco Products through Taxation and Other Measures. Available online: https://tobacconomics.org (accessed on 9 January 2023).
- Zielińska-Danch, W. The prevalence of waterpipe tobacco smoking among Polish youths—PubMed. Arch. Med. Sci. 2021, 17, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Valentine, G.; Sofuoglu, M. Cognitive effects of nicotine: Recent progress. Curr. Neuropharmacol. 2018, 16, 403–414. [Google Scholar] [CrossRef]
- Safarini, O.A.; Taya, H.; Abu Elhija, Y.; Qadous, M.; Farhoud, A.; Thabaleh, A.; Khayyat, A.; Nazzal, Z.; Abuhassan, A.M.; Ghanim, N.; et al. Assessment of the relationship of depression with tobacco and caffeine use among university students: A cross-sectional study. Cureus 2021, 13, e19098. [Google Scholar] [CrossRef]
- Wilms, W.; Woźniak-Karczewska, M.; Corvini, P.F.-X.; Chrzanowski, Ł. Nootropic drugs: Methylphenidate, modafinil and piracetam—Population use trends, occurrence in the environment, ecotoxicity and removal methods—A review. Chemosphere 2019, 233, 771–785. [Google Scholar] [CrossRef]
- Register of Medicinal Products [in Polish]. Available online: https://rejestrymedyczne.ezdrowie.gov.pl/rpl/search/public (accessed on 4 January 2023).
- Rozenek, E.B.; Górska, M.; Wilczyńska, K.; Waszkiewicz, N. In search of optimal psychoactivation: Stimulants as cognitive performance enhancers. Arch. Ind. Hyg. Toxicol. 2019, 70, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.E.; Farah, M.J. Are Prescription stimulants “Smart Pills”? The epidemiology and cognitive neuroscience of prescription stimulant use by normal healthy individuals. Psychol. Bull. 2011, 137, 717–741. [Google Scholar] [CrossRef] [Green Version]
- Sattler, S.; Sauer, C.; Mehlkop, G.; Graeff, P. The Rationale for consuming cognitive enhancement drugs in university students and teachers. PLoS ONE 2013, 8, e68821. [Google Scholar] [CrossRef]
- Lorca, C.; Mulet, M.; Arévalo-Caro, C.; Sanchez, M.Á.; Perez, A.; Perrino, M.; Bach-Faig, A.; Aguilar-Martínez, A.; Vilella, E.; Gallart-Palau, X.; et al. Plant-derived nootropics and human cognition: A systematic review. Crit. Rev. Food Sci. Nutr. 2022, 1–25. [Google Scholar] [CrossRef]
- Repantis, D.; Bovy, L.; Ohla, K.; Kühn, S.; Dresler, M. Cognitive enhancement effects of stimulants: A randomized controlled trial testing methylphenidate, modafinil, and caffeine. Psychopharmacology 2021, 238, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Dietz, P.; Werner, A.M.; Reichel, J.L.; Schäfer, M.; Mülder, L.M.; Beutel, M.; Simon, P.; Letzel, S.; Heller, S. The Prevalence of pharmacological neuroenhancement among university students before and during the COVID-19-pandemic: Results of three consecutive cross-sectional survey studies in Germany. Front. Public Health 2022, 10, 813328. [Google Scholar] [CrossRef] [PubMed]
- Carletto, S.; Lo Moro, G.; Zuccaroli Lavista, V.; Soro, G.; Siliquini, R.; Bert, F.; Leombruni, P. The impact of COVID-19 on mental health in medical students: A Cross-sectional survey study in Italy. Psychol. Rep. 2022, 332941221127632. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.-K.; Alkon, D.L. Stress: Perspectives on its impact on cognition and pharmacological treatment. Behav. Pharmacol. 2014, 25, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, G.; Mendinca, N.L.; Kar, M. Evaluation of Examination stress and its effect on cognitive function among first year medical students. J. Clin. Diagn. Res. 2014, 8, BC05-07. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Overall Use of Cognitive Enhancers | ||||
|---|---|---|---|---|
| YES | NO | p-Value | ||
| Gender | Women (n = 302) | 49% | 51% | p = 0.0154 |
| Men (n = 177) | 60.5% | 39.5% | ||
| Faculty | Medical (n = 421) | 52.3% | 47.7% | p = 0.2471 |
| Dentistry (n = 58) | 60.3% | 39.7% | ||
| Age | Students 18–21 years of age (n = 250) | 47.6% | 52.4% | p = 0.0098 |
| Students over 21 years of age older (n = 229) | 59.4% | 40.6% | ||
| The Frequency of the Cognitive Enhancers’ Usage | ||||||
|---|---|---|---|---|---|---|
| Every Day | A Few Times per Week | A Few Times per Month | A Few Times per Year | p-Value | ||
| Gender | Women (n = 148) | 47.3% | 23% | 12.2% | 17.5% | p = 0.5355 |
| Men (n = 107) | 40.2% | 24.3% | 11.2% | 24.3% | ||
| Faculty | Medical (n = 220) | 45% | 23.2% | 11.3% | 20.5% | p = 0.9244 |
| Dentistry (n = 36) | 40% | 25.7% | 14.3% | 20% | ||
| Age | Students 18–21 years of age (n = 119) | 42% | 26.9% | 16% | 15.1% | p = 0.0522 |
| Students over 21 years of age (n = 136) | 46.3% | 20.6% | 8.1% | 25% | ||
| Dependent Factors | The Use of Nicotine | The Use of Ginseng | The Use of Caffeine | The Use of Theanine | The Use of Ginkgo | The Use of Lecithin | |
|---|---|---|---|---|---|---|---|
| Independent Factors | |||||||
| OR | OR | OR | OR | OR | OR | ||
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | (95% CI) | ||
| B Coefficient | B Coefficient | B Coefficient | B Coefficient | B Coefficient | B Coefficient | ||
| p-Value | p-Value | p-Value | p-Value | p-Value | p-Value | ||
| Gender (ref. Women) | 3.30 | 0.48 | 0.91 | 0.67 | 0.45 | 0.57 | |
| (1.86–5.87) | (0.27–0.85) | (0.36–2.31) | (0.38–1.22) | (0.23–0.88) | (0.27–1.23) | ||
| 1.19 | −0.73 | −0.09 | −0.39 | −0.80 | −0.56 | ||
| p = 0.0001 | p = 0.0124 | p = 0.8449 | p = 0.1939 | p = 0.0193 | p = 0.1525 | ||
| Faculty (ref. Medical) | 0.73 | 0.99 | 1.47 | 0.64 | 2.69 | 3.37 | |
| (0.29–1.81) | (0.46–2.15) | (0.32–6.77) | (0.26–1.57) | (1.25–5.81) | (1.48–7/65) | ||
| −0.32 | −0.01 | 0.39 | −0.45 | 0.99 | 1.21 | ||
| p = 0.4877 | p = 0.9784 | p = 0.6173 | p = 0.3266 | p = 0.0115 | p = 0.0037 | ||
| Age (ref. Students 18–21 years of age) | 1.66 | 1.58 | 0.74 | 0.54 | 1.67 | 0.97 | |
| (0.93–2.95) | (0.92–2.74) | (0.29–1.87) | (0.31–0.95) | (0.90–3.13) | (0.48–1.97) | ||
| 0.50 | 0.46 | −0.31 | −0.62 | 0.52 | −0.03 | ||
| p = 0.0868 | p = 0.1002 | p = 0.5198 | p = 0.0335 | p = 0.1056 | p = 0.9377 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merwid-Ląd, A.; Passon, M.; Drymluch, P.; Głuszyński, M.; Szeląg, A.; Matuszewska, A. Do Medical Universities Students Use Cognitive Enhancers while Learning?—Conclusions from the Study in Poland. Life 2023, 13, 820. https://doi.org/10.3390/life13030820
Merwid-Ląd A, Passon M, Drymluch P, Głuszyński M, Szeląg A, Matuszewska A. Do Medical Universities Students Use Cognitive Enhancers while Learning?—Conclusions from the Study in Poland. Life. 2023; 13(3):820. https://doi.org/10.3390/life13030820
Chicago/Turabian StyleMerwid-Ląd, Anna, Michał Passon, Paweł Drymluch, Maciej Głuszyński, Adam Szeląg, and Agnieszka Matuszewska. 2023. "Do Medical Universities Students Use Cognitive Enhancers while Learning?—Conclusions from the Study in Poland" Life 13, no. 3: 820. https://doi.org/10.3390/life13030820