
A Preclinical Systematic Review and Meta-Analysis of Behavior Testing in Mice Models of Ischemic Stroke

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
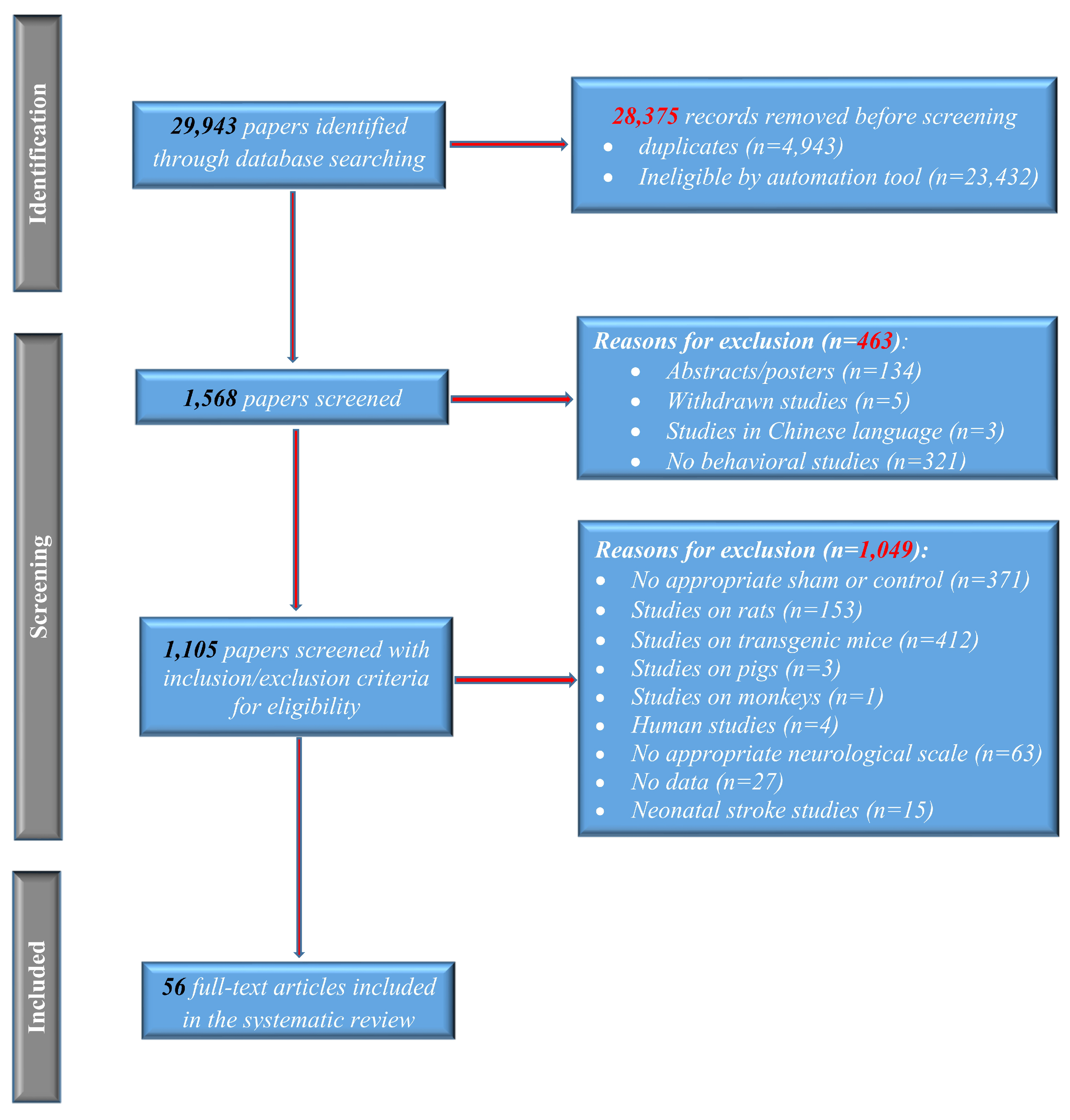
2.1. Retrieving the Literature
2.2. Selection of Studies and Data Extraction
2.3. Quality Assessment
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
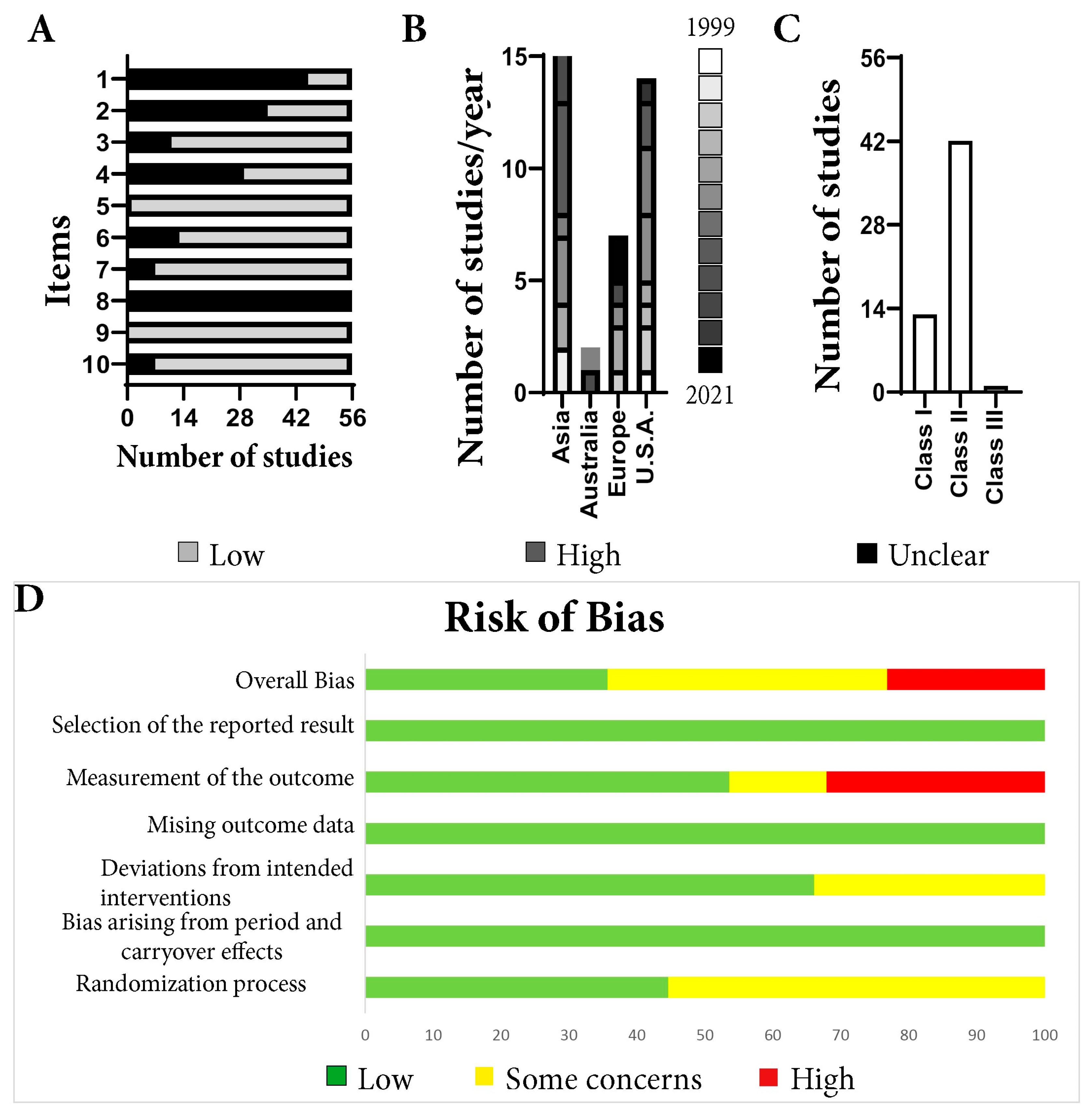
3.1. Risk of Bias and Quality Assessment
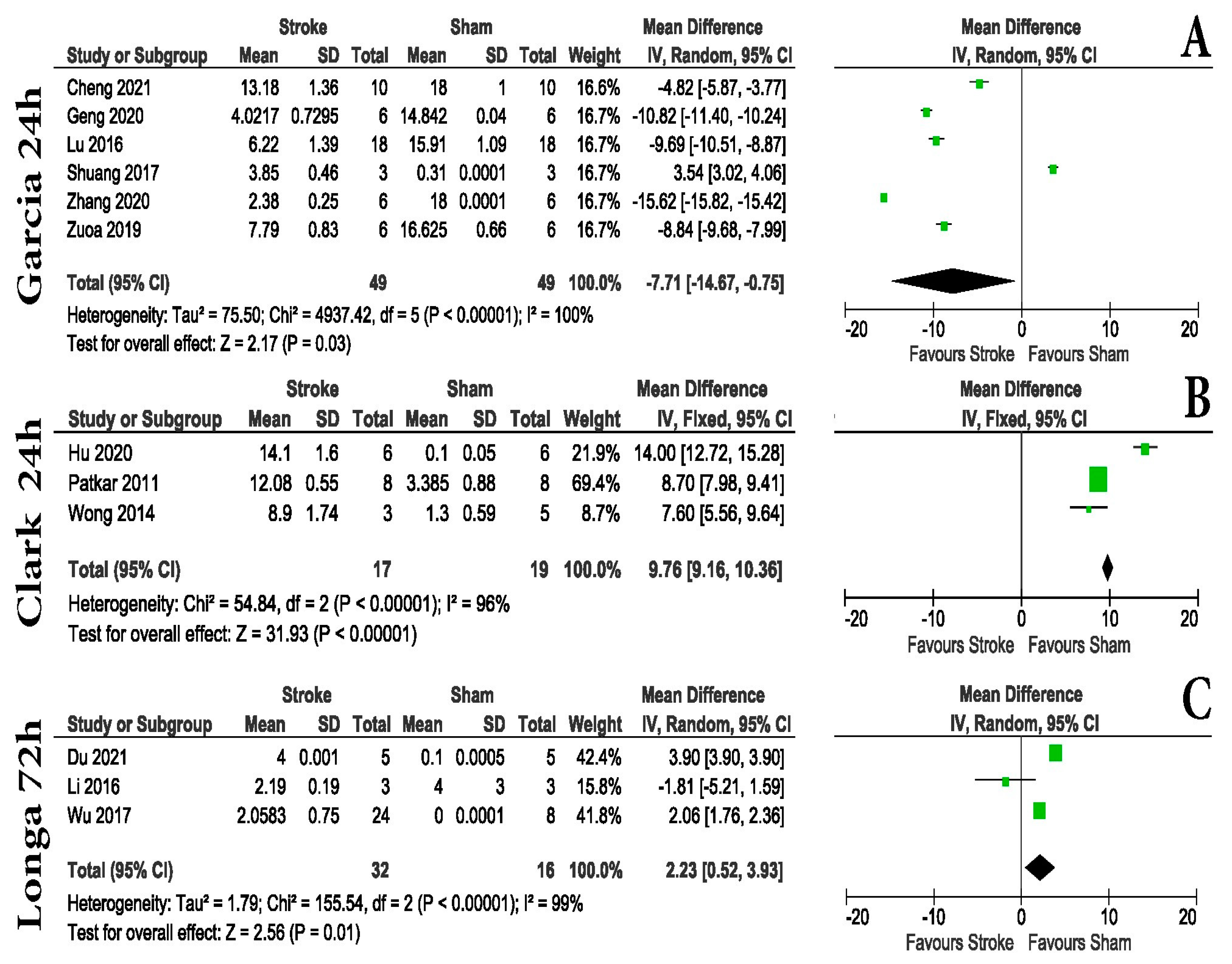
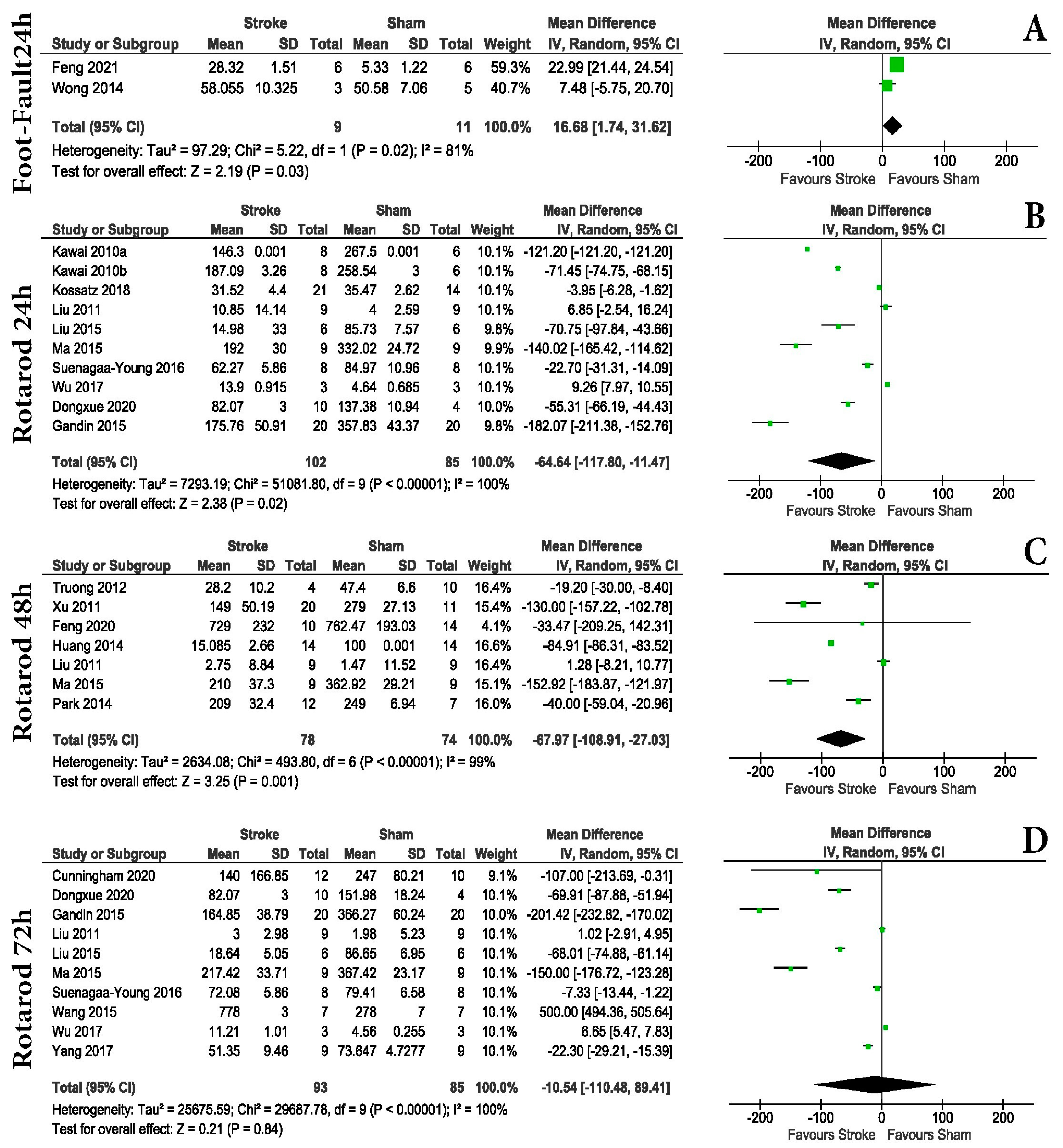
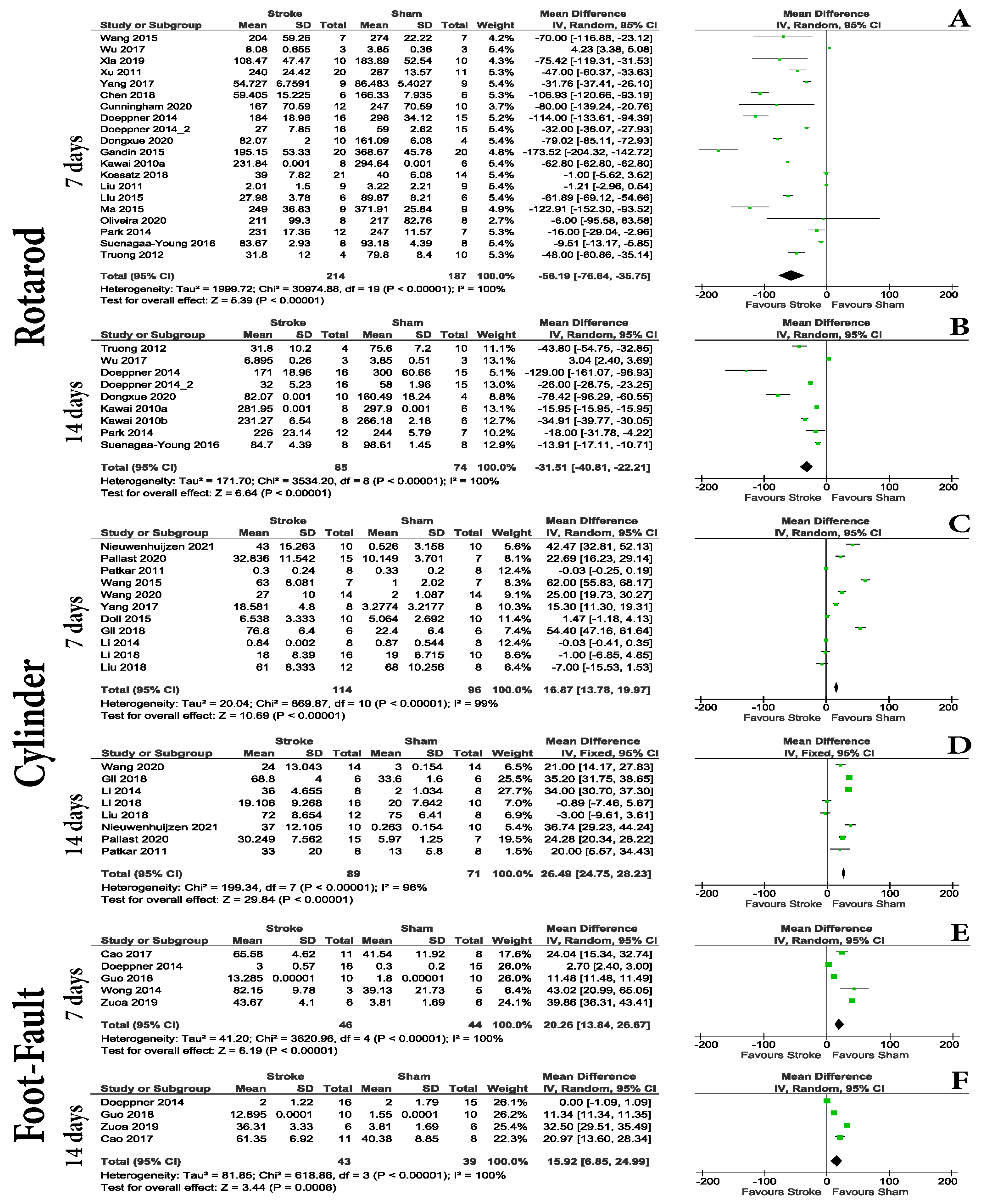
3.2. Animal Examination and Some Motor Tasks Are Effective in Establishing Differences in the Hyper-Acute Post-Stroke Interval
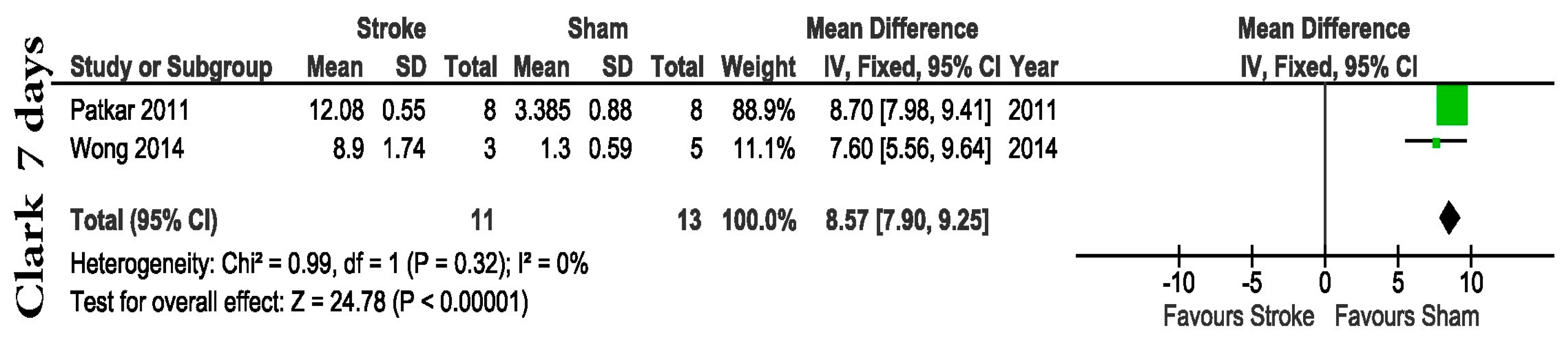
3.3. Motor Tests and Some Animal Examination Scoring Are Effective in Establishing Differences in the Acute and Early Sub-Acute Post-Stroke Intervals
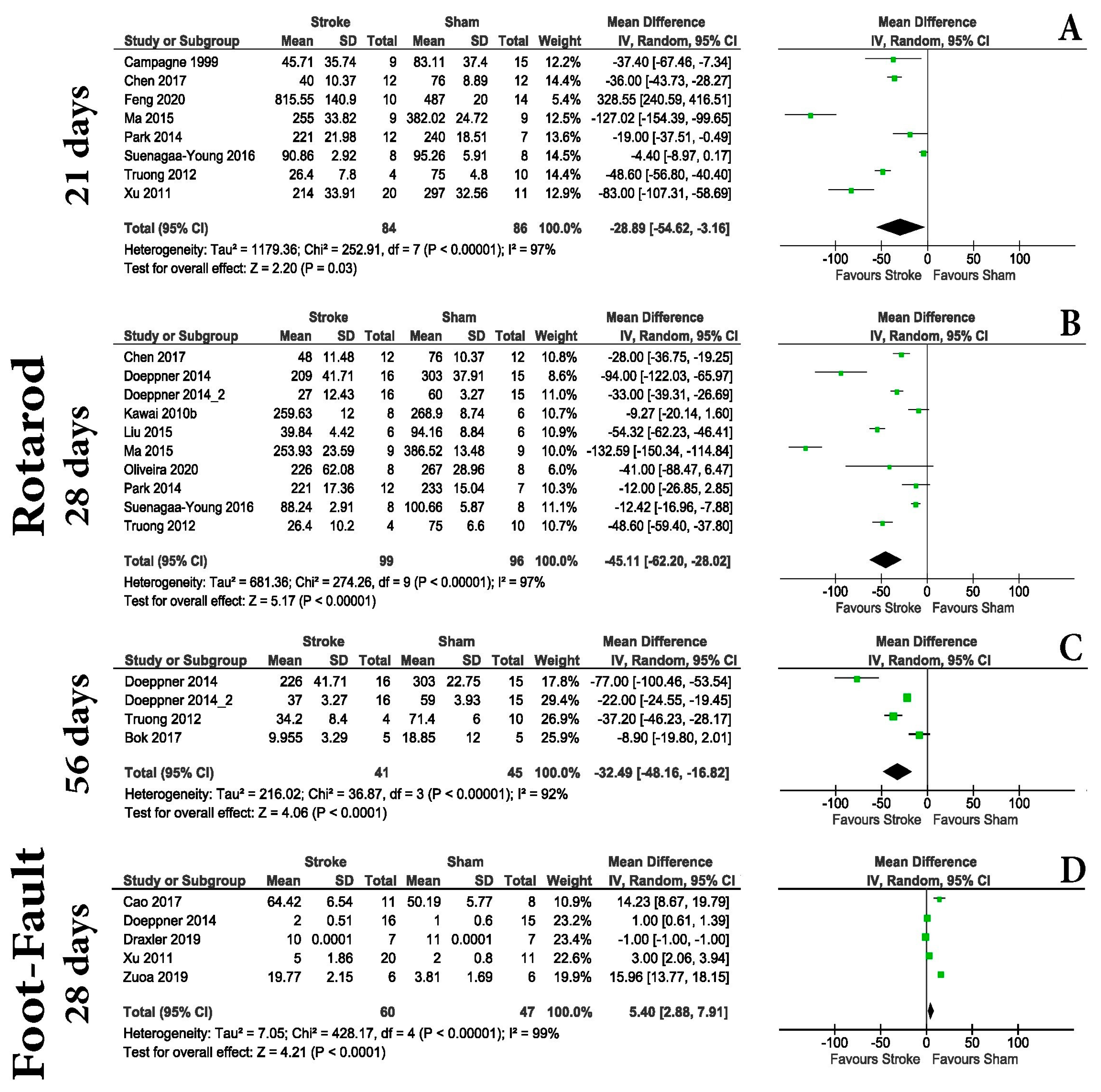
3.4. Motor Evaluation Is Unreliable for Distinguishing MCAo and Shams in the Chronic Post-Stroke Phase
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guzik, A.; Bushnell, C. Stroke Epidemiology and Risk Factor Management. Continuum 2017, 23, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, M.P.; Norrving, B.; Sacco, R.L.; Brainin, M.; Hacke, W.; Martins, S.; Pandian, J.; Feigin, V. World Stroke Organization (WSO): Global Stroke Fact Sheet 2019. Int. J. Stroke 2019, 14, 806–817. [Google Scholar] [CrossRef] [PubMed]
- Batista, T.F.P.; Manuel, P.F.; Correia, A.C. Essential Thrombocythemia—A Predisponent Factor for Stroke. Rev. Da Assoc. Med. Bras. 2019, 65, 772–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef] [PubMed]
- da Silva, H.; Nucci, M.P.; Mamani, J.B.; Mendez-Otero, R.; Nucci, L.P.; Tannus, A.; Gamarra, L.F. Evaluation of temperature induction in focal ischemic thermocoagulation model. PLoS ONE 2018, 13, e0200135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluri, F.; Schuhmann, M.K.; Kleinschnitz, C. Animal models of ischemic stroke and their application in clinical research. Drug Des. Dev. Ther. 2015, 9, 3445–3454. [Google Scholar] [CrossRef] [Green Version]
- Hånell, A.; Marklund, N. Structured evaluation of rodent behavioral tests used in drug discovery research. Front. Behav. Neurosci. 2014, 8, 252. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Truong, D.T.; Venna, V.R.; McCullough, L.D.; Fitch, R.H. Deficits in auditory, cognitive, and motor processing following reversible middle cerebral artery occlusion in mice. Exp. Neurol. 2012, 238, 114–121. [Google Scholar] [CrossRef]
- Suenaga, J.; Hu, X.; Pu, H.; Shi, Y.; Hassan, S.H.; Xu, M.; Leak, R.K.; Stetler, R.A.; Gao, Y.; Chen, J. White matter injury and microglia/macrophage polarization are strongly linked with age-related long-term deficits in neurological function after stroke. Exp. Neurol. 2015, 272, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Bok, S.; Kim, Y.E.; Woo, Y.; Kim, S.; Kang, S.J.; Lee, Y.; Park, S.K.; Weissman, I.L.; Ahn, G.O. Hypoxia-inducible factor-1α regulates microglial functions affecting neuronal survival in the acute phase of ischemic stroke in mice. Oncotarget 2017, 8, 111508–111521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.H.; Feng, D.; Zhang, Y.F.; Shang, Y.; Wu, Y.; Li, X.F.; Pei, L. Chloral Hydrate Preconditioning Protects Against Ischemic Stroke via Upregulating Annexin A1. CNS Neurosci. Ther. 2015, 21, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Liu, H.; Zuo, F.; Zhang, L. Adenoviruses-mediated RNA interference targeting cytosolic phospholipase A2α attenuates focal ischemic brain damage in mice. Mol. Med. Rep. 2018, 17, 5601–5610. [Google Scholar] [CrossRef] [Green Version]
- Kawai, H.; Yamashita, T.; Ohta, Y.; Deguchi, K.; Nagotani, S.; Zhang, X.; Ikeda, Y.; Matsuura, T.; Abe, K. Tridermal tumorigenesis of induced pluripotent stem cells transplanted in ischemic brain. J. Cereb. Blood Flow Metab. 2010, 30, 1487–1493. [Google Scholar] [CrossRef] [PubMed]
- Chang-Mu, C.; Cheng-Tien, W.; Ting-Hua, Y.; Liu, S.-H.; Feng-Yi, Y. Preventive Effect of Low Intensity Pulsed Ultrasound against Experimental Cerebral Ischemia/Reperfusion Injury via Apoptosis Reduction and Brain-derived Neurotrophic Factor Induction. Sci. Rep. 2018, 8, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Liu, H.; Zhang, H.; Ye, Q.; Wang, J.; Yang, B.; Mao, L.; Zhu, W.; Leak, R.K.; Xiao, B.; et al. ST2/IL-33-Dependent Microglial Response Limits Acute Ischemic Brain Injury. J. Neurosci. 2017, 37, 4692–4704. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Wong, S.; Snyder, E.Y.; Hamblin, M.H.; Lee, J.P. Human neural stem cells rapidly ameliorate symptomatic inflammation in early-stage ischemic-reperfusion cerebral injury. Stem Cell Res. Ther. 2014, 5, 129. [Google Scholar] [CrossRef] [Green Version]
- Li, D.J.; Li, Y.H.; Yuan, H.B.; Qu, L.F.; Wang, P. The novel exercise-induced hormone irisin protects against neuronal injury via activation of the Akt and ERK1/2 signaling pathways and contributes to the neuroprotection of physical exercise in cerebral ischemia. Metabolism 2017, 68, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Zuo, X.; Lu, J.; Manaenko, A.; Qi, X.; Tang, J.; Mei, Q.; Xia, Y.; Hu, Q. MicroRNA-132 attenuates cerebral injury by protecting blood-brain-barrier in MCAO mice. Exp. Neurol. 2019, 316, 12–19. [Google Scholar] [CrossRef]
- Zhang, Y.; Hu, Y.; Li, M.; Wang, J.; Guo, G.; Li, F.; Yu, B.; Kou, J. The Traditional Chinese Medicine Compound, GRS, Alleviates Blood-Brain Barrier Dysfunction. Drug Des. Dev. Ther. 2020, 14, 933–947. [Google Scholar] [CrossRef] [Green Version]
- Tian, Y.S.; Zhong, D.; Liu, Q.Q.; Zhao, X.L.; Sun, H.X.; Jin, J.; Wang, H.N.; Li, G.Z. Upregulation of miR-216a exerts neuroprotective effects against ischemic injury through negatively regulating JAK2/STAT3-involved apoptosis and inflammatory pathways. J. Neurosurg. 2018, 130, 977–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, J.; Jiang, Z.; Chen, Y.; Zhou, C.; Chen, C. Knockout of programmed cell death 5 (PDCD5) gene attenuates neuron injury after middle cerebral artery occlusion in mice. Brain Res. 2016, 1650, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Geng, W.; Cai, L.; Han, K.; Li, D.; Mo, Y.; Dai, Q.; Tang, H.; Zhang, M.; Akuetteh, P.D.P.; Balelang, M.F.; et al. Electroacupuncture Pretreatment Alleviates Cerebral Ischemia-Reperfusion Injury by Increasing GSK-3β Phosphorylation Level via Adenosine A1 Receptor. BioMed Res. Int. 2020, 2020, 6848450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Chen, X.; Li, D.; Liu, H.; Ding, Y.; Han, R.; Shi, Y.; Ma, X. PR-957 mediates neuroprotection by inhibiting Th17 differentiation and modulating cytokine production in a mouse model of ischaemic stroke. Clin. Exp. Immunol. 2018, 193, 194–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, R.; Gibson, C.L.; Kendall, D.A.; Bath, P.M.W. Evaluating the translational potential of progesterone treatment following transient cerebral ischaemia in male mice. BMC Neurosci. 2014, 15, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, B.; Meng, L.; Luan, L.; Fang, Z.; Zhao, P.; Zhao, G. Upregulation of Extracellular Vesicles-Encapsulated miR-132 Released From Mesenchymal Stem Cells Attenuates Ischemic Neuronal Injury by Inhibiting Smad2/c-jun Pathway via Acvr2b Suppression. Front. Cell Dev. Biol. 2020, 8, 568304. [Google Scholar] [CrossRef] [PubMed]
- Patkar, S.; Tate, R.; Modo, M.; Plevin, R.; Carswell, H.V. Conditionally immortalised neural stem cells promote functional recovery and brain plasticity after transient focal cerebral ischaemia in mice. Stem Cell Res. 2012, 8, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Gil, C.H.; Kim, Y.R.; Lee, H.J.; Jung, D.H.; Shin, H.K.; Choi, B.T. Aripiprazole exerts a neuroprotective effect in mouse focal cerebral ischemia. Exp. Ther. Med. 2018, 15, 745–750. [Google Scholar] [CrossRef] [Green Version]
- Draxler, D.F.; Lee, F.; Ho, H.; Keragala, C.B.; Medcalf, R.L.; Niego, B. t-PA Suppresses the Immune Response and Aggravates Neurological Deficit in a Murine Model of Ischemic Stroke. Front. Immunol. 2019, 10, 591. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; Peng, M.; Xu, P.; Huang, F.; Xie, Y.; Li, J.; Hong, Y.; Guo, H.; Liu, Q.; Zhu, W. Low-density lipoprotein receptor (LDLR) regulates NLRP3-mediated neuronal pyroptosis following cerebral ischemia/reperfusion injury. J. Neuroinflammation 2020, 17, 330. [Google Scholar] [CrossRef]
- Wang, D.; Liu, F.; Zhu, L.; Lin, P.; Han, F.; Wang, X.; Tan, X.; Lin, L.; Xiong, Y. FGF21 alleviates neuroinflammation following ischemic stroke by modulating the temporal and spatial dynamics of microglia/macrophages. J. Neuroinflammation 2020, 17, 257. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.; Fan, J.; Zhang, X.; Song, H.; Wan, R.; Wang, W.; Yin, Y. Decreased neuronal synaptosome associated protein 29 contributes to poststroke cognitive impairment by disrupting presynaptic maintenance. Theranostics 2021, 11, 4616–4636. [Google Scholar] [CrossRef]
- Xu, P.; Zhang, X.; Liu, Q.; Xie, Y.; Shi, X.; Chen, J.; Li, Y.; Guo, H.; Sun, R.; Hong, Y.; et al. Microglial TREM-1 receptor mediates neuroinflammatory injury via interaction with SYK in experimental ischemic stroke. Cell Death Dis. 2019, 10, 555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahid-Ansari, F.; Lagace, D.C.; Albert, P.R. Persistent post-stroke depression in mice following unilateral medial prefrontal cortical stroke. Transl. Psychiatry 2016, 6, e863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, Z.; Zhang, Z.; Ke, J.; Wang, Y.; Wu, H. Exercise-Linked Irisin Prevents Mortality and Enhances Cognition in a Mice Model of Cerebral Ischemia by Regulating Klotho Expression. Oxidative Med. Cell. Longev. 2021, 2021, 1697070. [Google Scholar] [CrossRef] [PubMed]
- Pallast, N.; Wieters, F.; Nill, M.; Fink, G.R.; Aswendt, M. Graph theoretical quantification of white matter reorganization after cortical stroke in mice. Neuroimage 2020, 217, 116873. [Google Scholar] [CrossRef]
- Gandin, C.; Widmann, C.; Lazdunski, M.; Heurteaux, C. MLC901 Favors Angiogenesis and Associated Recovery after Ischemic Stroke in Mice. Cerebrovasc. Dis. 2016, 42, 139–154. [Google Scholar] [CrossRef]
- Kamat, P.K.; Kalani, A.; Metreveli, N.; Tyagi, S.C.; Tyagi, N. A possible molecular mechanism of hearing loss during cerebral ischemia in mice. Can. J. Physiol. Pharmacol. 2015, 93, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Popescu, M.; Longo, S.; Gao, M.; Wang, D.; McGillis, S.; Zhao, L.R. Fibrinogen Reduction and Motor Function Improvement by Hematopoietic Growth Factor Treatment in Chronic Stroke in Aged Mice: A Treatment Frequency Study. Cell Transplant. 2016, 25, 729–734. [Google Scholar] [CrossRef] [Green Version]
- Feng, L.; Han, C.-X.; Cao, S.-Y.; Zhang, H.-M.; Wu, G.-Y. Deficits in motor and cognitive functions in an adult mouse model of hypoxia-ischemia induced stroke. Sci. Rep. 2020, 10, 20646. [Google Scholar] [CrossRef]
- Li, S.; Wang, Y.; Jiang, Z.; Huai, Y.; Liao, J.K.; Lynch, K.A.; Zafonte, R.; Wood, L.J.; Wang, Q.M. Impaired Cognitive Performance in Endothelial Nitric Oxide Synthase Knockout Mice After Ischemic Stroke: A Pilot Study. Am. J. Phys. Med. Rehabil. 2018, 97, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Balasubramanian, A.; Pedersen, S.E.; Romero, J.; Pautler, R.G.; Marrelli, S.P. TRPV1-mediated Pharmacological Hypothermia Promotes Improved Functional Recovery Following Ischemic Stroke. Sci. Rep. 2017, 7, 17685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doll, D.N.; Engler-Chiurazzi, E.B.; Lewis, S.E.; Hu, H.; Kerr, A.E.; Ren, X.; Simpkins, J.W. Lipopolysaccharide exacerbates infarct size and results in worsened post-stroke behavioral outcomes. Behav. Brain Funct. 2015, 11, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Q.; Chen, X.; Ma, J.; Jiang, X.; Chen, J.; Zhang, M.; Wu, Y.; Zhang, W.; Chen, C. Effect of Methylene Blue on White Matter Injury after Ischemic Stroke. Oxidative Med. Cell. Longev. 2021, 2021, 6632411. [Google Scholar] [CrossRef]
- Liu, D.; Croteau, D.L.; Souza-Pinto, N.; Pitta, M.; Tian, J.; Wu, C.; Jiang, H.; Mustafa, K.; Keijzers, G.; Bohr, V.A.; et al. Evidence that OGG1 glycosylase protects neurons against oxidative DNA damage and cell death under ischemic conditions. J. Cereb. Blood Flow Metab. 2011, 31, 680–692. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Gao, J.; Hou, B.; Liu, J.; Chen, S.; Yan, G.; Ren, H. Neural stem cell transplantation promotes behavioral recovery in a photothrombosis stroke model. Int. J. Clin. Exp. Pathol. 2015, 8, 7838–7848. [Google Scholar]
- Xia, Q.; Li, X.; Zhou, H.; Zheng, L.; Shi, J. S100A11 protects against neuronal cell apoptosis induced by cerebral ischemia via inhibiting the nuclear translocation of annexin A1. Cell Death Dis. 2018, 9, 657. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; Marasini, S.; Kim, G.H.; Ku, T.; Choi, C.; Park, M.Y.; Kim, E.H.; Lee, Y.D.; Suh-Kim, H.; Kim, S.S. A method for generating a mouse model of stroke: Evaluation of parameters for blood flow, behavior, and survival. Exp. Neurobiol. 2014, 23, 104–114. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Xia, J.; Zhang, F.; Shi, Y.; Wu, Y.; Pu, H.; Liou, A.K.; Leak, R.K.; Yu, X.; Chen, L.; et al. Galectin-1-secreting neural stem cells elicit long-term neuroprotection against ischemic brain injury. Sci. Rep. 2015, 5, 9621. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Xiang, Z.; Zhang, W.; Yu, Z.; Xin, X.; Zhang, R.; Deng, Y.; Yuan, Q. Protective effect of DLX6-AS1 silencing against cerebral ischemia/reperfusion induced impairments. Aging 2020, 12, 23096–23113. [Google Scholar] [CrossRef]
- Chen, J.-Y.; Yu, Y.; Yuan, Y.; Zhang, Y.-J.; Fan, X.-P.; Yuan, S.-Y.; Zhang, J.-C.; Yao, S.-L. Enriched housing promotes post-stroke functional recovery through astrocytic HMGB1-IL-6-mediated angiogenesis. Cell Death Discov. 2017, 3, 17054. [Google Scholar] [CrossRef] [Green Version]
- Li, P.C.; Jiao, Y.; Ding, J.; Chen, Y.C.; Cui, Y.; Qian, C.; Yang, X.Y.; Ju, S.H.; Yao, H.H.; Teng, G.J. Cystamine improves functional recovery via axon remodeling and neuroprotection after stroke in mice. CNS Neurosci. Ther. 2015, 21, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Doeppner, T.R.; Kaltwasser, B.; Bahr, M.; Hermann, D.M. Effects of neural progenitor cells on post-stroke neurological impairment-a detailed and comprehensive analysis of behavioral tests. Front. Cell. Neurosci. 2014, 8, 338. [Google Scholar] [CrossRef]
- Kossatz, E.; Silva-Peña, D.; Suárez, J.; de Fonseca, F.R.; Maldonado, R.; Robledo, P. Octadecylpropyl Sulfamide Reduces Neurodegeneration and Restores the Memory Deficits Induced by Hypoxia-Ischemia in Mice. Front. Pharmacol. 2018, 9, 376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Nieuwenhuijzen, P.S.; Parker, K.; Liao, V.; Houlton, J.; Kim, H.L.; Johnston, G.A.R.; Hanrahan, J.R.; Chebib, M.; Clarkson, A.N. Targeting GABA(C) Receptors Improves Post-Stroke Motor Recovery. Brain Sci. 2021, 11, 315. [Google Scholar] [CrossRef]
- de Oliveira, J.L.; Ávila, M.; Martins, T.C.; Alvarez-Silva, M.; Winkelmann-Duarte, E.C.; Salgado, A.S.I.; Cidral-Filho, F.J.; Reed, W.R.; Martins, D.F. Medium- and long-term functional behavior evaluations in an experimental focal ischemic stroke mouse model. Cogn. Neurodynamics 2020, 14, 473–481. [Google Scholar] [CrossRef]
- Du, J.; Yin, G.; Hu, Y.; Shi, S.; Jiang, J.; Song, X.; Zhang, Z.; Wei, Z.; Tang, C.; Lyu, H. Coicis semen protects against focal cerebral ischemia-reperfusion injury by inhibiting oxidative stress and promoting angiogenesis via the TGFβ/ALK1/Smad1/5 signaling pathway. Aging 2020, 13, 877–893. [Google Scholar] [CrossRef]
- Wang, G.; Han, B.; Shen, L.; Wu, S.; Yang, L.; Liao, J.; Wu, F.; Li, M.; Leng, S.; Zang, F.; et al. Silencing of circular RNA HIPK2 in neural stem cells enhances functional recovery following ischaemic stroke. EBioMedicine 2020, 52, 102660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cunningham, C.J.; Wong, R.; Barrington, J.; Tamburrano, S.; Pinteaux, E.; Allan, S.M. Systemic conditioned medium treatment from interleukin-1 primed mesenchymal stem cells promotes recovery after stroke. Stem Cell Res. Ther. 2020, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Vollmer, M.K.; Fernandez, V.M.; Dweik, Y.; Kim, H.; Doré, S. Korean Red Ginseng Pretreatment Protects against Long-Term Sensorimotor Deficits after Ischemic Stroke Likely through Nrf2. Front. Cell. Neurosci. 2018, 12, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Lookeren Campagne, M.; Thibodeaux, H.; van Bruggen, N.; Cairns, B.; Gerlai, R.; Palmer, J.T.; Williams, S.P.; Lowe, D.G. Evidence for a protective role of metallothionein-1 in focal cerebral ischemia. Proc. Natl. Acad. Sci. USA 1999, 96, 12870–12875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Xiong, X.; Ouyang, Y.; Barreto, G.; Giffard, R. Heat shock protein 72 (Hsp72) improves long term recovery after focal cerebral ischemia in mice. Neurosci. Lett. 2011, 488, 279–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, S.M.; Kim, Y.R.; Kim, H.N.; Choi, Y.W.; Lee, J.W.; Kim, C.M.; Baek, J.U.; Shin, H.K.; Choi, B.T. Neuroprotection and spatial memory enhancement of four herbal mixture extract in HT22 hippocampal cells and a mouse model of focal cerebral ischemia. BMC Complement. Altern. Med. 2015, 15, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroke Therapy Academic Industry Roundtable. Recommendations for standards regarding preclinical neuroprotective and restorative drug development. Stroke 1999, 30, 2752–2758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Cochrane: Lomdon, UK, 2022. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef]
- Borenstein, M.; Higgins, J.P.; Hedges, L.V.; Rothstein, H.R. Basics of meta-analysis: I(2) is not an absolute measure of heterogeneity. Res. Synth. Methods 2017, 8, 5–18. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M. Research Note: In a meta-analysis, the I(2) index does not tell us how much the effect size varies across studies. J. Physiother. 2020, 66, 135–139. [Google Scholar] [CrossRef]
- Borenstein, M. In a Meta-Analysis, the I-squared statistic does not tell us how much the effect size varies. J. Clin. Epidemiol. 2022, 152, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.M.; Hasso, A.N.; Handwerker, J.; Farid, H. Sequence-specific MR imaging findings that are useful in dating ischemic stroke. RadioGraphics 2012, 32, 1285–1297. [Google Scholar] [CrossRef] [Green Version]
- Willemsen, M.H.; Ba, W.; Wissink-Lindhout, W.M.; de Brouwer, A.P.; Haas, S.A.; Bienek, M.; Hu, H.; Vissers, L.E.; van Bokhoven, H.; Kalscheuer, V.; et al. Involvement of the kinesin family members KIF4A and KIF5C in intellectual disability and synaptic function. J. Med. Genet. 2014, 51, 487–494. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.; Stark, B.; Johnson, C.; Roth, G.; Bisignano, C.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; Abualhasan, A.; et al. Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Béjot, Y.; Christensen, L.M.; De Marchis, G.M.; Dichgans, M.; Hagberg, G.; Heldner, M.R.; Milionis, H.; Li, L.; Pezzella, F.R.; et al. European Stroke Organisation (ESO) guideline on pharmacological interventions for long-term secondary prevention after ischaemic stroke or transient ischaemic attack. Eur. Stroke J. 2022, 7, I–II. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.C.; Cutler, D.M.; Rosen, A.B. Trends in thrombolytic use for ischemic stroke in the United States. J. Hosp. Med. 2010, 5, 406–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hara, H.; Friedlander, R.M.; Gagliardini, V.; Ayata, C.; Fink, K.; Huang, Z.; Shimizu-Sasamata, M.; Yuan, J.; Moskowitz, M.A. Inhibition of interleukin 1beta converting enzyme family proteases reduces ischemic and excitotoxic neuronal damage. Proc. Natl. Acad. Sci. USA 1997, 94, 2007–2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morega, S.; Cătălin, B.; Simionescu, C.E.; Sapalidis, K.; Rogoveanu, I. Cerebrolysin Prevents Brain Injury in a Mouse Model of Liver Damage. Brain Sci. 2021, 11, 1622. [Google Scholar] [CrossRef]
- Osiac, E.; Mitran, S.I.; Manea, C.N.; Cojocaru, A.; Rosu, G.C.; Osiac, M.; Pirici, D.N.; Bălșeanu, A.T.; Cătălin, B. Optical coherence tomography microscopy in experimental traumatic brain injury. Microsc. Res. Tech. 2021, 84, 422–431. [Google Scholar] [CrossRef]
- Pirici, I.; Balsanu, T.A.; Bogdan, C.; Margaritescu, C.; Divan, T.; Vitalie, V.; Mogoanta, L.; Pirici, D.; Carare, R.O.; Muresanu, D.F. Inhibition of Aquaporin-4 Improves the Outcome of Ischaemic Stroke and Modulates Brain Paravascular Drainage Pathways. Int. J. Mol. Sci. 2017, 19, 46. [Google Scholar] [CrossRef] [Green Version]
- Catalin, B.; Rogoveanu, O.C.; Pirici, I.; Balseanu, T.A.; Stan, A.; Tudorica, V.; Balea, M.; Mindrila, I.; Albu, C.V.; Mohamed, G.; et al. Cerebrolysin and Aquaporin 4 Inhibition Improve Pathological and Motor Recovery after Ischemic Stroke. CNS Neurol. Disord. Drug Targets 2018, 17, 299–308. [Google Scholar] [CrossRef]
- Surugiu, R.; Catalin, B.; Dumbrava, D.; Gresita, A.; Olaru, D.G.; Hermann, D.M.; Popa-Wagner, A. Intracortical Administration of the Complement C3 Receptor Antagonist Trifluoroacetate Modulates Microglia Reaction after Brain Injury. Neural Plast. 2019, 2019, 1071036. [Google Scholar] [CrossRef] [Green Version]
- Gresita, A.; Glavan, D.; Udristoiu, I.; Catalin, B.; Hermann, D.M.; Popa-Wagner, A. Very Low Efficiency of Direct Reprogramming of Astrocytes Into Neurons in the Brains of Young and Aged Mice After Cerebral Ischemia. Front. Aging Neurosci. 2019, 11, 334. [Google Scholar] [CrossRef] [Green Version]
- Popescu, E.S.; Pirici, I.; Ciurea, R.N.; Bălşeanu, T.A.; Cătălin, B.; Mărgăritescu, C.; Mogoantă, L.; Hostiuc, S.; Pirici, D. Three-dimensional organ scanning reveals brain edema reduction in a rat model of stroke treated with an aquaporin 4 inhibitor. Rom. J. Morphol. Embryol. 2017, 58, 59–66. [Google Scholar] [PubMed]
- Demyanenko, S.; Nikul, V.; Rodkin, S.; Davletshin, A.; Evgen’ev, M.B.; Garbuz, D.G. Exogenous recombinant Hsp70 mediates neuroprotection after photothrombotic stroke. Cell Stress Chaperones 2021, 26, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, H.; Toyoda, K.; Omae, K.; Ishida, N.; Uchiyama, S.; Kimura, K.; Sakai, N.; Okada, Y.; Tanaka, K.; Origasa, H.; et al. Dual Antiplatelet Therapy Using Cilostazol with Aspirin or Clopidogrel: Subanalysis of the CSPS.com Trial. Stroke 2021, 52, 3430–3439. [Google Scholar] [CrossRef] [PubMed]
- Olinger, C.P.; Adams, H.P., Jr.; Brott, T.G.; Biller, J.; Barsan, W.G.; Toffol, G.J.; Eberle, R.W.; Marler, J.R. High-dose intravenous naloxone for the treatment of acute ischemic stroke. Stroke 1990, 21, 721–725. [Google Scholar] [CrossRef] [Green Version]
- Dávalos, A.; Alvarez-Sabín, J.; Castillo, J.; Díez-Tejedor, E.; Ferro, J.; Martínez-Vila, E.; Serena, J.; Segura, T.; Cruz, V.T.; Masjuan, J.; et al. Citicoline in the treatment of acute ischaemic stroke: An international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet 2012, 380, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.E.; Zoppo, G.J.d.; Demaerschalk, B.M.; Demchuk, A.M.; Diener, H.-C.; Howard, G.; Kaste, M.; Pancioli, A.M.; Ringelstein, E.B.; Spatareanu, C.; et al. Ancrod in Acute Ischemic Stroke. Stroke 2009, 40, 3796–3803. [Google Scholar] [CrossRef] [PubMed]
- Ibarrola, D.; Seegers, H.; Jaillard, A.; Hommel, M.; Décorps, M.; Massarelli, R. The effect of eliprodil on the evolution of a focal cerebral ischaemia in vivo. Eur. J. Pharmacol. 1998, 352, 29–35. [Google Scholar] [CrossRef]
- Gribkoff, V.K.; Starrett, J.E.; Dworetzky, S.I.; Hewawasam, P.; Boissard, C.G.; Cook, D.A.; Frantz, S.W.; Heman, K.; Hibbard, J.R.; Huston, K.; et al. Targeting acute ischemic stroke with a calcium-sensitive opener of maxi-K potassium channels. Nat. Med. 2001, 7, 471–477. [Google Scholar] [CrossRef]
- Chen, W.; Xia, M.; Guo, C.; Jia, Z.; Wang, J.; Li, C.; Li, M.; Tang, X.; Hu, R.; Chen, Y.; et al. Modified behavioural tests to detect white matter injury- induced motor deficits after intracerebral haemorrhage in mice. Sci. Rep. 2019, 9, 16958. [Google Scholar] [CrossRef] [Green Version]
- Ruan, J.; Yao, Y. Behavioral tests in rodent models of stroke. Brain Hemorrhages 2020, 1, 171–184. [Google Scholar] [CrossRef]
- Bieber, M.; Gronewold, J.; Scharf, A.C.; Schuhmann, M.K.; Langhauser, F.; Hopp, S.; Mencl, S.; Geuss, E.; Leinweber, J.; Guthmann, J.; et al. Validity and Reliability of Neurological Scores in Mice Exposed to Middle Cerebral Artery Occlusion. Stroke 2019, 50, 2875–2882. [Google Scholar] [CrossRef] [PubMed]
- Van Norman, G.A. Limitations of Animal Studies for Predicting Toxicity in Clinical Trials: Part 2: Potential Alternatives to the Use of Animals in Preclinical Trials. JACC Basic Transl. Sci. 2020, 5, 387–397. [Google Scholar] [CrossRef] [PubMed]
- de Boo, J.; Hendriksen, C. Reduction strategies in animal research: A review of scientific approaches at the intra-experimental, supra-experimental and extra-experimental levels. Altern. Lab. Anim. 2005, 33, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Charan, J.; Kantharia, N.D. How to calculate sample size in animal studies? J. Pharmacol. Pharmacother. 2013, 4, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkaya, M.; Kröber, J.M.; Rex, A.; Endres, M. Assessing post-stroke behavior in mouse models of focal ischemia. J. Cereb. Blood Flow Metab. 2013, 33, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Fritz, A.K.; Amrein, I.; Wolfer, D.P. Similar reliability and equivalent performance of female and male mice in the open field and water-maze place navigation task. Semin. Med. Genet. Part C Am. J. Med. Genet. 2017, 175, 380–391. [Google Scholar] [CrossRef] [Green Version]
- Oydanich, M.; Babici, D.; Zhang, J.; Rynecki, N.; Vatner, D.E.; Vatner, S.F. Mechanisms of sex differences in exercise capacity. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2019, 316, R832–R838. [Google Scholar] [CrossRef]
- Carmichael, S.T. Rodent models of focal stroke: Size, mechanism, and purpose. NeuroRx 2005, 2, 396–409. [Google Scholar] [CrossRef] [Green Version]
- McColl, B.W.; Carswell, H.V.; McCulloch, J.; Horsburgh, K. Extension of cerebral hypoperfusion and ischaemic pathology beyond MCA territory after intraluminal filament occlusion in C57Bl/6J mice. Brain Res. 2004, 997, 15–23. [Google Scholar] [CrossRef]
- Maeda, K.; Hata, R.; Hossmann, K.A. Regional metabolic disturbances and cerebrovascular anatomy after permanent middle cerebral artery occlusion in C57black/6 and SV129 mice. Neurobiol. Dis. 1999, 6, 101–108. [Google Scholar] [CrossRef]
- Belayev, L.; Obenaus, A.; Mukherjee, P.K.; Knott, E.J.; Khoutorova, L.; Reid, M.M.; Roque, C.R.; Nguyen, L.; Lee, J.B.; Petasis, N.A.; et al. Blocking pro-inflammatory platelet-activating factor receptors and activating cell survival pathways: A novel therapeutic strategy in experimental ischemic stroke. Brain Circ. 2020, 6, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Gillardon, F.; Lenz, C.; Waschke, K.F.; Krajewski, S.; Reed, J.C.; Zimmermann, M.; Kuschinsky, W. Altered expression of Bcl-2, Bcl-X, Bax, and c-Fos colocalizes with DNA fragmentation and ischemic cell damage following middle cerebral artery occlusion in rats. Mol. Brain Res. 1996, 40, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Sharp, F.R.; Lu, A.; Tang, Y.; Millhorn, D.E. Multiple molecular penumbras after focal cerebral ischemia. J. Cereb. Blood Flow Metab. 2000, 20, 1011–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermann, D.M.; Kilic, E.; Hata, R.; Hossmann, K.A.; Mies, G. Relationship between metabolic dysfunctions, gene responses and delayed cell death after mild focal cerebral ischemia in mice. Neuroscience 2001, 104, 947–955. [Google Scholar] [CrossRef]
- Belayev, L.; Busto, R.; Zhao, W.; Fernandez, G.; Ginsberg, M.D. Middle cerebral artery occlusion in the mouse by intraluminal suture coated with poly-L-lysine: Neurological and histological validation. Brain Res. 1999, 833, 181–190. [Google Scholar] [CrossRef]
- Hata, R.; Maeda, K.; Hermann, D.; Mies, G.; Hossmann, K.A. Evolution of brain infarction after transient focal cerebral ischemia in mice. J. Cereb. Blood Flow Metab. 2000, 20, 937–946. [Google Scholar] [CrossRef]
- da Costa Daniele, T.M.; de Bruin, P.F.C.; de Matos, R.S.; de Bruin, G.S.; Maia Chaves, C.J.; de Bruin, V.M.S. Exercise effects on brain and behavior in healthy mice, Alzheimer’s disease and Parkinson’s disease model-A systematic review and meta-analysis. Behav. Brain Res. 2020, 383, 112488. [Google Scholar] [CrossRef]
- Skinner, J.A.; Campbell, E.J.; Dayas, C.V.; Garg, M.L.; Burrows, T.L. The relationship between oxytocin, dietary intake and feeding: A systematic review and meta-analysis of studies in mice and rats. Front. Neuroendocrinol. 2019, 52, 65–78. [Google Scholar] [CrossRef]
- Schmidt, A.; Wellmann, J.; Schilling, M.; Strecker, J.K.; Sommer, C.; Schäbitz, W.R.; Diederich, K.; Minnerup, J. Meta-analysis of the efficacy of different training strategies in animal models of ischemic stroke. Stroke 2014, 45, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Bachour, S.P.; Hevesi, M.; Bachour, O.; Sweis, B.M.; Mahmoudi, J.; Brekke, J.A.; Divani, A.A. Comparisons between Garcia, Modo, and Longa rodent stroke scales: Optimizing resource allocation in rat models of focal middle cerebral artery occlusion. J. Neurol. Sci. 2016, 364, 136–140. [Google Scholar] [CrossRef]
- Zhu, W.; Casper, A.; Libal, N.L.; Murphy, S.J.; Bodhankar, S.; Offner, H.; Alkayed, N.J. Preclinical evaluation of recombinant T cell receptor ligand RTL1000 as a therapeutic agent in ischemic stroke. Transl. Stroke Res. 2015, 6, 60–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study/Year | Species | N | Gender | Age (Weeks) | Stroke Method | Stroke Time (min) | Reperfusion | Behaviour Test | Neurological Scale |
|---|---|---|---|---|---|---|---|---|---|
| Truong 2012 [9] | C57BL/6 | 4 | Male | 4 | MCAO monofilament | 60 | Yes | Rotarod Morris water maze | -------- |
| Suenagaa-Young 2016 [10] | C57BL/6J | 8 | Male | 10 | MCA ligaturation and electrocauterization | permanent | No | Rotarod Morris water maze | -------- |
| Bok 2017 [11] | C57BL/6J | 5 | --------- | -------- | MCAO monofilament | 60 | Yes | Rotarod | -------- |
| Liu 2015 [12] | C57BL/6J | 6 | Male | 12 | MCAO monofilament | 60 | Yes | Rotarod | -------- |
| Wu 2017 [13] | C57BL/6 | 3 | Male | 12–16 | MCAO monofilament | 60 | Yes | Rotarod | Longa |
| Kawai 2010 [14] | C57BL/6 | 8 | Male | 8–10 | MCAO monofilament | 30 | Yes | Rotarod | -------- |
| Chen 2018 [15] | C57BL/6 | 6 | Male | 6 | MCAO monofilament | 45 | Yes | Rotarod | -------- |
| Yang 2017 [16] | C57BL/6 | 8–9 | -------- | -------- | MCAO monofilament | 60 | Yes | Rotarod Cylinder | -------- |
| Huang 2014 [17] | C57BL/6J | 14 | Male | MCAO monofilament | 60 | Yes | Rotarod | -------- | |
| Li 2016 [18] | C57BL/6J | 8 | Male | -------- | MCAO monofilament | permanent | --------- | ----------- | Longa |
| Zuo 2019 [19] | C57BL/6 | 6 | Male | -------- | MCAO monofilament | 60 | Yes | Foot-fault | Garcia |
| Zhang 2020 [20] | C57BL/6J | 6 | -------- | 6–8 | MCAO monofilament | 60 | Yes | ----------- | Garcia |
| Shuang 2017 [21] | C57BL/6J | 3 | Male | -------- | MCAO monofilament | 120 | Yes | ----------- | Garcia |
| Lu 2016 [22] | C57BL/6N | 18 | Male | -------- | MCAO monofilament | 60 | Yes | ----------- | Garcia |
| Geng 2020 [23] | C57BL/6 | 6 | Male | MCAO monofilament | 90 | Yes | ----------- | Garcia | |
| Guo 2018 [24] | C57BL/6 | 10 | Male | 6–8 | MCAO monofilament | 60 | Yes | Foot-fault | -------- |
| Wong 2014 [25] | C57BL/6 | 3 | Male | -------- | MCAO monofilament | 30 | Yes | Foot-fault | Clark |
| Feng 2021 [26] | C57BL/6 | 6 | Male | -------- | ECA ligaturation | 60 | Yes | Foot-fault | -------- |
| Patkar 2011 [27] | C57BL/6 | 8 | Male | 12–14 | MCAO monofilament | 45 | Yes | Cylinder | Clark |
| Gil 2018 [28] | C57BL/6 | 6 | Male | 6 | MCAO monofilament | 30 | Yes | Cylinder | -------- |
| Draxler 2019 [29] | C57BL/6J | 7 | Male | 8–12 | MCAO monofilament | 60 | Yes | Foot-fault | -------- |
| Sun 2020 [30] | C57BL/6 | 8–12 | Male | 8–12 | MCAO monofilament | 90 | Yes | Morris water maze | -------- |
| Dongxue 2020 [31] | C57BL/6 | 4–10 | -------- | -------- | MCAO monofilament | 60 | Yes | Rotarod | -------- |
| Yan 2021 [32] | C57BL/6 | 8–9 | Male | 6–8 | MCAO monofilament | 60 | Yes | Morris water maze | ----------- |
| Xu 2019 [33] | C57BL/6J | ------- | -------- | -------- | MCAO monofilament | 90 | -------- | Morris water maze | -------- |
| Vahid-Ansari 2016 [34] | C57BL/6 | 10 | Male | 10–11 | Endothelin-1 | permanent | No | Cylinder | -------- |
| Jin 2021 [35] | C57BL/6J | ------- | -------- | -------- | MCAO monofilament | 120 | Yes | Morris water maze | -------- |
| Pallast 2020 [36] | C57BL/6J | 7–15 | -------- | 8 | Photothrombosis | permanent | No | Cylinder | -------- |
| Gandin 2015 [37] | C57BL/6 | 16 | Male | 9 | MCAO monofilament | 60 | Yes | Rotarod | -------- |
| Kamat 2015 [38] | C57BL/6J | 5 | Male | 10–12 | MCAO monofilament | 60 | Yes | -------- | Longa |
| Liu 2016 [39] | C57BL/6 | ------- | Male | 19–20 | MCA ligaturation and electrocauterization | permanent | No | Rotarod | -------- |
| Feng 2020 [40] | C57BL/6J | 10–14 | -------- | 12–14 | MCAO monofilament | 120 | Yes | Rotarod Morris water maze | -------- |
| Li 2018 [41] | C57BL/6 | 10–19 | Male | 10–14 | MCAO monofilament | 60 | Yes | Cylinder Morris water maze | -------- |
| Cao 2017 [42] | C57BL/6 | 8–11 | Male | 10–16 | Mechanically oclusion of MCA and CCA | 120 | Yes | Foot Fault | -------- |
| Doll 2015 [43] | C57BL/6J | 9–10 | Male | 12–16 | MCAO monofilament | 30 | Yes | Rotarod Cylinder | -------- |
| Cheng 2021 [44] | C57BL/6J | 10 | -------- | -------- | Photothrombosis | permanent | No | -------- | Garcia |
| Liu 2011 [45] | C57BL/6J | 9 | Male | 20–24 | Electrocauterization | permanent | No | Rotarod | -------- |
| Ma 2015 [46] | C57BL/6J | 9 | Male | -------- | Photothrombosis | permanent | No | Rotarod | -------- |
| Xia 2018 [47] | C57BL/6J | 10 | Male | -------- | MCAO monofilament | 60 | Yes | Rotarod Morris water maze | -------- |
| Kawai 2010 [14] | C57BL/6N | 6–8 | Male | 8–10 | MCAO monofilament | 30 | Yes | Rotarod | -------- |
| Park 2014 [48] | C57Bl/6J | ------- | Male | 13 | MCAO monofilament | 60–90 | Yes | Rotarod | -------- |
| Wang 2015 [49] | C57Bl/6 | 6–8 | Male | -------- | MCAO monofilament | 60 | Yes | Rotarod Cylinder Morris water maze | -------- |
| Hu 2020 [50] | C57Bl/6 | 6 | -------- | 8 | MCAO monofilament | 60 | Yes | Morris water maze | Clark |
| Chen 2017 [51] | C57Bl/6 | 12 | Male | 8–10 | MCAO monofilament | 60 | Yes | Rotarod | -------- |
| Li 2014 [52] | C57BL/6N | 8 | Male | 8–10 | Photothrombosis | permanent | No | Cylinder | -------- |
| Doeppner 2014 [53] | C57Bl/6 | ------- | Male | 10–12 | MCAO monofilament | 45 90 | Yes | Rotarod Foot Fault Morris water maze | -------- |
| Kossatz 2018 [54] | C57Bl/6J | ------- | Male | 8–11 | CCA ligaturation | permanent | No | Rotarod | -------- |
| Nieuwenhuijzen 2021 [55] | C57Bl/6J | 10 | Male | 8–12 | Photothrombosis | permanent | No | Cylinder | -------- |
| Oliveira 2020 [56] | C57Bl/6 | 8 | Male | -------- | MCA electrocauterization | permanent | No | Rotarod | -------- |
| Du 2021 [57] | C57Bl/6J | 5 | -------- | -------- | MCAO monofilament | 60 | Yes | -------- | Longa |
| Wang 2020 [58] | C57Bl/6J | 14 | Male | 8–9 | MCAO monofilament | 60 | Yes | Cylinder | -------- |
| Cunningham 2020 [59] | C57Bl/6 | 10–12 | Male | 12–20 | MCAO monofilament | 20 | Yes | Rotarod | -------- |
| Liu 2018 [60] | C57Bl/6 | ------- | Male | -------- | MCA electrocauterization | permanent | No | Cylinder | -------- |
| Campagne 1999 [61] | C57Bl/6J | 9–15 | -------- | 8–10 | MCA and CCA ligaturation | 45 | Yes | Rotarod | -------- |
| Xu 2011 [62] | C57Bl/6 | 11–20 | -------- | -------- | MCAO monofilament | 60 | Yes | Rotarod Foot-fault | -------- |
| Ahn 2015 [63] | C57Bl/6 | 10 | Male | -------- | MCAO monofilament | 30 | Yes | Morris water maze | -------- |
| Test/ Neurological Scale | Assesment | Time Window | Advantages | Disadventages | Articles |
|---|---|---|---|---|---|
| Garcia | Body symmetry Motor and sensoryal functions | 24 h up to 7 days post-stroke (hyper-acute post-stroke interval) | Easy to perform | Unable to assess long term outcome | [19,20,22,23,44,81] |
| Clark | Body symmetry Motor and sensoryal functions Reflex functions Body aspect | 24 h up to 7 days post-stroke (hyper-acute post-stroke interval up to acute and early sub-acute post-stroke interval) | Comprehensive evaluation | Complex Hard to perform | [25,27,50] |
| Longa | Motor function Cognitive impairment | 72 h post-stroke (the end of the hyper-acute post-stroke interval) | Easy to perform | Did not reveal the body symmeetry or sensory functions | [13,52,57] |
| Foot fault | Limb coordination Motor function | 24 h up to 28 days post-stroke (hyper-acute to acute-early subacute to chronic post-stroke interval) | Able to assess long term outcome Objective Effective Easy to perform | The results may be affected by individual variation Baseline masurements are requierd | [19,24,25,26,29,42,53,62] |
| Rotarod | Locomotor function Animal balance | 24 h up to 56 days post-stroke (hyper-acute to acute-early subacute to chronic post-stroke interval) | Able to assess long term outcome Objective Quantifiable | Training sesions are required Special apparature are required | [9,10,11,12,13,14,16,17,37,40,43,45,46,47,48,49,51,53,54,56,59,60,61,62,71] |
| Cylinder | Limb-use asymmetry | 7 to 14 days post-stroke (acute and early sub-acute post-stroke interval) | Easy to perform Objective Able to assess long-term outcome | It requires a lot of attention, preferably several operators Not useful for global stroke models | [16,27,28,34,36,41,43,49,53,55,58] |
| Morris water maze | Cognition Locomotor function | 24 h up to 56 days (hyper-acute to acute-early subacute to chronic post-stroke interval) | Able to assess both cognition and locomotor function Able to evaluate long-term outcome | Long trainings sesions, Trials are required, Large inter-individual variability in swimming ability | [9,10,30,32,33,35,40,47,49,50,53,63] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boboc, I.K.S.; Rotaru-Zavaleanu, A.D.; Calina, D.; Albu, C.V.; Catalin, B.; Turcu-Stiolica, A. A Preclinical Systematic Review and Meta-Analysis of Behavior Testing in Mice Models of Ischemic Stroke. Life 2023, 13, 567. https://doi.org/10.3390/life13020567
Boboc IKS, Rotaru-Zavaleanu AD, Calina D, Albu CV, Catalin B, Turcu-Stiolica A. A Preclinical Systematic Review and Meta-Analysis of Behavior Testing in Mice Models of Ischemic Stroke. Life. 2023; 13(2):567. https://doi.org/10.3390/life13020567
Chicago/Turabian StyleBoboc, Ianis Kevyn Stefan, Alexandra Daniela Rotaru-Zavaleanu, Daniela Calina, Carmen Valeria Albu, Bogdan Catalin, and Adina Turcu-Stiolica. 2023. "A Preclinical Systematic Review and Meta-Analysis of Behavior Testing in Mice Models of Ischemic Stroke" Life 13, no. 2: 567. https://doi.org/10.3390/life13020567