
Left Ventricular Unloading in Patients on Venoarterial Extracorporeal Membrane Oxygenation Therapy in Cardiogenic Shock: Prophylactic Versus Bail-Out Strategy
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
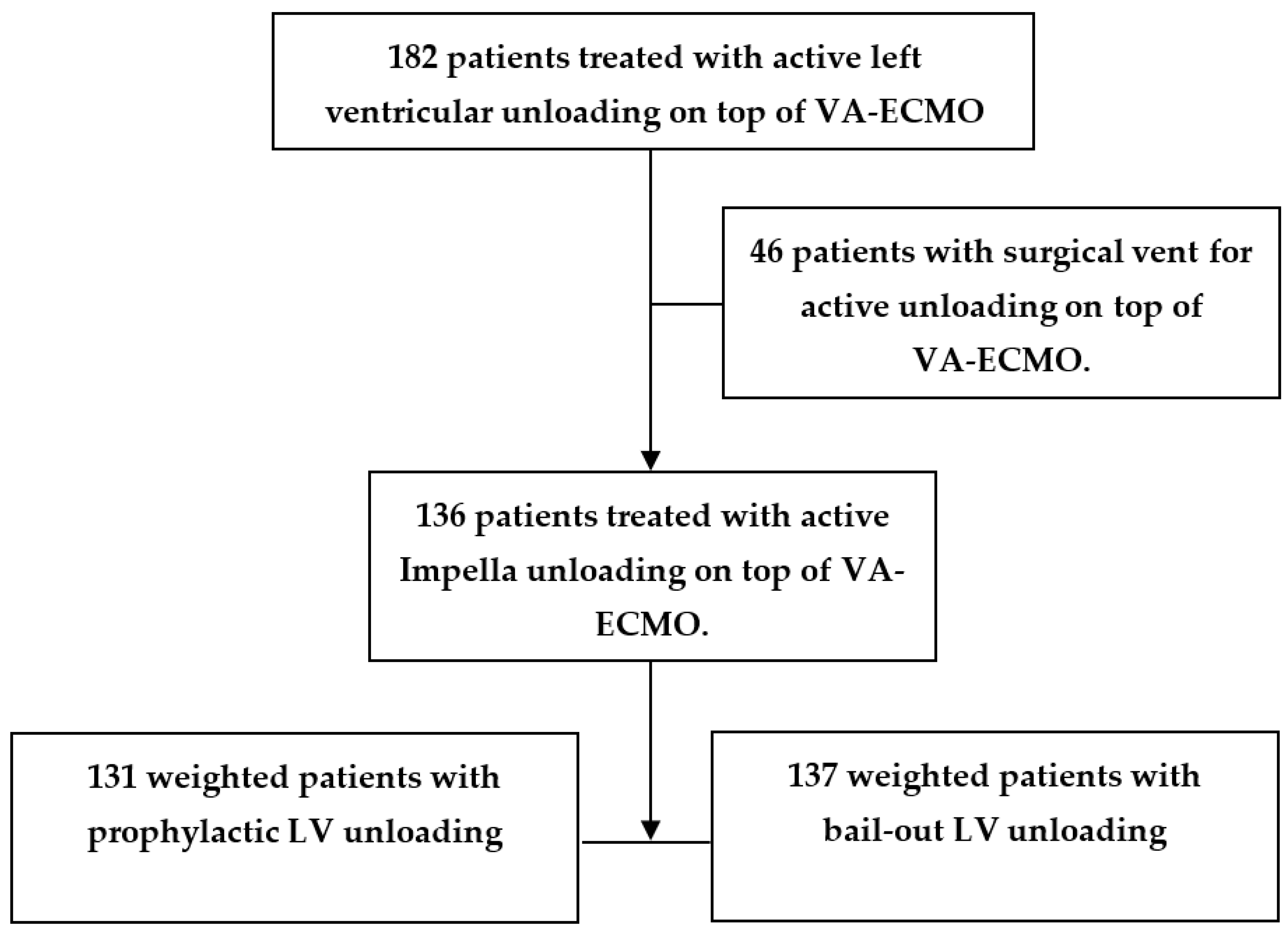
2.1. Study Design and Patients
2.2. Data Acquisition
2.3. Endpoints
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Endpoints
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Diepen, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary Management of Cardiogenic Shock: A Scientific Statement from the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Feldman, D.; Pamboukian, S.V.; Teuteberg, J.J.; Birks, E.; Lietz, K.; Moore, S.A.; Morgan, J.A.; Arabia, F.; Bauman, M.E.; Buchholz, H.W.; et al. The 2013 International Society for Heart and Lung Transplantation Guidelines for mechanical circulatory support: Executive summary. J. Heart Lung Transplant. 2013, 32, 157–187. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Samsky, M.D.; Morrow, D.A.; Proudfoot, A.G.; Hochman, J.S.; Thiele, H.; Rao, S.V. Cardiogenic Shock after Acute Myocardial Infarction: A Review. JAMA 2021, 326, 1840–1850. [Google Scholar] [CrossRef]
- Burkhoff, D.; Sayer, G.; Doshi, D.; Uriel, N. Hemodynamics of Mechanical Circulatory Support. J. Am. Coll. Cardiol. 2015, 66, 2663–2674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bratti, J.R.; Cavayas, Y.; Noly, P.; Serri, K.; Lamarche, Y. Modalities of Left Ventricle Decompression during VA-ECMO Therapy. Membranes 2021, 11, 209. [Google Scholar] [CrossRef] [PubMed]
- Radakovic, D.; Zittermann, A.; Knezevic, A.; Razumov, A.; Opacic, D.; Wienrautner, N.; Flottmann, C.; Rojas, S.V.; Fox, H.; Schramm, R.; et al. Left ventricular unloading during extracorporeal life support for myocardial infarction with cardiogenic shock: Surgical venting versus Impella device. Interact. Cardiovasc. Thorac. Surg. 2021, 34, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Radakovic, D.; Penov, K.; Hamouda, K.; Madrahimov, N.; Radakovic, D.; Bening, C.; Leyh, R.G.; Aleksic, I. Benefits of Intra-Aortic Balloon Pump Support in Patients with Postcardiotomy Shock Requiring Venoarterial Extracorporeal Membrane Oxygenation. Life 2022, 12, 1195. [Google Scholar] [CrossRef]
- Pappalardo, F.; Schulte, C.; Pieri, M.; Schrage, B.; Contri, R.; Soeffker, G.; Greco, T.; Lembo, R.; Müllerleile, K.; Colombo, A.; et al. Concomitant implantation of Impella® on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur. J. Heart Fail. 2016, 19, 404–412. [Google Scholar] [CrossRef]
- Grandin, E.W.; Nunez, J.I.; Willar, B.; Kennedy, K.; Rycus, P.; Tonna, J.E.; Kapur, N.K.; Shaefi, S.; Garan, A.R. Mechanical Left Ventricular Unloading in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation. J. Am. Coll. Cardiol. 2022, 79, 1239–1250. [Google Scholar] [CrossRef]
- Patel, S.M.; Lipinski, J.; Al-Kindi, S.G.; Patel, T.; Saric, P.; Li, J.; Nadeem, F.; Ladas, T.; Alaiti, A.; Phillips, A.; et al. Simultaneous Venoarterial Extracorporeal Membrane Oxygenation and Percutaneous Left Ventricular Decompression Therapy with Impella Is Associated with Improved Outcomes in Refractory Cardiogenic Shock. ASAIO J. 2019, 65, 21–28. [Google Scholar] [CrossRef]
- Schrage, B.; Becher, P.M.; Bernhardt, A.; Bezerra, H.; Blankenberg, S.; Brunner, S.; Colson, P.; Deseda, G.C.; Dabboura, S.; Eckner, D.; et al. Left Ventricular Unloading Is Associated with Lower Mortality in Patients with Cardiogenic Shock Treated with Venoarterial Extracorporeal Membrane Oxygenation: Results from an International, Multicenter Cohort Study. Circulation 2020, 142, 2095–2106. [Google Scholar] [CrossRef] [PubMed]
- Na, S.J.; Yang, J.H.; Yang, J.-H.; Sung, K.; Choi, J.-O.; Hahn, J.-Y.; Jeon, E.-S.; Cho, Y.H. Left heart decompression at venoarterial extracorporeal membrane oxygenation initiation in cardiogenic shock: Prophylactic versus therapeutic strategy. J. Thorac. Dis. 2019, 11, 3746–3756. [Google Scholar] [CrossRef] [PubMed]
- Russo, J.J.; Di Santo, P.; Kirtane, A.J.; Hibbert, B. Reply: Left Ventricle Unloading Strategy: Which One Is More Effective in Ven-oarterial Extracorporeal Membrane Oxygenation Patients? J. Am. Coll. Cardiol. 2019, 73, 3036. [Google Scholar] [CrossRef]
- Reddy, Y.N.V.; El-Sabbagh, A.; Nishimura, R.A. Comparing Pulmonary Arterial Wedge Pressure and Left Ventricular End Diastolic Pressure for Assessment of Left-Sided Filling Pressures. JAMA Cardiol. 2018, 3, 453–454. [Google Scholar] [CrossRef]
- Cevasco, M.; Takayama, H.; Ando, M.; Garan, A.R.; Naka, Y.; Takeda, K. Left ventricular distension and venting strategies for patients on venoarterial extracorporeal membrane oxygenation. J. Thorac. Dis. 2019, 11, 1676–1683. [Google Scholar] [CrossRef] [PubMed]
- Char, S.; Fried, J.; Melehy, A.; Mehta, S.; Ning, Y.; Kurlansky, P.; Takeda, K. Clinical efficacy of direct or indirect left ventricular unloading during venoarterial extracorporeal membrane oxygenation for primary cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2021, 165, 699–707.e5. [Google Scholar] [CrossRef]
- Schrage, B.; Sundermeyer, J.; Blankenberg, S.; Eitel, I.; Kirchhof, P.; Mangner, N.; Moebius-Winkler, S.; Orban, M.; Thiele, H.; Morrow, D.; et al. Timing of active left ventricular unloading in patients with cardiogenic shock on veno-arterial extracorporeal membrane oxygenation therapy. Eur. Heart J. 2022, 43 (Suppl. 2), ehac544.1504. [Google Scholar] [CrossRef]
- Rajagopal, K. Left Ventricular Distension in Veno-arterial Extracorporeal Membrane Oxygenation: From Mechanics to Therapies. ASAIO J. 2019, 65, 1–10. [Google Scholar] [CrossRef]
- Donker, D.W.; Brodie, D.; Henriques, J.P.; Broomé, M. Left ventricular unloading during veno-arterial ECMO: A review of percutaneous and surgical unloading interventions. Perfusion 2018, 34, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.; Khalpey, Z.; Smith, R.; Burkhoff, D.; Kociol, R.D.; Mehmood, M.; Alhussein, M.; Moayedi, Y.; Posada, J.D.; Ross, H.; et al. Venoarterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock and Cardiac Arrest. Circ. Heart Fail. 2018, 11, e004905. [Google Scholar] [CrossRef]
- Rupprecht, L.; Flörchinger, B.; Schopka, S.; Schmid, C.; Philipp, A.; Lunz, D.; Müller, T.; Camboni, D. Cardiac Decompression on Extracorporeal Life Support: A Review and Discussion of the Literature. ASAIO J. 2013, 59, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Truby, L.K.; Takeda, K.; Mauro, C.; Yuzefpolskaya, M.; Garan, A.R.; Kirtane, A.J.; Topkara, V.K.; Abrams, D.; Brodie, D.; Colombo, P.C.; et al. Incidence and Implications of Left Ventricular Distention during Venoarterial Extracorporeal Membrane Oxygenation Support. ASAIO J. 2017, 63, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Broomé, M.; Donker, D.W. Individualized real-time clinical decision support to monitor cardiac loading during venoarterial ECMO. J. Transl. Med. 2016, 14, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makdisi, G.; Hashmi, Z.A.; Wozniak, T.C.; Wang, I.-W. Left ventricular thrombus associated with arteriovenous extra corporeal membrane oxygenation. J. Thorac. Dis. 2015, 7, E552–E554. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Deppe, A.-C.; Sabashnikov, A.; Slottosch, I.; Kuhn, E.; Eghbalzadeh, K.; Scherner, M.; Choi, Y.-H.; Madershahian, N.; Wahlers, T. Left ventricular thrombus formation in patients undergoing femoral veno-arterial extracorporeal membrane oxygenation. Perfusion 2017, 33, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Russo, J.J.; Aleksova, N.; Pitcher, I.; Couture, E.; Parlow, S.; Faraz, M.; Visintini, S.; Simard, T.; Di Santo, P.; Mathew, R.; et al. Left Ventricular Unloading during Extracorporeal Membrane Oxygenation in Patients with Cardiogenic Shock. J. Am. Coll. Cardiol. 2019, 73, 654–662. [Google Scholar] [CrossRef]
- Schrage, B.; Sundermeyer, J.; Blankenberg, S.; Colson, P.; Eckner, D.; Eden, M.; Eitel, I.; Frank, D.; Frey, N.; Graf, T.; et al. Timing of Active Left Ventricular Unloading in Patients on Venoarterial Extracorporeal Membrane Oxygenation Therapy. JACC: Heart Fail. 2023; in press. [Google Scholar] [CrossRef]
- Shibasaki, I.; Masawa, T.; Abe, S.; Ogawa, H.; Takei, Y.; Tezuka, M.; Seki, M.; Kato, T.; Watanabe, R.; Koshiji, N.; et al. Benefit of veno-arterial extracorporeal membrane oxygenation combined with Impella (ECpella) therapy in acute coronary syndrome with cardiogenic shock. J. Cardiol. 2022, 80, 116–124. [Google Scholar] [CrossRef]
- Cappannoli, L.; Galli, M.; Zito, A.; Restivo, A.; Princi, G.; Laborante, R.; Vergallo, R.; Romagnoli, E.; Leone, A.M.; Aurigemma, C.; et al. Venoarterial extracorporeal membrane oxygenation (VA-ECMO) with vs. without left ventricular unloading by Impella: A systematic review and meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2022, qcac076. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Prophylactic Group n = 46 | Unweighted Patients Bail-Out Group n = 90 | SMD % | Prophylactic Group n = 131 | Weighted Patients Bail-Out Group n = 137 | SMD % |
|---|---|---|---|---|---|---|
| Age Group 1 | ||||||
| <50 Years | 8 (17) | 25 (28) | 34.0 | 28 (21.4) | 34 (24.8) | 10.9 |
| 50–60 Years | 16 (35) | 34 (38) | 8.6 | 51 (38.9) | 51 (37.2) | −4.9 |
| >60 Years | 22 (48) | 31 (34) | −41.2 | 52 (38.7) | 52 (38.0) | −2.0 |
| Sex, Males 2 | 34 (74) | 65 (72) | −6.3 | 96 (73.3) | 99 (72.8) | −1.6 |
| Body Mass Index (kg/m2) 1 | ||||||
| <20 | 4 (9) | 7 (8) | −4.9 | 10 (7.6) | 11 (8.0) | 2.0 |
| 20–30 | 30 (65) | 62 (69) | 12.1 | 89 (67.9) | 94 (68.6) | 2.1 |
| >30 | 12 (26) | 21 (23) | −9.9 | 32 (24.4) | 32 (23.4) | −3.3 |
| Diabetes Mellitus 1 | 12 (26) | 20 (22) | −13.4 | 35 (26.7) | 34 (24.8) | −6.1 |
| Pulmonary Hypertension 1 | 1 (2) | 5 (6) | 22.1 | 4 (3.1) | 6 (4.4) | 8.1 |
| Resuscitation 1 | 23 (50) | 54 (60) | 28.6 | 70 (56.9) | 78 (53.4) | −9.8 |
| Chronic Kidney Disease 1 | 7 (15) | 12 (13) | −8.1 | 17 (13.0) | 18 (13.1) | 0.4 |
| eGFR Group (mL/min/1.73m2) 1 | ||||||
| <30 | 18 (39) | 27 (30) | −27.3 | 45 (34.4) | 45 (32.8) | −4.7 |
| 30–60 | 21 (46) | 40 (44) | −5.6 | 60 (45.8) | 60 (44.5) | −3.7 |
| >60 | 7 (15) | 23 (26) | 34.8 | 26 (19.8) | 31 (22.6) | 9.3 |
| Total Bilirubin > 1.2 mg/dL 1 | 22 (48) | 50 (56) | 22.6 | 70 (53.4) | 72 (52.6) | −2.2 |
| Maximum Vasoactive Inotropic Score 2 | 40.9 (22.4) | 42.5 (22.7) | 7.1 | 41.9 (21.9) | 42.5 (22.4) | 2.7 |
| SOFA Score 2 | 10.8 (3.7) | 10.6 (5.4) | −4.3 | 10.8 (3.7) | 10.5 (4.8) | −7.0 |
| APACHE II Score 2 | 26.6 (7.8) | 26.3 (10.4) | −3.3 | 26.7 (8.0) | 26.8 (10.0) | −1.1 |
| SAVE Score 2 | −10.8 (4.6) | −10.4 (4.5) | −8.8 | −10.7 (4.6) | −10.3 (4.6) | −8.7 |
| Serum Lactate (mmol/L) 2 | 10.9 (5.2) | 10.1 (5.2) | −15.4 | 10.9 (5.3) | 10.4 (5.4) | −9.3 |
| Prophylactic Group n = 131 | Bail-Out Group n = 137 | Relative Risk (95%CI) | p-Value | |
|---|---|---|---|---|
| Primary Endpoint | ||||
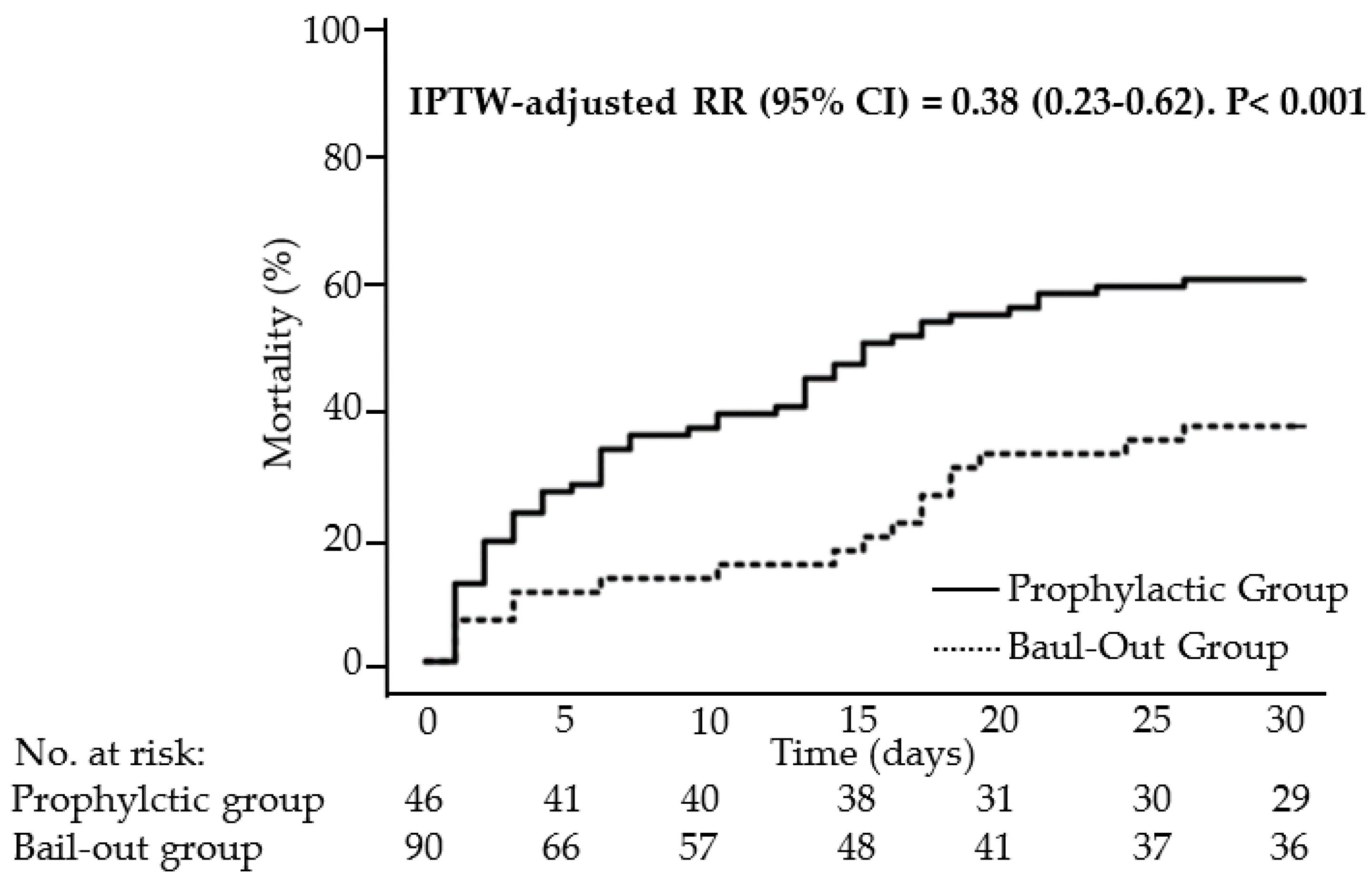
| Thirty-Day Mortality (n,%) | 47 (35.9) | 82 (59.9) | 0.38 (0.23–0.62) | <0.001 |
| Secondary Endpoints | ||||
| Myocardial Recovery (n,%) | 48 (36.6) | 25 (18.2) | 2.9 (1.48–4.54) | 0.001 |
| Heart Transplantation or VAD (n,%) | 30 (22.9) | 33 (24.1) | 0.94 (0.53–1.65) | 0.89 |
| Safety Endpoints | ||||
| Cannulation Site Bleeding (n,%) | 10 (7.6) | 19 (13.9) | 0.51 (0.23–1.15) | 0.12 |
| Stroke (n,%) | 14 (10.7) | 33 (24.1) | 0.39 (0.19–0.74) | 0.006 |
| Hemolysis (n,%) | 31 (23.7) | 52 (38.0) | 0.51 (0.30–0.86) | 0.012 |
| Access-Site-Related Ischemia (n,%) | 14 (10.8) | 20 (14.7) | 0.70 (0.34–1.45) | 0.36 |
| Abdominal Complications (n,%) | 45 (34.4) | 48 (35.0) | 0.97 (0.59–1.61) | >0.99 |
| Sepsis (n,%) | 49 (37.7) | 59 (43.1) | 0.80 (0.49–1.31) | 0.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radakovic, D.; Zittermann, A.; Rojas, S.V.; Opacic, D.; Razumov, A.; Prashovikj, E.; Fox, H.; Schramm, R.; Morshuis, M.; Rudolph, V.; et al. Left Ventricular Unloading in Patients on Venoarterial Extracorporeal Membrane Oxygenation Therapy in Cardiogenic Shock: Prophylactic Versus Bail-Out Strategy. Life 2023, 13, 582. https://doi.org/10.3390/life13020582
Radakovic D, Zittermann A, Rojas SV, Opacic D, Razumov A, Prashovikj E, Fox H, Schramm R, Morshuis M, Rudolph V, et al. Left Ventricular Unloading in Patients on Venoarterial Extracorporeal Membrane Oxygenation Therapy in Cardiogenic Shock: Prophylactic Versus Bail-Out Strategy. Life. 2023; 13(2):582. https://doi.org/10.3390/life13020582
Chicago/Turabian StyleRadakovic, Darko, Armin Zittermann, Sebastian V. Rojas, Dragan Opacic, Artyom Razumov, Emir Prashovikj, Henrik Fox, René Schramm, Michiel Morshuis, Volker Rudolph, and et al. 2023. "Left Ventricular Unloading in Patients on Venoarterial Extracorporeal Membrane Oxygenation Therapy in Cardiogenic Shock: Prophylactic Versus Bail-Out Strategy" Life 13, no. 2: 582. https://doi.org/10.3390/life13020582