
3D Exoscopes in Experimental Microanastomosis: A Comparison of Different Systems

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statements
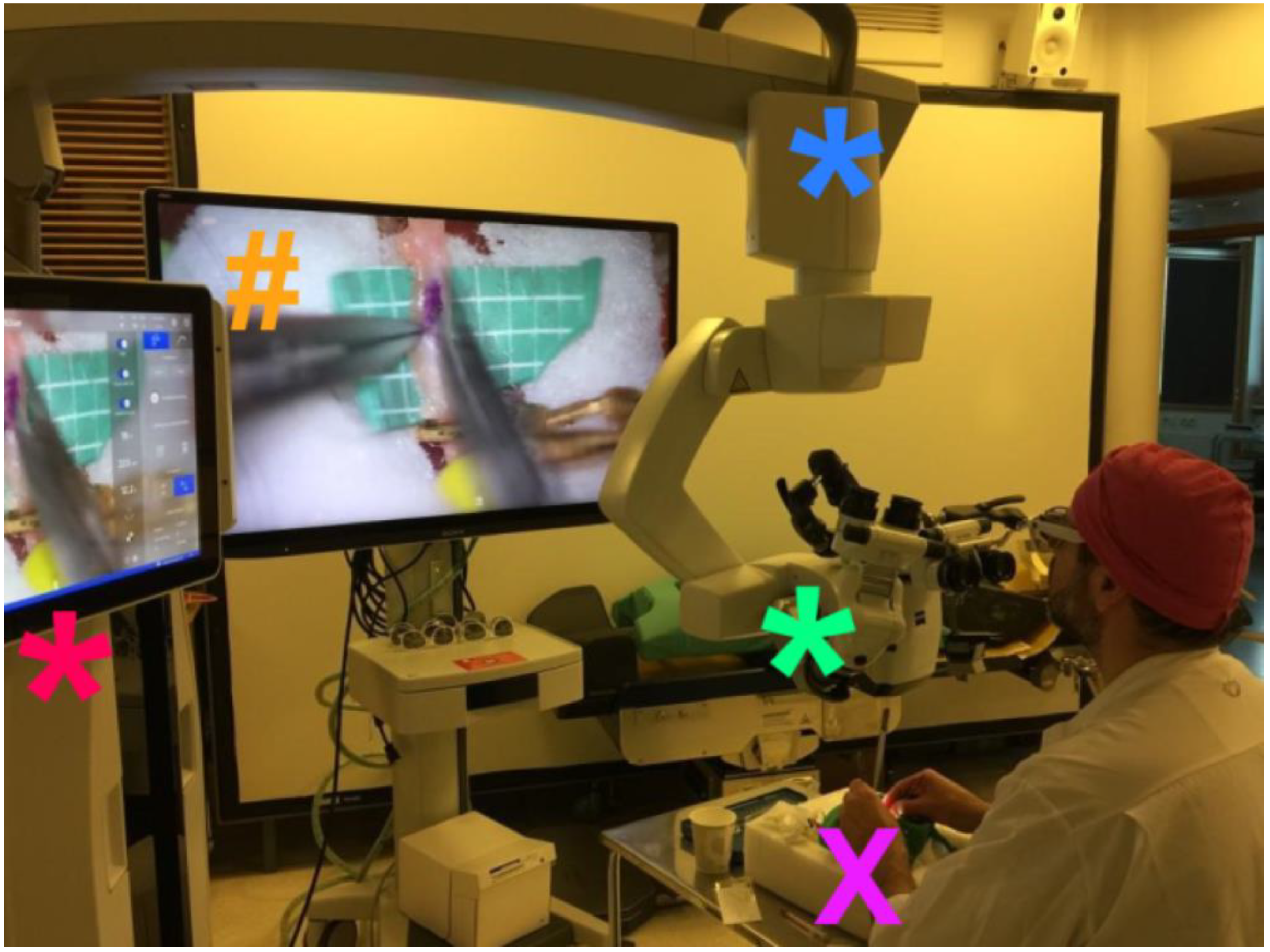
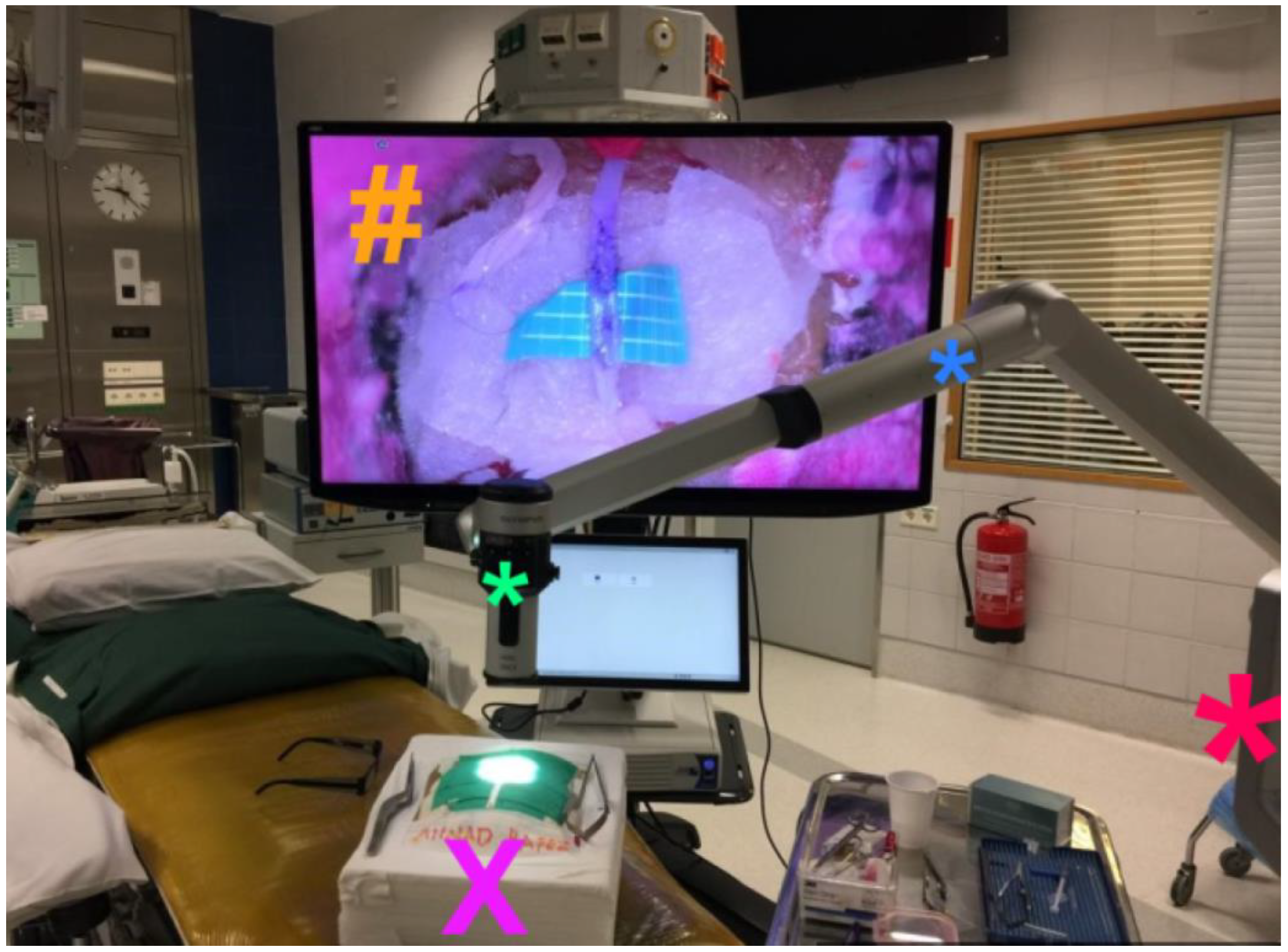
2.2. Exoscope Systems
2.3. Materials
2.4. Anastomosis Procedure
2.5. Outcome Parameters
2.6. Statistical Analyses
3. Results
3.1. Practical Setup and Subjective Evaluations
3.2. Bypass Procedures
3.3. Unnecessary Movements
4. Discussion
4.1. Technical Features
4.2. Practical Considerations
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hafez, A.; Elsharkawy, A.; Schwartz, C.; Muhammad, S.; Laakso, A.; Niemelä, M.; Lehecka, M. Comparison of Conventional Microscopic and Exoscopic Experimental Bypass Anastomosis: A Technical Analysis. World Neurosurg. 2020, 135, e293–e299. [Google Scholar] [CrossRef]
- Nossek, E.; Schneider, J.R.; Kwan, K.; Kulason, K.O.; Du, V.; Chakraborty, S.; Rahme, R.; Faltings, L.; Ellis, J.; Ortiz, R.; et al. Technical Aspects and Operative Nuances Using a High-Definition 3-Dimensional Exoscope for Cerebral Bypass Surgery. Oper. Neurosurg. 2019, 17, 157–163. [Google Scholar] [CrossRef]
- Ricciardi, L.; Chaichana, K.L.; Cardia, A.; Stifano, V.; Rossini, Z.; Olivi, A.; Sturiale, C.L. The Exoscope in Neurosurgery: An Innovative “Point of View”. A Systematic Review of the Technical, Surgical, and Educational Aspects. World Neurosurg. 2019, 124, 136–144. [Google Scholar] [CrossRef]
- Langer, D.J.; White, T.G.; Schulder, M.; Boockvar, J.A.; Labib, M.; Lawton, M.T. Advances in Intraoperative Optics: A Brief Review of Current Exoscope Platforms. Oper. Neurosurg. 2019, 19, 84–93. [Google Scholar] [CrossRef]
- Beez, T.; Munoz-Bendix, C.; Beseoglu, K.; Steiger, H.-J.; Ahmadi, S.A. First Clinical Applications of a High-Definition Three-Dimensional Exoscope in Pediatric Neurosurgery. Cureus 2018, 10, e2108. [Google Scholar] [CrossRef] [Green Version]
- Kwan, K.; Schneider, J.R.; Du, V.; Falting, L.; Boockvar, J.A.; Oren, J.; Levine, M.; Langer, D.J. Lessons Learned Using a High-Definition 3-Dimensional Exoscope for Spinal Surgery. Oper. Neurosurg. 2019, 16, 619–625. [Google Scholar] [CrossRef]
- Rossmann, T.; Veldeman, M.; Nurminen, V.; Huhtakangas, J.; Niemelä, M.; Lehecka, M. 3D Exoscopes are Noninferior to Operating Microscopes in Aneurysm Surgery: Comparative Single-Surgeon Series of 52 Consecutive Cases. World Neurosurg. 2022, 170, e200–e213. [Google Scholar] [CrossRef]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2022, 11, 223. [Google Scholar] [CrossRef]
- Hafez, A.; Haeren, R.H.; Dillmann, J.; Laakso, A.; Niemelä, M.; Lehecka, M. Comparison of Operating Microscope and Exoscope in a Highly Challenging Experimental Setting. World Neurosurg. 2020, 147, e468–e475. [Google Scholar] [CrossRef]
- Hafez, A.; Huhtakangas, J.; Muhammad, S.; Lawton, M.T.; Tanikawa, R.; Niemelä, M. The Identification of Factors That Influence the Quality of Bypass Anastomosis and an Evaluation of the Usefulness of an Experimental Practical Scale in This Regard. World Neurosurg. 2019, 121, e119–e128. [Google Scholar] [CrossRef] [Green Version]
- Roethe, A.L.; Landgraf, P.; Schröder, T.; Misch, M.; Vajkoczy, P.; Picht, T. Monitor-based exoscopic 3D4k neurosurgical interventions: A two-phase prospective-randomized clinical evaluation of a novel hybrid device. Acta Neurochir. 2020, 162, 2949–2961. [Google Scholar] [CrossRef]
- Sack, J.; Steinberg, J.A.; Rennert, R.C.; Hatefi, D.; Pannell, J.S.; Levy, M.; Khalessi, A.A. Initial Experience Using a High-Definition 3-Dimensional Exoscope System for Microneurosurgery. Oper. Neurosurg. 2018, 14, 395–401. [Google Scholar] [CrossRef]
- Shirzadi, A.; Mukherjee, D.M.; Drazin, D.G.; Paff, M.B.; Perri, B.D.; Mamelak, A.N.; Siddique, K. Use of the Video Telescope Operating Monitor (VITOM) as an Alternative to the Operating Microscope in Spine Surgery. Spine 2012, 37, E1517–E1523. [Google Scholar] [CrossRef]
- Mamelak, A.N.; Nobuto, T.; Berci, G. Initial Clinical Experience with a High-Definition Exoscope System for Microneurosurgery. Neurosurgery 2010, 67, 476–483. [Google Scholar] [CrossRef]
- Pafitanis, G.; Hadjiandreou, M.; Alamri, A.; Uff, C.; Walsh, D.; Myers, S. The Exoscope versus operating microscope in microvascular surgery: A simulation non-inferiority trial. Arch. Plast. Surg. 2020, 47, 242–249. [Google Scholar] [CrossRef]
- Murai, Y.; Sato, S.; Yui, K.; Morimoto, D.; Ozeki, T.; Yamaguchi, M.; Tateyama, K.; Nozaki, T.; Tahara, S.; Yamaguchi, F.; et al. Preliminary Clinical Microneurosurgical Experience With the 4K3-Dimensional Microvideoscope (ORBEYE) System for Microneurological Surgery: Observation Study. Oper. Neurosurg. 2018, 16, 707–716. [Google Scholar] [CrossRef]
- Belykh, E.G.; Zhao, X.; Cavallo, C.; Bohl, M.A.; Yagmurlu, K.; Aklinski, J.L.; Byvaltsev, V.A.; Sanai, N.; Spetzler, R.F.; Lawton, M.T.; et al. Laboratory Evaluation of a Robotic Operative Microscope-Visualization Platform for Neurosurgery. Cureus 2018, 10, e3072. [Google Scholar] [CrossRef] [Green Version]
- Haeren, R.; Hafez, A.; Lehecka, M. Visualization and Maneuverability Features of a Robotic Arm Three-Dimensional Exoscope and Operating Microscope for Clipping an Unruptured Intracranial Aneurysm: Video Comparison and Technical Evaluation. Oper. Neurosurg. 2022, 22, 28–34. [Google Scholar] [CrossRef]
- Raheja, A.; Mishra, S.; Garg, K.; Katiyar, V.; Sharma, R.; Tandon, V.; Goda, R.; Suri, A.; Kale, S.S. Impact of different visualization devices on accuracy, efficiency, and dexterity in neurosurgery: A laboratory investigation. Neurosurg. Focus 2021, 50, E18. [Google Scholar] [CrossRef]
- Smithee, W.; Chakravarthi, S.; Epping, A.; Kassam, M.; Monroy-Sosa, A.; Thota, A.; Kura, B.; Rovin, R.A.; Fukui, M.B.; Kassam, A.B. Initial Experience with Exoscopic-Based Intraoperative Indocyanine Green Fluorescence Video Angiography in Cerebrovascular Surgery: A Preliminary Case Series Showing Feasibility, Safety, and Next-Generation Handheld Form-Factor. World Neurosurg. 2020, 138, e82–e94. [Google Scholar] [CrossRef]
- Vogelbaum, M.A.; Kroll, D.; Etame, A.; Tran, N.; Liu, J.; Ford, A.; Sparr, E.; Kim, Y.; Forsyth, P.; Sahebjam, S.; et al. A Prospective Validation Study of the First 3D Digital Exoscope for Visualization of 5-ALA–Induced Fluorescence in High-Grade Gliomas. World Neurosurg. 2021, 149, e498–e503. [Google Scholar] [CrossRef]
- Piatkowski, A.A.; Keuter, X.H.; Schols, R.M.; van der Hulst, R.R. Potential of performing a microvascular free flap re-construction using solely a 3D exoscope instead of a conventional microscope. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 1664–1678. [Google Scholar] [CrossRef]
- Lefevre, E.; Ganau, M.; Zaed, I.; Machado-Filho, G.D.M.; Scibilia, A.; Mallereau, C.-H.; Bresson, D.; Todeschi, J.; Cebula, H.; Proust, F.; et al. Learning curve and influencing factors of performing microsurgical anastomosis: A laboratory prospective study. Neurosurg. Rev. 2022, 45, 3271–3280. [Google Scholar] [CrossRef]
- Veldeman, M.; Rossmann, T.; Huhtakangas, J.; Nurminen, V.; Eisenring, C.; Sinkkonen, S.T.; Niemela, M.; Lehecka, M. 3-Dimensional Exoscopic Versus Microscopic Resection of Vestibular Schwannomas: A Comparative Series. Oper. Neurosurg. 2023. [Google Scholar] [CrossRef]
- Motov, S.; Bonk, M.N.; Krauss, P.; Wolfert, C.; Steininger, K.; Picht, T.; Onken, J.; Shiban, E. Implementation of a three-dimensional (3D) robotic digital microscope (AEOS) in spinal procedures. Sci. Rep. 2022, 12, 22553. [Google Scholar] [CrossRef]
- Calloni, T.; Roumy, L.G.; Cinalli, M.A.; Rocca, A.; Held, A.; Trezza, A.; Carrabba, G.G.; Giussani, C.G. Exoscope as a Teaching Tool: A Narrative Review of the Literature. Front. Surg. 2022, 9, 878293. [Google Scholar] [CrossRef]
- Fiani, B.; Jarrah, R.; Griepp, D.W.; Adukuzhiyil, J. The Role of 3D Exoscope Systems in Neurosurgery: An Optical Innovation. Cureus 2021, 13, e15878. [Google Scholar] [CrossRef]
- Muhammad, S.; Lehecka, M.; Niemelä, M. Preliminary experience with a digital robotic exoscope in cranial and spinal surgery: A review of the Synaptive Modus V system. Acta Neurochir. 2019, 161, 2175–2180. [Google Scholar] [CrossRef] [Green Version]
- Bakhsheshian, J.; Strickland, B.A.; Jackson, C.; Chaichana, K.L.; Young, R.; Pradilla, G.; Chen, J.W.; Bailes, J.; Zada, G. Multicenter Investigation of Channel-Based Subcortical Trans-Sulcal Exoscopic Resection of Metastatic Brain Tumors: A Retrospective Case Series. Oper. Neurosurg. 2018, 16, 159–166. [Google Scholar] [CrossRef]
- Peng, Y.-J.; Zhao, T.-B.; Dai, J.; Wang, Q.-L.; Zhang, Q.-Z.; Cao, J.-Y.; Liu, X.-F. Clinical comparison of three-dimensional exoscope vs. operative microscope in transforaminal lumbar interbody fusion: A retrospective case-control study. Front. Surg. 2022, 9, 926329. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anastomosis Quality Factor | Value | Points | |
|---|---|---|---|
| T | Closure time for 20 stitches in 1 mm vessel | <20 min | 1 |
| >20 min | 0 | ||
| S | Good distribution of stitches | Yes | 1 |
| No | 0 | ||
| I | Thread hidden inside lumen (intima-intima contact) | Yes | 1 |
| No | 0 | ||
| O | Width of the orifice (equal or wider than vessel diameter) | Yes | 1 |
| No | 0 |
| Exoscope System | TSIO Score | Number of Favorable TSIO Scores * | ||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | ||
| VITOM | 2 | 1 | 4 | 3 | - | 7/10 |
| KINEVO | - | 2 | 8 | - | - | 8/10 |
| AEOS | - | 1 | 2 | 7 | - | 9/10 |
| ORBEYE | 1 | 1 | 2 | 6 | - | 6/10 |
| Exoscope System | Mean Duration of Bypass Procedure (± SD, Range) in Minutes | Mean Number of Unnecessary Movements (± SD, Range) |
|---|---|---|
| VITOM | 27.7 (± 1.8, 25–31) | 27.0 (± 4.6, 20–35) |
| KINEVO | 29.5 (± 1.8, 26–32) | 32.5 (± 9.5, 24–58) |
| AEOS | 26.2 (± 2.7, 21–29) | 25.6 (± 5.4, 20–37) |
| ORBEYE | 34.0 (± 3,1, 31–40) | 49.2 (± 11.1, 32–69) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hafez, A.; Haeren, R.; Huhtakangas, J.; Nurminen, V.; Niemelä, M.; Lehecka, M. 3D Exoscopes in Experimental Microanastomosis: A Comparison of Different Systems. Life 2023, 13, 584. https://doi.org/10.3390/life13020584
Hafez A, Haeren R, Huhtakangas J, Nurminen V, Niemelä M, Lehecka M. 3D Exoscopes in Experimental Microanastomosis: A Comparison of Different Systems. Life. 2023; 13(2):584. https://doi.org/10.3390/life13020584
Chicago/Turabian StyleHafez, Ahmad, Roel Haeren, Justiina Huhtakangas, Ville Nurminen, Mika Niemelä, and Martin Lehecka. 2023. "3D Exoscopes in Experimental Microanastomosis: A Comparison of Different Systems" Life 13, no. 2: 584. https://doi.org/10.3390/life13020584