
Relationship of FDG Uptake of the Reticuloendothelial System with Tumor Immune Microenvironment and Prognosis in Patients with Gastric Cancer
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. FDG PET/CT Acquisition and Image Analysis
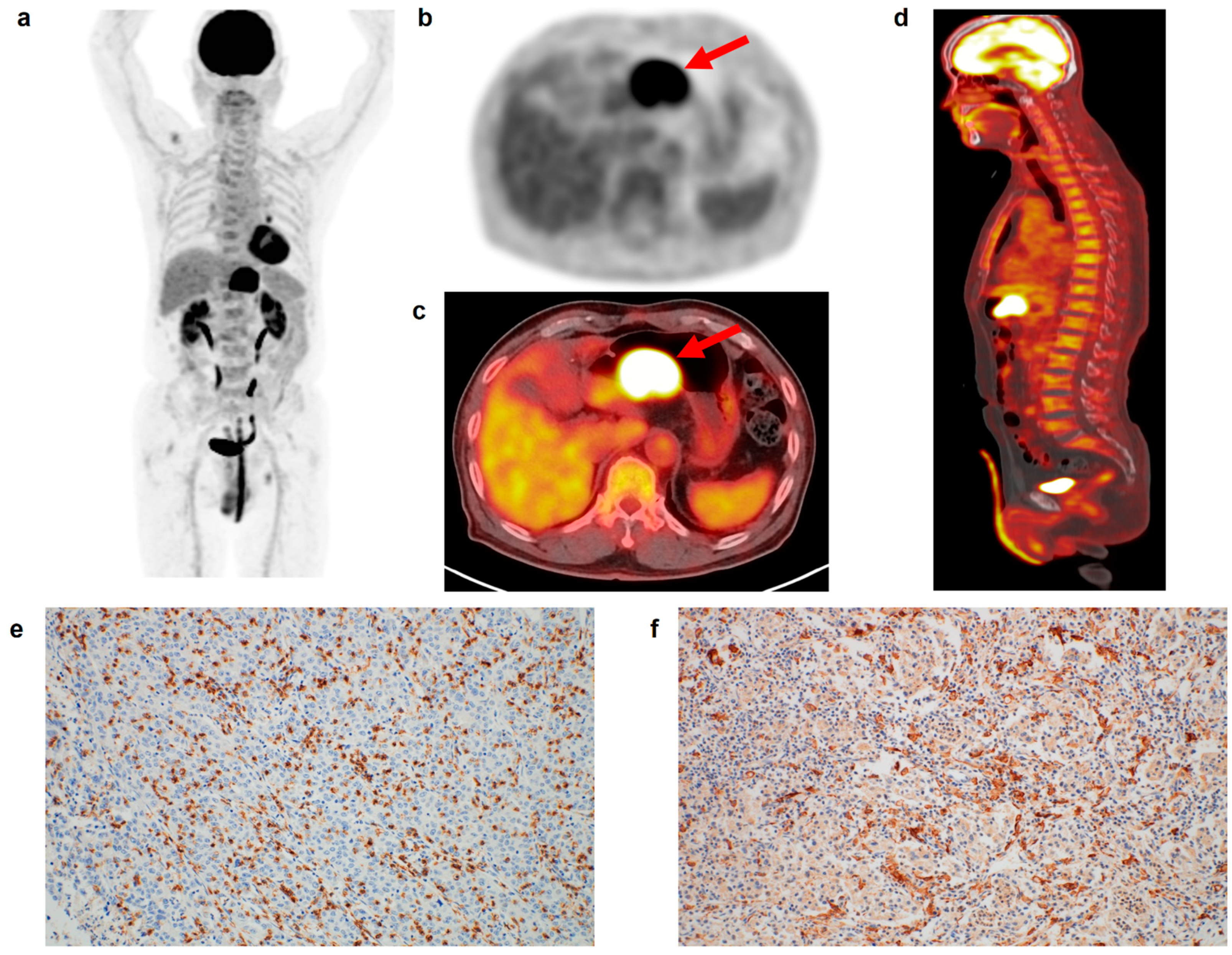
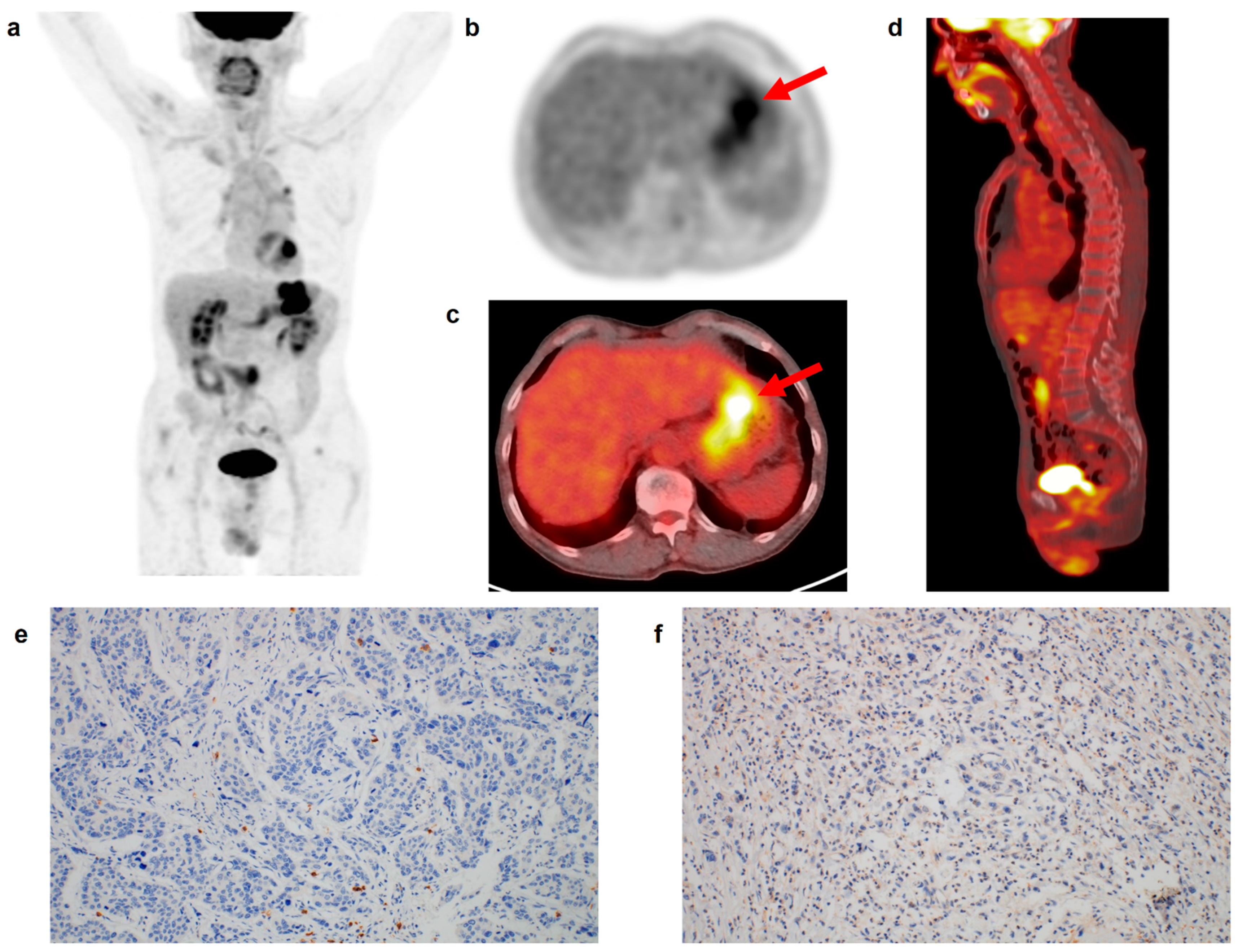
2.3. Immunohistochemical Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
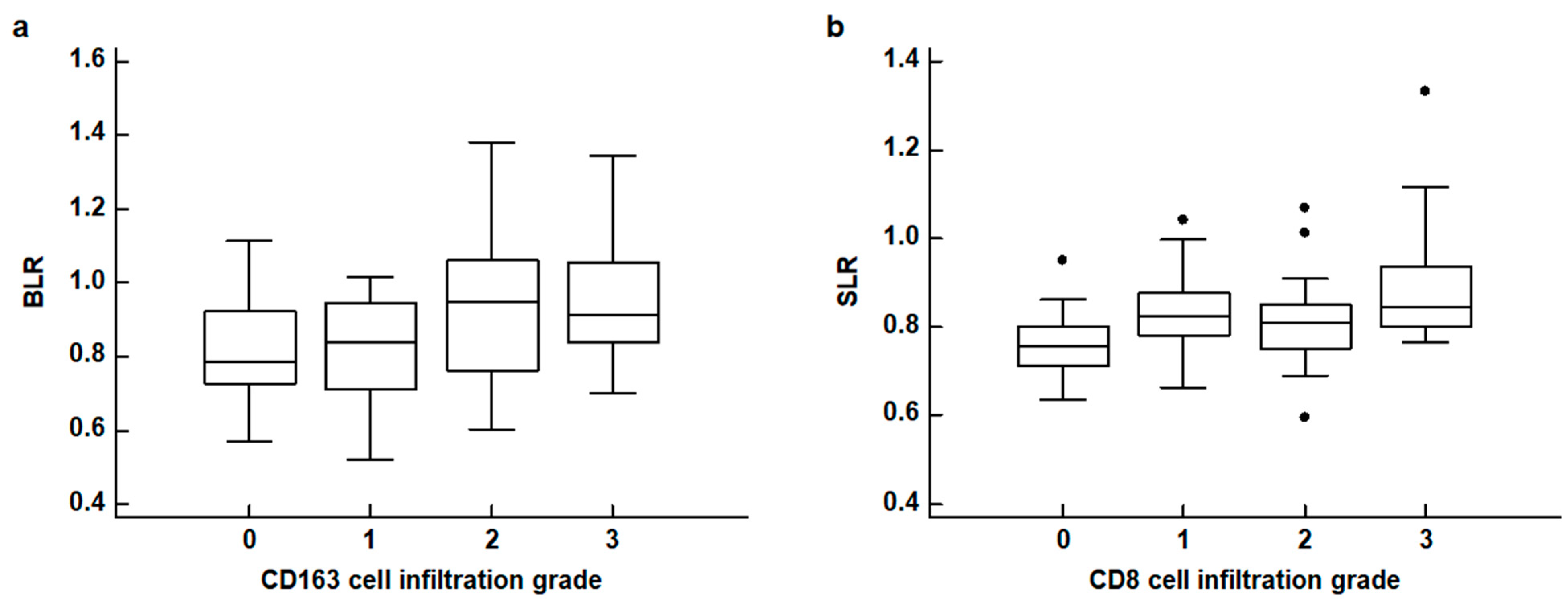
3.2. Correlation Analysis
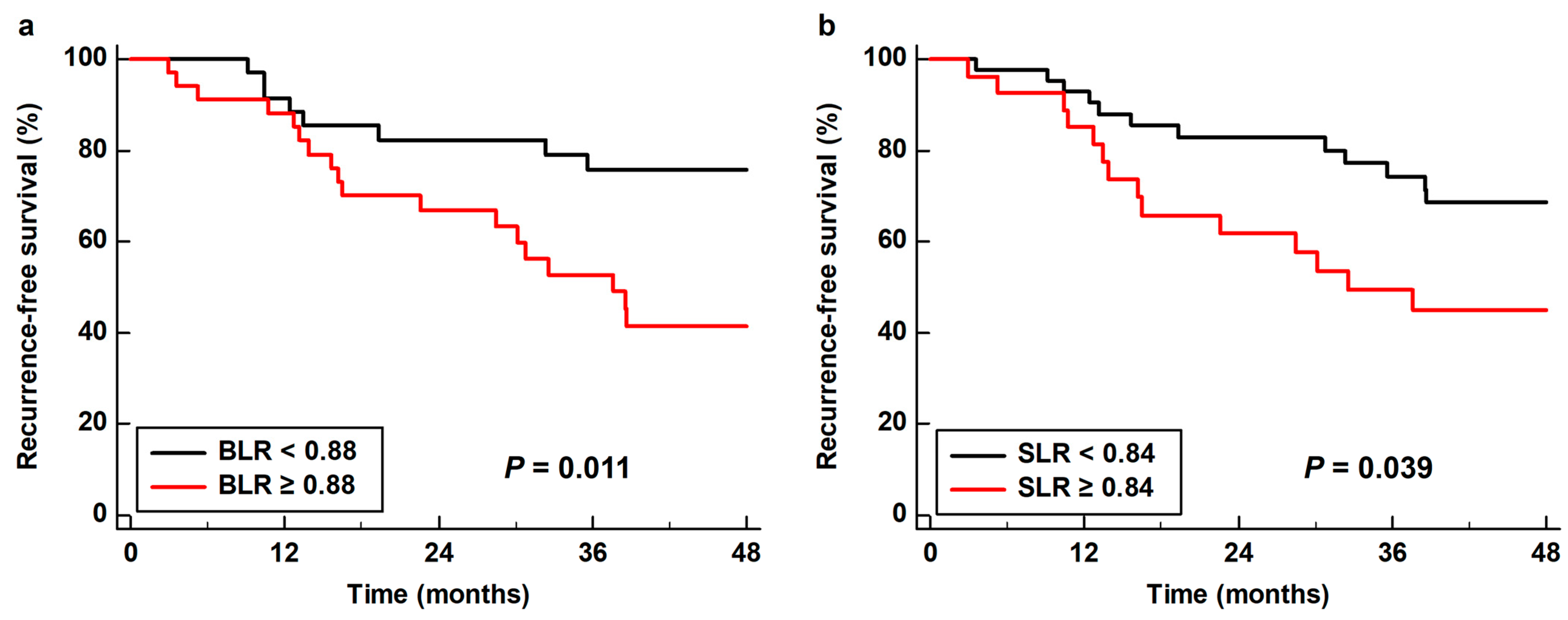
3.3. Survival Analysis for RFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hibino, S.; Kawazoe, T.; Kasahara, H.; Itoh, S.; Ishimoto, T.; Sakata-Yanagimoto, M.; Taniguchi, K. Inflammation-induced tumorigenesis and metastasis. Int. J. Mol. Sci. 2021, 22, 5421. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Zhu, Y.; Zhang, C.; Yang, X.; Gao, Y.; Li, M.; Yang, H.; Liu, T.; Tang, H. Chronic inflammation, cancer development and immunotherapy. Front. Pharmacol. 2022, 13, 1040163. [Google Scholar] [CrossRef]
- Kim, E.E.; Youn, H.; Kang, K.W. Imaging in tumor immunology. Nucl. Med. Mol. Imaging 2021, 55, 225–236. [Google Scholar] [CrossRef]
- Jaroenlapnopparat, A.; Bhatia, K.; Coban, S. Inflammation and gastric cancer. Diseases 2022, 10, 35. [Google Scholar] [CrossRef]
- Gu, L.; Wang, M.; Cui, X.; Mo, J.; Yuan, L.; Mao, F.; Zhang, K.; Ng, D.M.; Chen, P.; Wang, D. Clinical significance of peripheral blood-derived inflammation markers in advanced gastric cancer after radical resection. BMC Surg. 2020, 20, 219. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.R.; Kim, A.S.; Choi, H.I.; Jung, J.H.; Park, J.Y.; Ko, H.J. Inflammatory markers for predicting overall survival in gastric cancer patients: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0236445. [Google Scholar] [CrossRef]
- Liu, Y.; Li, C.; Lu, Y.; Liu, C.; Yang, W. Tumor microenvironment-mediated immune tolerance in development and treatment of gastric cancer. Front. Immunol. 2022, 13, 1016817. [Google Scholar] [CrossRef]
- Thompson, E.D.; Zahurak, M.; Murphy, A.; Cornish, T.; Cuka, N.; Abdelfatah, E.; Yang, S.; Duncan, M.; Ahuja, N.; Taube, J.M.; et al. Patterns of PD-L1 expression and CD8 T cell infiltration in gastric adenocarcinomas and associated immune stroma. Gut 2017, 66, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Piao, H.; Fu, L.; Wang, Y.; Liu, Y.; Wang, Y.; Meng, X.; Yang, D.; Xiao, X.; Zhang, J. A positive feedback loop between gastric cancer cells and tumor-associated macrophage induces malignancy progression. J. Exp. Clin. Cancer Res. 2022, 41, 174. [Google Scholar] [CrossRef]
- Zhang, Z.; Zheng, B.; Chen, W.; Xiong, H.; Jiang, C. Accuracy of 18F-FDG PET/CT and CECT for primary staging and diagnosis of recurrent gastric cancer: A meta-analysis. Exp. Ther. Med. 2021, 21, 164. [Google Scholar] [CrossRef]
- Moon, S.H.; Cho, Y.S.; Choi, J.Y. KSNM60 in clinical nuclear oncology. Nucl. Med. Mol. Imaging 2021, 55, 210–224. [Google Scholar] [CrossRef]
- Ahn, H.; Song, G.J.; Jang, S.H.; Lee, H.J.; Lee, M.S.; Lee, J.H.; Oh, M.H.; Jeong, G.C.; Lee, S.M.; Lee, J.W. Relationship of FDG PET/CT textural features with the tumor microenvironment and recurrence risks in patients with advanced gastric cancers. Cancers 2022, 14, 3936. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.W.; Lee, J.H.; Jo, I.Y.; Jang, S.J. Prognostic Value of Dual-Time-Point [18F]FDG PET/CT for predicting distant metastasis after treatment in patients with non-small cell lung cancer. J. Pers. Med. 2022, 12, 592. [Google Scholar] [CrossRef] [PubMed]
- De Jaeghere, E.A.; Laloo, F.; Lippens, L.; Van Bockstal, M.; De Man, K.; Naert, E.; Van Dorpe, J.; Van de Vijver, K.; Tummers, P.; Makar, A.; et al. Splenic 18F-FDG uptake on baseline PET/CT is associated with oncological outcomes and tumor immune state in uterine cervical cancer. Gynecol. Oncol. 2020, 159, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Bural, G.G.; Torigian, D.A.; Chen, W.; Houseni, M.; Basu, S.; Alavi, A. Increased 18F-FDG uptake within the reticuloendothelial system in patients with active lung cancer on PET imaging may indicate activation of the systemic immune response. Hell. J. Nucl. Med. 2010, 13, 23–25. [Google Scholar] [PubMed]
- Parker, C.C.; Lapi, S.E. Positron emission tomography imaging of macrophages in cancer. Cancers 2021, 13, 1921. [Google Scholar] [CrossRef] [PubMed]
- Kashimura, M. The human spleen as the center of the blood defense system. Int. J. Hematol. 2020, 112, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, H.S.; Kim, S.; Park, E.J.; Baik, S.H.; Jeon, T.J.; Lee, K.Y.; Ryu, Y.H.; Kang, J. Prognostic significance of bone marrow and spleen 18F-FDG uptake in patients with colorectal cancer. Sci. Rep. 2021, 11, 12137. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, M.; Norikane, T.; Yamamoto, Y.; Imajo, M.; Takami, Y.; Mitamura, K.; Tanaka, T.; Tsuruta, T.; Kanenishi, K.; Nishiyama, Y. Correlation of bone marrow 2-deoxy-2-[18F]fluoro-D-glucose uptake with systemic inflammation in patients with newly diagnosed endometrial cancer. Nucl. Med. Commun. 2022, 43, 916–921. [Google Scholar] [CrossRef]
- Lee, J.W.; Park, S.H.; Ahn, H.; Lee, S.M.; Jang, S.J. Predicting survival in patients with pancreatic cancer by integrating bone marrow FDG uptake and radiomic features of primary tumor in PET/CT. Cancers 2021, 13, 3563. [Google Scholar] [CrossRef]
- Kim, S.Y.; Moon, C.M.; Yoon, H.J.; Kim, B.S.; Lim, J.Y.; Kim, T.O.; Choe, A.R.; Tae, C.H.; Kim, S.E.; Jung, H.K.; et al. Diffuse splenic FDG uptake is predictive of clinical outcomes in patients with rectal cancer. Sci. Rep. 2019, 9, 1313. [Google Scholar] [CrossRef] [Green Version]
- Seban, R.D.; Rouzier, R.; Latouche, A.; Deleval, N.; Guinebretiere, J.M.; Buvat, I.; Bidard, F.C.; Champion, L. Total metabolic tumor volume and spleen metabolism on baseline [18F]-FDG PET/CT as independent prognostic biomarkers of recurrence in resected breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3560–3570. [Google Scholar] [CrossRef]
- Shimura, K.; Mabuchi, S.; Komura, N.; Yokoi, E.; Kozasa, K.; Sasano, T.; Kawano, M.; Matsumoto, Y.; Watabe, T.; Kodama, M.; et al. Prognostic significance of bone marrow FDG uptake in patients with gynecological cancer. Sci. Rep. 2021, 11, 2257. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, M.S.; Chung, I.K.; Son, M.W.; Cho, Y.S.; Lee, S.M. Clinical implication of FDG uptake of bone marrow on PET/CT in gastric cancer patients with surgical resection. World J. Gastroenterol. 2017, 23, 2385–2395. [Google Scholar] [CrossRef]
- Yoon, H.J.; Kim, B.S.; Moon, C.M.; Yoo, J.; Lee, K.E.; Kim, Y. Prognostic value of diffuse splenic FDG uptake on PET/CT in patients with gastric cancer. PLoS ONE 2018, 13, e0196110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seban, R.D.; Assié, J.B.; Giroux-Leprieur, E.; Massiani, M.A.; Bonardel, G.; Chouaid, C.; Deleval, N.; Richard, C.; Mezquita, L.; Girard, N.; et al. Prognostic value of inflammatory response biomarkers using peripheral blood and [18F]-FDG PET/CT in advanced NSCLC patients treated with first-line chemo- or immunotherapy. Lung Cancer 2021, 159, 45–55. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, S.C.; Kim, H.J.; Lee, S.M. Prognostic value of bone marrow (18)F-FDG uptake on PET/CT in lymphoma patients with negative bone marrow involvement. Hell. J. Nucl. Med. 2017, 20, 17–25. [Google Scholar] [CrossRef]
- Elstrom, R.L.; Tsai, D.E.; Vergilio, J.A.; Downs, L.H.; Alavi, A.; Schuster, S.J. Enhanced marrow [18F]fluorodeoxyglucose uptake related to myeloid hyperplasia in Hodgkin’s lymphoma can simulate lymphoma involvement in marrow. Clin. Lymphoma 2004, 5, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Ban, M.J.; Park, J.H.; Lee, S.M. Effect of F-18 fluorodeoxyglucose uptake by bone marrow on the prognosis of head and neck squamous cell carcinoma. J. Clin. Med. 2019, 8, 1169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pak, K.; Kim, S.J.; Kim, I.J.; Kim, D.U.; Kim, K.; Kim, H. Impact of cytokines on diffuse splenic 18F-fluorodeoxyglucose uptake during positron emission tomography/computed tomography. Nucl. Med. Commun. 2013, 34, 64–70. [Google Scholar] [CrossRef]
- Pak, K.; Kim, S.J.; Kim, I.J.; Kim, D.U.; Kim, K.; Kim, H.; Kim, S.J. Splenic FDG uptake predicts poor prognosis in patients with unresectable cholangiocarcinoma. Nuklearmedizin 2014, 53, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Na, J.O.; Kang, D.Y.; Lee, S.Y.; Lee, S.M. Prognostic significance of FDG uptake of bone marrow on PET/CT in patients with non-small-cell lung cancer after curative surgical resection. Clin. Lung. Cancer. 2017, 18, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Goto, R.; Okada, K.; Kinomura, S.; Fukuda, H. A bone marrow F-18 FDG uptake exceeding the liver uptake may indicate bone marrow hyperactivity. Ann. Nucl. Med. 2009, 23, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Yoo, I.D.; Lee, S.M.; Lee, J.W.; Oh, J.E.; Cho, Y.J.; Shin, H.S. The influence of adipose tissue volume can significantly affect the metabolic activity of reference organs in (18)F-FDG PET/CT studies of a normal healthy population. Hell. J. Nucl. Med. 2017, 20, 211–216. [Google Scholar] [CrossRef]
- Li, W.; Zhang, X.; Wu, F.; Zhou, Y.; Bao, Z.; Li, H.; Zheng, P.; Zhao, S. Gastric cancer-derived mesenchymal stromal cells trigger M2 macrophage polarization that promotes metastasis and EMT in gastric cancer. Cell Death Dis. 2019, 10, 918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwamoto, C.; Ohuchida, K.; Shinkawa, T.; Okuda, S.; Otsubo, Y.; Okumura, T.; Sagara, A.; Koikawa, K.; Ando, Y.; Shindo, K.; et al. Bone marrow-derived macrophages converted into cancer-associated fibroblast-like cells promote pancreatic cancer progression. Cancer Lett. 2021, 512, 15–27. [Google Scholar] [CrossRef]
- Wang, Z.; Dong, Z.; Zhao, G.; Ni, B.; Zhang, Z.Z. Prognostic role of myeloid-derived tumor-associated macrophages at the tumor invasive margin in gastric cancer with liver metastasis (GCLM): A single-center retrospective study. J. Gastrointest. Oncol. 2022, 13, 1340–1350. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Chen, T.; Lin, W.; Zheng, W.; Chen, J.; Huang, F.; Xie, X. Functional tumor specific CD8 + T cells in spleen express a high level of PD-1. Int. Immunopharmacol. 2020, 80, 106242. [Google Scholar] [CrossRef]
- Zhang, N.; Cao, M.; Duan, Y.; Bai, H.; Li, X.; Wang, Y. Prognostic role of tumor-infiltrating lymphocytes in gastric cancer: A meta-analysis and experimental validation. Arch. Med. Sci. 2020, 16, 1092–1103. [Google Scholar] [CrossRef]
- Wei, M.; Shen, D.; Mulmi Shrestha, S.; Liu, J.; Zhang, J.; Yin, Y. The progress of T cell immunity related to prognosis in gastric cancer. Biomed. Res. Int. 2018, 2018, 3201940. [Google Scholar] [CrossRef] [Green Version]
- Rahn, S.; Krüger, S.; Röcken, C.; Helm, O.; Sebens, S. Response to: ‘Patterns of PD-L1 expression and CD8 T cell infiltration in gastric adenocarcinomas and associated immune stroma’. Gut 2019, 68, 179–180. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.G.; Hwang, S.H.; Kim, K.H.; Yoon, H.I.; Shim, H.S.; Lee, J.H.; Han, Y.; Ahn, B.C.; Hong, M.H.; Kim, H.R.; et al. Predicting treatment outcomes using (18)F-FDG PET biomarkers in patients with non-small-cell lung cancer receiving chemoimmunotherapy. Ther. Adv. Med. Oncol. 2022, 14, 17588359211068732. [Google Scholar] [CrossRef]
- Lee, J.W.; Jeon, S.; Mun, S.T.; Lee, S.M. Prognostic value of fluorine-18 fluorodeoxyglucose uptake of bone marrow on positron emission tomography/computed tomography for prediction of disease progression in cervical cancer. Int. J. Gynecol. Cancer 2017, 27, 776–783. [Google Scholar] [CrossRef]
- Lee, J.W.; Kim, S.Y.; Han, S.W.; Lee, J.E.; Lee, H.J.; Heo, N.H.; Lee, S.M. [(18)F]FDG uptake of bone marrow on PET/CT for predicting distant recurrence in breast cancer patients after surgical resection. EJNMMI Res. 2020, 10, 72. [Google Scholar] [CrossRef]
- Wong, A.; Callahan, J.; Keyaerts, M.; Neyns, B.; Mangana, J.; Aberle, S.; Herschtal, A.; Fullerton, S.; Milne, D.; Iravani, A.; et al. (18)F-FDG PET/CT based spleen to liver ratio associates with clinical outcome to ipilimumab in patients with metastatic melanoma. Cancer Imaging 2020, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Mattonen, S.A.; Davidzon, G.A.; Benson, J.; Leung, A.N.C.; Vasanawala, M.; Horng, G.; Shrager, J.B.; Napel, S.; Nair, V.S. Bone marrow and tumor radiomics at (18)F-FDG PET/CT: Impact on outcome prediction in non-small cell lung cancer. Radiology 2019, 293, 451–459. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. of Patients (%) | Median (Interquartile Range) | |
|---|---|---|---|
| Age (years) | 60 (52–72) | ||
| Sex | Men | 39 (55.7%) | |
| Women | 31 (44.3%) | ||
| Tumor location | Upper | 8 (11.4%) | |
| Middle | 28 (40.0%) | ||
| Lower | 34 (48.6%) | ||
| WHO histopathological classification | Papillary/tubular types | 44 (62.9%) | |
| Mucinous/signet ring cells and other poorly cohesive types | 26 (37.1%) | ||
| Lauren classification | Intestinal type | 30 (42.9%) | |
| Diffuse/indeterminate types | 40 (57.1%) | ||
| T stage | T1–T2 stage | 26 (37.1%) | |
| T2–T4 stage | 44 (62.9%) | ||
| N stage | N0 stage | 29 (41.4%) | |
| N1–N3 stage | 41 (58.6%) | ||
| TNM stage | Stage I | 18 (25.7%) | |
| Stage II | 19 (27.1%) | ||
| Stage III | 33 (47.1%) | ||
| Adjuvant chemotherapy | Yes | 42 (60.0%) | |
| No | 28 (40.0%) | ||
| CD4 cell infiltration | Grade 0 | 16 (22.9%) | |
| Grade 1 | 25 (35.7%) | ||
| Grade 2 | 18 (25.7%) | ||
| Grade 3 | 11 (15.7%) | ||
| CD8 cell infiltration | Grade 0 | 12 (17.1%) | |
| Grade 1 | 18 (25.7%) | ||
| Grade 2 | 23 (32.9%) | ||
| Grade 3 | 17 (24.3%) | ||
| CD163 cell infiltration | Grade 0 | 23 (32.9%) | |
| Grade 1 | 22 (31.4%) | ||
| Grade 2 | 13 (18.6%) | ||
| Grade 3 | 12 (17.1%) | ||
| IL-6 expression | Grade 0 | 26 (37.1%) | |
| Grade 1 | 22 (31.4%) | ||
| Grade 2 | 17 (24.3%) | ||
| Grade 3 | 5 (7.1%) | ||
| FDG PET/CT parameters | Tumor SUV | 4.58 (3.32–7.57) | |
| BM SUV | 1.70 (1.48–2.00) | ||
| Spleen SUV | 1.66 (1.44–1.81) | ||
| BLR | 0.88 (0.75–0.98) | ||
| SLR | 0.81 (0.77–0.87) | ||
| Histopathological Factors | BM SUV | p-Value | Spleen SUV | p-Value | BLR | p-Value | SLR | p-Value | |
|---|---|---|---|---|---|---|---|---|---|
| WHO histopathological classification | Papillary/tubular types | 1.69 (1.52–1.97) | 0.723 * | 1.68 (1.44–1.83) | 0.693 * | 0.86 (0.75–0.97) | 0.879 * | 0.82 (0.77–0.87) | 0.346 * |
| Mucinous/signet ring cells and other poorly cohesive types | 1.72 (1.46–2.07) | 1.63 (1.52–1.77) | 0.88 (0.76–0.98) | 0.79 (0.76–0.86) | |||||
| Lauren classification | Intestinal type | 1.67 (1.48–1.95) | 0.618 * | 1.55 (1.39–1.85) | 0.639 * | 0.84 (0.72–0.98) | 0.614 * | 0.81 (0.76–0.85) | 0.753 * |
| Diffuse/indeterminate types | 1.75 (1.51–2.00) | 1.67 (1.52–1.80) | 0.88 (0.76–0.97) | 0.81 (0.77–0.90) | |||||
| TNM stage | Stage I | 1.62 (1.48–1.95) | 0.170 † | 1.70 (1.43–1.81) | 0.636 † | 0.80 (0.71–0.95) | 0.094 † | 0.79 (0.75–0.83) | 0.080 † |
| Stage II | 1.68 (1.46–1.90) | 1.61 (1.40–1.70) | 0.88 (0.75–0.94) | 0.81 (0.77–0.89) | |||||
| Stage III | 1.79 (1.56–2.02) | 1.67 (1.50–1.82) | 0.93 (0.77–1.01) | 0.83 (0.77–0.91) | |||||
| CD4 cell infiltration | Grade 0 | 1.67 (1.47–1.90) | 0.799 † | 1.58 (1.42–1.72) | 0.818 † | 0.80 (0.74–0.91) | 0.571 † | 0.78 (0.74–0.83) | 0.223 † |
| Grade 1 | 1.72 (1.49–2.10) | 1.67 (1.49–1.80) | 0.93 (0.75–0.98) | 0.84 (0.78–0.91) | |||||
| Grade 2 | 1.67 (1.52–2.07) | 1.70 (1.36–88) | 0.87 (0.76–0.98) | 0.81 (0.77–0.91) | |||||
| Grade 3 | 1.73 (1.49–1.90) | 1.66 (1.53–1.75) | 0.84 (0.74–1.01) | 0.81 (0.77–0.86) | |||||
| CD8 cell infiltration | Grade 0 | 1.68 (1.53–1.90) | 0.943 † | 1.58 (1.45–1.64) | 0.472 † | 0.80 (0.68–0.94) | 0.637 † | 0.76 (0.71–0.80) | 0.016 † |
| Grade 1 | 1.75 (1.46–1.99) | 1.72 (1.46–1.88) | 0.88 (0.75–0.95) | 0.82 (0.78–0.88) | |||||
| Grade 2 | 1.65 (1.48–2.07) | 1.56 (1.43–1.75) | 0.89 (0.73–0.98) | 0.81 (0.75–0.85) | |||||
| Grade 3 | 1.79 (1.51–1.96) | 1.71 (1.44–1.85) | 0.88 (0.79–1.02) | 0.84 (0.80–0.94) | |||||
| CD163 cell infiltration | Grade 0 | 1.53 (1.38–1.81) | 0.096 † | 1.60 (1.44–1.76) | 0.474 † | 0.79 (0.73–0.92) | 0.032 † | 0.80 (0.75–0.85) | 0.394 † |
| Grade 1 | 1.67 (1.48–1.90) | 1.64 (1.35–1.73) | 0.84 (0.71–0.94) | 0.82 (0.77–0.88) | |||||
| Grade 2 | 1.95 (1.58–2.18) | 1.72 (1.52–1.89) | 0.95 (0.76–1.06) | 0.81 (0.75–0.86) | |||||
| Grade 3 | 1.73 (1.58–2.20) | 1.72 (1.58–1.78) | 0.92 (0.84–1.05) | 0.84 (0.79–0.95) | |||||
| IL-6 expression | Grade 0 | 1.66 (1.48–1.94) | 0.878 † | 1.61 (1.51–1.73) | 0.813 † | 0.81 (0.75–0.94) | 0.743 † | 0.80 (0.75–0.88) | 0.794 † |
| Grade 1 | 1.75 (1.52–2.00) | 1.66 (1.44–1.85) | 0.90 (0.75–1.01) | 0.82 (0.79–0.91) | |||||
| Grade 2 | 1.63 (1.46–2.07) | 1.69 (1.43–1.80) | 0.87 (0.74–0.96) | 0.81 (0.77–0.85) | |||||
| Grade 3 | 1.73 (1.50–2.24) | 1.81 (1.43–2.03) | 0.89 (0.74–0.97) | 0.81 (0.77–0.83) | |||||
| Variables | p-Value * | Hazard Ratio (95% Confidence Interval) | |
|---|---|---|---|
| Age (<65 years vs. ≥65 years) | 0.951 | 0.99 (0.45–2.16) | |
| Sex (women vs. men) | 0.346 | 1.67 (0.57–4.84) | |
| WHO histopathological classification (papillary/tubular vs. mucinous/signet ring cells and other poorly cohesive types) | 0.287 | 1.52 (0.70–3.29) | |
| Lauren classification (intestinal vs. diffuse/indeterminate) | 0.426 | 1.38 (0.63–3.04) | |
| T stage (T1–T2 vs. T3–T4) | 0.003 | 22.02 (2.98–162.79) | |
| N stage (N0 vs. N1–3) | <0.001 | 12.92 (3.04–54.88) | |
| TNM stage (stage I–II vs. stage III) | <0.001 | 15.26 (4.54–51.25) | |
| Adjuvant chemotherapy (yes vs. no) | 0.004 | 4.85 (1.67–14.11) | |
| CD4 cell infiltration (grade 0 vs.) | Grade 1 | 0.526 | 1.41 (0.49–4.05) |
| Grade 2 | 0.381 | 1.63 (0.55–4.88) | |
| Grade 3 | 0.206 | 1.25 (0.29–2.14) | |
| CD8 cell infiltration (grade 0 vs.) | Grade 1 | 0.848 | 1.15 (0.29–4.58) |
| Grade 2 | 0.209 | 2.27 (0.63–8.15) | |
| Grade 3 | 0.087 | 1.90 (0.89–4.15) | |
| CD163 cell infiltration (grade 0 vs.) | Grade 1 | 0.842 | 0.90 (0.33–2.49) |
| Grade 2 | 0.146 | 1.24 (0.41–3.79) | |
| Grade 3 | 0.047 | 2.19 (1.05–5.51) | |
| IL-6 expression (grade 0 vs.) | Grade 1 | 0.493 | 1.41 (0.53–3.79) |
| Grade 2 | 0.491 | 1.45 (0.51–4.12) | |
| Grade 3 | 0.042 | 3.12 (1.07–10.81) | |
| Tumor SUV (<7.53 vs. ≥7.53) | <0.001 | 4.18 (1.91–9.13) | |
| BM SUV (<1.64 vs. ≥1.64) | 0.013 | 5.79 (1.99–16.88) | |
| Spleen SUV (<1.67 vs. ≥1.67) | 0.033 | 2.41 (1.07–5.42) | |
| BLR (<0.88 vs. ≥0.88) | 0.015 | 2.82 (1.22–6.50) | |
| SLR (<0.84 vs. ≥0.84) | 0.040 | 2.21 (1.02–4.79) | |
| Variables | p-Value * | Hazard Ratio (95% Confidence Interval) |
|---|---|---|
| BM SUV (<1.64 vs. ≥1.64) | 0.301 | 3.58 (0.66–13.78) |
| Spleen SUV (<1.67 vs. ≥1.67) | 0.159 | 1.75 (0.80–3.80) |
| BLR (<0.88 vs. ≥0.88) | 0.022 | 3.55 (1.20–10.54) |
| SLR (<0.84 vs. ≥0.84) | 0.049 | 2.27 (1.01–5.13) |
| TNM Stage | |||
|---|---|---|---|
| Stage I–II | Stage III | ||
| FDG uptake of BM and spleen | BLR <0.88 and SLR <0.84 | 0/17 (0.0%) | 6/10 (60.0%) |
| BLR ≥0.88 and SLR <0.84 Or BLR <0.88 and SLR ≥0.84 | 0/13 (0.0%) | 8/12 (66.7%) | |
| BLR ≥0.88 and SLR ≥0.84 | 3/7 (42.9%) | 9/11 (81.8%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, H.; Song, G.J.; Lee, M.-S.; Lee, J.-H.; Jang, S.-H.; Oh, M.-H.; Yun, J.H.; Lee, S.M.; Lee, J.W. Relationship of FDG Uptake of the Reticuloendothelial System with Tumor Immune Microenvironment and Prognosis in Patients with Gastric Cancer. Life 2023, 13, 771. https://doi.org/10.3390/life13030771
Ahn H, Song GJ, Lee M-S, Lee J-H, Jang S-H, Oh M-H, Yun JH, Lee SM, Lee JW. Relationship of FDG Uptake of the Reticuloendothelial System with Tumor Immune Microenvironment and Prognosis in Patients with Gastric Cancer. Life. 2023; 13(3):771. https://doi.org/10.3390/life13030771
Chicago/Turabian StyleAhn, Hyein, Geum Jong Song, Moon-Soo Lee, Ji-Hye Lee, Si-Hyong Jang, Mee-Hye Oh, Jong Hyuk Yun, Sang Mi Lee, and Jeong Won Lee. 2023. "Relationship of FDG Uptake of the Reticuloendothelial System with Tumor Immune Microenvironment and Prognosis in Patients with Gastric Cancer" Life 13, no. 3: 771. https://doi.org/10.3390/life13030771